
Abstract
Purpose
To examine the association of epicardial and pericardial fat volume (EFV, PFV) with cardiovascular risk factors and kidney function in Native Americans of southwestern heritage with youth and early adult onset type 2 diabetes mellitus (T2DM) versus healthy controls.
Methods
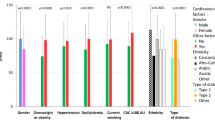
Using computed tomography, we quantified EFV and PFV in 149 Native Americans (92 women, 57 men), 95 of which had T2DM (38 diagnosed prior to age 20 years). Duration of T2DM, mean carotid arterial mass (AM), coronary artery calcification (CAC), IL-6, and estimated glomerular filtration rate eGFRcr(CKD-EPI) were measured.
Results
EFV and PFV were associated with BMI (r = 0.37, p < 0.0001; r = 0.26, p = 0.001) and did not differ between onset age-groups and controls (p > 0.05). EFV was associated with AM only in controls (r = 0.51, p < 0.0001). After adjustment for BMI, T2DM duration, HbA1C, age, and sex, EFV was a predictor of CAC and IL-6 concentrations in early adult onset T2DM (β = 0.05 ± 0.02 cm3, p = 0.03; β = 0.05 ± 0.01 pg/ml/cm3, p = 0.002). EFV and PFV were independent predictors of reduced eGFRcr(CKD-EPI) in the youth onset T2DM group (β = −0.3 ± 0.08 ml/min/cm3, p = 0.001; β = −0.25 ± 0.05 ml/min/cm3, p < 0.0001).
Conclusions
Epicardial fat volume may be a risk factor for heart disease in individuals with early adult onset T2DM and a predictor of decreased kidney function in individuals with youth onset T2DM.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Epicardial adipose tissue (EAT) has emerged as a local and systemic risk factor for cardiovascular and metabolic diseases [1]. Located within the pericardium, epicardial fat is the “visceral fat” of the heart, while pericardial adipose tissue (PAT) is located externally attached to the parietal layer of the pericardium [2].
Several studies have found a positive association between epicardial fat volume and coronary [3, 4], and extracranial carotid artery atherosclerosis [5], independent of other cardiovascular risk factors. In patients with type 2 diabetes mellitus (T2DM), trans- and conjugated fatty acids in epicardial fat may accelerate plaque formation [6]. The expression and secretion of inflammatory cytokines, mediators, and other bioactive molecules indicate that epicardial fat acts as an endocrine organ [3, 7], sharing many of the pathophysiological properties of other ectopic fat depots such as abdominal visceral adipose tissue (VAT). In fact, epicardial fat and VAT volumes are highly correlated [8]. Increased inflammatory cell infiltration of EAT and PAT is observed in patients with coronary artery disease (CAD) [9, 10]. Furthermore, EAT is associated with more traditional metabolic risk factors, such as body mass index, hypertension, hyperlipidemia, impaired fasting glucose, and especially, T2DM [8].
Chronic kidney disease (CKD), the possible result of the prevalence of one or more of the above risk factors [11], is associated with an increased prevalence of coronary atherosclerosis [12, 13]. Interestingly, increased volumes of EAT in patients with chronic kidney disease (stages 3–5) are a better predictor of the risk of cardiovascular events than abdominal VAT [14]. Inflammation, also in EAT, could possibly be a link between the pathogenesis of CAD and chronic kidney disease. Two recent studies independently demonstrated that EAT thickness was significantly greater in patients on hemodialysis compared with healthy controls and positively correlated with hemodialysis duration [15, 16].
Individuals who develop T2DM in childhood and adolescence are affected by the microvascular complications of diabetes mellitus (i.e., retinopathy and nephropathy) in early adulthood [17]. In Native Americans of southwestern heritage, the prevalence of T2DM in youth (age < 20 years) doubled between 1967 and 1998 [18]. Kidney disease is a major complication in this population, with 93% of end-stage renal disease attributable to T2DM [19]. Onset of T2DM in Native Americans of southwestern heritage younger than 20 years is associated with a nearly fivefold increase in the incidence of end stage renal disease (ESRD) between the ages of 25 and 54 years, compared with those with later onset of diabetes mellitus [23]. The incidence of ESRD and mortality increases with age and with duration of T2DM in this population [20].
In this study, we examined the impact of epi- and pericardial fat volume on cardiovascular risk factors and kidney function in three groups of Native Americans of southwestern heritage: those with youth onset (age < 20 years) T2DM, those with early adult onset T2DM, and healthy controls. We hypothesized that fat volumes would be positively associated with risk factors for heart disease and negatively associated with measures of kidney function in youth onset (age less than 20 years), rather than in early adult onset (age between 20 and 40 years) T2DM or healthy individuals.
Patients and methods
Study population
Between 1965 and 2007, Native Americans of southwestern heritage participated in a longitudinal study of T2DM and its complications (NCT00339482). Individuals greater than 5 years were invited to have an examination including an oral glucose tolerance test (OGTT) as frequently as every 2 years, regardless of health status. T2DM was diagnosed by OGTT according to American Diabetes Association guidelines [21] or by documented previous clinical diagnosis confirmed by review of the medical records. Based on these diagnosis dates, from 2001 to 2003, we invited individuals diagnosed with diabetes at age < 40 years and control subjects with normal glucose regulation (NGR) of similar age to participate in additional studies examining prevalence of cardiovascular disease and risk factors. NGR was determined by existing criteria: fasting plasma glucose < 110 mg/dl and 2 h plasma glucose < 140 mg/dl. A total of 111 subjectswith diabetes were recruited based on the age of diagnosis and current age in 5 year blocks (i.e., diabetes diagnosis age 10–14 years but current age 20–24 years, 25–29 years, etc.) along with 60 controls approximately matched for current age at exam. Of these, 95 with diabetes and 54 controls had imaging data (computed tomography of the heart and carotid ultrasound). Seven of the 54 control individuals would be defined as having impaired glucose tolerance according to current criteria [22]. At each examination, participants completed questionnaires on T2DM and medical history (including Rose Angina questionnaire). Fasting blood samples were drawn for plasma glucose, hemoglobin A1C (HbA1c), lipid, serum creatinine, and inflammatory-, and hemostatic markers. The physical examination included standardized measurements of height and body weight, systolic- (SBP) and diastolic blood pressure (DBP), measured in the supine position in the right arm using an appropriate-sized cuff for arm circumference. SBP and DBP were recorded seated after 5 min to the nearest 2 mm Hg using the first and fifth Korotkoff sound. The mean arterial pressure (MAP), a well-established marker of cardiovascular risk [23], was calculated as: (2 × DBP + SBP)/3. This study was approved by the NIDDK Institutional Review Board. All participants gave written and verbal informed consent for the studies.
Assessments of subclinical atherosclerotic indices and kidney function
All subjects underwent electron beam computerized tomography (EBCT) scan using the GE Model Imatron 150 Scanner (Arizona Heart Institute, Phoenix, AZ). Scans were obtained during one breath-holding sequence in 3 mm slices using a 100 ms sweep time triggered by ECG signals at 80% of the RR interval. Variability was reduced by doing two scans on each subject, and the results were averaged. Evidence of calcification was defined as four continuous pixels with Hounsfield units > 130. Agatston score was calculated using a standard formula that accounts for area (number of pixels) and intensity (maximum Hounsfield units) [24].
The carotid ultrasound was done bilaterally in the M-mode by two well-trained technicians to assess intima-media thickness (IMT) and the presence of plaque (discrete focal thickening) separately. Media thickness of the near and the far walls of the common carotid artery were measured in the end-diastolic and end-systolic carotid diameters. These ultrasound results were interpreted by a trained reader without knowledge of individual clinical status. Mean IMTs were calculated in each subject from bilateral measurements and mean of two values was used in the analysis. Mean carotid arterial mass (AM) was calculated based on the measured IMT and lumen diameter in diastole (DD) using the formula as: AM = π [(DD + 2 × IMT)/2]2 −π [(DD/2)]2.
All blood samples were stored at − 80 °C until the day of assay. Plasma glucose concentration was measured by the hexokinase method (Ciba-Corning, Palo Alto, CA). Serum creatinine (SCr) was measured by a modified Jaffé reaction with calibration traceable to an isotope-dilution mass spectrometry measurement procedure [25]. Glomerular filtration rate was estimated from SCr using the CKD-EPI Creatinine Equation (2009, [26]) (eGFRcr(CKD-EPI)), accounting for differences in age and gender. Total cholesterol, triglycerides (TG), and HDL cholesterol (HDL-C) were measured by the enzymatic method (Ciba-Corning, Palo Alto, CA), then LDL-cholesterol (LDL-C) was estimated using the Friedewald equation, for those with TG < 400 mg/dl. Interleukin-6 (IL-6) was measured by ultra-sensitive ELISA with CV of 6.3%. Hemoglobin A1C was measured by A1C 2.2 Plus Glycohemoglobin Analyzer (TOSOH Medics, Inc.). C-reactive protein (CRP) was measured by a colorimetric competitive enzyme-linked immunosorbent assay ELISA with CV of 5.14%.
Quantification of epicardial and pericardial adipose tissue
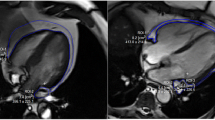
Fat volumes were quantified using the Osirix Imaging Software v6.5.2. In each computed tomography slice, a semi-automatic selection by radio density window ranging from − 30 to − 200 Hounsfield units was utilized. Tissues within this density threshold and located within the pericardium were selected, yielding a quantifiable total EFV. Pericardial adipose tissue (PAT), located externally attached to the parietal layer of the pericardium, was measured in the same manner. The pulmonary artery bifurcation served as the upper anatomical limit and the left ventricular apex served as lower boundary for measurement of EFV and pericardial fat volume (PFV). Inter-observer variability for EFV measurements was 8.3% and 11.8% for PFV, respectively.
Statistical analysis
Investigated variables were normally distributed and are described using means and standard deviations. Significant correlations between EFV, PFV and continuous variables were adjusted for the association between EFV, PFV, and BMI in all groups (whole group, healthy subjects, subjects with T2DM, subjects with youth onset, and early adult onset T2DM), by calculating the remaining variance (i.e., the residuals or the differences between observed and expected) of these variables after accounting for BMI. Differences in average EFV and PFV between all men and women were analyzed using Student's t test. Differences between youth-, early adult onset T2DM, and healthy controls were assessed by one-way ANOVA. Significant differences (p <0.05) between the three groups were further investigated using post hoc analysis (Tukey's studentized range test). The associations between EFV, PFV, AM, IL-6, CRP, SBP, DBP, MAP, and eGFRcr(CKD-EPI) were assessed by means of Pearson analysis, adjusted for BMI, and BMI and HbA1C (to adjust for diabetes control) by creating the respective residuals, as described above. The associations between EFV, PFV, and IL-6 were analyzed in all groups after adjustments for differences in BMI, duration of T2DM, age, and sex. Logistic regression was used to determine whether EFV or PFV was positive predictors of the presence of CAC, after adjusting for differences in BMI, HbA1C as a marker for T2DM control, duration of T2DM, age, and sex in the whole group. Logistic regression, adjusting for differences in BMI, HbA1C, age, and sex, was used to determine whether EFV was a positive predictor of the presence of CAC. Linear regression models, adjusted for differences in duration of T2DM, BMI and MAP, were also employed to investigate the associations of EFV, PFV and eGFRcr(CKD-EPI).
Individuals who develop T2DM in childhood and adolescence are affected by the microvascular complications of diabetes mellitus in early adulthood [17] and the onset of T2DM in Native Americans of southwestern heritage younger than 20 years is associated with a nearly fivefold increase in the incidence of end stage renal disease between the ages of 25 and 54 [20]. There were significant interactions (p < 0.05) between the associations of EFV (adjusted for BMI by creating residuals) and AM, CAC, IL-6, eGFRcr(CKD-EPI), and PFV and CAC, eGFRcr(CKD-EPI) by youth onset-versus early adult onset T2DM group.
Statistical analysis was performed using SAS statistical software (SAS E-guide 4.2 and SAS version 9.2; SAS Institute, Cary, NC, USA). Alpha was set at 0.05. As the study was primarily exploratory in nature, adjustments were not made for multiple comparisons.
Results
Summary measures for continuous and discrete variables of the study population are shown in Table 1. Both EFV and PFV were positively associated with BMI in the whole group (r = 0.37, p < 0.0001 (Fig. 1); r = 0.26, p = 0.001), in healthy subjects (r = 0.31, p = 0.02; r = 0.32, p = 0.02), in all subjects with T2DM (r = 0.41, p < 0.0001; r = 0.22, p = 0.03), in youth onset—(r = 0.5, p < 0.0001; r = 0.36, p = 0.03), and early adult onset T2DM for EFV only (r = 0.30, p = 0.02; r = 0.06, p = 0.7). Because of the strong correlation of BMI with EFV and PFV, all further analyses of associations between EFV, PFV and variables of interest were done after adjustment for BMI.

Correlation between body mass index (BMI) and epicardial fat volume. Figure 1 shows the correlation between body mass index (BMI) and epicardial fat volume (r = 0.37, p < 0.0001)
PFV, but not EFV, was greater in men compared to women (62.6 cm3 ± 38.0 vs. 37.9 cm3 ± 24.8, p < 0.0001; 78.3 cm3 ± 26.7 vs. 70.4 cm3 ± 24.6, p = 0.09); however, after adjustment for BMI both were greater in men compared to women (p < 0.0001; p = 0.006). EFV and PFV did not differ between groups with youth onset-, early adult onset T2DM, and healthy controls (one-way ANOVA p > 0.05); this was also true after adjusting EFV and PFV for BMI.
In the group of all subjects, EFV was positively associated with AM (r = 0.21, p = 0.014), IL-6 concentrations (r = 0.17, p < 0.05), DBP (r = 0.23, p = 0.0048), and MAP (r = 0.22, p = 0.01), but only showed a positive trend for the association with SBP (r = 0.15, p = 0.07); further adjustments for HbA1C did not change these results. PFV was positively associated with AM (r = 0.3, p = 0.0003), IL-6 (r = 0.19, p = 0.03), DBP (r = 0.32, p < 0.0001), SBP (r = 0.26, p = 0.0017), and MAP (r = 0.32, p < 0.0001), in the group of all subjects, and adjustments for HbA1C did not alter the results. There were no associations (p > 0.05) between EFV or PFV, and CRP in the group of all subjects; further adjustments for HbA1C did not change these results. There was no association between EFV and eGFRcr(CKD-EPI) (r = −0.08, p = −0.33), but a negative association between PFV and eGFRcr(CKD-EPI) (r = −0.17, p = −0.034) was observed in the group of all subjects.
Sub-analyses showed that EFV was associated with AM only in the healthy controls (r = 0.51, p < 0.0001) and that EFV was positively associated with IL-6 in individuals with early adult onset T2DM (r = 0.38, p = 0.006). Further adjustment for differences in duration of T2DM, HbA1C, age, and sex in linear regression models showed that EFV was predictive of IL-6 in subjects with early adult onset T2DM (β = 0.05 ± 0.01 pg/ml/cm3, p = 0.002, Fig. 2), but not in youth onset subjects (β = −0.018 ± 0.02 pg/ml/cm3, p = 0.36). In a logistic regression model of the whole group, adjusting for differences in BMI, HbA1C, duration of T2DM, age, and sex, EFV was an independent positive predictor of the presence of CAC (β = 0.034 ± 0.01 cm3, p = 0.0024; PFV: p = 0.1). Adding LDL-Cholesterol and MAP (risk factors for cardiovascular disease) to the model did not change the results (β = 0.035 ± 0.01 cm3, p = 0.0058; PFV: p = 0.42). Parameter estimates for EFV were similar after stratification by T2DM versus control and age of onset of T2DM (β = 0.04 ± 0.02 cm3, p = 0.008; β = 0.04 ± 0.03 cm3, p = 0.15), but statistically significant only for T2DM. In youth versus early adult onset T2DM, EFV was a positive predictor of the presence of CAC only in early adult onset, but not youth onset of T2DM (β = 0.05 ± 0.02 cm3, p = 0.03; β = 0.06 ± 0.06 cm3, p = 0.27). Stratification by T2DM status and onset showed that PFV was not an independent predictor of CAC (controls: β = 0.03 ± 0.02 cm3, p = 0.065; T2DM: β = 0.01 ± 0.01 cm3, p = 0.32; youth onset: β = 0.03 ± 0.04 cm3, p = 0.56; early adult onset: β = 0.004 ± 0.02 cm3, p = 0.8).

Correlation of epicardial fat with Interleukin-6. Figure 2 correlation of epicardial fat (adjusted for BMI, HbA1C, duration of T2DM, age, and sex) with Interleukin-6 in the group of early adult onset T2DM (r = 0.39, p = 0.005)
In two linear regression models adjusted for differences in duration of T2DM, BMI and MAP, EFV and PFV were independent negative predictors of eGFRcr(CKD-EPI) only in the youth onset T2DM group (β = −0.3 ± 0.08 ml/min/cm3, p = 0.001; β = −0.25 ± 0.05 ml/min/cm3, p < 0.0001; early adult onset: β = 0.025 ± 0.06 cm3, p = 0.7; β = 0.01 ± 0.01 cm3, p = 0.79, Fig. 3), adjustments for HbA1C did not alter the results in either model. Besides EFV and PFV, duration of T2DM was the only other independent predictor of eGFRcr(CKD-EPI), in both the youth onset (model with EFV: β = −1.7 ± 0.37 cm3, p = 0.0001; model with PFV: β = −1.2 ± 0.33 cm3, p = 0.001), and early adult onset T2DM (model with EFV: β = −0.7 ± 0.35 cm3, p < 0.05; model with PFV: β = −0.7 ± 0.35 cm3, p < 0.05) groups.

Correlations between epicardial fat volume and glomerular filtration rate. Figure 3 Correlations between epicardial fat volume and glomerular filtration rate in the groups of youth onset T2DM (r = − 0.43, p = 0.007) and early adult onset T2DM (r = 0.04, p = 0.75), each including adjustments for differences in duration of T2DM, body mass index and mean arterial blood pressure
Discussion
In this study, epicardial fat volume was associated with interleukin-6 and coronary artery calcification, both risk factors for heart disease, in individuals with early adult onset T2DM, defined as age of onset less than 40 years (but greater than 20 years). EFV was also a predictor of decreased kidney function (eGFRcr(CKD-EPI)) in individuals with youth onset T2DM, defined as age less than 20 years.
An association of inflammatory markers with EFV and PFV is consistent with previous reports, including one study from the framingham heart study [7]. Both epicardial and pericardial fat are visceral fat depots with pericardial fat sharing an embryonic origin with visceral adipose tissue, known to be associated with systemic inflammation [27]. Atherosclerosis has been characterized as a chronic inflammatory disease that frequently involves coronary artery calcification [28]. Epicardial fat produces multiple bioactive factors such as interleukins and chemokines, adiponectin, and TNF-α [3], which may locally interact with the coronary arteries [29, 30]. In addition, it has been proposed that perivascular fat might directly contribute to perivascular inflammation [31] and smooth muscle cell proliferation [32]. The Framingham Heart Study also observed associations between EFV and CAC, and EFV and diabetes [8]. It is notable that the mean age of participants in the Framingham study was 63 years, while we found the same associations in a group of subjects diagnosed with diabetes prior to the age of 40 years. Furthermore, we were able to specifically investigate whether age of onset influenced this association, finding that when examined at the same age, EFV is a predictor of CAC in those with early adult onset T2DM, but not youth onset T2DM or healthy controls studied. We originally hypothesized that these associations would be found primarily in the youth onset group, due to the longer duration of T2DM, but these associations were independent of the T2DM duration. This indicates that the pathophysiology of vascular disease may differ by age. Chronic inflammation in epicardial fat may directly influence the pathogenesis of coronary atherosclerosis in individuals with early adult onset T2DM but in a less direct manner in youth onset T2DM. The latter group does develop significant microvascular disease at a young age [17] and we did find an inverse association between EFV and eGFR. While EFV might have an effect on renal disease in youth, and renal disease is a precursor to macrovascular disease, it is more likely that EFV is marker of metabolic syndrome predisposing to both conditions. EFV was associated with carotid arterial mass only in the healthy control group. Progression of atherosclerosis can be categorized into six grades in which increased IMT and subsequently AM represent earlier stages while the presence of CAC follows at later stages [33]. Thus, in the absence of hyperglycemia, EFV may still play a role in early stage atherosclerosis.
EFV was associated with IL-6 concentration, in the early adult onset group only. In agreement with our findings, epicardial fat is known to be a source of inflammatory metabolites [3, 7, 34]. Several studies have shown that IL-6 is an upstream inflammatory cytokine that plays a central role in propagating the downstream inflammatory response responsible for atherosclerosis [35]. Individuals with an IL-6 receptor variant that impairs usual IL-6 signaling were found to have a decreased risk for coronary heart disease [36].
Diabetes mellitus in Native Americans of southwestern heritage is entirely T2DM [37]. Unlike retinopathy, nephropathy in youth onset T2DM occurs at the same frequency as for adult onset T2DM, indicating that younger age does not offer the same protection from progressive diabetic kidney disease as it does from diabetic retinopathy [17]. Furthermore, the higher rates of ESRD in young- and middle-aged Native American adults of southwestern heritage with youth onset T2DM may contribute to a rise in cardiovascular complications in these age groups [38]. The underlying mechanisms of the association of EFV, PFV, and renal dysfunction in general and especially in subjects with youth onset T2DM are not well understood. A prominent candidate is metabolic syndrome, which is linked to epicardial fat storage [1] and is a strong predictor for new onset of chronic kidney disease [39]. Epicardial fat might just be a marker of metabolic syndrome or exacerbate the risk of metabolic syndrome on kidney disease.
The cross-sectional design of our study cannot determine causal relations between the investigated risk factors for heart disease and markers of renal function. The Native Americans of southwestern heritage who participated in this study are from a relatively small population, so even though the prevalence of early adult- and youth onset T2DM is relatively high in this population, the total numbers of those with youth and early adult onset are not. However, the more exact dates of diagnosis in this study with subjects diagnosed at research visits or by comprehensive medical record review are a strength. The relatively small sample size of our study might have limited the ability to detect modest associations between epi- and pericardial adipose tissue and risk factors for heart disease and impaired renal function. In this light, our findings are even more noteworthy. Modest associations, e.g., between EFV and eGFR in the group of early adult onset T2DM (Fig. 3) might be underrepresented due to the small sample size and resulting lack of statistical power.
Epicardial adipose tissue volume is associated with heart disease in individuals with early adult onset T2DM and with decreased kidney function in individuals with youth onset T2DM. Our findings indicate that epicardial fat may be involved in the pathophysiology of vascular disease but, due to age-related innate differences in epicardial fat biology, may have different effects across age spans.
References
Iacobellis G (2014) Epicardial adipose tissue in endocrine and metabolic diseases. Endocrine 46(1):8–15
Iozzo P (2011) Myocardial, Perivascular, and Epicardial Fat. Diabetes Care 34(Supplement 2):S371–S379
Mazurek T, Zhang L, Zalewski A, Mannion JD, Diehl JT, Arafat H et al (2003) Human epicardial adipose tissue is a source of inflammatory mediators. Circulation 108(20):2460–2466
Konishi M, Sugiyama S, Sugamura K, Nozaki T, Ohba K, Matsubara J et al (2010) Association of pericardial fat accumulation rather than abdominal obesity with coronary atherosclerotic plaque formation in patients with suspected coronary artery disease. Atherosclerosis 209(2):573–578
Bos D, Shahzad R, van Walsum T, van Vliet LJ, Franco OH, Hofman A et al (2015) Epicardial fat volume is related to atherosclerotic calcification in multiple vessel beds. Eur Heart J Cardiovasc Imaging 16:1264–1269
Pezeshkian M, Mahtabipour M-R (2013) Epicardial and subcutaneous adipose tissue Fatty acids profiles in diabetic and non-diabetic patients candidate for coronary artery bypass graft. BioImpacts 3(2):83–89
Tadros TM, Massaro JM, Rosito GA, Hoffmann U, Vasan RS, Larson MG et al (2010) Pericardial fat volume correlates with inflammatory markers: the framingham heart study. Obesity 18(5):1039–1045
Rosito GA, Massaro JM, Hoffmann U, Ruberg FL, Mahabadi AA, Vasan RS et al (2008) Pericardial fat, visceral abdominal fat, cardiovascular disease risk factors, and vascular calcification in a community-based sample: the framingham heart study. Circulation 117(5):605–613
Konishi M, Sugiyama S, Sato Y, Oshima S, Sugamura K, Nozaki T et al (2010) Pericardial fat inflammation correlates with coronary artery disease. Atherosclerosis 213(2):649–655
Hirata Y, Kurobe H, Akaike M, Chikugo F, Hori T, Bando Y et al (2011) Enhanced inflammation in epicardial fat in patients with coronary artery disease. Int Heart J 52(3):139–142
Saran R, Robinson B, Abbott KC, Agodoa LY, Albertus P, Ayanian J et al (2017) US renal data system 2016 annual data report: epidemiology of kidney disease in the US. Am J Kidney Dis 69(3 Suppl 1):A7–A8. https://doi.org/10.1053/j.ajkd.2016.12.004
Foley RN, Murray AM, Li S, Herzog CA, McBean AM, Eggers PW et al (2005) Chronic kidney disease and the risk for cardiovascular disease, renal replacement, and death in the United States medicare population, 1998 to 1999. J Am Soc Nephrol JASN 16(2):489–495
Kerr JD, Holden RM, Morton AR, Nolan RL, Hopman WM, Pruss CM et al (2013) Associations of epicardial fat with coronary calcification, insulin resistance, inflammation, and fibroblast growth factor-23 in stages 3–5 chronic kidney disease. BMC Nephrol 14:26
Cordeiro AC, Amparo FC, Oliveira MAC, Amodeo C, Smanio P, Pinto IMF et al (2015) Epicardial fat accumulation, cardiometabolic profile and cardiovascular events in patients with stages 3–5 chronic kidney disease. J Intern Med 278(1):77–87
Altun B, Tasolar H, Eren N, Binnetoğlu E, Altun M, Temiz A et al (2014) Epicardial adipose tissue thickness in hemodialysis patients. Echocardiography 31(8):941–946
Atakan A, Macunluoglu B, Kaya Y, Ari E, Demir H, Asicioglu E et al (2014) Epicardial fat thickness is associated with impaired coronary flow reserve in hemodialysis patients. Hemodial Int Int Symp Home Hemodial 18(1):62–69
Krakoff J, Lindsay RS, Looker HC, Nelson RG, Hanson RL, Knowler WC (2003) Incidence of retinopathy and nephropathy in youth-onset compared with adult-onset type 2 diabetes. Diabetes Care 26(1):76–81
Dabelea D, Hanson RL, Bennett PH, Roumain J, Knowler WC, Pettitt DJ (1998) Increasing prevalence of type II diabetes in American Indian children. Diabetologia 41(8):904–910
Nelson RG, Newman JM, Knowler WC, Sievers ML, Kunzelman CL, Pettitt DJ et al (1988) Incidence of end-stage renal disease in type 2 (non-insulin-dependent) diabetes mellitus in Pima Indians. Diabetologia 31(10):730–736
Pavkov ME, Bennett PH, Knowler WC, Krakoff J, Sievers ML, Nelson RG (2006) EFfect of youth-onset type 2 diabetes mellitus on incidence of end-stage renal disease and mortality in young and middle-aged pima indians. JAMA 296(4):421–426
Lillioja S, Mott DM, Spraul M, Ferraro R, Foley JE, Ravussin E et al (1993) Insulin resistance and insulin secretory dysfunction as precursors of non-insulin-dependent diabetes mellitus: prospective studies of pima Indians. N Engl J Med 329(27):1988–1992
Association AD (2005) Diagnosis and classification of diabetes mellitus. Diabetes Care 28(suppl 1):s37–s42
Safar ME, Boudier HS (2005) Vascular development, pulse pressure, and the mechanisms of hypertension. Hypertension 46(1):205–209
Agatston AS, Janowitz WR, Hildner FJ, Zusmer NR, Viamonte JM, Detrano R (1990) Quantification of coronary artery calcium using ultrafast computed tomography. J Am Coll Cardiol 15(4):827–832
Chasson AL, Grady HJ, Stanley MA (1960) Determination of creatinine by means of automatic chemical analysis. Tech Bull Regist Med Technol 30:207–212
Levey AS, Stevens LA, Schmid CH, Zhang YL, Castro AF, Feldman HI et al (2009) A new equation to estimate glomerular filtration rate. Ann Intern Med 150(9):604–612
Ho E, Shimada Y (1978) Formation of the epicardium studied with the scanning electron microscope. Dev Biol 66(2):579–585
Weissberg PL, Bennett MR (1999) Atherosclerosis—an inflammatory disease. N Engl J Med 340(24):1928–1929
Sacks HS, Fain JN (2007) Human epicardial adipose tissue: a review. Am Heart J 153(6):907–917
Yudkin JS, Eringa E, Stehouwer CDA (2005) “Vasocrine” signalling from perivascular fat: a mechanism linking insulin resistance to vascular disease. Lancet Lond Engl 365(9473):1817–1820
Henrichot E, Juge-Aubry CE, Pernin A, Pache J-C, Velebit V, Dayer J-M et al (2005) Production of chemokines by perivascular adipose tissue: a role in the pathogenesis of atherosclerosis? Arterioscler Thromb Vasc Biol 25(12):2594–2599
Barandier C, Montani J-P, Yang Z (2005) Mature adipocytes and perivascular adipose tissue stimulate vascular smooth muscle cell proliferation: effects of aging and obesity. Am J Physiol Heart Circ Physiol 289(5):H1807–H1813
Iacobellis G, Bianco AC (2011) Epicardial adipose tissue: emerging physiological, pathophysiological and clinical features. Trends Endocrinol Metab 22(11):450–457
Belcaro G, Nicolaides AN, Laurora G, Cesarone MR, De Sanctis M, Incandela L et al (1996) Ultrasound morphology classification of the arterial wall and cardiovascular events in a 6-year follow-up study. Arterioscler Thromb Vasc Biol 16(7):851–856
Hartman J, Frishman WH (2014) Inflammation and atherosclerosis: a review of the role of interleukin-6 in the development of atherosclerosis and the potential for targeted drug therapy. Cardiol Rev 22(3):147–151
Interleukin-6 receptor mendelian randomisation analysis (IL6R MR) consortium, Swerdlow DI, Holmes MV, Kuchenbaecker KB, Engmann JEL, Shah T et al (2012) The interleukin-6 receptor as a target for prevention of coronary heart disease: a mendelian randomisation analysis. Lancet Lond Engl 379(9822):1214–1224
Knowler WC, Pettitt DJ, Saad MF, Bennett PH (1990) Diabetes mellitus in the pima Indians: incidence, risk factors and pathogenesis. Diabetes Metab Rev 6(1):1–27
Pavkov ME, Sievers ML, Knowler WC, Bennett PH, Nelson RG (2004) An explanation for the increase in heart disease mortality rates in diabetic Pima Indians: effect of renal replacement therapy. Diabetes Care 27(5):1132–1136
Luk AOY, So W-Y, Ma RCW, Kong APS, Ozaki R, Ng VSW et al (2008) Metabolic syndrome predicts new onset of chronic kidney disease in 5829 patients with type 2 diabetes: a 5-year prospective analysis of the Hong Kong Diabetes Registry. Diabetes Care 31(12):2357–2361
Funding
This research was supported by the Intramural Research Program of the National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases.
Author information
Authors and Affiliations
Contributions
MR wrote the manuscript. MR and TC analyzed the data. MR, MST, TC, and JK designed the study. MR and TC quantified epicardial and pericardial adipose tissue. MR, TC, MST, and JK contributed to the interpretations of findings and commented on and edited the drafts. JK is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflict of interest.
Ethical standards
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Research involving human participants and/or animals
This article does not contain any studies with animals performed by any of the authors. This study was approved by the NIDDK Institutional Review Board.
Informed consent
All participants gave written and verbal informed consent for the studies.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Reinhardt, M., Cushman, T.R., Thearle, M.S. et al. Epicardial adipose tissue is a predictor of decreased kidney function and coronary artery calcification in youth- and early adult onset type 2 diabetes mellitus. J Endocrinol Invest 42, 979–986 (2019). https://doi.org/10.1007/s40618-019-1011-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40618-019-1011-8