
Abstract
Due to the increasing occurrence of renal cell carcinoma (RCC) in the general population and the high prevalence of chronic kidney disease among cancer patients, many people with a previous RCC may eventually require renal replacement therapy including kidney transplantation. They should accordingly be evaluated to assess their life expectancy and the risk that the chronic immunosuppressive therapy needed after grafting might impair their long-term outcome. Current guidelines on listing patients for renal transplantation suggest that no delay is required for subjects with small or incidentally discovered RCC, while the recommendations for patients who have been treated for a symptomatic RCC or for those with large or invasive tumours are conflicting. The controversial results reported by even recent studies focusing on the cancer risk in kidney graft recipients with a prior history of malignancy do not help to clarify the doubts arising in everyday clinical practice. Several tools, including integrated scoring systems, are currently available to assess the prognosis of patients with a previous RCC and, although they have not been validated in subjects receiving long-term immunosuppressive drugs, they can be used to identify patients suitable to be listed for grafting. Among these, the Leibovich score is currently the most widely used as it has proved simple and reliable enough and helps categorize renal transplant candidates. According to this system, subjects with a score from 0 to 2 are at low risk and may be listed without delay, while those with a score of 6 or higher should be excluded from grafting. In addition, other factors have an established positive prognostic value, including chromophobe or clear cell papillary tumour, or G1 grade cancer; on the contrary, medullary or Bellini’s duct carcinoma or those with sarcomatoid dedifferentiation at histological examination should be excluded. All other patients would be better submitted to careful individual evaluation by an Oncologist before being listed for renal transplantation, pending studies specifically focusing on cancer risk evaluation in people already treated for malignancy receiving long-term immunosuppressive therapy.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The incidence of renal cell carcinoma (RCC) in the general population has progressively increased in the last few years and at present it accounts for approximately 2–3% of all adult malignancies, being the 7th most common cancer in men and the 9th most common cancer in women [1].
According to the American Urological Association guidelines [2] as well as the European Association of Urology (EAU) guidelines [3], nephron-sparing surgery is at present the standard of care for T1a and most T1b lesions (i.e. lesions confined to the kidney that are no larger than 4 cm or 7 cm, respectively), with an A and B grade of recommendation, respectively, while in elderly and/or comorbid patients with small renal masses and limited life expectancy, active surveillance, radiofrequency ablation and cryotherapy can be considered (grade C) [3, 4]. Radical nephrectomy is the preferred option for T2 tumours exceeding 7 cm, and for locally advanced (T3 and T4) lesions (grade B).
Given the high prevalence of chronic kidney disease among cancer patients [5], and as a result of surgery, some patients require dialysis treatment and, if they have no comorbid conditions, might be considered for transplantation listing, provided the cancer has been cured.
However, considering that transplanted patients themselves have an increased risk of cancer when compared with the general population, mainly due to prolonged immunosuppressive therapy [6], they should be evaluated carefully before listing in order to avoid, first of all, the risk of worsening the patient prognosis instead of improving it, and secondly the use of a scarce resource, such as donated organs, for subjects with a limited life span.
Current guidelines
Several guidelines have already addressed this problem suggesting a minimum waiting period between successful treatment of malignancy and transplantation pending achievement of the highest possible likelihood of 5-year patient survival. Decision-making will still need to be individualized, accounting for the features of previous malignancy in individual patients and their clinical conditions.
Most international guidelines draw their data from the seminal publications by Penn and his collaborators [7]. These articles summarize the outcomes of patients with a prior malignancy undergoing renal transplantation, who were voluntarily enrolled in the Cincinnati Tumour Transplant Registry. Thus, they do not include all patients undergoing transplantation with a history of prior malignancy. Despite its imperfections, this Registry analysis remains the most informative and essentially the only published series of any substance in the literature. The concept of waiting times post successful treatment of a malignancy and prior to transplantation is based on the observation that cancer recurrence becomes less likely with an increasing disease-free interval post-treatment. Penn et al. reported 54% of recurrences in patients who received a graft within 2 years of treatment for malignancy, while 33% were documented in patients transplanted between 2 and 5 years, and only 13% among those treated more than 5 years before grafting [7].
Only one out of 72 patients with a previous incidentally found RCC showed cancer recurrence after transplantation and no recurrence was reported in patients transplanted more than 5 years after cancer treatment. On the contrary, among 222 patients with symptomatic RCC the recurrence rate was 27%, and the large majority of patients with recurrence (93%) had received a transplant less than 5 years after cancer removal. Moreover, recurrence of RCC after grafting was associated with increased mortality, and 49 (80%) deaths occurred in 61 patients with recurrence.
After these observations Penn et al. suggested that a 2-year waiting period is unnecessary for patients with an incidentally discovered RCC unless the tumour is large (i.e. > 5 cm) or infiltrates the kidney capsule, while a 5-year recurrence-free interval is appropriate for patients with symptomatic RCCs exceeding 5 cm. It is important to highlight that the presence of symptoms is often, but not always, related to the local extension of the neoplasm; a small mass could induce haematuria or not, depending on its position, central or peripheral. Thus, it is questionable that the extent of the waiting time should be determined by the presence or absence of symptoms.
However, the KHA-CARI Guidelines suggest that the evaluation include TNM staging (Tumour, regional lymphNodes, distant Metastases) and a histological examination to identify lesions with a higher likelihood of recurrence [8].
On the other hand, no delay in listing for transplantation patients with small, incidentally discovered tumours is recommended by current guidelines [9,10,11,12,13] (Table 1). On the contrary, current guideline recommendations for patients who have been treated for a symptomatic RCC are variable, ranging from 2 to 5 years’ waiting time, since they apply to subjects with large or invasive tumours, which are considered a contraindication to renal transplantation by some guidelines but accepted by others (Table 1).
Cancer risk in kidney transplanted patients with a prior history of malignancy
Generally speaking, patients with a prior history of malignancy are known to have an increased risk of cancer-specific mortality after renal transplantation although the data hitherto reported are rather conflicting, even when derived from studies involving a large number of subjects (Table 2).
Two large registry data analyses have examined the risk of any malignancy in patients after renal transplantation [14, 15]. It is of interest that patients with a prior history of malignancy are at increased risk of developing a de novo malignancy after transplantation but this risk exceeds that of recurrence of the original malignancy. An analysis of the Australia and New Zealand Dialysis and Transplant registry (ANZDATA) [14] reported an unadjusted hazard ratio of 2.08 (1.54–2.8) and an adjusted hazard ratio of 1.4 (1.03–1.89) for de novo malignancy in patients with a prior history of cancer, as compared to those without prior malignancy. Similarly, on analyzing data from the Organ Procurement and Transplantation Network (OPTN), Kauffman et al. reported a de novo malignancy incidence of 7.8% in subjects with a prior history of malignancy vs. 2.8% in those without [15]. In the same study, the rate of recurrence of the original malignancy was 2.3%. Their data do not appear to be adjusted for recipient age.
In regard to the recurrence of a previous cancer, a more recent study analyzed 21,415 patients transplanted in Australia and New Zealand between 1965 and 2012 where 651 (3%) had a history of cancer before transplantation [16]. Only 23 of them (3.5%) developed cancer recurrence after transplantation; since seven of these had a malignancy of the urinary tract and three died during follow-up, it would seem that patients with a cancer history before transplantation may not be at a greater risk of death. From investigations in a Swedish cohort of 10,448 patients transplanted with a solid organ between 1970 and 2008 [17], 416 of whom (4%) had a cancer history before grafting—kidney and urothelial cell cancer being the most common types of cancer (21.9%), it emerged that among 66 out of 416 who died of cancer during follow-up, 39 (9.4%) died of the same cancer type as diagnosed before transplantation. In this cohort multivariate analysis revealed a more than threefold increased rate of dying from cancer compared to other transplanted patients. However, patients who suffered from kidney or urothelial cell cancer before transplantation proved to have a fivefold increased relative risk of dying of cancer [17].
On the other hand, a study carried out in 19,103 patients who received a kidney transplant in England between 2001 and 2012 reported that subjects with a pre-transplant history of cancer had a significantly higher risk of dying from malignancy as compared with those who did not and, interestingly, in this sub-group of patients, over half of all malignancy-related deaths were renal in origin [18]. This study confirmed the finding of an earlier study in 164,078 first kidney transplant recipients registered in the United States Renal Data System between 1990 and 2004, namely that a prior cancer history is an independent risk factor for cancer-related death after transplantation [19].
The controversial results of even recent studies definitely challenge the waiting time suggested by different authors before listing a patient who has suffered from cancer.
Dahle et al. analyzed the Norwegian registry—where, in accordance with local policy, patients with a cancer history were listed 1 year on from cancer treatment—and failed to find a significant difference in overall survival between patients with or without a previous cancer, although cancer-related mortality was increased in the former group, particularly in the first 5 years after grafting [20]. Since they found no association between the waiting period and recurrent cancer mortality, they proposed shortening the waiting time currently suggested by the guidelines [20]. Similarly, Nguyen et al. investigated the outcome of patients with end-stage renal disease (ESRD) related to renal malignancy who received a graft reported in the United States Renal Data System (USRDS), and concluded that cancer-specific mortality was not affected by waiting-time duration, while the overall survival rate was better in patients with a shorter waiting time [21].
Of course, discrepancies in the reported studies may be due to several factors, including previous modes of cancer treatment, accuracy of patient follow-up, investigation of cancer recurrence before listing, and the criteria adopted in listing patients for transplantation. All these biases are even more relevant when dealing with studies based on registry data or metanalyses. However, taken together, they underline the need for a more precise approach to the problem allowing for planning the waiting time before listing according to the clinical setting of individual patients.
Criteria for listing patients with previous renal cancer
The issue of listing for kidney transplantation subjects with previous RCC is far from a trivial problem in view of the implicit question underlying: when should a cancer patient be considered cured? In other words, are we able to precisely quantify the risk of relapse in a patient who has been radically operated on for a given tumour (in this case RCC)? This is further complicated by the fact that no specific data are available for transplanted patients on immunosuppressive therapy.
So far, the decision has been based on current guidelines which are mainly derived from observations coming from the Cincinnati Registry, which essentially considers the type of tumour and the time elapsed between treatment and kidney transplantation as the main criteria. Certainly there is not enough evidence to support a fixed waiting period before transplantation for these patients, and there is need for a different approach to reach a more accurate evaluation of the risk of recurrence after transplantation in individual patients. However, when restricting our quest to kidney cancer, some useful tools are currently available to help us decide, including histological features and new staging systems, briefly reviewed below.
TNM (tumour, regional lymphnodes, distant metastases) staging
Correct tumour staging—using the latest version [22] of the widely applied and easy-to-use TNM system—is the first tool to predict the risk of recurrence in a patient treated with radical nephrectomy for a kidney tumour. According to the SATURN project [23], which analysed more than 5000 cases of kidney cancer that underwent surgery during the period 1997–2007 in 16 Italian Centres, the probability of survival at 5 years is inversely related to tumour size: it was respectively 94.9% in the case of pT1a tumours, 92.6% in pT1b tumours, 85.4% in pT2a tumours, 70% in pT2b tumours, 64.7% in pT3a tumours, 54.7% in pT3b tumours, 17.9% in pT3c tumours, and finally 27.1% in pT4 tumours.
Other parameters, not included in the TNM system, have been proposed over time to play a negative prognostic role, including the infiltration of the urinary tract and infiltration of the kidney sinus [24]. As expected, the spread of the tumour to regional lymphnodes is associated with a significantly worse survival, as compared to organ-confined disease, as again demonstrated by the SATURN project data [23]. Of course, metastatic kidney cancer patients have the worst prognosis and even though patients who are rendered metastasis-free by surgery are known to have a better prognosis compared to those who did not undergo metastasis removal, they should be regarded as incurable, and should not be considered for organ transplantation.
Histology
Histology is another important prognostic feature. Clear cell RCCs, by far the commonest histotype of kidney carcinoma, have a cause-specific survival significantly worse than papillary and chromophobe tumours or multilocular cystic RCC; furthermore, among papillary renal cell carcinomas, type I is characterized by a slightly better prognosis than type II. Finally, chromophobe carcinomas are considered to be particularly indolent, even though no significant differences in terms of prognosis have been reported compared to papillary tumours [25, 26].
As a whole, the percentage of cause-specific survival at 5 years varies between 43 and 83% for clear cell carcinomas, between 61 and 90% for papillary carcinomas, and between 80 and 100% for chromophobe carcinomas [25]. This wide range of cause-specific survival suggests that histology should not be taken into account as a single prognostic index for transplantation purposes, at least when only the three commonest histotypes are considered. Certainly, patients who have renal carcinomas with particularly poor prognosis such as medullary carcinomas or Bellini’s duct carcinomas should be excluded as renal graft recipients, since their prognosis is dramatically dismal [27], even after a radical resection of a localized primary.
Tumour grade
Tumour grade is another pathological feature of kidney carcinomas that has proved to hold prognostic significance; however, its evaluation is closely dependent on the specific expertise of the pathologist who examines the histological specimens. Furthermore, following the 2013 Vancouver ISUP consensus conference, a simplified nucleolar grading system is now recommended and is being gradually implemented in everyday clinical practice [28]. This new grading system seems to reduce the inter-observer variability in pathological assessment.
Sarcomatoid de-differentiation
Sarcomatoid de-differentiation represents a transformation of the tumour towards a higher degree of malignancy [29]. At the morphological level, it is characterized by the presence of spindle or rhabdoid cells with ultrastructural and immunohistochemical evidence of epithelial and mesenchymal differentiation. This can be considered a common aspect, irrespective of the primary tumour histology, suggesting an increased biological aggressiveness.
Literature results suggest that the presence of a framework of sarcomatoid de-differentiation is generally associated with a median survival of approximately 12 months and with a 5- and 10-year cause-specific survival of 22 and 13%, respectively [30]. In relation to the main tumour histologies, data from the Mayo Clinic show that 2 years after surgical treatment in patients with sarcomatoid differentiation, survival was 30, 40 and 25% in patients with clear cell, papillary or chromophobe histology, respectively, whilst in patients without sarcomatoid de-differentiation the figures were 84, 96 and 96%, respectively [31].
Integrated prognostic systems
With a view to improving the prognostic accuracy of the individual clinico-pathological factors considered, in recent years many authors have proposed the use of mathematical models based on integration of the major prognostic factors [32]. The two systems which are most widely utilized are probably the UCLA Integrated Staging System (UISS) [33] and the Leibovich score [34], which have also been utilized recently to stratify patients for clinical trials of adjuvant therapy [35].
The UISS [33] is able to predict the overall survival of patients with RCC according to the disease pathology stage (according to the 1997 TNM classification), Fuhrman’s nuclear grading and the Eastern Cooperative Oncology Group (ECOG) performance status. This system may be applied to kidney cancer patients with both localised and metastatic disease, and helps subdivide them into groups with low, intermediate and high risk of mortality. In patients with non-metastatic disease, application of the UISS can correctly predict the prognostic performance of these patients in a percentage ranging from 76.5 to 86.3%. Notably, this system has been developed regardless of histology.
In 2003, Leibovich et al. [34] developed another scoring system which proved to have higher than 80% predictive accuracy and enabled identification of three groups of patients with a different risk of developing metastasis: high, intermediate and low, respectively. This model has the advantage of taking into account the lack of lymphnodes at pathological evaluation of the surgical specimen (Nx status), an event which occurs with increasing frequency for several reasons, including the widespread use of mini-invasive surgical techniques [34].
In 2010, Klatte et al. [36] developed and validated another prognostic nomogram specifically designed for papillary kidney carcinomas. This nomogram takes into consideration the following variables: incidental presentation of the tumour, T stage, M stage, presence of vascular invasion, and presence of necrosis. External independent validation revealed a 94.2% predictive accuracy of this nomogram.
At present, however, no study has compared the different integrated prognostic systems available, with a view to identifying the ideal one, if any. Even though no specific study has been carried out in immune suppressed subjects, these tools could help in selecting potential kidney transplant recipients. Patients with a high probability of being disease- or metastasis-free at a given time point could thus receive a kidney graft safely enough, whilst those at high risk of relapsing or of dying from the tumour should not be listed for transplantation, given the probability of a short survival.
Conclusions and current suggestions
As already highlighted by others [19, 20], a fixed waiting time before a patient with a previous renal cancer gets listed for renal transplantation is no longer justified, since it may lead to an unnecessary and harmful delay in receiving a graft. At present there is enough evidence that some patients may be listed immediately, while others are at too high a risk of metastasis to benefit from a transplanted kidney or improve their life expectancy due to the prolonged immunosuppressive therapy needed.
It is now clear that patients should be individually evaluated for their own risk of cancer recurrence after transplantation and the powerful tools presently available can accurately predict overall survival, cause-specific survival, or metastasis-free survival (in the short- and medium-term) of patients with completely resected, organ-confined or locally-advanced, renal cell carcinoma of all histotypes and specifically of papillary histotype. The main limit of these tools is that they have not been validated in subjects assuming immunosuppressive drugs for years, as in the case of transplanted patients.
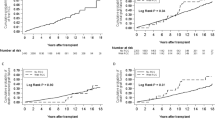
However, information is now available to help classifying some patients more easily. For instance, of the several scoring systems proposed to date, the one by Leibovich et al. [33] is being widely used in clinical practice since it proves simple and reliable enough, allowing stratification of patients according to their risk of metastasis (Fig. 1). By this system subjects with a score from 0 to 2 are at low risk since more than 90% of them are metastasis-free after 10 years while, on the contrary, only 23% of patients with a score of 6 or higher do not have metastases after the same length of time. Thus, the former may be listed with a short or no waiting time, while the latter should be excluded from a transplantation programme.
The group of subjects with a score of 3–5 are at intermediate risk, 64% of them being metastasis-free after 10 years, thus requiring individual evaluation before taking a decision as to listing them or not.

Modified from Ref. [34]
Metastasis-free survival probability after renal carcinoma resection according to the Leibovich risk model score. Patients can be stratified into three prognostic groups: low, intermediate and high risk.
Likewise, histological examination or tumour grading may be useful in this setting. As synthesized in Fig. 2, patients with a medullary or Bellini’s duct carcinoma or those with sarcomatoid de-differentiation at histology are unfit to receive a graft and should not be listed. Again, renal transplantation is contraindicated in subjects with a G4 carcinoma. On the other hand, patients treated for a chromophobe or clear cell papillary tumour or G1 carcinoma carry a low risk and may be listed. Unfortunately, difficulties in risk assessment still remain in all other patients, and they require individual and careful evaluation by an oncologist and urologist to decide whether they are suitable to be listed.

A suggested algorithm for approaching patients with ESRD and a previous renal cancer as possible candidates for renal transplantation ESRD, end-stage renal disease
Finally, given the increasing relevance of the problem, a consensus conference involving all specialists in the field is called for, pending studies focusing specifically on the risk assessment of patients with a previous renal cancer who become candidates for renal transplantation.
References
Siegel RL, Miller KD, Jemal A (2018) Cancer statistics, 2018. CA Cancer J Clin 68:7–30. https://doi.org/10.3322/caac.21442
Campbell SC, Novick AC, Belldegrun A et al (2009) Guideline for management of the clinical T1 renal mass. J Urol 182:1271–1279. https://doi.org/10.1016/j.juro.2009.07.004
Ljungberg B, Bensalah K, Canfield S et al (2015) EAU guidelines on renal cell carcinoma: 2014 update. Eur Urol 67:913–924. https://doi.org/10.1016/j.eururo.2015.01.005
Psutka SP, Feldman AS, McDougal WS et al (2013) Long-term oncologic outcomes after radiofrequency ablation for T1 renal cell carcinoma. Eur Urol 63:486–492. https://doi.org/10.1016/j.eururo.2012.08.062
Launay-Vacher V (2016) Renal dysfunction has statistically and clinically significant deleterious effects on anticancer drug safety. J Clin Oncol 34:2428–2428. https://doi.org/10.1200/JCO.2015.65.1554
Frascà GM, Sandrini S, Cosmai L et al (2015) Renal cancer in kidney transplanted patients. J Nephrol 28:659–668. https://doi.org/10.1007/s40620-015-0219-8
Penn I (1997) Evaluation of transplant candidates with pre-existing malignancies. Ann Transpl 2:14–17
Campbell S, Pilmore H, Gracey D et al (2013) KHA-CARI guideline: recipient assessment for transplantation. Nephrology (Carlton) 18:455–462. https://doi.org/10.1111/nep.12068
Kasiske BL, Cangro CB, Hariharan S et al (2001) The evaluation of renal transplantation candidates: clinical practice guidelines. Am J Transpl 1(Suppl 2):3–95
Bunnapradist S, Danovitch GM (2007) Evaluation of adult kidney transplant candidates. Am J Kidney Dis 50:890–898. https://doi.org/10.1053/j.ajkd.2007.08.010
European Best Practice Guidelines for Renal Transplantation (2000) Evaluation, selection and preparation of the potential transplant recipient. Work-up for cancer and waiting time for pre-existing cancer. Nephrol Dial Transpl 15(supp 7):6. https://doi.org/10.1093/oxfordjournals.ndt.a027999
Karam G, Kälble T, Alcaraz A et al (2014) Guidelines on renal transplantation of the European Association of Urology. https://uroweb.org/wp-content/uploads/EAU-Guidelines-Renal_Transplant-2013.pdf. Accessed 8 May 2018
Knoll G, Cockfield S, Blydt-Hansen T et al (2005) Canadian Society of Transplantation consensus guidelines on eligibility for kidney transplantation. CMAJ 173:1181–1184. https://doi.org/10.1503/cmaj.051291
Webster AC, Craig JC, Simpson JM et al (2007) Identifying high risk groups and quantifying absolute risk of cancer after kidney transplantation: a cohort study of 15,183 recipients. Am J Transpl 7:2140–2151. https://doi.org/10.1111/j.1600-6143.2007.01908.x
Kauffman HM, Cherikh WS, McBride MA et al (2005) Transplant recipients with a history of a malignancy: risk of recurrent and de novo cancers. Transpl Rev 19:55–64. https://doi.org/10.1016/j.trre.2005.02.002
Viecelli AK, Lim WH, Macaskill P et al (2015) Cancer-specific and all-cause mortality in kidney transplant recipients with and without previous cancer. Transplantation 99:2586–2592. https://doi.org/10.1097/TP.0000000000000760
Brattström C, Granath F, Edgren G et al (2013) Overall and cause-specific mortality in transplant recipients with a pretransplantation cancer history. Transplantation 96:297–305. https://doi.org/10.1097/TP.0b013e31829854b7
Farrugia D, Mahboob S, Cheshire J et al (2014) Malignancy-related mortality following kidney transplantation is common. Kidney Int 85:1395–1403. https://doi.org/10.1038/ki.2013.458
Kiberd BA, Rose C, Gill JS (2009) Cancer mortality in kidney transplantation. Am J Transpl 9:1868–1875. https://doi.org/10.1111/j.1600-6143.2009.02728.x
Dahle DO, Grotmol T, Leivestad T et al (2017) Association between pretransplant cancer and survival in kidney transplant recipients. Transplantation 101:2599–2605. https://doi.org/10.1097/TP.0000000000001659
Nguyen KA, Syed JS, Luciano R et al (2017) Optimizing waiting duration for renal transplants in the setting of renal malignancy: is 2 years too long to wait? Nephrol Dial Transpl 32:1767–1773. https://doi.org/10.1093/ndt/gfx254
Greene FL, Sobin LH (2009) A worldwide approach to the TNM staging system: collaborative efforts of the AJCC and UICC. J Surg Oncol 99:269–272. https://doi.org/10.1002/jso.21237
Novara G, Ficarra V, Antonelli A et al (2011) Corrigendum to “Validation of the 2009 TNM version in a large multi-institutional cohort of patients treated for renal cell carcinoma: are further improvements needed?”. Eur Urol 59:182. https://doi.org/10.1016/j.eururo.2010.10.017 (Eur Urol 58:588–595)
Klatte T, Chung J, Leppert JT et al (2007) Prognostic relevance of capsular involvement and collecting system invasion in stage I and II renal cell carcinoma. BJU Int 99:821–824. https://doi.org/10.1111/j.1464-410X.2006.06729.x
Cheville JC, Lohse CM, Zincke H et al (2003) Comparisons of outcome and prognostic features among histologic subtypes of renal cell carcinoma. Am J Surg Pathol 27:612–624
Ficarra V, Martignoni G, Galfano A et al (2006) Prognostic role of the histologic subtypes of renal cell carcinoma after slide revision. Eur Urol 50:786–794. https://doi.org/10.1016/j.eururo.2006.04.009
Gupta R, Billis A, Shah RB et al (2012) Carcinoma of the collecting ducts of bellini and renal medullary carcinoma. Am J Surg Pathol 36:1265–1278. https://doi.org/10.1097/PAS.0b013e3182635954
Delahunt B, Cheville JC, Martignoni G et al (2013) The International Society of Urological Pathology (ISUP) grading system for renal cell carcinoma and other prognostic parameters. Am J Surg Pathol 37:1490–1504. https://doi.org/10.1097/PAS.0b013e318299f0fb
Jones TD, Eble JN, Wang M et al (2005) Clonal divergence and genetic heterogeneity in clear cell renal cell carcinomas with sarcomatoid transformation. Cancer 104:1195–1203. https://doi.org/10.1002/cncr.21288
Delahunt B (1999) Sarcomatoid renal carcinoma: the final common dedifferentiation pathway of renal epithelial malignancies. Pathology 31:185–190
Lohse CM, Cheville JC (2005) A review of prognostic pathologic features and algorithms for patients treated surgically for renal cell carcinoma. Clin Lab Med 25:433–464. https://doi.org/10.1016/j.cll.2005.01.013
Galfano A, Novara G, Iafrate M et al (2008) Mathematical models for prognostic prediction in patients with renal cell carcinoma. Urol Int 80:113–123. https://doi.org/10.1159/000112599
Zisman A, Pantuck AJ, Figlin RA, Belldegrun AS (2001) Validation of the UCLA integrated staging system for patients with renal cell carcinoma. J Clin Oncol 19:3792–3793. https://doi.org/10.1200/JCO.2001.19.17.3792
Leibovich BC, Blute ML, Cheville JC et al (2003) Prediction of progression after radical nephrectomy for patients with clear cell renal cell carcinoma. Cancer 97:1663–1671. https://doi.org/10.1002/cncr.11234
Leibovich BC, Han K, Bui MHT et al (2003) Scoring algorithm to predict survival after nephrectomy and immunotherapy in patients with metastatic renal cell carcinoma. Cancer 98:2566–2575. https://doi.org/10.1002/cncr.11851
Klatte T, Said JW, Seligson DB et al (2011) Pathological, immunohistochemical and cytogenetic features of papillary renal cell carcinoma with clear cell features. J Urol 185:30–36. https://doi.org/10.1016/j.juro.2010.09.013
Funding
None.
Author information
Authors and Affiliations
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Informed consent
For this type of study formal consent is not required.
Human and animal participants right statement
This article does not contain any studies with human participants or animals performed by any of the authors.
Rights and permissions
About this article

Cite this article
Frascà, G.M., Brigante, F., Volpe, A. et al. Kidney transplantation in patients with previous renal cancer: a critical appraisal of current evidence and guidelines. J Nephrol 32, 57–64 (2019). https://doi.org/10.1007/s40620-018-0542-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40620-018-0542-y