
Abstract
The functional analysis (FA) methodology was developed to provide an empirical basis for understanding the reinforcers contributing to the maintenance of problem behavior. Previous research has demonstrated that multiple formats have been established to address some areas, such as practicality, efficiency, and safety. We reviewed the research on a new replication and extension of the standard FA format, the interview-informed synthesized contingency analysis (IISCA) and its subsequent treatment. We discuss the efficiency and effectiveness of the IISCA across various populations, settings, topographies of problem behaviors, and maintaining functions across 17 studies. Common treatment trends, novel developments, and other critical intervention components are also reviewed. We provide suggestions for future directions and guidelines for practitioners when considering the use of the IISCA.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Functional analysis (FA) methodology allows for the systematic manipulation of reinforcement contingencies to identify the most likely variables maintaining problem behavior (Iwata, Dorsey, Slifer, Bauman, & Richman, 1982/1994). The FA method can guide practitioners toward creating function-based interventions to effectively treat problem behavior. The procedures described by Iwata et al., (1982/1994) have sometimes been referred to as the “gold standard” (Oliver, Pratt, & Normand, 2015) because of the influence they have had on our functional assessment technology. Moreover, an abundance of evidence supporting the standard FA in the applied behavior-analytic literature across varying ages, diagnoses, settings, topographies of problem behavior, and procedural formats has emerged (Beavers, Iwata, & Lerman, 2013). As of 2012, there have been almost 1,000 published replications or variations of the original FA method (Beavers et al., 2013).
Despite its wide research base, an alarming number of Board Certified Behavior Analysts (BCBAs; 63%) reported never or almost never using FA methods to identify problem behavior in a recent survey (Oliver et al., 2015). The most common barriers reported were due to a lack of time or resources. Hanley (2012) reviewed a list of potential obstacles to implementation of the standard FA and addressed these barriers with possible design or methodological refinements (e.g., latency-based, trial-based FA; for a full review, see Hanley, 2012). Fortunately, the standard FA method has been shown to be modifiable with the goal of increasing the accuracy of identifying behavioral functions (Hagopian, Rooker, Jessel, & DeLeon, 2013).
An emerging literature base has proposed another extension of the original format and has been referred to as the interview-informed synthesized contingency analysis (IISCA; Hanley, Jin, Vanselow, & Hanratty, 2014). The functional assessment process of the IISCA begins with an open-ended interview, followed by the presentation of synthesized antecedents and consequences emulating the context in which natural contingencies of problem behavior have been reported. The goal of the IISCA is to readdress some of the limitations attributed by Hanley et al. to the standard FA (e.g., timeliness, requires too many resources, potentially dangerous, generic contingencies) and to create a more efficient approach for practitioners. It is also important to note that none of the individual components of the IISCA are novel (i.e., interview informed, synthesized contingencies, single test condition, matched control). For example, a growing number of FAs have evaluated synthesized contingencies since 1995 (see Slaton & Hanley, 2018, for a review). Where the IISCA departs from previous FA models is that it is a comprehensive collection of these components in a functional assessment package that is conducted from the onset, rather than introducing individual modifications following the failure of the standard FA.
The purpose of this paper is to briefly review the IISCA research and subsequent treatment results based on these assessments. We review the effectiveness and limitations of the IISCA across various populations, settings, topographies of behaviors, and maintaining functions. We also discuss critical developments derived from the extant literature and provide suggestions for future research and clinical application.
Method
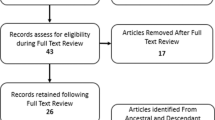
The first and second authors conducted an independent search of the published literature following 2014 using PsycINFO and included any articles that reported the use of the IISCA, with or without treatment, through October 2018. Specifically, this included a reference to the procedures conducted by Hanley et al. (2014), but without having to specifically refer to the IISCA by name. Studies that used an interview to inform the FA, or studies that used synthesized conditions within their FA, without reference to the Hanley et al. methodology, were excluded. We included all studies that used a single-subject design (e.g., reversal design, multielement design) to evaluate the suspected contingency during the IISCA with the effects replicated at least once in the test and control conditions. Furthermore, we reported on the results of the treatment evaluation if the study included repeated measures and direct (e.g., reversal) or systematic replication of the treatment effects across different behaviors, contexts, or people (e.g., multiple baseline).
Interrater Agreement
Interrater agreement was scored for 40% of all studies (i.e., seven studies). A second rater scored each variable using exact interrater agreement. The specific variables reviewed were the age and diagnosis of participants; the setting in which the assessment/treatment was conducted; participants’ problem behavior and language ability; the duration of the interview, direct observation, and FA conditions; the number of FA sessions; and whether social validity, generalization, maintenance, or treatment integrity were reported. Exact agreement included two observers reporting the same responses for each variable. For example, if both raters scored problem behavior as aggression and property destruction, this was considered an agreement. A disagreement was defined as two raters scoring different responses for a variable. For example, if one rater scored aggression and the other rater scored property destruction, this would count as a disagreement. The total interrater agreement was scored by dividing the total number of agreements by the sum of agreements and disagreements, multiplied by 100. Overall interrater agreement was 99.3%.
Treatment Effectiveness
Treatment outcomes were evaluated in the studies that included function-based interventions informed by the results of the IISCA. Percentage reductions in problem behavior were calculated by comparing the mean of the last three points from the first baseline phase to the mean of the last three points from the final treatment phase. The treatment was determined to be effective if it produced a 90% reduction in problem behavior. We used this nonparametric statistical analysis because it is identical to that from Jessel, Ingvarsson, Metras, Kirk, and Whipple (2018). A 90% reduction in problem behavior was chosen in the current review as the criterion to be considered an effective treatment because all 25 participants in the Jessel, Ingvarsson, Metras, Kirk, et al. (2018) consecutive case series were found to have 90% reductions using this statistical analysis.
Results
Based on the review of the literature, we identified 17 studies across five journals that conducted a total of 102 IISCA applications with 89 participants. From the 102 applications, 97 (95%) were differentiated. Furthermore, 55 treatment evaluations informed by the IISCA were conducted in 14 of these studies. Six of 17 studies (Fisher, Greer, Romani, Zangrillo, & Owen, 2016; Herman, Healy, & Lydon, 2018; Lambert et al., 2017; Strand & Eldevik, 2017; Strohmeier, Murphy, & O’Connor, 2016; Taylor, Phillips, & Gertzog, 2018) were not affiliated with the original author’s (Hanley et al., 2014) research laboratory and did not have previous experience under Dr. Hanley’s mentorship. In addition, we identified studies conducted across four geographical locations (i.e., North America, Norway, Ireland, New Zealand). The details of these studies are reported next.
Participant Demographics and Settings
Participant and setting information are summarized in Fig. 1. Participants ranged from 1 to 30 years of age (Median = 6 years old). Diagnoses varied and included autism spectrum disorder (ASD), attention-deficit hyperactivity disorder, oppositional defiant disorder, pervasive developmental disorder–not otherwise specified, mood disorder, generalized anxiety disorder, seizure disorder, dyspraxia, and four individuals with no reported diagnoses. The wide range of diagnoses and ages demonstrate some generality of the IISCA’s effectiveness across differing populations. However, the majority of participants were under the age of 21 and were reported to be diagnosed with ASD. Notably, only one study reported any measurements pertaining to IQ or other adaptive scores that were used when defining the ASD diagnosis (Herman et al., 2018). No other studies provided such information (e.g., IQ, Autism Diagnostic Observation Schedule score [ADOS], Gilliam Autism Rating Scale score), providing minimal information on the severity of ASD symptoms. The IISCA was conducted across various settings, including outpatient clinics, homes, schools, and day habilitation programs. Treatment effects were reported for all but three studies in the home or inpatient setting.

Participant demographic information
Problem behaviors were reported to vary across topographies. The severity and intensity of problem behaviors were reported as being mild to severe; however, no study utilized a standardized assessment to measure the “severity” of behavior (e.g., the SIB Trauma Scale; Iwata, Pace, Kissel, Nau, & Farber, 1990). Although the level of risk to self or others for which the IISCA is effective may benefit from a standardized assessment, the IISCA (as the traditional FA has done on occasion; Smith & Churchill, 2002), has targeted less severe topographies of problem behavior within the same functional class in three studies (e.g., Herman et al., 2018; Jessel, Hanley, & Ghaemmaghami, 2016; Slaton, Hanley, & Raftery, 2017). Seventy-five percent of participants were reported to communicate vocally using between single-word utterances to full sentences, whereas 22% of participants were nonvocal. Two studies did not report language skills, but one did report the use of a standardized assessment to measure IQ and adaptive behavior (Herman et al., 2018).
Analytic Efficiency and Control
Across all 17 studies, the number of control and test conditions of the IISCA varied but ranged from 5 to 10 sessions total, with a median of 5 sessions (i.e., control, test, control, test, test). Session durations were programmed between 3 and 15 min with a median session duration of 5 min. Lastly, the entire analysis (session duration multiplied by the total number of sessions) required between 15 and 100 min to conduct with a median of 25 min. The median reported time to complete the interview and observation was 30 and 20 min, respectively; thus, the entire functional assessment process could take around 75 min to conduct before treatment is introduced. In the original publication, Hanley et al. (2014) conducted the interview during one visit and the IISCA over the subsequent one to four visits. It seems, based on the current review, that the entire assessment process could be completed within one 90-min outpatient visit if the interview, observation, and analysis were conducted on the same day. Assuming an hourly rate of $125 for the BCBA and $75 for the assistant behavior analyst, this visit would cost around $300.
This seems to be a considerable improvement in analytic efficiency from the standard FA. In one of the largest collections of standard FAs published in the literature, Iwata et al. (1994) found the mean duration of 152 analyses to be 6.5 hr (390 min) with a minimum of 2 hr (120 min). Therefore, the mean duration of the 102 IISCAs we reviewed was a 75% improvement to the minimum of that required to conduct the standard FA.
Two studies (Fisher et al., 2016; Slaton et al., 2017) have directly compared the standard FA to the IISCA, across a total of 14 participants who engaged in problem behaviors. Thirteen of 14 participants demonstrated differentiation in the IISCA, whereas the standard FA produced differentiation in 8 of 14 cases. Slaton et al. (2017) found the IISCA to be more efficient, requiring a mean of 28 min to complete, compared to 90 min for the standard FA. Similarly, Fisher et al. (2016) reported that the IISCA took an average of 33 min to complete, compared to 90 min for the standard FA. The IISCA was still reported to be three times more efficient than the standard FA in a within-subject comparison conducted by an independent laboratory.
Finally, Fisher et al. (2016) compared the strength of experimental control across the standard FA and IISCA test and control conditions. Fisher et al. used the same criteria of level of control as described in a previously unpublished work and currently adapted in Jessel, Metras, Hanley, Jessel, and Ingvarsson (2019). The criteria categorized three possible levels of control. Strong control referred to no overlap and minimal problem behavior in the control condition. Moderate control referred to some overall and minimal problem behavior in the control condition. Weak control referred to more than minimal problem behavior in the control. Overall, Fisher et al. reported that strong experimental control was demonstrated in both the IISCA and standard FA formats. Using the same criteria, the first and second authors reviewed experimental control in the only other comparative study (Slaton et al., 2017). We found that 80% of the IISCAs demonstrated strong experimental control compared to 36% when the authors used the standard FA method. Two of the IISCAs were categorized as moderate control, whereas none were considered weak. Comparatively, when the standard FA method was used, 9% were found to be of moderate control, whereas 55% were found to be of weak control. Results were reported with 95% exact interrater agreement.
Furthermore, when the criteria of levels of control are applied to all the IISCAs in the current review, the majority are determined to have strong control (89%), with only a few having moderate (8%) and weak control (3%). Future studies should continue to evaluate the parameters affecting the varying levels of experimental control strength between different FA formats (e.g., latency based, trial based, brief).
Outcomes
Characteristics of the IISCA and the treatment outcomes are summarized in Table 1. The IISCA produced effective treatment gains (i.e., 90% reductions in problem behavior) across all studies. Furthermore, 100% reductions across the entire study were obtained in half of those reviewed. Thus, problem behavior was eliminated, or nearly eliminated, and improved social skills were reported when treatments were informed by the IISCA. All but one study used functional communication training (FCT) as the intervention. Herman et al. (2018) instead used a function-based treatment package that included most-to-least prompting, escape extinction, differential reinforcement, and a high-probability instructional sequence. This package was successful in eliminating problem behavior while increasing the child’s overall compliance with work demands. Three studies did not report treatment subsequent to the IISCA.
Treatment Extensions
Across IISCA studies, social validity was measured via interviews with caregivers, teachers, or staff, using rating scales for 40% of all participants. Experimenters asked parents at the end of each study to rate the effectiveness and feasibility of treatments, as well as their overall experience (Hanley et al., 2014; Jessel, Ingvarsson, Metras, Kirk, et al., 2018). Jessel, Ingvarsson, Metras, Kirk, et al. reported that caregivers rated a 76% decrease in the number of concerns following assessment and treatment. Conversely, there was a 74% increase reported from pre-post evaluation of the number of situations that were not a concern before treatment. All but two caregivers rated the treatment a 7 (highest acceptability) and were satisfied with their child’s behavioral improvements. Social validity could be further assessed when comparing the standard FA to the IISCA and its treatments. This may be especially true as there currently is a lack of social validity data for the entire standard FA and treatment process. Should both formats produce similar treatment outcomes, the pragmatic choice would be to select the FA format that is the most efficient and preferred by clients.
A low percentage of published IISCA studies tested for treatment maintenance effects (20%), ranging from 6 weeks to 2 months. Generalization was tested in 47% of all published studies. Generalization occurred across various areas, such as settings, behaviors, stimuli, and people. Last, treatment integrity was evaluated in 20% of the studies that included some form of intervention; however, when conducted, the treatment was typically conducted with high accuracy.
The lack of these treatment extensions (e.g., maintenance, treatment integrity) is not specific to IISCA-related research. In general, the field of applied behavior analysis demonstrates a significant lack of studies demonstrating generalization and maintenance effects (Ghaemmaghami, Hanley, & Jessel, in press). In a review of studies conducting FCT, Ghaemmaghami et al. (in press) found that we have an abundance of evidence for the efficacy (i.e., demonstration of causal relations) of FCT to reduce problem behavior in experimentally controlled environments, with highly trained professionals, using dense schedules of reinforcement, over a brief evaluation period. However, as we move down the continuum toward effectiveness (i.e., clinical utility) of FCT, we find minimal studies evaluating FCT in the relevant context, conducted by parents or caregivers, using socially validated schedules of reinforcement, across extended periods of time. The results of this review seem to echo the call for more real-world extensions to evaluate the effectiveness of an assessment and treatment process. In other words, we must conduct more research displaying our success in changing the behavior of not only individual change agents but also the systems and comprehensive programs that can be developed for the greater population based on that work.
Novel Developments
The application of an omnibus mand as a functional communication response (FCR), like “my way,” was taught in all but two studies (Beaulieu et al., 2018; Rose & Beaulieu, 2019). The authors instead provided the reinforcers specified by any FCR the participant emitted. These studies exemplify the flexible features of the FCR commonly used in treatment following IISCA from solely omnibus mands to the inclusion of specific mands. Interestingly, teaching an omnibus mand allows for the FCR to generalize to novel contexts in which the participant would like things “their way,” whereas teaching individual responses requires training for each new reinforcer introduced. Future studies may want to evaluate the general therapeutic outcomes across multiple problematic contexts after teaching the omnibus mand for the reinforcers identified during the IISCA. It may be that teaching one mand for the entire synthesized contingency may improve treatment efficiency and the generality of the procedures.
Another important area of inquiry includes the outcomes produced by the IISCA and the standard FA. Fisher et al. (2016) found the standard FA and IISCA produced different hypotheses for reinforcers maintaining the same problem behavior. Fisher et al. identified that the divergence from the standard FA was a false positive. Specifically, the authors purported that the open-ended interview during the IISCA may identify more functionally irrelevant than relevant contingencies, even though only the contingencies specified by the caregivers to occur in the natural environment are evaluated during the IISCA. For instance, the IISCA may have suggested that problem behavior was maintained by escape from parent-directed play to child-directed play (possible combination of attention, escape, and tangibles), whereas the standard FA method only suggested sensitivity to generic forms of attention (e.g., “Don’t do that,” “You are hurting yourself.”). Although an ecologically relevant context is identified during an IISCA, the influence of the individual components of the synthesized reinforcement contingency remain unknown. In general, false positives could be concerning, as Fisher et al. argued that they could lead to more complex and unnecessary treatments; however, the authors did not address this concern directly because treatment was only conducted based on the hypotheses generated from the standard FA. Future research could compare the difficulty and complexity of treatments informed by the interview process to treatments not informed by the interview. This critical examination would allow for the evaluation of the interview process as a crucial component of the IISCA.
Slaton et al. (2017) addressed the aforementioned limitations when they compared treatments following the standard FA method and IISCA for four participants diagnosed with ASD. Treatment consisted of FCT with the response depending on the FA format used (i.e., omnibus mand for the IISCA or specific mand for the standard FA). Their results indicated that FCT informed by the IISCA was more effective at reducing problem behavior and increasing appropriate behaviors for two participants, but it was generally effective for the remaining two participants. In other words, the treatment informed by the IISCA was either just as effective or more effective than the treatments informed by the standard FA. Although preliminary, this finding calls into question the necessity of an extended standard FA process when a more efficient format is available. Future researchers may want to consider furthering this comparative analysis of different FA formats to thin reinforcement schedules that represent more socially acceptable treatment outcomes.
Although the IISCA has demonstrated effective findings, the IISCA and its treatment could be classified as an example of affirming the consequent (Ghaemmaghami, Hanley, Jin, & Vanselow, 2015; Sidman, 1960). Sidman was clear on both the inherent risks with affirming the consequent but also how it could be used to increase confidence in the reliability and generality of data. Specifically, Sidman referred to the logical fallacy that if B is true then A is true. Therefore, should the function-based treatment demonstrate effective results, one may infer that the findings from the assessment must also be true. Demonstrations of affirming the consequent have been exemplified with multiple assessment and treatment procedures in the past (e.g., Ghaemmaghami et al., 2015; Smith, Iwata, Vollmer, & Zarcone, 1993). In essence, the importance of an FA can be determined by its ability to inform effective action during the function-based treatment. This has been identified as a pragmatic form of evaluating the FA (Slaton et al., 2017) and has been referred to as treatment validity or utility in the past (Hayes, Nelson, & Jarrett, 1987; Shapiro & Kratochwill, 2000). The direct comparison of what FAs identify may not be as particularly fruitful as comparisons of treatment outcomes informed by those identified variables. Further comparative studies of different FA formats could use this form of validation.
Discussion
Conclusion
The IISCA has been described to be efficacious, effective, and efficient while producing “meaningful” outcomes. Hanley et al. (2014) referred to “meaningful” results as large, generalizable, and socially valid outcomes emulated from ecologically relevant conditions. Based on this review, it is clear that many of the studies focused on producing meaningful outcomes; however, other important treatment variables need to be further assessed to improve the overall effectiveness of the IISCA. Specifically, treatment integrity, generalization, and maintenance of treatment effects should be further explored with IISCA-based treatments.
Other considerations include the critical examination of the value in synthesizing contingencies during an FA. Future research could directly compare treatment integrity of the interventions developed from isolated and synthesized contingencies to determine the level of difficulty in implementing each of the procedures. On the one hand, it is possible that isolating contingencies could improve accurate implementation because the treatment may require fewer training components. On the other hand, synthesized contingencies that more readily represent the participants’ ecology could reduce the necessity to learn new procedures for unrepresented contexts. In addition, social validity of the treatment procedures may help to determine the level of synthesis preferred by the caregivers and teachers implementing the treatment.
Future research may also aim to standardize measures of global functioning prior to and following treatment for problem behavior informed by the IISCA (Hanley et al., 2014). As previously mentioned, only one study reviewed contained a component of standardized measures of functioning. For example, the ADOS would be an appropriate tool to be used at the outset of the IISCA and again at the end of treatment. In addition, researchers may want to evaluate other, more socially impactful outcomes, such as classroom attendance or changes in IQ if the problem behavior occurs in the school. If the problem behavior occurs in the home, the researcher could collect data on parental stress or the improvement in the participants’ overall well-being using the Clinical Global Impression Scale (Guy, 1976).
Final considerations of the IISCA include its minimal representation of procedural variations. The IISCA was originally designed as a component within a comprehensive and structured assessment and treatment process. This process in its entirety has been replicated but rarely modified. For example, if there is no differentiation between test and control conditions, currently, the recommendation is to return to open-ended questions with the caregiver and conduct further iterations until differentiation occurs. However, significant changes or additions to the conditions and procedures have not been discussed in depth and may contradict the expediency of the IISCA, if required. One recent exception is demonstrated in Jessel, Ingvarsson, Metras, Whipple, et al. (2018), in which the IISCA was modified to test for reinforcing contingencies of elopement by using latency-based measures (similar to the standard FA method; Thomason-Sassi, Iwata, Neidert, & Roscoe, 2011). Researchers may want to evaluate the flexibility of the IISCA and modify the procedures to adapt it to other concerns clinicians may have (e.g., trial based in a classroom setting, single session for severe behavior).
Clinical Recommendations
Overall, the IISCA has been demonstrated to be an effective functional assessment leading to successful treatment outcomes for socially mediated problem behaviors. Especially considering its speedy implementation, we recommend that practitioners consider using the IISCA, as it has been found to inform function-based treatment within as little as one clinical visit. Moreover, the IISCA has (a) improved analytic efficiency while maintaining strong demonstrations of control, (b) been used to develop effective language and skill building among participants, and (c) been found to be highly acceptable among caregivers and teachers.
Although the brevity of the IISCA reduces exposure to a potentially dangerous environment, some practitioners may be concerned with the safety of their clients or staff when any severe problem behavior is evoked. To improve safety during the assessment period, we recommend the careful selection of less severe forms of problem behavior likely to precede the more dangerous topographies. The broadening of the contingency class reduces the likelihood of observing the dangerous forms of problem behavior during the FA period while effectively identifying the appropriately motivating context to begin teaching alternative forms of communication (Borrero & Borrero, 2008; Smith & Churchill, 2002).
We also recommend that clinicians teach omnibus mands that are informed by the synthesized contingency of the IISCA. Although the omnibus mand was not specified to be a defining feature of the assessment and treatment process, it was evaluated during the treatment of the majority of the studies reviewed. Furthermore, it seems the combinatorial nature of the reinforcement contingency during the IISCA is uniquely prepared to motivate and evoke a communication response that produces the entire synthesized outcome.
Last, much like any FA format, the IISCA is not designed to detect automatically maintained problem behavior. As such, our recommendation to practitioners is to identify cases during the open-ended interview and forego the FA entirely when automatic reinforcement is likely to be the sole contributor to the problem behavior. Other screening methods, such as multiple extended alone/ignore sessions, should be conducted in place of the FA to rule out socially mediated environmental consequences and to establish a baseline rate of problem behavior (see Querim et al., 2013).
References
*References marked with an asterisk indicate studies included in the review.
*Beaulieu, L., Van Nostrand, M. E., Williams, A. L., & Herscovitch, B. (2018). Incorporating interview-informed functional analyses into practice. Behavior Analysis in Practice, 11, 385–389. https://doi.org/10.1007/s40617-018-0247-7.
Beavers, G. A., Iwata, B. A., & Lerman, D. C. (2013). Thirty years of research on the functional analysis of problem behavior. Journal of Applied Behavior Analysis, 46, 1–21. https://doi.org/10.1002/jaba.30.
Borrero, C. S., & Borrero, J. C. (2008). Descriptive and experimental analyses of potential precursors to problem behavior. Journal of Applied Behavior Analysis, 41, 83–96. https://doi.org/10.1901/jaba.2008.41-83.
*Fisher, W. W., Greer, B. D., Romani, P. W., Zangrillo, A. N., & Owen, T. M. (2016). Comparisons of synthesized and individual reinforcement contingencies during functional analysis. Journal of Applied Behavior Analysis, 49, 596–616. https://doi.org/10.1002/jaba.314.
*Ghaemmaghami, M., Hanley, G. P., & Jessel, J. (2016). Contingencies promote delay tolerance. Journal of Applied Behavior Analysis, 49, 548–575. https://doi.org/10.1002/jaba.333.
Ghaemmaghami, M., Hanley, G. P., & Jessel, J. (in press). Functional communication training: From efficacy to effectiveness. Journal of Applied Behavior Analysis.
*Ghaemmaghami, M., Hanley, G. P., Jessel, J., & Landa, L. (2018). Shaping complex communication responses. Journal of Applied Behavior Analysis, 51, 502–520. https://doi.org/10.1002/jaba.468.
*Ghaemmaghami, M., Hanley, G. P., Jin, S. C., & Vanselow, N. R. (2015). Affirming control by multiple reinforcers via progressive treatment analysis. Behavioral Interventions, 31, 70–86. https://doi.org/10.1002/bin.1425.
Guy, W. (1976). ECDEU assessment manual for psychopharmacology. Rockville, MD: NIMH Publications.
Hagopian, L. P., Rooker, G. W., Jessel, J., & DeLeon, I. G. (2013). Initial functional analysis outcomes and modifications in pursuit of differentiation: A summary of 176 outpatient cases. Journal of Applied Behavior Analysis, 46, 88–100. https://doi.org/10.1002/jaba.25.
Hanley, G. P. (2012). Functional assessment of problem behavior: Dispelling myths, overcoming implementation obstacles, and developing new lore. Behavior Analysis in Practice, 5, 54–72. https://doi.org/10.1007/BF03391818.
*Hanley, G. P., Jin, C. S., Vanselow, N. R., & Hanratty, L. A. (2014). Producing meaningful improvements in problem behavior of children with autism via synthesized analyses and treatments. Journal of Applied Behavior Analysis, 47, 16–36. https://doi.org/10.1002/jaba.106.
Hayes, S. C., Nelson, R. O., & Jarrett, R. B. (1987). The treatment utility of assessment: A functional approach to evaluating assessment quality. American Psychologist, 42, 963–974. https://doi.org/10.1037/0003-066X.42.11.963.
*Herman, C., Healy, O., & Lydon, S. (2018). An interview-informed synthesized contingency analysis to inform the treatment of challenging behavior in a young child with autism. Developmental Neurorehabilitation, 21, 202–207. https://doi.org/10.1080/17518423.2018.1437839.
Iwata, B. A., Dorsey, M. F., Slifer, K. J., Bauman, K. E., & Richman, G. S. (1994). Toward a functional analysis of self-injury. Journal of Applied Behavior Analysis, 27, 197–209. (Reprinted from Analysis and Intervention in Developmental Disabilities, 2, 3–20, 1982). https://doi.org/10.1901/jaba.1994.27-197.
Iwata, B. A., Pace, G. M., Dorsey, M. F., Zarcone, J. R., Vollmer, T. R., Smith, R. G., . . . Goh, H. L. (1994). The functions of self-injurious behavior: An experimental-epidemiological analysis. Journal of Applied Behavior Analysis, 27, 215–240. https://doi.org/10.1901/jaba.1994.27-215
Iwata, B. A., Pace, G. M., Kissel, R. C., Nau, P. A., & Farber, J. M. (1990). The Self-Injury Trauma (SIT) Scale: A method for quantifying surface tissue damage caused by self-injurious behavior. Journal of Applied Behavior Analysis, 23, 99–110. https://doi.org/10.1901/jaba.1990.23-99.
*Jessel, J., Hanley, G. P., & Ghaemmaghami, M. (2016). Interview-informed synthesized contingency analysis: Thirty replications and reanalysis. Journal of Applied Behavior Analysis, 49, 576–595. https://doi.org/10.1002/jaba.316.
*Jessel, J., Ingvarsson, E. T., Metras, R., Kirk, H., & Whipple, R. (2018). Achieving socially significant reductions in problem behavior following the interview-informed synthesized contingency analysis: A summary of 25 outpatient applications. Journal of Applied Behavior Analysis, 51, 130–157. https://doi.org/10.1002/jaba.436.
*Jessel, J., Ingvarsson, E. T., Metras, R., Whipple, R., Kirk, H., & Solsbery, L. (2018). Treatment of elopement following a latency-based interview-informed, synthesized contingency analysis. Behavioral Interventions, 33, 271–283. https://doi.org/10.1002/bin.1525.
Jessel, J., Metras, R., Hanley, G. P., Jessel, C., & Ingvarsson, E. T. (2019). Evaluating the boundaries of analytic efficiency and control: A consecutive controlled case series of 26 functional analyses. Journal of Applied Behavior Analysis. Advanced online publication. https://doi.org/10.1002/jaba.544.
*Lambert, J. M., Staubitz, J. E., Torelli Roane, J., Houchins-Juárez, N. J., Juárez, A. P., Sanders, K. B., & Warren, Z. E. (2017). Outcome summaries of latency-based functional analyses conducted in hospital inpatient units. Journal of Applied Behavior Analysis, 50, 487–494. https://doi.org/10.1002/jaba.399.
Oliver, A. C., Pratt, L. A., & Normand, M. P. (2015). A survey of FBA methods used by behavior analysts in practice. Journal of Applied Behavior Analysis, 48, 817–829. https://doi.org/10.1002/jaba.256.
Querim, A. C., Iwata, B. A., Roscoe, E. M., Schlichenmeyer, K. J., Virues Ortega, J., & Hurl, K. E. (2013). Functional analysis screening for problem behavior maintained by automatic reinforcement. Journal of Applied Behavior Analysis, 46, 47–60. https://doi.org/10.1002/jaba.26.
Rose, J. C., & Beaulieu, L. (2019). Assessing the generality and durability of interview-informed functional analyses and treatment. Journal of Applied Behavior Analysis, 52, 271-285. https://doi.org/10.1002/jaba.504.
*Santiago, J. L., Hanley, G. P., Moore, K., & Jin, C. S. (2015). The generality of interview-informed functional analyses: Systematic replication in school and home. Journal of Autism and Developmental Disorders, 46, 797–811. https://doi.org/10.1007/s10803-015-2617-0.
Shapiro, E. S., & Kratochwill, T. R. (2000). Behavioral assessment in schools. New York, NY: The Guilford Press.
Sidman, M. (1960). Tactics of scientific research: Evaluating experimental data in psychology (Vol. 5). New York, NY: Basic Books.
Slaton, J. D., & Hanley, G. P. (2018). Nature and scope of synthesis in functional analysis and treatment of problem behavior. Journal of Applied Behavior Analysis, 51, 943–973. https://doi.org/10.1002/jaba.498.
*Slaton, J. D., Hanley, G. P., & Raftery, K. J. (2017). Interview-informed functional analyses: A comparison of synthesized and isolated components. Journal of Applied Behavior Analysis, 50, 252–277. https://doi.org/10.1002/jaba.384.
Smith, R. G., & Churchill, R. M. (2002). Identification of environmental determinants of behavior disorders through functional analysis of precursor behaviors. Journal of Applied Behavior Analysis, 35, 125–136. https://doi.org/10.1901/jaba.2002.35-125.
Smith, R. G., Iwata, B. A., Vollmer, T. R., & Zarcone, J. R. (1993). Experimental analysis and treatment of multiply controlled self-injury. Journal of Applied Behavior Analysis, 26, 183–196. https://doi.org/10.1901/jaba.1993.26-183.
*Strand, R. C., & Eldevik, S. (2017). Improvements in problem behavior in a child with autism spectrum diagnosis through synthesized analysis and treatment: A replication in an EIBI home program. Behavioral Interventions, 33, 102–111. https://doi.org/10.1002/bin.1505.
*Strohmeier, C. W., Murphy, A., & O’Connor, J. T. (2016). Parent-informed test-control functional analysis and treatment of problem behavior related to combined establishing operations. Developmental Neurorehabilitation, 20, 247–252. https://doi.org/10.3109/17518423.2015.1133723.
*Taylor, S. A., Phillips, K. J., & Gertzog, M. G. (2018). Use of synthesized analysis and informed treatment to promote school reintegration. Behavioral Interventions, 33, 364–379. https://doi.org/10.1002/bin.1640.
Thomason-Sassi, J. L., Iwata, B. A., Neidert, P. L., & Roscoe, E. M. (2011). Response latency as an index of response strength during functional analyses of problem behavior. Journal of Applied Behavior Analysis, 44, 51–67. https://doi.org/10.1901/jaba.2011.44-51.
Author Note
The authors would like to thank Mary Jane Weiss and Sarah Frampton for their critical feedback and insight on previous versions of this manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflicts of interest.
Ethical Approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Additional information
This manuscript has not been previously published and has not been or will not be submitted elsewhere during the review process.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Coffey, A.L., Shawler, L.A., Jessel, J. et al. Interview-Informed Synthesized Contingency Analysis (IISCA): Novel Interpretations and Future Directions. Behav Analysis Practice 13, 217–225 (2020). https://doi.org/10.1007/s40617-019-00348-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40617-019-00348-3