
Abstract
Gestational diabetes mellitus (GDM), defined as any glucose intolerance with the onset or first recognition during pregnancy, is characterized by rising incidence, fostered by the worldwide increase of pathological nutritional status from young age. Clinical research has intended to identify potential risk factors, suggested improvements in screening strategies, and recommended the combination between promotion of an appropriate lifestyle before and during pregnancy and selected therapeutic approaches. Preventing pathological hyperglycemia could have several benefits, ranging from clinical side (reduction in the risk of adverse perinatal and long-term sequelae) to financial side (cost reduction to healthcare systems). Among risk factors recognized, deficiency in 25-hydroxyvitamin D [25(OH)D], already acknowledged as involved in calcium homeostasis, pathogenesis of cardiovascular, oncological, infective and immunity diseases, could predispose to the development of both type 1 and 2 diabetes, modifying the activity of pancreatic β-cells vitamin D (VD) receptor. In pregnant women, lower 25(OH)D concentrations have been suggested to present an inverse association with maternal glycaemia, insulin resistance, and increased risk of GDM. In spite of growing body of evidence, there is not full agreement on the therapeutic association between GDM based on VD deficiency and 25(OH)D supplementation. In the attempt to bring up-to-date the role of low VD levels on subsequent development of GDM, this narrative review, based on medium–high-quality randomized clinical trials, systematic reviews, and meta-analysis published in last decade, has a twofold purpose: firstly, to elucidate the relationship between maternal VD status and GDM; and secondly, to illuminate the impact of VD supplementation on GDM onset.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Among all obstetric complications, a rising prevalence of gestational diabetes mellitus (GDM), a disorder characterized by variable severity of glucose intolerance with onset or first recognition in pregnancy, has been reported over the years, reaching 10–15% in the world [1].
Physiologically, the pregnancy is a diabetogenic condition since the steroid hormones increase and insulin resistance occurs in peripheral tissues, as well as inflammatory cytokines secreted from both adipose tissue and placenta, can contribute to insulin resistance and pathogens of GDM [1, 2]. This physiological condition might be exacerbated by well-established risk factors for GDM, including ethnic group, advanced maternal age, hypertension prior GDM, history of miscarriage and type 2 diabetes mellitus (T2DM) in first degree, pregestational overweight and obesity, and excessive gestational weight gain (Fig. 1) [1,2,3,4].

Risk factors for the GDM development
Despite a delayed discovery, vitamin D (VD) has emerged as one of the most controversial nutrients and prohormones of the twenty-first century. If its role in calcium metabolism and bone health is undisputed, its influence on other diseases and, more in general, long-term health is debated. Predominantly, VD appears as an intriguing research topic for perinatal investigators dedicated to GDM because its status is easily modified by supplementation [5]. Besides, the clinical research, justified both by similar pathogenesis and risk factors to T2DM and by more than a decade of observational studies reporting a consistent association between low levels of VD and T2DM, proposes to consider VD insufficiency as potential trigger and, consequently, as a modifiable contributor in the etiology of GDM [6, 7].
In this review, we have described the epidemiology of GDM and the metabolic functions of VD, reported the medium–high-quality studies linking GDM to VD, including systematic reviews, meta-analyses, and results from clinical trials on VD supplementation during pregnancy for prevention and/or GDM treatment. Finally, moving from latest evidence, we emphasized the open question requiring future investigations.
Mechanisms of glucose regulation during pregnancy
In humans, a balance between adequate insulin secretion and insulin sensitivity determines a normal glucose tolerance, while the secretory response of the pancreatic β-cells to glucose and the sensitivity of the glucose utilizing tissues to insulin determine the ability of insulin to dispose of carbohydrates [1, 2]. In individuals with the same degree of glucose tolerance, the product of insulin sensitivity and insulin secretion is constant, reaching an approximate hyperbola [8], reflecting the ability of the β-cell to compensate for insulin resistance.
The pregnant status is a diabetogenic condition favorited by some well-studied mechanisms: human placental lactogen has anti-insulin and lipolytic effects, increasing glucose levels in maternal plasma and, as consequence, higher availability to the fetus; steroid hormones increase insulin resistance in peripheral tissues; and some insulin may be destroyed by the placenta [1,2,3, 7]. These processes cause decreased phosphorylation of insulin receptor substrate, causing a condition of insulin resistance, but then compensated by pancreatic increases of insulin secretion [1, 2].
In a physiopathological context, a deterioration of β-cell function, particularly the first-phase insulin secretion, has been found, and the combination of insulin resistance and secretory defects during pregnancy results in GDM [1, 2]. In contrast to healthy women, the majority of women affected by GDM is characterized by a β-cell dysfunction that occurs on a background of chronic insulin resistance, preexisting pregnant status [9]. Many defects, such as alterations in the insulin signaling pathway, reduced expression of peroxisome proliferator-activated receptor gamma (PPAR-γ or PPARG), and reduced insulin-mediated glucose transport, have been found in skeletal muscle or fat cells of women with GDM [10]. It has recently been suggested that post-receptor defects are present in the insulin signaling pathway in the placenta of women with pregnancies complicated by diabetes and obesity [11]. In addition, expression studies demonstrate that post-receptor alterations in insulin signaling may be under selective maternal regulation and are not regulated by the fetus [11].
Recently, it has also been proposed that the GDM development is triggered by the fetus itself [12]. Human leukocyte antigen-G (HLA-G) expression, which functions to protect the fetus from immune attack by down-regulating cytotoxic T cell responses to fetal trophoblast antigens, is postulated to protect pancreatic islet cells as well [12]. To endorse, it has been hypothesized that the development of DM in patients who have undergone organ transplantation is analogous to GDM development in a proportion of pregnancies [13]. In both cases, an antigenic load triggers the diabetogenic process. If future studies will confirm this hypothesis, it may be possible to use recombinant HLA-G for the prevention of GDM in high-risk patients. Finally, among rare causes for GDM, it should be included both autoimmune destruction of pancreatic β-cells and mutations in autosomes (commonly referred to as maturity-onset diabetes of the young (MODY), with different genetic subtypes designated as MODY-1, MODY-2, etc.).
Action mechanism of vitamin D in glucose regulation
In humans, the naturally occurring form of VD is cholecalciferol or VD3 and it can be ingested by the diet or produced in the skin by UV light interaction with a cholesterol derivative ( Fig. 2) [14]. VD2 or ergocalciferol is derived from plant sterols and contained in most VD supplements [5, 6]. Both D2 and D3 travel in the blood bound to VD Binding Protein and must be hydroxylated to become active. D3 and D2 metabolites are thought to have equal physiologic activity, but D3 levels may increase more quickly after supplementation [5, 14]. 25-hydroxyvitamin D (25(OH)D) is first hydroxylated in the liver. Such resulting metabolite is very stable and is therefore most commonly used to measure VD status. The second hydroxylation to the active form 1,25(OH)D occurs mostly in the kidneys in a process tightly regulated by calcium, phosphorus, and parathyroid hormone levels. After the second hydroxylation, 1,25(OH)D binds to the VD Receptor (VDR). VDR is a transcription factor whose products are involved in a wide array of activities including bone metabolism, cellular growth and differentiation, glucose metabolism, and immune function. Both the enzyme responsible for VD activation (1α-hydroxyase) and its receptor have been located in peripheral tissues, such as the placenta, suggesting a farther-reaching role for VD than bone metabolism alone [15].

Vitamin D metabolism (by Deeb KK et al. Vitamin D signaling pathways in cancer: potential for anticancer therapeutics. Nature Reviews Cancer. 2007;7:684–700)
In order to summarize the most relevant biological mechanisms involving low levels of VD in GDM pathogenesis, we listed below those described in animal and human models [7, 16,17,18,19]:
-
1.
via calcium pool dysregulation in the pancreas → VD deficiency may contribute to the development of GDM by a 1,25(OH)D-VDR binding in pancreatic β-cells to regulate the balance between extra- and intracellular;
-
2.
via effects on insulin-sensitive tissues → VD may promote insulin sensitivity by stimulating insulin receptor expression and enhancing insulin responsiveness to glucose;
-
3.
via genetic variations → interactions of VD and VD related (i.e., VDR) with the insulin-like growth factor system influence glucose homeostasis;
-
4.
via inflammation → VD may contribute to lower GDM risk by its role in mitigating inflammation and its effects, as demonstrated in T2DM; and
-
5.
via co-factor of risk → the close relationship of VD deficiency with other common risk factors, such as obesity, may account, in part, for its association with GDM and other related pregnancy complications.
VDR polymorphisms and its potential role in the GDM pathogenesis
Because single-nucleotide polymorphisms, frequently called SNPs, are the most common type of genetic variation among people, they can act as biological markers if associated with diseases or predictors of individual response to drugs or spies of the inheritance of disease genes within families. An increasing literature is investigating the potential role of polymorphisms on VDR in breast cancer, multiple sclerosis, and coronary artery disease, achieving contrasting results. Similarly, in metabolic disease, including T1DM and T2DM, the results are controversial. In a recent meta-analysis, BsmIBB, BsmIBb, and TaqItt polymorphisms were associated with an increased risk of T1DM, whereas BsmIbb and TaqITT had protective effect for T1DM in children [20]. In an updated meta-analysis, a significant association between the BsmI polymorphism and T2DM was weak, and the FokI polymorphism was significantly associated with T2DM risk only in Chinese people, but not in Caucasians [21]. In GDM, few studies are available, due to lack of statistical power, small effect size of common variants, or ethnic heterogeneity among different populations. In studies conducted on Iranian and Chinese pregnant women, a linkage between VDR ApaI, TaqI, and FokI gene polymorphisms and susceptibility to GDM has been suggested [22,23,24]. However, in view of the limited research available with contrasting finding on VDR genetic polymorphisms on GDM pathogenesis, further studies are warranted in order to confirm or exclude the potential aid from genetic biomarkers for an early risk prediction of GDM, and an ad hoc treatment by VD supplementation.
Diagnostic method for GDM diagnosis
Since GDM is associated with adverse perinatal outcomes (APO), lesser degrees of glucose intolerance have also been shown to be harmful, opening the question about the correct modality for defining the level of glucose intolerance in pregnancy. The diagnostic dilemma is related to the large number of procedures and glucose cut-offs proposed, as reported in Table 1 [25,26,27,28]. In response to the need for internationally agreed upon diagnostic criteria for GDM, the Hyperglycemia and Adverse Pregnancy Outcome (HAPO) study was performed, based upon their predictive value for APO [29]. Mainly, increases in each of the three values on the 75 g 2-h oral glucose tolerance test (OGTT) were associated with graded increases in the likelihood of pregnancy outcomes [29].
Based upon an iterative process of decision making, the task force of the International Association of Diabetes in Pregnancy Study Groups (IADPSG) recommended that the diagnosis of GDM be made when any of the following three 75 g 2-h OGTT thresholds are met or exceeded: fasting 92 mg/dl, 1 h 180 mg/dl, and 2 h 153 mg/dl [26]. In 2013, the adoption of these criteria was deliberated by WHO/NMH/MND/13.2 as well [28].
Diagnostic method for vitamin D status
To date, definition of VD status is still an open research area. Several difficulties have been found in the attempt to standardize the most appropriate diagnostic method, including the gold standard, laboratory methods, reference levels conditioned by geographical areas, physiological human condition, such as pregnancy [30].
As summation of both intake and produced from sun exposure, 25(OH)D has been recognized as the clinical and research gold standard measure of VD status, with a half-life of approximately 2–3 weeks and circulating levels thousand-fold more than 1,25(OH)D [31, 32]. An absolute consensus about a normal range for 25(OH)D is still lacking. Historically, the first attempt to define normal ranges (10–55 ng/ml), based on blood samples analysis in European and US healthy population, was considered inadequate subsequently due to 30–50% of both present VD insufficiency or deficiency [33]. Next, the observation that parathyroid hormone (PTH) levels started to plateau at their nadir when 25(OH)D levels were between 30 and 40 ng/ml, adjusted the previous cut-off [34]. Finally, from the evidence that VD supplementation in subjects with 25(OH)D > 20 ng/ml did not change their PTH level [35], it was suggested that VD deficiency should be defined as 25(OH)D above 20 ng/ml, as accepted most experts. Accordingly, VD deficiency should be defined as a 25(OH)D of <20 ng/ml, VD insufficiency as a 25(OH)D of 21–29 ng/ml, and the preferred level to be >30 ng/ml [32].
No full agreement is achieved in terms of use of standardized assay method. Over recent years, there has been a significant increase in 25(OH)D requests prompting many laboratories to consider the use of automated immunoassays. Among major techniques, binding assay (i.e., chemiluminescence immunoassays (CLIA), radioimmunoassay (RIA), binding protein assay) and chemical assay techniques (i.e., high-performance liquid chromatography (HPLC) and liquid chromatography-tandem mass spectrometry (LC–MS/MS)) are the most used, but significant differences in the 25(OH)D determination were observed between various assays, requiring an urgent standardization and harmonization of 25(OH)D measurements.
Measuring VD insufficiency in pregnant women is complicated by a lack of agreement in some aspects. Given the complexity of the VD system, it is unclear whether 25(OH)D levels have the same clinical implications in all women or throughout all stages of pregnancy. In the past, some researchers suggested to measure PTH levels as a biologic marker of VD deficiency, but they have been inconsistently associated with 25(OH)D levels in pregnancy [36, 37]. Recently, the Institute of Medicine (IOM) defined adequate VD status as having serum 25-hydroxyvitamin D concentrations greater than 50 nmol/L (or 20 ng/mL) in both the general population and pregnant women [38].
Association between maternal VD levels and GDM risk
Evidence from studies conducted for the assessment of 25(OH)D at multiple time points in pregnancy confirm the complexity of the association between maternal VD status and feto-maternal glucose homeostasis [39,40,41,42,43]. In Table 2, we listed the most relevant meta-analysis performed in the last decade, selecting only studies with medium–high quality.
While most case–control or nested case–control studies strengthen the linkage between low 25(OH)D levels and an increased risk of APO, meta-analysis are not conclusive for a reliable VD involvement on GDM onset, assessed at the first trimester especially. In their meta-analysis based on 12 studies with 5615 patients, Wei et al. concluded that among women with 25(OH)D levels <50 nmol/L, a modest increase in odds of GDM was found (crude OR 1.38, 95% CI 1.12–1.70) [41]. Similarly, Poel and colleagues observed that low VD levels were associated with increased odds of GDM (OR 1.61, 95% CI 1.19–2.17) in a meta-analysis of seven studies [39]. Albeit significant odd ratios for GDM risk reported range from 1.38 to 1.61, it seems conceivable to speculate that the association could be also causal, probably due to the study design of the researches developed. This has been confirmed performing subgroup analysis, where differences based on countries, measurement method, sample size, age at baseline, adjusted models, and study quality have been found by Lu and co-workers [43], debunking the already weak cause–effect relationship between VD status and GDM onset. As a demonstration, in a recent systematic review in the Mediterranean region with a high prevalence of maternal hypovitaminosis D during pregnancy, despite high levels of sunshine, analyzing 15 studies and 2649 patients, Karras et al. described a positive association with 25(OH)D concentrations and light skin color, white race, uncovered dressing pattern, maternal VD supplementation, and season of gestation (spring/summer); an inverse association for BMI and gestational age; and controversial data for smoking and socio-economic status [44]. This shows the complexity of interactions among individual, lifestyle, and geographical factors, being able to negate the benefits of sun exposure not only in adulthood in general, but also during pregnancy.
Unfortunately, although selecting meta-analyses developed only on medium–high-quality studies, their clinical impact is limited by the observational nature of the included studies, the mixing of diverse study populations from various regions, the different laboratory techniques, and timing of measurement of serum 25(OH)D level, leaving unknown the understanding of the VD contribution to the pathophysiology of the GDM development.
Effects of VD supplementation on GDM development
Since VD deficiency during pregnancy may be a common health problem worldwide, more prominent in some latitudes, with impact on obstetric outcomes, maintaining high enough levels of 25(OH)D could be a successful approach in obstetric care. However, if there is controversy regarding the 25(OH)D levels considered as adequate or optimal for overall health and pregnant women (50 nmol/L or 20 ng/ml vs. ≥75 nmol/L or 30 ng/ml), a regular supplemental VD dose of 1000–1600 IU (25–40 mg/day) might be defined as necessary to achieve and maintain optimal levels in the body, but the VD dose during pregnancy is not yet clear, as well as its combination with calcium supplements, health eating, and physical activity is explored in randomized trials [45,46,47,48,49,50,51,52] (Table 3).
In Australian low-risk patients, high-dose vs. low-dose VD supplementation, started at first trimester of pregnancy, did not change glucose levels [47], while in an Indian setting development of DGM was recorded in 44% of cases treated and in 20.3% of those not treated, by dosages depending upon 25(OH)D levels, started at 24–28 weeks [49]. In pregnancies at risk for GDM due to overweight or obesity, a gain in insulin sensitivity and prevention of increase in blood glucose levels by the combination of health eating, physical activity, and VD supplementation has been observed in 880 women, 110 per arm, managed by eight options of interventions, including combination of treatments or alone in an European study [45].
Conflicting results have been reported in patients with diagnosis of GDM. In a recent randomized trial, including pregnancies complicated by DGM not on oral hypoglycemic agents and treated by 50,000 IU D3 vs. placebo twice during the study, Asemi et al. reported improved pregnancy outcomes, in terms of decreased maternal polyhydramnios and infant hyperbilirubinemia and hospitalization, but not a significant impact on the need to insulin therapy after intervention [50]. Adding 1000 mg calcium per day to VD3, a significant reduction in fasting plasma glucose, serum insulin levels, HOMA-IR, and LDL-cholesterol and significant elevation in HDL-cholesterol levels were found [46]. After delivery, patients with former DGM were randomized to receive either daily 4000 IU vitamin D3 or placebo capsules by Yeow and colleagues, obtaining a better basal pancreatic ß-cell function and metabolic state [51].
In the last biennium, three meta-analyses have been published and joined by the similar aim to examine whether oral supplements with VD alone or in combination with calcium or other vitamins and minerals given to women during pregnancy could safely improve maternal and neonatal outcomes [30, 53, 54] (Table 4). Related to GDM, Pérez-López and colleagues observed that low VD levels were not associated with increased odds of GDM [OR 1.05 (95% CI 0.60–1.84)] in a meta-analysis of 13 studies [53]. Similarly, in the Cochrane review, where only 2 of 15 studies included were focused on GDM, any association was met between VD supplementation and GDM (RR 0.43 (95% CI 0.05–3.45), hypothesizing as reason the very low quality of trials evaluated [30].
Future challenges
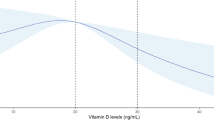
Investigating VD status and their health outcomes is fascinating for researchers from different fields, due to its pluripotent action, the receptors ubiquity in humans, the epidemiology of VD deficiency-related, and the feasibility of treatment. In obstetrics, findings of higher rates of some complications (preeclampsia, GDM, preterm birth, and bacterial vaginosis) in women with low VD levels open to an easy therapeutic strategy. Challenge for clinical researchers includes the optimal VD status to prevent GDM, the most effective and safe dose for reducing obstetric complications, the optimal timing to start, and interval to treat (Fig. 3). Also the correct understanding of interactions between VD, its receptor, and co-factor risks will be crucial. Only in well-designed randomized trials we could find adequate answers.

Future challenges about the relationship between VD supplementation and GDM
References
Association AD (2013) Diagnosis and classification of diabetes mellitus. Diabetes Care 36(Suppl 1):S67–S74
Chiefari E, Arcidiacono B, Foti D, Brunetti A (2017) Gestational diabetes mellitus: an updated overview. J Endocrinol Invest. doi:10.1007/s40618-016-0607
Cozzolino M, Serena C, Maggio L et al (2017) Analysis of the main risk factors for gestational diabetes diagnosed with International Association of Diabetes and Pregnancy Study Groups (IADPSG) criteria in multiple pregnancies. J Endocrinol Invest. doi:10.1007/s40618-017-0646-6
Saucedo R, Rico G, Vega G et al (2015) Osteocalcin, under-carboxylated osteocalcin and osteopontin are not associated with gestational diabetes mellitus but are inversely associated with leptin in non-diabetic women. J Endocrinol Invest 38:519–526
Triunfo S, Lanzone A (2016) Potential impact of maternal vitamin D status on obstetric well-being. J Endocrinol Invest 39:37–44
Thorne-Lyman A, Fawzi WW (2012) Vitamin D during pregnancy and maternal, neonatal and infant health outcomes: a systematic review and meta-analysis. Paediatr Perinat Epidemiol 26(S1):75–90
Senti J, Thiele DK, Anderson CM (2012) Maternal vitamin D status as a critical determinant in gestational diabetes. J Obstet Gynecol Neonatal Nurs 41:328–338
Kahn SE, Prigeon RL, McCulloch DK et al (1993) Quantification of the relationship between insulin sensitivity and b-cell function in human subjects. Evidence for a hyperbolic function. Diabetes 42:1663–1672
Kautzky-Willer A, Prager R, Waldhausl W et al (1997) Pronounced insulin resistance and inadequate beta cell secretion characterize lean gestational diabetes during and after pregnancy. Diabetes Care 20:1717–1723
Buchanan TA, Xiang AH (2005) Gestational diabetes mellitus. J Clin Invest 115:485–491
Colomiere M, Permezel M, Riley C, Desoye G, Lappas M (2009) Defective insulin signalling in placenta from pregnancies complicated by gestational diabetes mellitus. Eur J Endocrinol 160:567–578
Oztekin O (2007) New insights into the pathophysiology of gestational diabetes mellitus: possible role of human leukocyte antigen-G. Med Hypotheses 69:526–530
Ellard S, Beards F, Allen LL et al (2000) A high prevalence of glucokinase mutations in gestational diabetic subjects selected by clinical criteria. Diabetologia 43:250–253
Haddad JG, Stamp TC (1974) Circulating 25-hydroxyvitamin D in man. Am J Med 57:57–62
Mulligan ML, Felton SK, Riek AE et al (2010) Implications of vitamin D deficiency in pregnancy and lactation. Am J Obstet Gynecol 202(429):e1–e9
Holick MF (2007) Vitamin D deficiency. N Engl J Med 357:266–281
Hypponen E, Laara E, Reunanen A et al (2001) Intake of vitamin D and risk of type 1 diabetes: a birth-cohort study. Lancet 358:1500–1503
Bourlon PM, Billaudel B, Faure-Dussert A (1999) Influence of vitamin D3 deficiency and 1,25 dihydroxyvitamin D3 on de novo insulin biosynthesis in the islets of the rat endocrine pancreas. J Endocrinol 160:87–95
Cade C, Norman AW (1986) Vitamin D3 improves impaired glucose tolerance and insulin secretion in the vitamin D-deficient rat in vivo. Endocrinology 119:84–90
Sahin OA, Goksen D, Ozpinar A et al (2017) Association of vitamin D receptor polymorphisms and type 1 diabetes susceptibility in children: a meta-analysis. Endocr Connect 6(3):159–171
Yu F, Cui LL, Li X et al (2016) The genetic polymorphisms in vitamin D receptor and the risk of type 2 diabetes mellitus: an updated meta-analysis. Asia Pac J Clin Nutr 25(3):614–624
Aslani S, Hossein-Nezhad A, Mirzaei K et al (2011) DR FokI polymorphism and its potential role in the pathogenesis of gestational diabetes mellitus and its complications. Gynecol Endocrinol 27(12):1055–1060
Wang Y, Wang O, Li W et al (2015) Variants in vitamin D binding protein gene are associated with gestational diabetes mellitus. Medicine (Baltimore) 94(40):e1693
Rahmannezhad G, Mashayekhi FJ, Goodarzi MT et al (2016) Association between vitamin D receptor ApaI and TaqI gene polymorphisms and gestational diabetes mellitus in an Iranian pregnant women population. Gene 581(1):43–47
Canadian Diabetes Association (2008) Clinical practice guidelines for the prevention and management of diabetes in Canada. Can J Diabetes 32:S1–S201
International Association of Diabetes And Pregnancy Study Groups Consensus Panel (2010) International association of diabetes and pregnancy study groups recommendations on the diagnosis and classification of hyperglycemia in pregnancy. Diabetes Care 33:676–682
American College of Obstetricians and Gynecologists (2011) Screening and diagnosis of gestational diabetes mellitus. Committee Opinion No. 504. Obstet Gynecol 118:751–753
WHO/NMH/MND/13.2 (2013) Diagnostic criteria and classification of hyperglycaemia first detected in pregnancy. http://www.who.int/diabetes/publications/Hyperglycaemia_In_Pregnancy/en/. Accessed 14 Jan 2017
Coustan DR, Lowe LP, Metzger BE, Dyer AR (2010) The hapo study: paving the way for new diagnostic criteria for GDM. Am J Obstet Gynecol 202:654.e1–654.e6
De-Regil LM, Palacios C, Lombardo LK, Peña-Rosas JP (2016) Vitamin D supplementation for women during pregnancy Issue 1. Art. No.: CD008873
ACOG Committee Opinion No. 495 (2011) Vitamin D: screening and supplementation during pregnancy. Obstet Gynecol 118:197–198
Holick MF (2009) Vitamin D status: measurement, interpretation, and clinical application. Ann Epidemiol 19:73–78
Holick MF (2006) High prevalence of vitamin D inadequacy and implications for health. Mayo Clin Proc 81(3):353–373
Chapuy MC, Preziosi P, Maaner M et al (1997) Prevalence of vitamin D insufficiency in an adult normal population. Osteopor Int 7:439–443
Malabanan AO, Turner AK et al (1998) Severe generalized bone pain and osteoporosis in a premenopausal black female: effect of vitamin D replacement. J Clin Densitometr 1:201–204
Haddow JE, Neveux LM, Palomaki GE et al (2011) The relationship between PTH and 25-hydroxy vitamin D early in pregnancy. Clin Endocrinol (Oxf) 75:309–314
Essley BV, McNanley TJ, Cooper EM et al (2012) Vitamin D insufficiency is prevalent and vitamin D is inversely associated with PTH and calcitriol in pregnant adolescents. J Bone Miner Res 27:177–186
IOM (Institute of Medicine) (2011) Dietary reference intakes for calcium and vitamin D. The National Academies Press, Washington, DC, IOM guidelines for VD supplementation with a special section devoted to pregnancy
Poel YH, Hummel P, Lips P et al (2012) Vitamin D and gestational diabetes: a systematic review and meta-analysis. Eur J Intern Med 23:465–469
Aghajafari F, Nagulesapillai T, Ronksley PE et al (2013) Association between maternal serum 25-hydroxyvitamin D level and pregnancy and neonatal outcomes: systematic review and meta-analysis of observational studies. BMJ 346:f1169
Wei SQ, Qi HP, Luo ZC et al (2013) Maternal vitamin D status and adverse pregnancy outcomes: a systematic review and meta-analysis. J Matern Fetal Neonatal Med 26:889–999
Zhang MX, Pan GT, Guo JF et al (2015) Vitamin D deficiency increases the risk of gestational diabetes mellitus: a meta-analysis of observational studies. Nutrients 7:8366–8375
Lu M, Xu Y, Lv L, Zhang M (2016) Association between vitamin D status and the risk of gestational diabetes mellitus: a meta-analysis. Arch Gynecol Obstet 293:959–966
Karras S, Paschou SA, Kandaraki E et al (2016) Hypovitaminosis D in pregnancy in the Mediterranean region: a systematic review. Eur J Clin Nutr 70:979–986
Simmons D, Devlieger R, van Assche A et al (2017) Effect of physical activity and/or healthy eating on GDM risk: the DALI Lifestyle Study. J Clin Endocrinol Metab 102:903–913
Asemi Z, Karamali M, Esmaillzadeh A (2015) Favorable effects of vitamin D supplementation on pregnancy outcomes in gestational diabetes: a double blind randomized controlled clinical trial. Horm Metab Res 47:565–570
Yap C, Cheung NW, Gunton JE et al (2014) Vitamin D supplementation and the effects on glucose metabolism during pregnancy: a randomized controlled trial. Diabetes Care 37:1837–1844
Hossain N, Kanani FH, Ramzan S et al (2014) Obstetric and neonatal outcomes of maternal vitamin D supplementation: results of an open-label, randomized controlled trial of antenatal vitamin D supplementation in Pakistani women. J Clin Endocrinol Metab 99:2448–2455
Sablok A, Batra A, Thariani K et al (2015) Supplementation of vitamin D in pregnancy and its correlation with feto-maternal outcome. Clin Endocrinol (Oxf) 83:536–541
Asemi Z, Karamali M, Esmaillzadeh A (2014) Effects of calcium-vitamin D co-supplementation on glycaemic control, inflammation and o xidative stress in gestational diabetes: a randomised placebo-controlled trial. Diabetologia 57:1798–806
Yeow TP, Lim SL, Hor CP et al (2015) Impact of vitamin D replacement on markers of glucose metabolism and cardio-metabolic risk in women with former gestational diabetes—a double-blind, randomized controlled trial. PLoS One 10:e0129017
Karamali M, Asemi Z, Ahmadi-Dastjerdi M et al (2015) Calcium plus vitamin D supplementation affects pregnancy outcomes in gestational diabetes: randomized, double-blind, placebo-controlled trial. Public Health Nutr 19:156–163
Pérez-López FR, Pasupuleti V, Mezones-Holguin E et al (2015) Effect of vitamin D supplementation during pregnancy on maternal and neonatal outcomes: a systematic review and meta-analysis of randomized controlled trials. J Steroid Biochem Mol Biol 164:148–155
Palacios C, De-Regil LM, Lombardo LK et al (2015) Vitamin D supplementation during pregnancy: updated meta-analysis on maternal outcomes. Fertil Steril 103(1278–88):e4
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed consent
No informed consent was necessary for the study.
Rights and permissions
About this article

Cite this article
Triunfo, S., Lanzone, A. & Lindqvist, P.G. Low maternal circulating levels of vitamin D as potential determinant in the development of gestational diabetes mellitus. J Endocrinol Invest 40, 1049–1059 (2017). https://doi.org/10.1007/s40618-017-0696-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40618-017-0696-9