
Abstract
Purpose
To investigate whether the metabolic score for insulin resistance (METS-IR) is associated with an increased risk of cardiovascular disease (CVD).
Methods
A total of 6489 participants aged 35–70 years without a history of CVD were included in this prospective cohort study. The median follow-up time was 10.6 years. The METS-IR was calculated as ln [2 × FPG (mg/dL) + fasting TG (mg/dL)] × BMI (kg/m2)/ln [HDL-C (mg/dL)]. The primary outcome was CVD, defined as the composite of coronary heart disease (CHD) and stroke.
Results
During follow-up, 396 individuals developed CVD. Kaplan–Meier survival curves by quintiles of METS-IR showed statistically significant differences (log-rank test, P < 0.001). Multivariate Cox regression analysis showed that the hazard ratio [95% confidence interval (95% CI)] of CVD was 1.80 (1.24–2.61) in quintile 5 and 1.17 (1.05–1.31) for per standard deviation (SD) increase in METS-IR. In subgroup analysis, the significant association between METS-IR and CVD was mainly observed among females and subjects without diabetes mellitus. A significant interaction was found between gender and METS-IR (P-interaction = 0.001). Moreover, adding METS-IR to models with traditional risk factors yielded a significant improvement in discrimination and reclassification of incident CVD.
Conclusion
The elevated METS-IR was independently associated with incident CVD, suggesting that the METS-IR might be a valuable indicator for risk stratification and early intervention of CVD.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Despite advances in prevention, diagnosis, and treatment, cardiovascular disease (CVD), especially coronary heart disease (CHD) and stroke, remains the leading cause of death worldwide [1, 2]. Therefore, it is crucial to recognize and control potential risk factors. Insulin resistance (IR), which is a prominent characteristic of metabolic syndrome and type 2 diabetes mellitus (T2DM), also contributes to the progression of CVD [3,4,5]. The increase of metabolic risk factors impeded the control of CVD, which presented major and persistent challenges for the reduction in cardiovascular disease burden, particularly in developing countries [6]. These facts show that early identification of IR has clinical implications in the prevention of CVD development.
In this regard, the metabolic score for insulin resistance (METS-IR) has been evaluated as a surrogate for IR and demonstrated a high concordance with the hyperinsulinemic–euglycemic clamp [7]. Previous studies showed that the METS-IR was associated with multiple risk factors of CVD, such as diabetes, obesity, hypertension, hyperuricemia, and nonalcoholic fatty liver disease [7,8,9,10]. A cohort study conducted among Korean has found that elevated METS-IR level was an independent risk factor for incident ischemic heart disease (IHD) in community-dwelling individuals without diabetes [11].
CVD mortality is higher in middle-income countries compared with high- or low-income countries [12]. In China, the largest middle-income country, CVD accounts for 40% of deaths [13]. Eastern China has distinct geographic characteristics and lifestyles compared with other regions of the country. In Eastern China, with rapid economic development, the metabolic risk factors increased remarkably over the past 2 decades and the mortality and morbidity of CVD continue to rise at an alarming rate [14]. Due to the heavy burden of metabolic risk factors and CVD among Eastern Chinese population, we prospectively examined the association between the METS-IR and incident CVD in a 10-year follow-up cohort.
Materials and methods
Study design and participants
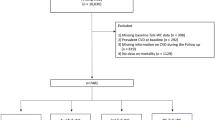
Participants were selected through a random, multi-stage and cluster sampling scheme and assessed at baseline from 2005 to 2006. Twelve communities were selected and a total of 8161 participants aged 35–70 years (4276 women and 3885 men) who had lived in Eastern China for at least 5 years were enrolled. During the follow-up period, 987 participants were lost to follow up, and the follow-up rate was 87.9%. After exclusion of subjects with CVD at baseline and those with missing baseline covariates (n = 685), 6489 individuals [3291 women (1535 postmenopausal women, 46.6%) and 3198 men] were included in the final analysis.
This study complied with the Declaration of Helsinki and was approved by the Ethics Review Committee of the Shandong Academy of Medical Sciences. All participants provided written informed consent.
Data collection
Clinical data were collected using standardized interviewer-administered questionnaires by trained clinicians who were blinded to the study arm. The data included participants’ demographic factors, socioeconomic status, health history, tobacco and alcohol use, physical activity, diet, and other CVD risk factors. Physical activity was assessed by the International Physical Activity Questionnaire (IPAQ) [15]. The Food Frequency Questionnaire (FFQ) was used to record data on food consumption and calculate the percentage of energy provided by fat and carbohydrate [16]. Physical measurements included weight, height, waist and hip circumferences, and blood pressure. Research staff were trained to minimize the errors in measurements. The mean of two measurements was used in this study. All blood samples of subjects were collected in the morning after overnight fasting (12 h minimum). The biochemical testing was performed at the central laboratory of the city hospital by standard and quality-controlled procedures. The levels of fasting plasma glucose (FPG), total cholesterol (TC), triglyceride (TG), and high-density lipoprotein-cholesterol (HDL-C) were measured enzymatically using an autoanalyzer (Type 7600; Hitachi Ltd., Tokyo, Japan). Low‐density lipoprotein-cholesterol (LDL-C) was calculated by the Friedewald equation [17] when TG level was less than 4.5 mmol/L.
Definition of terms
Body mass index (BMI) was calculated as weight (kg) divided by the square of height (m2). Waist-to-hip ratio (WHR) was calculated as waist circumference (cm) divided by hip circumference (cm). High WHR was defined as a WHR greater than 0.9 in men or greater than 0.85 in women. Hypertension was defined as baseline blood pressure \(\ge \) 140/90 mm Hg, self-reported history of hypertension, or use of antihypertensive medications. Diabetes was defined as a baseline fasting glucose \(\ge \) 7 mmol/L, self-reported history of diabetes, or use of antidiabetic drugs or insulin. Energy intake from fat and carbohydrate was split into tertiles (Energy intake from fat: tertile 1, < 13.4%; tertile 2, 13.4% to 17.8%; tertile 3, > 17.8%. Energy intake from carbohydrate: tertile 1, < 59.6%; tertile 2, 59.6% to 68.4%; tertile 3, > 68.4%). Low physical activity was defined as < 600 metabolic equivalent task (MET)\(\times \) minutes per week or < 150 min per week of moderate intensity physical activity. METS-IR was calculated as ln [(2 × FPG (mg/dL)) + fasting TG (mg/dL)] × BMI (kg/m2)/ln [HDL-C (mg/dL)] [7].
Assessment and definition of the outcome
The primary outcome of our study was CVD, defined as the composite of CHD and stroke (ischemic, hemorrhagic, or unspecified). CHD was defined as myocardial infarction, angina pectoris, and angiography-proven CHD. The secondary outcomes included CHD and stroke. These events were collected using standardized case-report forms and reported based on common definitions.
Statistical analysis
Statistical analysis was performed using SPSS version 25.0 (SPSS, Chicago, IL) and R software version 4.1.3 (R Foundation for Statistical Computing). Continuous variables were presented as mean ± standard deviation (SD) and compared using the ANOVA test. Categorical variables were expressed with counts and percentages and compared using the Chi-square test. The associations between METS-IR and clinical parameters were assessed using Pearson or Spearman correlation analysis, as appropriate. The 10-year cumulative CVD incidence in quintiles of the METS-IR was studied using the Kaplan–Meier method. We performed Cox regression analysis to further determine whether METS-IR was an independent predictor for the incidence of CVD. We built 3 regression models of increasing confounders: Model 1 was the unadjusted model; Model 2 was the partially adjusted model that was adjusted for age and gender; Model 3 was the fully adjusted model that was controlled for age, gender, high WHR, tobacco use, alcohol use, energy intake from fat, energy intake from carbohydrate, physical activity, education, diabetes mellitus (DM), hypertension, family history of cardiovascular disease (FH-CVD), TC, LDL-C, use of antihypertensive drugs, and use of antidiabetic drugs or insulin. METS-IR was entered into the models as continuous variables and categorical variables (the quartiles of METS-IR), respectively. METS-IR was further standardized to determine the predictive value of per SD increase. The variance inflation factor (VIF) of the variables included in the models was calculated to avoid the result deviation caused by multicollinearity. We did not find evidence of collinearity in the models, given the VIF of < 5. We compared the nonlinear restricted cubic spline models with linear models and tested the potential nonlinearity. The value of Akaike information criterion (AIC) was lowest when the METS-IR was entered into the models as linear term and no statistically significant evidence for nonlinearity was found (all nonlinear P values > 0.05). Therefore, we performed the analysis by including METS-IR as linear term in this study. We also performed subgroup analysis based on age, gender, DM, and hypertension to determine whether the association between METS-IR and incident CVD differed across various subgroups and P for interaction was calculated. To evaluate whether an increased METS-IR had incremental predictive value for incident CVD, we compared the partially and fully adjusted models (Model 2 and Model 3) with and without METS-IR, and C-statistics and continuous net reclassification improvement (NRI) were obtained. A p value of less than 0.05 was considered to be statistically significant.
Results
Baseline characteristics
A total of 6489 participants (3291 women and 3198 men) without a history of CVD were enrolled in this study, with an average age of 49.03 ± 9.98 years, and the average METS-IR index value was 38.24 ± 6.61. Participants were divided into five groups according to the quintiles of METS-IR. As shown in Table 1, subjects in the quintile 5 group had the highest mean age, BMI, WHR, SBP, DBP, FPG, TC, and TG values, and the highest proportions of high WHR, DM, hypertension, FH-CVD, antihypertensive drugs’ use, and antidiabetic drugs or insulin use (Table 1).
Correlations between METS-IR and cardiovascular risk factors
The associations between METS-IR and cardiovascular risk factors were examined using Spearman or Pearson correlation analysis. As shown in Table 2, METS-IR was positively associated with age, BMI, WHR, SBP, DBP, FPG, TC, TG, and LDL-C (P < 0.001), and negatively associated with HDL-C (P = 0.004) (Table 2).
METS-IR and incidence of CVD
After a median follow-up of 10.6 years (interquartile range: 9.9–10.8), a total of 396 individuals (6.1%) developed CVD. We compared the 10-year cumulative incidence rate of CVD according to the quintiles of the METS-IR. The highest 10-year CVD incidence was observed in the quintile 5 group (9.2%; 95% CI 7.8–10.9%), while the lowest incidence was observed in the quintile 1 group (4.0%; 95% CI 3.1–5.2%) (log-rank test, P < 0.001) (Fig. 1).

Cumulative incidence of CVD by quintiles of METS-IR over 10 years. METS-IR the metabolic score for insulin resistance, CVD Cardiovascular disease
As presented in Table 3, the unadjusted HR (95% CI) for incidence of CVD with per SD increase in METS-IR was 1.27 (1.17–1.39). Multivariate Cox regression analyses showed that METS-IR, whether considered as a categorical or continuous variable, remained significant after adjusting for confounders. In the partially adjusted regression model (adjusted for age and gender), the adjusted HR (95% CI) for incident CVD with per SD increase in METS-IR was 1.22 (1.12–1.34). Compared with individuals in the lowest quintile, the partially adjusted HR for CVD was 2.01 (95% CI 1.45–2.79) in the highest quintile. The increased risk of incident CVD from quintile 1 to quintile 5 was statistically significant (P for trend < 0.001). A similar pattern was observed in fully adjusted model (Per SD increase: HR = 1.17, 95% CI 1.05–1.31; Quintile 5: HR = 1.80, 95% CI 1.24–2.61; P for trend = 0.008) (Table 3).
During the follow-up period, 247 (3.8%) and 169 (2.6%) cases of CHD and stroke occurred. We further studied the associations between METS-IR and CHD and stroke. As shown in Table 4, for each SD increase in METS-IR, the HR (95% CI) for CHD was 1.28 (1.12–1.47) in the fully adjusted regression model. A test for trend with increasing quintiles of METS-IR was significant (P for trend = 0.001) for incident CHD. The fully adjusted HR (95% CI) for CHD was 2.93 (1.73–4.97) in the highest quintile. Although the incidence of stroke was likely to increase with increasing quintiles of METS-IR, no statistical significance between METS-IR and incident stroke was found (Table 4).
Moreover, multivariate Cox regression analyses showed that aging, hypertension, higher carbohydrate intake, and family history of CVD increased the risk of CVD/CHD (Figs. 2, 3).

Hazard Ratios (95% CI) of incident CVD for covariates. P values in bold are < 0.05. HR Hazard ratio, METS-IR the metabolic score for insulin resistance, WHR waist-to-hip ratio, DM diabetes mellitus, FH-CVD family history of cardiovascular disease, TC total cholesterol, LDL-C low-density lipoprotein-cholesterol

Hazard ratios (95% CI) of incident CHD for covariates. P values in bold are < 0.05. HR hazard ratio, METS-IR the metabolic score for insulin resistance, WHR waist-to-hip ratio, DM diabetes mellitus, FH-CVD family history of cardiovascular disease, TC total cholesterol, LDL-C low-density lipoprotein-cholesterol
Subgroup analysis
The association between METS-IR and CVD was examined in the subgroup analysis and the P value for interaction was calculated. A significant interaction was found between gender and the METS-IR for incident CVD in the fully adjusted model (Model 3) (P values for interaction = 0.001). Accordingly, a significant association between METS-IR and CVD was found only among females (Fig. 4). The association was significant both in premenopausal women and postmenopausal women (Table S1). Although no interaction was found between DM and METS-IR (P value for interaction = 0.469), the statistical significance was observed only among patients without DM. No interaction was found between age, hypertension, and METS-IR for incidence of CVD (Both P values for interaction > 0.05) (Fig. 4).

Subgroup and interaction analysis between METS-IR (Per SD) and CVD across various subgroups. P values in bold are < 0.05. HR hazard ratio
Given that a gender-by-METS-IR interaction was observed, we explored the association between METS-IR and CHD and stroke in males and females. A significant association between METS-IR and CHD was found only among females (Table S2). The METS-IR was an independent predictor for stroke in females as a continuous variable, but not in males (Table S3).
Evaluation of the predictive performance of METS-IR for CVD
The incremental predictive value of METS-IR for CVD is shown in Table 5. Risk prediction was improved by adding METS-IR to the model including age and sex (Model 2) [the C-statistic increased from 0.696 to 0.702 (difference, 0.6%; P < 0.001); continuous NRI (95% CI) 0.187 (0.085–0.288), P < 0.001]. Adding the METS-IR to the fully adjusted model (Model 3) also significantly improved risk discrimination and reclassification of incident CVD [the C-statistic increased from 0.725 to 0.728 (difference, 0.3%; P = 0.006; continuous NRI (95% CI) 0.126 (0.025–0.228), P = 0.015]. The models with METS-IR showed a reduction of false positives while not at the expense of increasing false negatives [Model 2: continuous NRI for CVD (95% CI): 0.020 (− 0.078 to 0.119), P = 0.688; continuous NRI for Non-CVD (95% CI) 0.167 (0.142–0.192), P < 0.001. Model 3: continuous NRI for CVD (95% CI) − 0.005 (− 0.104 to 0.093), P = 0.920; continuous NRI for Non-CVD (95% CI) 0.132 (0.107–0.157), P < 0.001].
Discussion
In Eastern China, the metabolic risk factors have remarkably increased along with an economic boom over recent decades. In this study, we investigated the relationship between the METS-IR and incident CVD among Eastern Chinese population. The main findings of our study were as follows: (1) The METS-IR was significantly associated with increased risk for incident CVD/CHD, independent of traditional cardiovascular risk factors. (2) A significant interaction was found between gender and METS-IR for incident CVD, and the significant association between METS-IR and CVD was mainly observed among females. (3) Adding the METS-IR to the models with traditional risk factors yielded a significant improvement in outcome prediction. Taken together, this 10-year follow-up cohort among Eastern Chinese population revealed the predictive value of the METS-IR for incident CVD and CHD.
Metabolic risk factors have been one of the leading drivers of the burden of CVD [6]. Insulin resistance (IR) is a general term, meaning that adipose tissue, skeletal muscle, liver, and pancreas display a low response to insulin action. Several mechanisms that IR aggravates atherosclerosis have been elucidated, including systemic inflammation, endothelial dysfunction, and oxidative stress [18, 19]. Previous studies have shown that IR was an independent risk factor for CVD [20, 21]. The hyperinsulinemic–euglycemic clamp technique is the gold standard to assess IR and HOMA-IR is the most widely used method. However, the hyperinsulinemic–euglycemic clamp technique is costly and time‐consuming [22], whereas HOMA-IR is likely to cause significant bias because of insulin measurements [23, 24]. In this regard, the METS-IR, as a simple surrogate for IR, has proven to be associated with multiple risk factors of CVD [7,8,9,10]. However, the predictive value of METS-IR for CVD remains poorly known.
In our present study, we found that participants with high METS-IR had more cardiovascular risk factors. Our results also revealed the correlation between METS-IR and other risk factors, which was consistent with previous studies [7, 8]. Yoon J et al. found that METS-IR was an independent predictor of incident ischemic heart disease (IHD) in a longitudinal study among Korean without diabetes [11]. However, the previous study was limited to subjects without diabetes, and the relationship between METS-IR and CVD other than IHD was not studied. The predictive value of METS-IR for CVD in the Eastern Chinese population was first discovered in this study. In our data analysis, per SD increase in METS-IR was associated with 17% and 28% higher risks for CVD and CHD events in the fully adjusted model, respectively. We also found that the fifth quintile of METS-IR had 80% and 193% higher risks for incident CVD and CHD, respectively.
In subgroup analyses, a significant interaction was found between gender and METS-IR for incident CVD (P value for interaction = 0.001). Accordingly, a significant association between METS-IR and CVD was found only among females. Previous studies have reported the sex differences in the risk of cardiovascular disease associated with IR. A meta-analysis included 87 studies found that females with metabolic syndrome had a higher risk of CVD than males [25]. The Framingham study also showed that females with impaired fasting glucose had increased CVD risk to a similar degree as established diabetes, but not in males [26]. This excess risk in females could be attributable partly to sex differences in the body anthropometry and preferred location of fat storage [27]. Moreover, the heavier risk factor burden and a greater effect of elevated blood pressure, low HDL-C, and high triglycerides in women might also be part of the reason for this difference [28].
In subjects without diabetes, a significant association between METS-IR and incident CVD was observed, which suggested that METS-IR might be independent of diabetes to influence cardiovascular outcomes. Yoon J et al. also reported the independent predictive value of METS-IR among Korean without diabetes [11]. However, the association between METS-IR and CVD was not statistically significant in subjects with diabetes. In patients with T2DM, the classic CVD risk factors are major predictors of CVD events, and the risk is further increased by hyperglycemia, but to a lesser extent as by insulin resistance alone [18]. In addition, different antidiabetic drugs may have different effects on insulin action. In patients receiving antidiabetic therapy, the calculation of METS-IR was affected by drugs, and, as a result, diminished the predictive value for incident CVD.
The usefulness of METS-IR in the improvement of CVD risk prediction was uncertain when combining the traditional risk factors. In our study, adding the METS-IR to the model including age and sex yielded an increment of 0.006 in the C-statistic (P < 0.001) and a continuous NRI of 18.7% (P < 0.001). Adding the METS-IR to the fully adjusted model also provided a statistically significant improvement in risk discrimination and reclassification, with an increment of 0.003 in the C-statistic (P = 0.006) and a continuous NRI of 12.6% (P = 0.015). These results had clinical implications for risk stratification and early intervention of CVD.
Several limitations of this study should be considered. First, laboratory parameters were only detected once at admission with a potential bias due to measurement error. Second, our analysis was restricted to participants aged 35–70 years. Finally, all participants in this study were selected from Eastern China; therefore, our findings cannot be generalized to other population.
Conclusion
In conclusion, the present data demonstrate that METS-IR is a valuable predictor of incident CVD and CHD. Therefore, we propose that METS-IR is a simple, inexpensive, and timely index for the risk stratification and early intervention of CVD.
Data availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Virani SS, Alonso A, Benjamin EJ et al (2020) Heart disease and stroke statistics-2020 update: a report from the American Heart Association. Circulation 141:e139-139e596. https://doi.org/10.1161/CIR.0000000000000757
Murray CJ (2020) Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet 396:1204–1222. https://doi.org/10.1016/S0140-6736(20)30925-9
Taube A, Schlich R, Sell H, Eckardt K, Eckel J (2012) Inflammation and metabolic dysfunction: links to cardiovascular diseases. Am J Physiol Heart Circ Physiol 302:H2148-2165. https://doi.org/10.1152/ajpheart.00907.2011
Bornfeldt KE, Tabas I (2011) Insulin resistance, hyperglycemia, and atherosclerosis. Cell Metab 14:575–585. https://doi.org/10.1016/j.cmet.2011.07.015
Beverly JK, Budoff MJ (2020) Atherosclerosis: pathophysiology of insulin resistance, hyperglycemia, hyperlipidemia, and inflammation. J Diabetes 12:102–104. https://doi.org/10.1111/1753-0407.12970
Wang W, Hu M, Liu H et al (2021) Global Burden of Disease Study 2019 suggests that metabolic risk factors are the leading drivers of the burden of ischemic heart disease. Cell Metab 33:1943-1956.e2. https://doi.org/10.1016/j.cmet.2021.08.005
Bello-Chavolla OY, Almeda-Valdes P, Gomez-Velasco D et al (2018) METS-IR, a novel score to evaluate insulin sensitivity, is predictive of visceral adiposity and incident type 2 diabetes. Eur J Endocrinol 178:533–544. https://doi.org/10.1530/EJE-17-0883
Han KY, Gu J, Wang Z et al (2022) Association between METS-IR and prehypertension or hypertension among normoglycemia subjects in Japan: a retrospective study. Front Endocrinol (Lausanne) 13:851338. https://doi.org/10.3389/fendo.2022.851338
Li Y, You A, Tomlinson B et al (2021) Insulin resistance surrogates predict hypertension plus hyperuricemia. J Diabetes Investig 12:2046–2053. https://doi.org/10.1111/jdi.13573
Cai X, Gao J, Hu J et al (2022) Dose-response associations of metabolic score for insulin resistance index with nonalcoholic fatty liver disease among a nonobese Chinese population: retrospective evidence from a population-based cohort study. Dis Markers 2022:4930355. https://doi.org/10.1155/2022/4930355
Yoon J, Jung D, Lee Y, Park B (2021) The metabolic score for insulin resistance (METS-IR) as a predictor of incident ischemic heart disease: a longitudinal study among korean without diabetes. J Pers Med. https://doi.org/10.3390/jpm11080742
Mensah GA, Roth GA, Fuster V (2019) The global burden of cardiovascular diseases and risk factors: 2020 and beyond. J Am Coll Cardiol 74:2529–2532. https://doi.org/10.1016/j.jacc.2019.10.009
Zhao D, Liu J, Wang M, Zhang X, Zhou M (2019) Epidemiology of cardiovascular disease in China: current features and implications. Nat Rev Cardiol 16:203–212. https://doi.org/10.1038/s41569-018-0119-4
Zhou M, Wang H, Zeng X et al (2019) Mortality, morbidity, and risk factors in China and its provinces, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 394:1145–1158. https://doi.org/10.1016/S0140-6736(19)30427-1
Craig CL, Marshall AL, Sjöström M et al (2003) International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports Exerc 35:1381–1395. https://doi.org/10.1249/01.MSS.0000078924.61453.FB
Dehghan M, Mente A, Teo KK et al (2012) Relationship between healthy diet and risk of cardiovascular disease among patients on drug therapies for secondary prevention: a prospective cohort study of 31 546 high-risk individuals from 40 countries. Circulation 126:2705–2712. https://doi.org/10.1161/CIRCULATIONAHA.112.103234
Friedewald WT, Levy RI, Fredrickson DS (1972) Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin Chem 18:499–502
Laakso M, Kuusisto J (2014) Insulin resistance and hyperglycaemia in cardiovascular disease development. Nat Rev Endocrinol 10:293–302. https://doi.org/10.1038/nrendo.2014.29
Ormazabal V, Nair S, Elfeky O, Aguayo C, Salomon C, Zuñiga FA (2018) Association between insulin resistance and the development of cardiovascular disease. Cardiovasc Diabetol 17:122. https://doi.org/10.1186/s12933-018-0762-4
Jeppesen J, Hansen TW, Rasmussen S, Ibsen H, Torp-Pedersen C, Madsbad S (2007) Insulin resistance, the metabolic syndrome, and risk of incident cardiovascular disease: a population-based study. J Am Coll Cardiol 49:2112–2119. https://doi.org/10.1016/j.jacc.2007.01.088
Gast KB, Tjeerdema N, Stijnen T, Smit JW, Dekkers OM (2012) Insulin resistance and risk of incident cardiovascular events in adults without diabetes: meta-analysis. PLoS One 7:e52036. https://doi.org/10.1371/journal.pone.0052036
Pacini G, Mari A (2003) Methods for clinical assessment of insulin sensitivity and beta-cell function. Best Pract Res Clin Endocrinol Metab 17:305–322. https://doi.org/10.1016/s1521-690x(03)00042-3
Rudvik A, Månsson M (2018) Evaluation of surrogate measures of insulin sensitivity - correlation with gold standard is not enough. BMC Med Res Methodol 18:64. https://doi.org/10.1186/s12874-018-0521-y
Manley SE, Stratton IM, Clark PM, Luzio SD (2007) Comparison of 11 human insulin assays: implications for clinical investigation and research. Clin Chem 53:922–932. https://doi.org/10.1373/clinchem.2006.077784
Mottillo S, Filion KB, Genest J et al (2010) The metabolic syndrome and cardiovascular risk a systematic review and meta-analysis. J Am Coll Cardiol 56:1113–1132. https://doi.org/10.1016/j.jacc.2010.05.034
Levitzky YS, Pencina MJ, D’Agostino RB et al (2008) Impact of impaired fasting glucose on cardiovascular disease: the Framingham Heart Study. J Am Coll Cardiol 51:264–270. https://doi.org/10.1016/j.jacc.2007.09.038
de Ritter R, de Jong M, Vos RC et al (2020) Sex differences in the risk of vascular disease associated with diabetes. Biol Sex Differ 11:1. https://doi.org/10.1186/s13293-019-0277-z
Juutilainen A, Kortelainen S, Lehto S, Rönnemaa T, Pyörälä K, Laakso M (2004) Gender difference in the impact of type 2 diabetes on coronary heart disease risk. Diabetes Care 27:2898–2904. https://doi.org/10.2337/diacare.27.12.2898
Funding
This work was supported by the grants of the National Natural Science Foundation of China (No. 81800761 and No. 81970366) and the Key Research and Development Plan of Shandong Province (No. 2021SFGC0503).
Author information
Authors and Affiliations
Contributions
ZW, HC, JP, and JY: drafted and revised the manuscript and contributed to the conception and design of this article. YZ and LL: contributed to the case collection and database organization. WZ, FL, and WX: were responsible for statistical analysis of the data. ZW, HC, JP, and JY: interpreted the results. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Conflict of interest
The authors have no competing interests to declare that are relevant to the content of this article.
Ethical approval
This study complied with the Declaration of Helsinki and was approved by the Ethics Review Committee of the Shandong Academy of Medical Sciences. All participants provided written informed consent (Approval No. 202111120194).
Informed consent
Written informed consent was obtained from all participants.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Wu, Z., Cui, H., Zhang, Y. et al. The impact of the metabolic score for insulin resistance on cardiovascular disease: a 10-year follow-up cohort study. J Endocrinol Invest 46, 523–533 (2023). https://doi.org/10.1007/s40618-022-01925-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40618-022-01925-0