
Abstract
Purpose
Cervical cancer is the second most common cancers of women in India, despite being largely preventable. This review traces the journey of formulation of the Operational Guidelines for the management of common cancers and its implementation.
Methods
A literature review was done to document the process of formulation of the guidelines, in addition to inputs from the officials involved in the process of developing them.
Results
The review covers the pre-existing challenges in the National cancer control program and helps in providing recommendations for the future of cervical cancer screening, considering the COVID pandemic and the limitations of the public health system in India.
Conclusion
The implementation of early diagnosis of cervical cancer on a national scale as envisaged in the Operational Guidelines for the management of common cancers is a herculean task. A concerted approach for the implementation of cervical cancer control and HPV vaccination will hopefully bring fruitful results going forward.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Cervical Cancer Burden and Current Situation in India
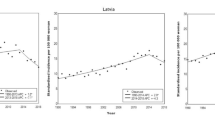
As per Globocan 2020, 604,100 new cases of cervical cancer were detected globally in 2020 and 341,831 deaths were attributed to this malignancy. In India, cervical cancer accounted for 9.4% of all cancers and 18.3% (123,907) of new cases in 2020. It still is amongst the commoner cancers in India and a leading cause of cancer-related deaths in women in low- and middle-income countries [1]. Although the age-standardized incidence rate of cervical cancer decreased substantially by 39.7% (95% UI 26·5–57.3) from 1990 to 2016, it is the second leading cause of cancer deaths for females in 12 Indian states [2].
The situation is more alarming in the rural areas where the majority of women are illiterate and ignorant about the hazards of cervical cancer as well as healthcare resources are scarce [3]. Poor prognosis due to late diagnosis is common in similar resource-constrained settings around the world, where women present with advanced stages of Human Papilloma Virus (HPV) caused cervical cancer and lack treatment facilities [4]. In addition to HPV infection, factors like age at the time of marriage, number of pregnancies genital hygiene, use of oral contraceptives, nutritional status, smoking, etc., are associated with the development of cervical cancer. Interventions ranging from prophylactic HPV vaccines to various screening approaches such as visual inspection with acetic acid or Lugol’s iodine (VIA/VILI), Papanicolaou test (Pap test or Pap smear) and HPV DNA (Deoxyribose Nucleic Acid) testing are used for early detection and prevention of cervical cancer [5].
Department of Health Research has recently released a Health Technology Assessment for early diagnosis of cervical cancer. There is sufficient evidence that suggests that screening leads to a reduction in the occurrence of cervical cancer cases with a decrease in cancer deaths. It also concludes that among various screening strategies, VIA every 5 year is the most cost-effective screening method in the context of India [5]. In India, the incidence of cervical cancer significantly rises around the age of 45 years and peaks at 55 years of age. The natural history of the disease suggests that early diagnosis should initially target those women who have a higher prevalence of high-grade precancerous lesions (Cervical Intraepithelial Neoplasia 2/3)—women mostly in their 30 s and 40 s [6].
The most effective prevention strategy for cervical cancer is the systematic screening of women through an organized program along with treatment and follow-up of the screen-detected precursor lesions. The focus on the detection and prevention of cervical cancer must be emphasized in a highly populated country like India [6].
World Health Organization (WHO) Guidelines
WHO South-East Asia Region developed a strategic framework for cervical cancer control in the region. The framework recommends a multipronged approach towards comprehensive cervical cancer control. The HPV vaccine is one of the recommended interventions for girls aged 9–13 years. for primary prevention. Cervical cancer screening programs using cost-effective tests can be implemented for the early detection of pre-cancerous conditions and cancers. Health systems need to be strengthened for preventive, curative and palliative care services for cancers [7]. Management algorithms for screen‐positive women in cervical cancer prevention programs have undergone substantial changes in recent years. Recently, the WHO headquarter released its global strategy to accelerate the elimination of cervical cancer in November 2020 which outlined three key steps: vaccination, screening and treatment [8]. Meeting the following targets by 2030 will hopefully place countries on the path toward elimination: 90% of girls fully vaccinated with the HPV vaccine by 15 years of age, 70% of women screened using a high-performance test by age 35 and again by 45 as well as 90% of women identified with cervical disease receive treatment (90% of women with pre-cancer treated and 90% of women with invasive cancer managed). The strategy also stresses that investing in the interventions to meet these targets can generate substantial economic and societal returns [9].
Evolution of Cancer Control Programs in India
The National Cancer Control Programme (NCCP) was first launched in 1975, with priorities given for equipping the premier cancer hospital/institutions. Central assistance at the rate of Rs. 2.50 lakhs was given to each cancer institution for the purchase of cobalt machines for radiotherapy. In 1984, the strategy was revised and stress was laid on primary prevention and early detection of cancer cases. In 1990–91, the District Cancer Control Programme was started in selected districts (near the medical college hospitals). And during the 2000s, it was further modified. In 2004, evaluation of NCCP was done and the program was further revised [10]. Cancer control is now a part of the National Programme for Prevention and Control of Cancer, Diabetes, Cardiovascular Diseases and Stroke (NPCDCS) program which was launched in 2010 to prevent and control major non-communicable diseases [11]. Unfortunately, despite these programs being in place for many years, the cancer burden in real terms is mounting, as evident from the data coming from cancer registries across Indian states.
Journey of Formulation of India’s Cervical Cancer Guidelines
Recognising the key role that effective early detection and screening programs could have in reducing the cancer burden, the Indian Council of Medical Research’s (ICMR) Institute for Cytology and Preventive Oncology (ICPO), now rechristened as ICMR-National Institute of Cancer Prevention and Research (NICPR) at Noida, in collaboration with the US National Cancer Institute—Center for Global Health, held a 2-day brainstorming workshop in 2013 to summarise relevant evidence and feasible options for screening and early detection of common cancers in India which was attended by national and international experts in the subject. Keeping in view that in most developing countries, due to the lack of necessary manpower, infrastructure and quality control, high-quality cytology screening may not be feasible for wide-scale implementation of the cervical cancer screening program [12], it was recommended that visual screening tests such as VIA/VILI could be adopted till a low-cost reliable HPV test became available in India. These techniques could be conducted by trained doctors and paramedical staff, with adequate training and quality assurance, and would also have the advantage of on-site screen and treatment of low degrees of abnormalities detected. The report of the workshop with recommendations of the experts was submitted to ICMR and was developed into a major international publication in 2015 [13].
Another factor that needed due consideration was that screening at the population level, when planned and organized, can greatly benefit the population, while disorganized screening can increase costs and reduce benefits. Hence, the International Cancer Screening Network (ICSN) also convened a meeting to share lessons, experience, and evidence regarding cancer screening in countries with established organized screening programs. The first regional consultation of the ICSN was held in Agartala (Sept 5–7, 2016) and recommendations were published and submitted to the relevant stakeholders [14].
The Prime Minister’s office took note of this development and emphasised the importance of a quick release of the necessary guidelines [15]. Later the recommendations of this meeting were followed by further deliberations of national experts in two more stakeholder workshops held by ICPO in conjunction with WHO India and the consensus findings were submitted to the Ministry of Health and Family Welfare (MoHFW), which constituted a high-powered expert panel to finalise the modalities of early diagnosis of not only cervical cancer but also breast and oral cancers and the Operational Framework for Management of Common Cancers was prepared and released in Tirupati in 2016 by MoHFW.
On the release of the guidelines the key contributors, the Minister of Health promised that the Initial implementation of the screening program across 100 districts will provide data for wider implementation across India. This will be accompanied by awareness campaigns in the community. The roadblocks, if any, would be removed, and the lessons learned may result in course corrections wherever essential [16].
Cervical Cancer Control Accompanied by HPV Vaccination
Globally, it is now widely accepted that vaccination against high-risk strains of the human papillomavirus (HPV) is a safe and effective means of primary prevention of cervical cancer. Although the HPV vaccination was introduced in India in 2008, it is yet to be included in the universal immunization program in India [17]. A vaccine delivery and demonstration project led by an international non-profit organization, PATH, was started in 2009 in Andhra Pradesh and Gujarat but had to be suspended in 2010 as a result of public concern, allegedly arising from the deaths of seven girls who received HPV vaccine [18]. In 2016, a multidisciplinary Expert Group constituted by the Secretary, Department of Health Research and Director-General, Indian Council of Medical Research, Ministry of Health and Family Welfare, Government of India, reviewed the available evidence globally regarding immunogenicity and efficacy, adverse effects, and cost-effectiveness of the HPV vaccine. In addition, the burden of HPV infection and the status of the HPV vaccine in India were also reviewed. The Group discussed the available guidelines and recommendations of WHO for the introduction of HPV vaccine at the country level and came up with the recommendation that adolescent girls 9–13 years should be vaccinated with two doses of the HPV vaccine [19]. They recommended that the health system capacity should be assessed before introduction to ensure effective implementation and a reliable system should be established to monitor the adverse events. Vaccine coverage should be monitored within the program framework and cervical cancer trends need to be monitored through a network of cancer registries [19].
Once the recommendations were received, a first of its kind HPV vaccination program for school children was launched in New Delhi, on the occasion of National Cancer Awareness Day (November 7, 2016) which vaccinated nearly 1200 girls [20]. It was supposed to be expanded to cover 250,000 girls per annum. Simultaneously, the Government of Punjab initiated a similar campaign and succeeded in vaccinating young girls with 97.5% and 98.5% coverage initially [21]. The Government of Sikkim also introduced HPV vaccination along similar lines and achieved high coverage and safety in 2018 with spectacular success [22]. The key barriers encountered in the implementation of HPV vaccine rollout were sociocultural, health systems, and financial barriers as well as consistency in policy with change in governance [23]. It is suggested that a policy of screening of the mother and vaccinating the accompanying girl child (if of appropriate age) could be a viable approach.
Training of Health Care Workers
As per the Operational guidelines, the existing health care providers (HCPs) at various facilities were supposed to roll out the population-based cancer screening in the country. It was felt evident that the framework required a team representing a range of relevant medical specialties at all levels of care [24]. However, the existing HCPs lacked the skills and were not trained in cancer screening. Considering the size of the country and the number of personnel involved, it was neither feasible nor economically viable to provide in-person training for all cadres of HCPs [25]. To support the implementation of the cervical cancer screening program, the ICMR-NICPR was designated as a training hub for the Project ECHO (Extension for Community Healthcare Outcomes) model for training health care providers in cancer screening following which a study was conducted which reported the effectiveness of the training program in reaching primary care physicians/other HCPs across the country and improving their knowledge and skills related to screening for breast, oral, and cervical cancer. The ECHO model provided a cost-effective way to exponentially expand the capacity to mentor and train these HCPs in cancer screening best practices. ECHO used widely available video-conferencing technology, didactic presentations and case-based learning techniques to mentor and support HCPs to implement best practices in the field [26]. The author’s group earlier reported on the effectiveness of the innovative feasible approach of ‘satellite clinic’ which could enable tertiary hospitals to contribute to cancer prevention, without compromising their primary mandate to provide treatment [27]. In addition to online training, hard copies of training manuals were also designed by the MoHFW for doctors and paramedical workers.
The preparedness of the Indian healthcare system for implementing large-scale cervical cancer screening is also a concern. Dhillon et al. reported in their study that overall, readiness scores were low for cervical cancer screening. At Sub Health Centres, the lowest scores were observed in 'infrastructure’ (0.55) and 'infection prevention (0.44), while Primary Health Centres (PHCs) had low ‘potential staffing’ scores (0.50) due to limited manpower to diagnose and treat (cryotherapy) potential cases. Scores were higher for tiers conducting diagnostic work-up and treatment/referral. Infrastructure and staffing were large barriers to screening at PHCs, which are crucial for the referral of high-risk patients [28].
Practical on-Field Implementation of the Guidelines and Challenges
Apart from the infrastructural barriers, a recent study reported that poor knowledge about cervical cancer, benefits of screening service availability, as well as a general sense of well-being, embarrassment or anxiety related to the screening procedure, fear of being judged for lack of modesty, and stigma were common barriers to screening uptake [29].
Computer software was also released for recording and follow-up of the individuals screened to ensure prompt real-time recording of data and minimizing loss to follow-up. The cervical cancer screening was bundled with breast and oral cancer screening as part of the NPCDCS program as a comprehensive package to be delivered at the Wellness centers and covered by the Ayushman Bharat Scheme of the MoHFW. At the time of writing, 70,000+ wellness centers catered to 41.35 crore people and 917 hospitals impanelled under the scheme for oncology care, catering to slightly less than 2 lakh beneficiaries. These 900+ hospitals include quite a range of hospitals from multi-modal treatment facilities to stand-alone nursing homes. These facilities are provided by the 174 oncology packages in the scheme [26, 30].
Evaluation
Van Dyne et al. [31] conducted a study to establish baseline cervical cancer screening coverage in India, which reported only 29.8% of women reported were being screened and that the prevalence of screening was higher in the urban areas. It was also reported that the diagnosis of carcinoma cervix was usually based on opportunistic screening or after the onset of the symptoms [6].
After the release of the Operational Guidelines, several barriers were found along the road of implementation of the cervical cancer screening guidelines. Evaluation of the implementation of Population‐based Cancer Screening Program as a Pilot Study was conducted at Silchar, Assam by the authors’ group in 2018 which highlighted the lack of human resources, overburdening of the existing staff, and difficulty in motivating community for screening as the top 3 challenges, as observed by the healthcare providers involved in the implementation [32].
A recent study, in 2020, reported that according to the NFHS (National Family Health Survey) report, 22% of women have undergone a cervical examination in India and the majority of the districts fall in the range of 10–20% [33] whereas as per 2021 India factsheet, the coverage of Cervical cancer screening coverage, % (age and screening interval, reference) has been reported to be only 3.1% [34]. Another study conducted in 2020, in south India revealed that only 14.3% had at least one lifetime pelvic exam and 7.1% had undergone cervical cancer screening [35]. The higher percentage reported here maybe due to the fact that cervical cancer screening may have been perceived by responders as speculum exam or even a pelvic exam of any sort, most likely related to antenatal and pregnancy care. NFHS-5 data is also in line with the WHO data, where percentage of women ever undergone cervical cancer screening in India is 1.9% (2.2% urban and 1.7% rural) [36]. Andhra Pradesh, Bihar, Jammu and Kashmir, Telangana, and West Bengal have more rural women participating in cervical cancer screening than those in urban areas. The women living in the urban regions of Mizoram, Himachal Pradesh, Kerala, and Maharashtra have a significant number of women undergoing a screening test for cervical cancer. The practice of cervical cancer screening is close to insignificant in Nagaland, Ladakh, and Gujarat [37].
Even though the alternative screening and management algorithms have simplified the logistics of cervical cancer screening, implementation of the programs in the country is limited for several reasons (Fig. 1). Among these are the needs to optimize fiscal and human resources, mobilize and educate communities, organize services that meet women's needs and preferences, and strengthen health information systems to track screen‐positive women for follow‐up. A truly point‐of‐care and affordable HPV test is still elusive [8, 38].

Source: Operational Framework for Management of Common Cancers)
Screening and management algorithm (
Way Forward Keeping COVID-19 in Mind
There are still a lot of unanswered questions and challenges ahead, viz. determining appropriate cost-effective and point of care screening strategy, deciding intervals of screening, motivation of women to come forward for screening with optimal utilization and augmentation of existing health care infrastructure including diagnostic and treatment facilities [39].
India needs to develop health system capacity to ensure efficient cervical cancer screening program and community-level efforts to improve knowledge about cervical cancer and screening programs via enhancing community participation which can only be achieved by creating a workforce of health professionals and paramedical workers with screening awareness [40].
A recent review found that community healthcare workers (CHWs) can improve community awareness and help to carry out cancer screening and follow-up. Adopting participatory approaches in CHW interventions would enhance acceptability [41].
A recent study by Ginsburg et al. reported that HPV has also caused a slow-moving health crisis akin to a pandemic that is hiding in plain sight. Immediate, coordinated action is needed to bring together global partners into collaboration with private-sector manufacturers of vaccines, diagnostics, and cancer treatments. This is critical for facilitating effective intervention to prevent nearly 350,000 cervical cancer deaths in 2021 and the future [42].
The pandemic has deeply affected all levels of our lives. New vulnerable groups and inequalities have emerged that require recognition and action. To prevent long-term increases in the cervical cancer burden due to the COVID-19 pandemic, it is crucial that organized screening is maintained and monitored in settings where it can be safely and comprehensively provided [43]. Otherwise, this disruption to cancer screening services may have a significant impact on patients, health care practitioners, and health systems [44]. Apart from early detection and screening, the treatment aspect has also been compromised and needs due attention (Fig. 2).

Source: Ref. [31]: Van Dyne EA, Hallowell BD, Saraiya M, et al. Establishing Baseline Cervical Cancer Screening Coverage—India, 2015–2016. MMWR Morb Mortal Wkly Rep 2019;68:14–19. https://doi.org/10.15585/mmwr.mm6801a4
Prevalence of cervical cancer screening among women aged 30–49 years, by district—National Family Health Survey-4, India, 2015–2016.
Recommendations
We have come a long way since the development of the Operational Guidelines for the management of common cancers in India. However, the on-field implementation of early diagnosis of cervical cancer on a national scale is still a herculean task. ECHO training programs and satellite clinic models do help, however, a more robust commitment from the Government is required for the full-fledged implementation of these guidelines, with time-to-time modifications, to yield lasting fruits in the formation of an independent dedicated cell entrusted with the job of Monitoring and Evaluation the NPCDCS program and coordinating with the various stakeholders, including the various state players. With health being a state subject in India, a concerted approach for the implementation of state-wide cervical cancer control and HPV vaccination will hopefully bring fruitful results, as evident from the success of the Sikkim model [45].
References
International Agency for Research on Cancer. Globocan; 2020. https://gco.iarc.fr/. Accessed 29 April 2021.
India State-Level Disease Burden Initiative Cancer Collaborators. The burden of cancers and their variations across the states of India: the Global Burden of Disease Study 1990–2016. Lancet Oncol. 2018;19(10):1289–1306. https://doi.org/10.1016/S1470-2045(18)30447-9. Epub 2018 Sep 12. Erratum in: Lancet Oncol. 2018 Oct 3;: PMID: 30219626; PMCID: PMC6167407.
Srivastava AN, Misra JS, Srivastava S, Das BC, Gupta S. Cervical cancer screening in rural India: status and current concepts. Indian J Med Res. 2018;148(6):687–96.
Marima R, Hull R, Mathabe K, Setlai B, Batra J, Sartor O, Mehrotra R, Dlamini Z. Cervical cancer in low and middle-income countries. Oncol Lett. 2020;20(3):2058–74. https://doi.org/10.3892/ol.2020.11754.
Health Technology Assessment of Strategies for Cervical Cancer Screening in India. School of Public Health Postgraduate Institute of Medical Education and Research Chandigarh (India). https://dhr.gov.in/sites/default/files/HTA_CaCx%20Screening%20in%20India.pdf. Accessed 29 April 2021.
Consensus Document for the Management of Cancer Cervix. Indian Council of Medical Research. 2016. https://main.icmr.nic.in/sites/default/files/reports/Cervix%20Cancer.pdf. Accessed 29 April 2021.
World Health Organization, Regional Office for South-East Asia. Strategic framework for the comprehensive control of cancer cervix in South-East Asia Region. New Delhi: WHO; 2015.
Basu P, Meheus F, Chami Y, Hariprasad R, Zhao F, Sankaranarayanan R. Management algorithms for cervical cancer screening and precancer treatment for resource-limited settings. Int J Gynaecol Obstet. 2017;138(Suppl 1):26–32. https://doi.org/10.1002/ijgo.12183 (PMID: 28691336).
A cervical cancer-free future: First-ever global commitment to eliminate a cancer. WHO. https://www.who.int/news/item/17-11-2020-a-cervical-cancer-free-future-first-ever-global-commitment-to-eliminate-a-cancer. Accessed 29 April 2021.
National Cancer Control Program. Ministry of Health and Family Welfare. https://main.mohfw.gov.in/sites/default/files/1493693747note_0.pdf. Accessed 29 April 2021.
National Programme for Prevention and Control of Cancer, Diabetes, Cardiovascular Diseases and Stroke (NPCDCS). National Health Mission. https://nhm.gov.in/images/pdf/NPCDCS.pdf. Accessed 29 April 2021.
Bobdey S, Sathwara J, Jain A, Balasubramaniam G. Burden of cervical cancer and role of screening in India. Indian J Med Paediatr Oncol. 2016;37(4):278–85. https://doi.org/10.4103/0971-5851.195751.
Rajaraman P, Anderson BO, Basu P, Belinson JL, Cruz AD, Dhillon PK, Gupta P, Jawahar TS, Joshi N, Kailash U, Kapambwe S, Katoch VM, Krishnan S, Panda D, Sankaranarayanan R, Selvam JM, Shah KV, Shastri S, Shridhar K, Siddiqi M, Sivaram S, Seth T, Srivastava A, Trimble E, Mehrotra R. Recommendations for screening and early detection of common cancers in India. Lancet Oncol. 2015;16(7):e352–61. https://doi.org/10.1016/S1470-2045(15)00078-9 (PMID: 26149887).
Sivaram S, Majumdar G, Perin D, Nessa A, Broeders M, Lynge E, Saraiya M, Segnan N, Sankaranarayanan R, Rajaraman P, Trimble E, Taplin S, Rath GK, Mehrotra R. Population-based cancer screening programs in low-income and middle-income countries: regional consultation of the International Cancer Screening Network in India. Lancet Oncol. 2018;19(2):e113–22. https://doi.org/10.1016/S1470-2045(18)30003-2 (PMID: 29413465; PMCID: PMC5835355).
Ghosh A. PMO sets 3-month deadline for the cancer screening framework. https://indianexpress.com/article/india/india-news-india/pmo-sets-3-month-deadline-for-cancer-screening-framework/. Accessed 6 May 2021.
Bagchi S. India launches a plan for the national cancer screening program. BMJ. 2016;17(355): i5574. https://doi.org/10.1136/bmj.i5574 (PMID: 27754831).
Mehrotra R, Hariprasad R, Rajaraman P, Mahajan V, Grover R, Kaur P, Swaminathan S. Stemming the wave of cervical cancer: human papillomavirus vaccine introduction in India. J Glob Oncol. 2018; 4:1–4. https://doi.org/10.1200/JGO.17.00030. Epub 2017 Sep 8. PMID: 30241163; PMCID: PMC6180758.
Lamontagne DS, Sherris JD. Addressing questions about the HPV vaccine project in India. Lancet Oncol. 2013;14:e492.
Kaur P, Mehrotra R, Rengaswamy S, Kaur T, Hariprasad R, Mehendale SM, Rajaraman P, Rath GK, Bhatla N, Krishnan S, Nayyar A, Swaminathan S. Human papillomavirus vaccine for cancer cervix prevention: rationale and recommendations for implementation in India. Indian J Med Res. 2017;146:153–7.
Chatterjee P: Delhi first state to launch the HPV vaccine as public health program in schools. http://indianexpress.com/article/cities/delhi/delhi-first-state-to-launch-hpv-vaccine-as-public-healthprogramme-in-schools/. Accessed 29 April 2021.
WHO: Punjab launches HPV vaccine with WHO support. http://www.searo.who.int/india/mediacentre/events/2016/Punjab_HPV_vaccine/en/. Accessed 29 April 2021.
Sankaranarayanan R, Basu P, Kaur P, Bhaskar R, Singh GB, Denzongpa P, Grover RK, Sebastian P, Saikia T, Oswal K, Kanodia R, Dsouza A, Mehrotra R, Rath GK, Jaggi V, Kashyap S, Kataria I, Hariprasad R, Sasieni P, Bhatla N, Rajaraman P, Trimble EL, Swaminathan S, Purushotham A. Current status of HPV vaccination introduction in India’s cervical cancer prevention efforts. Lancet Oncol. 2019. PMID:31674322.
Wigle J, Coast E, Watson-Jones D. Human papillomavirus (HPV) vaccine implementation in low and middle-income countries (LMICs): health system experiences and prospects. Vaccine. 2013;31:3811–7.
Maggi R. Assessing breast and cervical cancer in India: a literature review; 2018.
Hariprasad R, Babu R, Arora S, Mehrotra R. Capacity building in cancer screening using ECHO (extension for community healthcare outcomes): innovative and cost-effective model. J Glob Oncol. 2018;4(Supplement 2):160s–160s.
Press Trust of India. 70,000 Ayushman Bharat-Health and Wellness Centres operationalized: Govt. https://www.business-standard.com/article/current-affairs/70-000-ayushman-bharat-health-and-wellness-centres-operationalised-govt-121032100276_1.html. Accessed 29 April 2021.
Dhanasekaran K, Verma C, Kumar V, Hariprasad R, Gupta R, Gupta S, Mehrotra R. Cervical cancer screening services at tertiary healthcare facility: an alternative approach. Asian Pac J Cancer Prev. 2019;20(4):1265–9. https://doi.org/10.31557/APJCP.2019.20.4.1265.PMID:31030504;PMCID:PMC6948876.
Dhillon PK, Hallowell B, Agrawal S, Ghosh A, Yadav A, Van Dyne E, Senkomago V, Patel SA, Saraf D, Hariprasad R, Dumka N, Mehrotra R, Saraiya M. Is India’s Public health care system prepared for cervical cancer screening: evaluating facility readiness from the fourth round of the district level household and facility survey (DLHS-4). Prev Med. 2020. PMID: 32473272.
Dsouza JP, Van Broucke S, Pattanshetty S, Dhoore W (2020) Exploring the Barriers to Cervical Cancer Screening through the Lens of Implementers and Beneficiaries of the National Screening Program: A Multi-Contextual Study. Asian Pac J Cancer Prev 21(8):2209–2215. Doi: https://doi.org/10.31557/APJCP.2020.21.8.2209
Kaur S, Jain N, Bhatnagar PC. Early trends from Utilization of Oncology services: insights from Ayushman Bharat Pradhan Mantri Jan Arogya Yojana (PM-JAY). Working Paper 004. https://www.pmjay.gov.in/sites/default/files/2019-11/Working%20paper-4%20%281%29.pdf.
Van Dyne EA, Hallowell B, Saraiya M, Senkomago V, Patel S, Agrawal S, Ghosh A, Saraf D, Mehrotra R, Dhillon P. Establishing baseline cervical cancer screening coverage—India 2015–2016. Morb Mortal Wkly Rep; 2019. PMID: 30629571.
Kedar A, Kannan R, Mehrotra R, Hariprasad R. Implementation of population-based cancer screening program in a pilot study from India: views from health personnel. Indian J Community Med. 2019;44(1):68–70. https://doi.org/10.4103/ijcm.IJCM_268_18 (PMID: 30983720; PMCID: PMC6437804).
Mishra R. An epidemiological study of cervical and breast screening in India: district-level analysis. BMC Womens Health. 2020;20:225. https://doi.org/10.1186/s12905-020-01083-6.
Human Papillomavirus and Related Diseases Report. India. HPV Information centre. 2021. https://hpvcentre.net/statistics/reports/IND_FS.pdf.
Reichheld A, Mukherjee PK, Rahman SM, David KV, Pricilla RA. Prevalence of cervical cancer screening and awareness among women in an urban community in South India—a cross-sectional study. Ann Glob Health. 2020;86(1):30. https://doi.org/10.5334/aogh.2735.
National Family Health Survey. Government of India. http://rchiips.org/nfhs/factsheet_NFHS-5.shtml.
Gunnal GS, Guha S, Akhil PM. How do Indian states handle cancer screening among women? NFHS-5 data reveals. 2020. Down to Earth. https://www.downtoearth.org.in/blog/health/how-do-indian-states-handle-cancer-screening-among-women-nfhs-5-data-reveals-74666.
Hariprasad R, Tulsyan S, Babu R, Dhanasekaran K, Thakur N, Hussain S, Tripathi R, Sreenivas V, Sharma S, Sriram L, Singh S, Mehrotra R. Evaluation of a chip-based, point-of-care, portable, real-time micro PCR analyzer for the detection of high-risk human papillomavirus in uterine cervix in India. JCO J Glob Oncol. 2020. PMID: 32697666.
Gupta R, Gupta S, Mehrotra R, Sodhani P. Cervical cancer screening in resource-constrained countries: current status and future directions. Asian Pac J Cancer Prev. 2017. PMID 28669152.
Vora KS, Saiyed S. Cervical cancer screening in India: need of the hour. Cancer Res Stat Treat. 2020;3:796–7.
O’Donovan J, O’Donovan C, Nagraj S. The role of community health workers in cervical cancer screening in low-income and middle-income countries: a systematic scoping review of the literature. BMJ Glob Health. 2019;4:e001452.
Ginsburg O, Basu P, Kapambwe S, et al. Eliminating cervical cancer in the COVID-19 era. Nat Cancer. 2021;2:133–4. https://doi.org/10.1038/s43018-021-00178-9.
Ivanuš U, Jerman T, Gašper Oblak U, Meglič L, Florjančič M, Strojan Fležar M, et al. The impact of the COVID-19 pandemic on organizedorganised cervical cancer screening: the first results of the Slovenian cervical screening programprogramme and registry. Lancet Reg Health Europe. 2021;5:100101.
Cancino RS, Su Z, Mesa R, Tomlinson GE, Wang J. The impact of COVID-19 on cancer screening: challenges and opportunities. JMIR Cancer. 2020;6(2): e21697. https://doi.org/10.2196/21697.
Salaria S. Focus on Sikkim model to check cervical cancer. 2018. https://timesofindia.indiatimes.com/city/noida/focus-on-sikkim-model-to-check-cervical-cancer/articleshow/65600408.cms. Accessed 29 April 2021.
Funding
Nil.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Nil.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Mehrotra, R., Yadav, K. Cervical Cancer: Formulation and Implementation of Govt of India Guidelines for Screening and Management. Indian J Gynecol Oncolog 20, 4 (2022). https://doi.org/10.1007/s40944-021-00602-z
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1007/s40944-021-00602-z