
Abstract
Background
Stress and sleep disturbance have been found to be associated with numerous adverse health outcomes, including cancer. Our study aimed to measure the association between quality of sleep, short-temperedness, and stress in life with the risk of thyroid cancer.
Methods
The present study is conducted on 361 newly diagnosed TC patients and 347 sex–age frequency matched controls. Control and case participants were registered with the same health centers. We used multiple logistic regression to investigate the association between TC risk and the interested factors.
Results
Based on the results of the multivariate analysis, stress (ORalways stressful/often calm = 3.07, 95% CI 1.42–6.63) and short-temperedness (ORnervous/calm = 2.00, 95% CI 1.28–3.11) were directly associated with the risk of TC. On the other hand having a quality sleep (ORsometimes/never = 0.36, 95% CI 0.16–0.79) and quality sleep (ORoften/no = 0.45, 95% CI 0.21–0.96, P = 0.041) seems to be a protective factor.
Conclusions
Some community-based interventions, e.g., lowering stress levels and improving sleep quality, may help in preventing different types of cancer, including TC. We suggest further evaluation of these important findings in the prevention of TC cancer.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Stress and sleep disorders are common in the modern world [1]. As a result, the impact of stress and sleep disorders on health has attracted the interest of medical community. For example, the impacts of these conditions on chronic diseases, such as cardiovascular diseases, stroke, diabetes, metabolic syndrome have been studied before [2]. In addition, several researchers who studied the association of stress and prostate, breast, stomach, lung, and skin cancers reported stress as a promoter of tumorigenesis and cancer development [3,4,5].
Among different types of cancer, thyroid cancer (TC) is the most common malignancy in the endocrine glands [3] and despite the diminishing mortality [6], the rising incidence of this type of cancer has caused serious concerns worldwide [7]. Thyroid cancer is reported to be the fifth and ninth most common types of cancer in women and men, respectively, [8] and the published reports suggested that in several countries, including the United States, France, and Italy, the incidence of TC in women has tripled in a decade. In Korea, in 2012, the incidence of the disease in women was nine times higher than its corresponding figure in 1999 [9]. Similarly, in Iran, it is believed that the incidence of TC is being significantly rising [10]. Although at least a part of the observed significant raises in the incidence of TC in different parts of the world is suggested to be due to overdiagnosis, the issue remains an important global public health concern [11]. Previous studies highlighted a group of contributing factors to TC. These factors include radiation exposure, overweight, hormone therapy, estrogen level, alcohol consumption, benign thyroid diseases, and family history of thyroid cancer [12, 13]. In addition, it has been reported that in those with stress and sleep disorders, thyroid-stimulation hormone concentration is higher and it is suggested that a higher level of thyroid hormone may increase the risk of thyroid cancer [14,15,16].
As the literature suggest, there is limited solid evidence on the relationship between TC risk and sleep disorders, personality, and stress. Planning for cancer prevention, the very high prevalence of stress and sleep disorders among communities makes understanding the association between sleep quality and stress with the risk of different types of cancer including TC very important [17, 18]. Our study aimed to measure the associations of stress, short-temperedness, and lower sleep quality during normal life (before diagnosis of TC) with the risk of TC among Iranian population.
Materials and methods
This is the second phase of a previously published case–control study that was performed to identify the contributing factors to TC [12]. During the first phase, we noticed that TC is potentially associated with some aspects of our lifestyle. Accordingly, we instantly initiated the second phase of the study and collected further information regarding personality, sleeping pattern, and stress in the patients and the controls.
Setting
The present study was conducted in 2019 in Kohgiluyeh and Boyer–Ahmad (K&B), a province with a population of about 345,000 people located in the southern of Iran. The province is selected, because according to the Iranian national cancer registration (NCR) program in 2014, K&B province had the highest annual incidence rate (IR = 16.24 × 105) of TC in the country [19].
Selection of cases
The address and contact information of all patients who were newly diagnosed with TC and their place of residence was K&B province were extracted from the Iranian national cancer registry (NCR) database. Patients were diagnosed based on their pathology report. In addition, patients were included if they were able to participate in the interview.
Selection of controls
From a list of family physicians who the patients were registered with, we randomly selected the same number of control participants (frequency matched). The control participants were also age and sex frequency-matched.
Inclusion and exclusion criteria
Only new cases of thyroid cancer with positive pathology report were included. The control participants were those who report no history of thyroid cancer at the beginning of the interview. Those who refused to participate in the study were also excluded. Verbal consent was obtained from all participants as a significant number of the participants were illiterate.
Data collection
We designed an interview-administered questionnaire to conduct the interview and obtain the required data. Further details regarding the methods of data collection are presented before [12]. Briefly, the required data form the first phase of the study was collected from the participants’ family health and hospital files and an interview conducted by a trained nurse. We evaluated the questionnaire and the interviewing procedure by measuring the reliability of the data in a pilot study on 50 cases with the test–retest method (Cronbach's alpha = 0.77). Data on age, gender, place of residence, educational status, occupation, economic status, marital status, the type of salt consumed, radiation exposure, smoking, body mass index, thyroid disease or cancer in family members, and a history of benign thyroid disease was collected during the first phase of the study. In the second phase, the required data was collected via interviewing the participants by health nurses in the corresponding health centers. In the second phase, data was collected regarding the perceived level of stress, short-temperedness, and sleep quality in their normal life years before starting the symptoms of TC among patients or normal life years before the interview among the controls (all self-reported). The reliability of the questions used in the second phase is evaluated before [5, 20, 21]. The interviewers were selected from trained nurses of the health centers. Neither the participants nor the interviewers were aware of the hypotheses of the study.
Statistical analysis
In the previous article, the relationship between TC and demographic/ health related factors were reported in details [12]. Chi-square test was used to calculate crude associations between the study variables and TC. We calculated the adjusted associations between the new variables with the risk of TC by fitting a multiple logistic regression model. Using forward selection procedure, we refitted the final model of the previous analysis by adding the new variables for the purpose of adjustment for the potential confounders. To conduct statistical analysis, STATA software version 12 was used.
Result
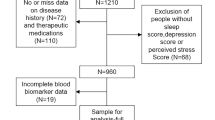
Of total patients (n = 400), 39 (%9.7) were excluded, because they did not agree to participate or had incomplete diagnostic reports. Of the included patients (n = 361), %83.7 were female. Patients were on average 13.6 ± 44.7 years at diagnosis and controls were on average 43.9 ± 13.6, at the interview. The distribution of the study variables among cases and controls are presented in Table 1. Accordingly, a statistically significant relationship was found between the risk of TC and stress, temperedness, and sleep quality (P < 0.05 for all).
As shown in Table 2, after fitting the final model adjusting for other covariates, significant associations were observed between the risk of TC and the new explanatory variables. Accordingly, being under stress (ORalways/seldom = 3.07, 95% CI 1.42–6.63, P = 0.004) and short-temperedness (ORshort-tempered/calm = 2.00, 95% CI 1.28–3.11, P = 0.002) were directly and significantly associated with the risk of TC. On the other hand, quality sleep (ORsometimes/no = 0.36, 95% CI 0.16–0.79, P = 0.011) and (ORoften/no = 0.45, 95%CI 0.21–0.96, P = 0.041) was a significant protective factor for TC.
Discussion
To the best of our knowledge, this is the first case–control study on such a wide range of health, social, and behavioral factors to investigate the relationships between perceived life stresses, short-temperedness, and sleep quality with the risk of TC. In the first phase of this study on the same participants, several factors, mainly radiation, history of thyroid diseases, family history of thyroid diseases and thyroid cancer were related to TC [12]. The results of the present study showed that having stress in everyday life and being short-tempered increase the risk of developing thyroid cancer. In addition, having a good quality sleep appeared to be a protective factor for this type of cancer.
Our study showed that having stress in life increases the risk of TC. Several previously published studies suggested that stress can increase cancer risk by weakening our immune system [3, 5, 22]. In addition, it appeared that chronic stress activates the hypothalamic–pituitary–adrenal (HPA) axis and the sympathetic nervous system (SNS), functions that may cause shrieked and dysfunctional prefrontal cortex and the hippocampus, alterations that may cause tumorigenesis [3]. Mizokami et al. showed that psychological and physiological stressors cause various immunological changes that affect the body's immune system through the nervous and endocrine systems. These changes may increase the susceptibility of individuals to autoimmune diseases [23]. It is also reported that, in addition to a decrease in immune function, chronic stress can also cause inflammatory response, a significant contributor to tumorigenesis in the body [3]. Our study result is in line with that from a Korean study that reported that stress in patients with TC was significantly higher than in healthy controls [24]. Li et al. showed that people with benign nodules have less mental distress than TC patients [25].
Despite the results of current and very few previously published studies, due to the limited knowledge on the involvement of stressful life in developing cancer, we need more studies to understand the precise role of this common and important factor in TC in different populations.
The results of our study also showed that short-temperedness increases the risk of developing TC. Augustine et al. showed that people with more negative personality traits are at a higher risk of lung cancer in the early years of their life [26]. On the other hand, another study showed no association between personality and risk of cancer or its mortality [27]. Similarly, Nakaya et al. found no association between personality traits, such as extraversion and neuroticism and risk or prognosis of cancer [28]. Given these conflicting findings, the role of personality in causing cancer is controversial and need to be examined in more precise approaches.
The importance of quality sleep in reducing the risk of TC is another rare and significant finding of the present study. According to the results, good quality sleep has a protective role in the development of TC. Raising the risk of reverse causation, several studies on the same subject used cross-sectional interpretation to study the association. For example, He et al. showed that sleep disorder is more common in patients with thyroid cancer. It is possible that fear and psychological consequences of being diagnosed with cancer, caused major emotional problems and insomnia [29]. Another study showed that insomnia is one of the most common problems in patient with TC patients [30]. However, similar to the current study, in a retrospective view, a study on women found that those with sleep disorders had a significantly higher risk of TC than women with no sleeping problem [14]. One potential clue (though not clinically relevant) to search for the mechanism throughout which sleep disorder may increase the risk of TC is that thyroid hormones (T4 and TSH) are increased in poor sleep [31], suggesting a tight association between sleep quality and thyroid function. Another possible clue for the observed association is that sleep disorders can lead to immune dysfunction and suppression of the immune system [32]. In addition, it is believed that the complexity of hormonal synthesis, unique oligoelement requirements, and the specific capabilities of the thyroid cell can predispose the thyroid to autoimmune diseases [33]. For example, Hashimoto's autoimmune disease is associated with elevated TSH levels, decreased thyroxin, and increased antithyroid peroxidase (anti-TPO) antibodies [34]. Accordingly, sleep disorder can suppress immune response through negatively affecting the physiological functioning and circadian rhythms in the endocrine system [35]. On the other hand, other researchers reported an association between subclinical hypothyroidism and poor sleep quality [36]. This may suggest the presence of reverse causation in the associations detected by the current study. However, regarding the fact that we specifically asked for the status of the participants from their life well (years) before the occurrence of the first symptoms, reverse causation is highly improbable.
Of the limitations of the present study is the potential of recall bias as at the start of the interview we insisted that all questions regard the status of the participants during the normal life before diagnosis of the disease. However, we believe that the status of the interested conditions are easily and reliably memorable [5]. Another limitation of our study was the difficulty of accessing patients and controls. The problem was addressed with using the national health registry database and the help of health nurses in the health centers with which the participants were registered. Finally, the study design prevents us from making any causal inference and further studies with ability to explore causal associations are recommended before making any practical application of the results.
Conclusion
This case–control study suggested that stressful life and short-temperedness raise the risk of TC. We also reported that quality sleep might protect individuals from developing TC. Due to the importance of the role of quality sleep in health and chronic diseases, implementation of effective programs for affected individuals is highly recommended. We believe helping and training individuals to have a quality sleep, especially among high-risk individuals or even patients, is a potentially good step toward prevention and better prognosis of TC cancer. However, it is necessary to implement more studies to evaluate the effect of interventions to reduce stress in life and to control short-temperedness and sleep disorders in reducing the risk of different types of cancer including TC.
Availability of data and materials
The data that support the findings of this study are not publicly available due to its being the intellectual property of Shiraz University of Medical Sciences but is available from the corresponding author on reasonable request.
References
Leggett A, Burgard S, Zivin K (2016) The impact of sleep disturbance on the association between stressful life events and depressive symptoms. J Gerontol B Psychol Sci Soc Sci 71(1):118–128
Zhang S, Xie L, Yu H, Zhang W, Qian B (2019) Association between nighttime-daytime sleep patterns and chronic diseases in Chinese elderly population: a community-based cross-sectional study. BMC Geriatr 19(1):1–10
Dai S, Mo Y, Wang Y, Xiang B, Liao Q, Zhou M et al (2020) Chronic stress promotes cancer development. Front Oncol 10:1492
Kruk J, Aboul-Enein BH, Bernstein J, Gronostaj M (2019) Psychological stress and cellular aging in cancer: a meta-analysis. Oxid Med Cell Longev. https://doi.org/10.1155/2019/1270397
Dianatinasab M, Fararouei M, Mohammadianpanah M, Zare-Bandamiri M, Rezaianzadeh A (2017) Hair coloring, stress, and smoking increase the risk of breast cancer: a case-control study. Clin Breast Cancer 17(8):650–659
La Vecchia C, Malvezzi M, Bosetti C, Garavello W, Bertuccio P, Levi F et al (2015) Thyroid cancer mortality and incidence: a global overview. Int J Cancer 136(9):2187–2195
Khodamoradi F, Ghoncheh M, Mehri A, Hassanipour S, Salehiniya H (2018) Incidence, mortality, and risk factors of thyroid cancer in the world: a review. World Cancer Res J 5(2):9
Cao W, Chen H-D, Yu Y-W, Li N, Chen W-Q (2021) Changing profiles of cancer burden worldwide and in China: a secondary analysis of the global cancer statistics 2020. Chin Med J 134(7):783
Li M, Brito JP, Vaccarella S (2020) Long-term declines of thyroid cancer mortality: an international age–period–cohort analysis. Thyroid 30(6):838–846
Safavi A, Azizi F, Jafari R, Chaibakhsh S, Safavi AA (2016) Thyroid cancer epidemiology in Iran: a time trend study. Asian Pac J Cancer Prev 17(1):407–412
Vaccarella S, Franceschi S, Bray F, Wild CP, Plummer M, Dal Maso L (2016) Worldwide thyroid-cancer epidemic? The increasing impact of overdiagnosis. N Engl J Med 375(7):614–617
Parad MT, Fararouei M, Mirahmadizadeh AR, Afrashteh S (2021) Thyroid cancer and its associated factors: a population-based case-control study. Int J Cancer 149(3):514–521
Liu Y, Su L, Xiao H (2017) Review of factors related to the thyroid cancer epidemic. Int J Endocrinol. https://doi.org/10.1155/2017/5308635
Luo J, Sands M, Wactawski-Wende J, Song Y, Margolis KL (2013) Sleep disturbance and incidence of thyroid cancer in postmenopausal women the Women’s Health Initiative. Am J Epidemiol 177(1):42–49
Helmreich DL, Tylee D (2011) Thyroid hormone regulation by stress and behavioral differences in adult male rats. Horm Behav 60(3):284–291
Lou X, Wang H, Tu Y, Tan W, Jiang C, Sun J et al (2021) Alterations of sleep quality and circadian rhythm genes expression in elderly thyroid nodule patients and risks associated with thyroid malignancy. Sci Rep 11(1):1–12
Von Ruesten A, Weikert C, Fietze I, Boeing H (2012) Association of sleep duration with chronic diseases in the European Prospective Investigation into Cancer and Nutrition (EPIC)-Potsdam study. PLoS ONE 7(1):e30972
Liu Y, Wheaton AG, Chapman DP, Croft JB (2013) Sleep duration and chronic diseases among US adults age 45 years and older: evidence from the 2010 Behavioral Risk Factor Surveillance System. Sleep 36(10):1421–1427
Roshandel G, Ghanbari-Motlagh A, Partovipour E, Salavati F, Hasanpour-Heidari S, Mohammadi G et al (2019) Cancer incidence in Iran in 2014: results of the Iranian National Population-based Cancer Registry. Cancer Epidemiol 61:50–58
Hardy SE, Concato J, Gill TM (2002) Stressful life events among community-living older persons. J Gen Intern Med 17(11):841–847
Bos SC, Macedo A, Marques M, Pereira AT, Maia BR, Soares MJ et al (2013) Is positive affect in pregnancy protective of postpartum depression? Rev Bras Psiquiatr 35(1):5–12
Li J, Zhang B, Bai Y, Liu Y, Zhang B, Jin J (2020) Health-related quality of life analysis in differentiated thyroid carcinoma patients after thyroidectomy. Sci Rep 10(1):1–7
Mizokami T, Wu Li A, El-Kaissi S, Wall JR (2004) Stress and thyroid autoimmunity. Thyroid 14(12):1047–1055
Kim M, Hwang SY (2021) Influence of sleep quality, coffee consumption, and perceived stress on the incidence of thyroid cancer in healthy Korean adults. Korean J Adult Nurs 33(2):125–133
Li R, Li G, Wang Y, Bao T, Lei Y, Tian L et al (2021) Psychological distress and sleep disturbance throughout thyroid nodule screening, diagnosis, and treatment. J Clin Endocrinol Metab 106(10):e4221–e4230
Augustine AA, Larsen RJ, Walker MS, Fisher EB (2008) Personality predictors of the time course for lung cancer onset. J Res Pers 42(6):1448–1455
Jokela M, Batty GD, Hintsa T, Elovainio M, Hakulinen C, Kivimäki M (2014) Is personality associated with cancer incidence and mortality? An individual-participant meta-analysis of 2156 incident cancer cases among 42 843 men and women. Br J Cancer 110(7):1820–1824
Nakaya N, Bidstrup PE, Saito-Nakaya K, Frederiksen K, Koskenvuo M, Pukkala E et al (2010) Personality traits and cancer risk and survival based on Finnish and Swedish registry data. Am J Epidemiol 172(4):377–385
He Y, Meng Z, Jia Q, Hu F, He X, Tan J et al (2015) Sleep quality of patients with differentiated thyroid cancer. PLoS ONE 10(6):e0130634
Singer S, Lincke T, Gamper E, Bhaskaran K, Schreiber S, Hinz A et al (2012) Quality of life in patients with thyroid cancer compared with the general population. Thyroid 22(2):117–124
Nazem MR, Bastanhagh E, Emami A, Hedayati M, Samimi S, Karami M (2020) The relationship between thyroid function tests and sleep quality: cross-sectional study. Sleep Sci. https://doi.org/10.5935/1984-0063.20200050
Patel SR, Zhu X, Storfer-Isser A, Mehra R, Jenny NS, Tracy R et al (2009) Sleep duration and biomarkers of inflammation. Sleep 32(2):200–204
Saranac L, Zivanovic S, Bjelakovic B, Stamenkovic H, Novak M, Kamenov B (2011) Why is the thyroid so prone to autoimmune disease? Horm Res Paediatr 75(3):157–165
Mincer DL, Jialal I (2020) Hashimoto thyroiditis. In: StatPearls. StatPearls Publishing, Treasure Island
Bollinger T, Bollinger A, Oster H, Solbach W (2010) Sleep, immunity, and circadian clocks: a mechanistic model. Gerontology 56(6):574–580
Song L, Lei J, Jiang K, Lei Y, Tang Y, Zhu J et al (2019) The association between subclinical hypothyroidism and sleep quality: a population-based study. Risk Manag Healthc Policy 12:369
Acknowledgements
The present study is a part of the M.Sc. thesis (factors associated with thyroid cancer in K&B province) written by Mohammad Parad under the supervision of professor Mohammad Fararouei.
Funding
This study was financially supported by Shiraz University of Medical Sciences, Shiraz, Iran. (Grant number: 2668).
Author information
Authors and Affiliations
Contributions
MP was responsible data analysis and contributed to the data collection; AM was responsible for confirmation and interpretation of Medical files and manuscripts preparation; MF gave the idea of research, responsible for coordination and management of the project, data analysis and critically reviewed the manuscript, SA was responsible for data analysis and preparation of the manuscript. All authors have read and approved the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no competing interests.
Ethics approval
The study protocol was reviewed and approved by ethical commttee of Shiraz University of Medical Sciences.
Consent to participate
Because of the illiteracy of a considerable number of the patients, verbal consent was obtained from the participants.
Consent for publication
Written informed consent for publication was obtained from each participant.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Novelty and impact: This is the first study on the factors affecting the risk of TC include stress, quality of sleep and short-temperedness in general population of a province with a very high incidence in Iran We have shown that stress and short-temperedness can increase the risk of developing TC. On the other hand having a quality sleep seems to be a protective factor.
Rights and permissions
About this article

Cite this article
Afrashteh, S., Fararouei, M., Parad, M.T. et al. Sleep quality, stress and thyroid cancer: a case–control study. J Endocrinol Invest 45, 1219–1226 (2022). https://doi.org/10.1007/s40618-022-01751-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40618-022-01751-4