
Abstract
Purpose
Denosumab has been proven to reduce fracture risk in breast cancer (BC) women under aromatase inhibitors (AIs). Quantitative ultrasound (QUS) provides information on the structure and elastic properties of bone. Our aim was to assess bone health by phalangeal QUS and by dual-energy X-ray absorptiometry (DXA), and to evaluate bone turnover in AIs-treated BC women receiving denosumab.
Methods
35 Postmenopausal BC women on AIs were recruited (mean age 61.2 ± 4.5 years) and treated with denosumab 60 mg administered subcutaneously every 6 months. Phalangeal QUS parameters [Amplitude Dependent Speed of Sound (AD-SoS), Ultrasound Bone Profile Index (UBPI), Bone Transmission Time (BTT)] and DXA at lumbar spine and femoral neck were performed. Serum C-telopeptide of type 1 collagen (CTX) and bone-specific alkaline phosphatase (BSAP) were also measured. The main outcomes were compared with a control group not receiving denosumab (n = 39).
Results
In patients treated with denosumab, differently from controls, QUS and DXA measurements improved after 24 months, and a reduction of CTX and BSAP was detected at 12 and 24 months in comparison to baseline (P < 0.05). The percent changes (Δ) of QUS measurements were significantly associated with ΔBMD at femoral neck, and ΔCTX and ΔBSAP were associated with ΔBMD at lumbar spine (r = −0.39, P = 0.02; r = −0.49, P = 0.01, respectively).
Conclusions
Denosumab preserves bone health as assessed by phalangeal QUS and DXA. Since inexpensive and radiation-free, phalangeal QUS may be considered in the follow-up of AIs-treated BC women receiving denosumab.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Aromatase inhibitors (AIs) represent the gold-standard adjuvant treatment for postmenopausal women with hormone receptor-positive breast cancer (BC) and for the management of metastatic disease. Previous trials involving tamoxifen and AIs have shown the latter being associated to better disease-free survival, time to recurrence and time to metastasis [1–3]. Because of their use, accelerated bone loss and increased risk of fractures due to near-complete ablation of estrogen production have been reported, and increased awareness about AIs-induced osteoporosis has led to several recommendations for patient management during treatment with these drugs [4–8].
Denosumab is a fully human IgG2 monoclonal antibody that binds with high affinity and specificity to the tumor necrosis factor (TNF)-related cytokine receptor activator of nuclear factor kappa B ligand (RANKL), a key cytokine inducing differentiation of hematopoietic precursors common to the monocyte/macrophage and osteoclast lineages into multinucleated, active bone-resorbing cells [9, 10]. By preventing the interaction of RANKL with its receptor RANK, on osteoclasts and osteoclast precursors, denosumab reversibly inhibits osteoclast-mediated bone resorption [9].
Denosumab has been previously reported to reduce the risk of vertebral, non-vertebral, and hip fractures in postmenopausal women and to improve bone mineral density (BMD) in men with low bone mineral density [10, 11]. Also, denosumab has been recently proven to preserve bone mass and reduce the risk of vertebral fractures in men receiving androgen depletion therapy for prostate cancer and in BC women treated with AIs [12–14].
As known, a decreased BMD is the major risk factor for fractures, and measuring BMD by dual-energy X-ray absorptiometry (DXA) is considered the gold-standard tool in assessing osteoporosis [15].
Several studies have generally found significant correlations between quantitative ultrasound (QUS), DXA and prevalent vertebral fractures; the ten-year probability of clinical vertebral fractures was also associated to QUS [16–22]. QUS at phalangeal site was proven to be a reliable tool to screen for osteoporosis and to predict incident fractures independently from DXA; indeed, ultrasound transmission on bone tissue depends on physical properties of bone not measured by DXA but able to modulate bone strength and, consequently, the risk of fractures [18, 20]. However, a limited use in clinical practice of phalangeal QUS is due to questions related to the reproducibility of the measurements performed by different operators using the same device, or the performance of measurements using different devices applied to the same anatomical site, and the lacking of standardizing procedure for commercially available QUS devices.
Recently, we demonstrated that phalangeal QUS measurements were able to detect the AIs-induced changes of bone, and were associated to DXA [23]. The possibility to evaluate the effects of bone-active drugs by QUS was also proven in postmenopausal women [24, 25]. There are no data on whether phalangeal QUS may be affected under denosumab in AIs users.
Aim of this research was to evaluate bone status by QUS and DXA in BC women receiving denosumab to counteract the expected accelerated bone loss induced by AIs.
Materials and methods
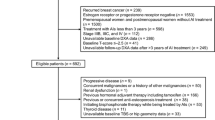
Our prospective study included a group of Caucasian women (n = 38), with early BC (carcinoma in situ and stage I and stage II breast cancers) who started (within the last 12 months previous enrollment) adjuvant treatment with AIs (i.e. anastrozole, letrozole, exemestane). Recruited subjects were all postmenopausal women referring to the outpatients clinics for the prevention and treatment of osteoporosis at the Department of Clinical and Experimental Medicine of Messina University (Messina, Italy). Low bone mass (osteopenia or osteoporosis in accordance with the WHO criteria) with at least one prevalent morphometric vertebral fracture were required to participate in this study, in accordance with the Italian drug reimbursement issues at the time of recruitment. Exclusion criteria were: other malignancies, known or suspected bone metastases, liver or renal failure, hyperthyroidism, hyperparathyroidism, hypercalcemia or hypocalcemia, use of medications affecting bone and mineral metabolism within the last 6 months (including corticosteroids, heparin, and anticonvulsants), ongoing or previous use of active bone agents (e.g. bisphosphonates, selective estrogen receptor modulators, strontium ranelate, teriparatide or PTH, calcitonin).
Recruited women received subcutaneous denosumab 60 mg every 6 months (Dmab group), and were compared, for ethical reasons, with a historical control group (n = 39) of AIs-treated BC postmenopausal women attending the same center and matched for age and anthropometric features, but without vertebral fractures at baseline evaluation.
All the participants received an oral supplementation of cholecalciferol (25,000 IU bimonthly); moreover, women with an estimated poor dietary calcium intake were accordingly supplied with calcium carbonate (500–1000 mg, daily) to reach the recommended daily allowance of calcium.
The study was conducted in accordance with the ethical standards of our institutional research committee and with the 1964 Declaration of Helsinki and its later amendments, and written informed consent was obtained from all the participants.
QUS measurements were obtained at the proximal phalangeal metaphysis of the last four fingers of the non-dominant hand using a DBM Sonic Bone Profiler (Igea, Carpi, Italy) as previously described [26]. The following parameters were measured: amplitude-dependent speed of sound (AD-SoS), bone transmission time (BTT), fast wave amplitude (FWA), signal dynamic (SDy), and ultrasound bone profile index (UBPI) automatically calculated (UBPI= −(0.0018 × SDy −0.0560 × FWA 0.0560–1.1467 × BTT + 3.0300)). The coefficient of variation (CV) for AD-SoS was of 0.9%.
BMD was assessed by a dual-energy X-ray absorptiometry (DXA) scan device (Hologic Discovery) at the lumbar spine (L1-L4) in AP projection and at the femoral neck. Calibration of DXA densitometer was carried out on a daily basis in accordance with the manufacturer’s indications, and the CV was 0.5% with the standard phantom.
Fracture assessment was based on the analysis of lateral radiographs of the dorsal and lumbar spine according to the Genant’s semiquantitative visual score: vertebral fractures were defined as height reductions in the anterior, middle or posterior height compared with the same or adjacent vertebra of 20–25% or more on radiographs. QUS, DXA and vertebral morphometry by X-ray were performed at baseline and after 24 months.
At baseline, 12 and 24 months, C-telopeptide of type 1 collagen (CTX), as a marker of bone resorption, bone-specific alkaline phosphatase (BSAP), as a marker of bone formation, 25-hydroxyvitamin D (25(OH)D), albumin-corrected calcium, phosphorus, and creatinine, were measured. CTX (Roche, Basel, Switzerland) and BSAP (Beckman Coulter, Fullerton, California) were measured by enzyme-linked immunosorbent assay, with intra-assay coefficient of variation CV of 1.6–3% and inter-assay CV of 1.3–4.3% for CTX, and intra-assay CV of 2.3–3.7% and inter-assay CV of 4.9–9.8% for BSAP. 25(OH)D were detected by high-performance liquid chromatography; calcium, phosphorus and creatinine were measured using standard laboratory techniques.
Statistical analyses were performed using MedCalc software (version 10.2.0.0; Mariakerke, 173 Belgium). The normal distribution of values was verified with the Kolmogorov–Smirnov test. Comparisons between the groups were performed using Student’s t test or Mann–Whitney test as appropriate. A repeated-measures ANOVA model was used to assess the changes of parameters within each group over time. Spearman’s coefficient was used to measure the degree of association between two variables. Values of P < 0.05 were considered to indicate statistical significance. All reported P values were two-sided.
Results
A total of thirty-five BC postmenopausal women, in the Dmab group, completed the study; three patients were excluded from the final analysis: two women because of introducing drugs potentially involving bone metabolism (heparin, corticosteroid), the other one because of having moved to other city and, thus, missed to follow-up. The main clinical characteristics of participants are shown in Table 1. At baseline, no significant differences were detected between Dmab and control groups, except for the above-mentioned absence of vertebral fractures in controls.
DXA measurements are presented in Table 2. At the end of the study, BMD values at lumbar spine and femoral neck were significantly improved (P < 0.05) in the Dmab group (+3.4 and +1.5%, respectively), but resulted significantly worsened in controls (−2.7 and −3.0%, respectively). The same trend was observed in QUS measurements (Table 2), with a significant increase (P < 0.05) in AS-SoS, UBPI and BTT values (+3.8, +6.4 and +8.4%, respectively) in the Dmab group, and a significant reduction (P < 0.05) of these values (−3, −6.4 and −7%) in controls. A significant reduction of bone turnover markers was also observed at 12 and 24 months (Table 3). 25(OH)D levels rose over the observation period in both groups, but no significant changes of calcium, phosphorus and creatinine were detected. In the Dmab group, the percent changes (Δ) of QUS measurements (AD-SoS, UBPI and BTT) were significantly associated with Δ BMD at femoral neck, and the highest degree of association was observed for AD-SoS (r = 0.5, P = 0.003), as shown in Fig. 1.

Correlations between percent changes (Δ) of femoral neck BMD detected by DXA and the phalangeal QUS parameters AD-SoS (panel a), UBPI (panel b) and BTT (panel c) in AIs-treated BC women receiving denosumab
ΔCTX and Δ BSAP were associated with Δ BMD at lumbar spine (r = −0.39, P = 0.02; r = −0.49, P = 0.01, respectively).
During the study period, none of the patients reported any new vertebral fractures.
Discussion
In postmenopausal patients with hormone receptor-positive early-stage BC who receive therapy with AIs, the subcutaneous administration of denosumab every 6 months significantly improved bone health as suggested both by DXA and QUS evaluations. Accordingly to other authors, denosumab has been confirmed to be effective in improving BMD, by reducing bone turnover [13, 14]; moreover, for the first time, we have shown the potential ability of phalangeal QUS to detect bone changes due to denosumab, over a period of accelerated bone loss in postmenopausal BC survivors on AIs.
As known, in addition to DXA, QUS at the phalanges provides additional data useful to the study of bone fragility, possibly by capturing more and different information on the physical properties of bone tissue (e.g. structure and elasticity) that contribute to bone strength and are not recognized by DXA.
Both cortical and trabecular bone determine bone strength; 80% of bone is cortical, and up to 70% of all appendicular bone loss is cortical and occurs mainly by intracortical remodeling; the increase in intracortical porosity reduces bone strength exponentially [27]. The phalanx of adult subjects can be expected to mostly consist of cortical bone; thus, phalangeal QUS may be affected when cortical bone is impaired [28]. We previously observed a positive association between the percent changes of AD-SoS and femoral neck BMD in AIs users, consistent with the wide representation of cortical bone tissue in the femur [23]. Here, we observed an improvement of QUS parameters over a 24-month course of denosumab in BC women on AIs. In comparison with alendronate, denosumab has been proven to reduce remodeling more rapidly, more completely and to decrease intracortical porosity to a greater extent [29]; in fact, in comparison with trabecular bone, less bisphosphonate may be incorporated into the large mineralized cortical bone matrix because of less surface area per unit volume of mineralized bone matrix upon which bisphosphonates can be adsorbed. A more pronounced effect on cortical bone is, thus, expected for denosumab, and reversing cortical porosity may contribute to further reduction of fracture risk. Since AD-SoS is mainly affected by cortical area, cortical bone density, and cortical porosity, it may be a potentially useful parameter to explore the skeletal effects over time of denosumab when administered to prevent bone loss in AIs-treated BC women.
Previously, it was observed by other authors using high-resolution quantitative computed tomography (QCT), that both volumetric BMD and cortical thickness were deteriorated more dramatically than detected by DXA, in BC women treated with exemestane [30]. Similarly, the trabecular bone score (TBS), a recently developed analytical tool that performs novel grey-level texture measurements on DXA images, capturing information related to trabecular microarchitecture, has been proven to be significantly decreased at the lumbar spine and hip, irrespective of DXA-measured BMD [31]. Considered altogether, these data suggest that the predictive performance of BMD measured by DXA may be affected in this cohort of women. Furthermore, it could be speculated that the denosumab-mediated fracture risk reduction that was observed by Gnant A et coll. in BC postmenopausal women with baseline apparently normal BMD at the same extent of women with low BMD could be ascribed to favorable changes of bone properties beyond DXA-derived BMD, but further bone evaluations with QUS, QCT or TBS were not performed in their study [14].
At baseline, we observed suboptimal 25(OH)D serum levels in BC women involved in this research; however, 25(OH)D levels rose over time due to cholecalciferol supplementation, and improving vitamin D status could have contributed in boosting the effects of denosumab; it was also reported that vitamin D increases aromatase expression in bone, leading to a reduction of the deleterious effects of estrogen deprivation in bone caused by the AIs, and may play a role in musculoskeletal pain management [32].
We acknowledge that our research has some limitations: the small sample size, the absence of a matched control group with regard to prevalent vertebral fractures, the observation period not long enough to account for fractures and the lack of DXA data on distal forearm, which is rich in cortical bone and would have allowed additional correlations with our QUS measurements. On the other hand, phalangeal QUS, a radiation-free and inexpensive tool, for the first time, has been highlighted to be helpful in the follow-up of bone health evaluation in BC postmenopausal women on AIs and starting treatment with denosumab. Data from phalangeal QUS may be useful in studying the bone quality and, therefore, in the fracture risk assessment in this particular set of patients.
In conclusion, over a period of 2 years, denosumab at a dose of 60 mg twice a year has been confirmed to be able to improve bone health as recognized by phalangeal QUS and DXA measurements. Further researches with larger numbers of patients treated for longer periods are needed to determine if the changes over time in phalangeal QUS measurements are associated with fracture risk reduction in this cohort of women.
References
Coombes RC, Hall E, Gibson LJ et al (2004) A randomized trial of exemestane after two to three years of tamoxifen therapy in postmenopausal women with primary breast cancer. N Engl J Med 350(11):1081–1092
Mouridsen H, Sun Y, Gershanovich M et al (2004) Superiority of letrozole to tamoxifen in the first-line treatment of advanced breast cancer: evidence from metastatic subgroups and a test of functional ability. Oncologist 9(5):489–496
Nabholtz JM, Buzdar A, Pollak M et al (2000) Anastrozole is superior to tamoxifen as first-line therapy for advanced breast cancer in postmenopausal women: results of a North American multicenter randomized trial. Arimidex Study Group. J Clin Oncol 18(22):3758–3767
Eastell R, Hannon R (2005) Long-term effects of aromatase inhibitors on bone. J Steroid Biochem Mol Biol 95(1–5):151–154
Vescini F, Attanasio R, Balestrieri A, Bandeira F, Bonadonna S, Camozzi V, Cassibba S, Cesareo R, Chiodini I, Francucci CM, Gianotti L, Grimaldi F, Guglielmi R, Madeo B, Marcocci C, Palermo A, Scillitani A, Vignali E, Rochira V, Zini M (2016) Italian association of clinical endocrinologists (AME) position statement: drug therapy of osteoporosis. J Endocrinol Invest 39(7):807–834
Papadimitriou DT, Dermitzaki E, Papagianni M, Papaioannou G, Papaevangelou V, Papadimitriou A (2016) Anastrozole plus leuprorelin in early maturing girls with compromised growth: the “GAIL” study. J Endocrinol Invest 39(4):439–446
Hadji P, Aapro MS, Body JJ et al (2011) Management of aromatase inhibitor-associated bone loss in postmenopausal women with breast cancer: practical guidance for prevention and treatment. Ann Oncol 22(12):2546–2555
Rizzoli R, Body JJ, DeCensi A, Reginster JY, Piscitelli P, Brandi ML; European Society for Clinical and Economical aspects of Osteoporosis and Osteoarthritis (ESCEO) (2012) Guidance for the prevention of bone loss and fractures in postmenopausal women treated with aromatase inhibitors for breast cancer: an ESCEO position paper. Osteoporos Int 23(11):2567–2576
Kostenuik PJ, Nguyen HQ, McCabe J et al (2009) Denosumab, a fully human monoclonal antibody to RANKL, inhibits bone resorption and increases BMD in knock-in mice that express chimeric (murine/human) RANKL. J Bone Min Res 24:182–195
Cummings SR, San Martin J, McClung MR et al (2009) Denosumab for prevention of fractures in postmenopausal women with osteoporosis. N Engl J Med 361(8):756–765
Orwoll E, Teglbjaerg CS, Langdahl BL et al (2012) A randomized, placebo-controlled study of the effects of denosumab for the treatment of men with low bone mineral density. J Clin Endocrinol Metab 97:3161–3169
Smith MR, Egerdie B, Hernandez Toriz N et al (2009) Denosumab in men receiving androgen-deprivation therapy for prostate cancer. N Engl J Med 361:745–755
Ellis GK, Bone HG, Chlebowski R et al (2008) Randomized trial of denosumab in patients receiving adjuvant aromatase inhibitors for non metastatic breast cancer. J Clin Oncol 26:4875–4882
Gnant M, Pfeiler G, Dubsky PC et al (2015) Adjuvant denosumab in breast cancer (ABCSG-18): a multicentre, randomised, double-blind, placebo-controlled trial. Lancet 386(9992):433–443
Kalder M, Hans D, Kyvernitakis I, Lamy O, Bauer M, Hadji P (2014) Effects of Exemestane and Tamoxifen treatment on bone texture analysis assessed by TBS in comparison with bone mineral density assessed by DXA in women with breast cancer. J Clin Densitom 17(1):66–71
Gluer CC (1997) Quantitative ultrasound techniques for the assessment of osteoporosis: expert agreement on current status. The International Quantitative Ultrasound Consensus Group. J Bone Miner Res 8:1280–1288
Wüster C, Albanese C, De Aloysio D et al (2000) Phalangeal osteosonogrammetry study: age-related changes, diagnostic sensitivity, and discrimination power. The Phalangeal Osteosonogrammetry Study Group. J Bone Miner Res 15(8):1603–1614
Glüer CC, Eastell R, Reid DM et al (2004) Association of five quantitative ultrasound devices and bone densitometry with osteoporotic vertebral fractures in a population-based sample: the OPUS Study. J Bone Miner Res 19(5):782–793
Kanis JA, Johnell O, Oden A, De Laet C, De Terlizzi F (2005) Ten-year probabilities of clinical vertebral fractures according to phalangeal quantitative ultrasonography. Osteoporos Int 16(9):1065–1070
Catalano A, Morabito N, Basile G et al (2013) Fracture risk assessment in postmenopausal women referred to an Italian center for osteoporosis: a single day experience in Messina. Clin Cases Miner Bone Metab 10(3):191–194
Catalano A, Morabito N, Di Vieste G et al (2013) Phalangeal quantitative ultrasound and metabolic control in pre-menopausal women with type 1 diabetes mellitus. J Endocrinol Invest 36(5):347–351
Atteritano M, Lasco A, Mazzaferro S et al (2013) Bone mineral density, quantitative ultrasound parameters and bone metabolism in postmenopausal women with depression. Intern Emerg Med 8(6):485–491
Catalano A, Morabito N, Agostino RM et al (2016) Bone health assessment by quantitative ultrasound and dual-energy X-ray absorptiometry in postmenopausal women with breast cancer receiving aromatase inhibitors. Menopause. DOI:10.1097/GME.0000000000000722
Mauloni M, Rovati LC, Cadossi R, de Terlizzi F, Ventura V, de Aloysio D (2000) Monitoring bone effect of transdermal hormone replacement therapy by ultrasound investigation at the phalanx: a four-year follow-up study. Menopause 7(6):402–412
Machado ABC, Ingle BM, Eastell R (1999) Monitoring alendronate therapy with Quantitative Ultrasound (QUS) and Dual X-ray Absorptiometry (DXA). J Bone Miner Res 14(S1):S526
Catalano A, Pintaudi B, Morabito N et al (2014) Gender differences in sclerostin and clinical characteristics in type 1 diabetes mellitus. Eur J Endocrinol 171(3):293–300
Zebaze RM, Ghasem-Zadeh A, Bohte A et al (1010) Intracortical remodelling and porosity in the distal radius and post-mortem femurs of women: a cross-sectional study. The Lancet 375:1729–1736
Sakata S, Barkmann R, Lochmüller EM, Heller M, Glüer CC (2004) Assessing bone status beyond BMD: evaluation of bone geometry and porosity by quantitative ultrasound of human finger phalanges. J Bone Miner Res 19(6):924–930
Zebaze RM, Libanati C, Austin M et al (2014) Differing effects of denosumab and alendronate on cortical and trabecular bone. Bone 59:173–179
Cheung AM, Tile L, Cardew S et al (2012) Bone density and structure in healthy postmenopausal women treated with exemestane for the primary prevention of breast cancer: a nested substudy of the MAP.3 randomised controlled trial. Lancet Oncol 13(3):275–284
Prasad C, Greenspan SL, Vujevich KT et al (2016) Risedronate may preserve bone microarchitecture in breast cancer survivors on aromatase inhibitors: A randomized, controlled clinical trial. Bone 90:123–126
Krishnan AV, Swami S, Peng L, Wang J, Moreno J, Feldman D (2010) Tissue-selective regulation of aromatase expression by calcitriol: implications for breast cancer therapy. Endocrinology 151(1):32–42
Acknowledgements
We would like to thank Dr Andrè Corrado for the DXA measurements.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments.
Informed consent
Informed consent was obtained from all participants included in the study.
Conflict of interest
Catalano Antonino, Gaudio Agostino, Morabito Nunziata, Basile Giorgio, Agostino Rita Maria, Xourafa Anastasia, Atteritano Marco, Morini Elisabetta, Natale Giuseppe and Lasco Antonino declare that they have no conflicts of interest.
Funding
This research did not receive any specific grant from any funding agency in the public, commercial or not-for-profit sector.
Rights and permissions
About this article

Cite this article
Catalano, A., Gaudio, A., Morabito, N. et al. Quantitative ultrasound and DXA measurements in aromatase inhibitor-treated breast cancer women receiving denosumab. J Endocrinol Invest 40, 851–857 (2017). https://doi.org/10.1007/s40618-016-0606-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40618-016-0606-6