
Abstract
No research has used latency-based functional analysis (FA) outcomes as baseline data from which to evaluate the effectiveness of subsequent function-based treatments. This approach to analysis calls for the continued collection of latency-based measures for all targeted variables throughout all phases of treatment. We tracked client progress during treatment using latency-based, rate-based, and percentage-of-opportunity measures of relevant behavior and compared graphical representations of each. Visual inspection of all data indicates that changes in variability level and trend of latency-based measures correspond well with said changes in more traditional measures.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Some researchers have used functional analysis (FA; Iwata et al. 1984/1992) outcomes as baseline data from which to evaluate the effectiveness of subsequent treatments (e.g., Baker et al. 2006; Lloyd et al. 2014). Practitioners with limited time could benefit from replicating this approach to analysis because of its potential to increase the efficiency of service delivery (i.e., they do not need to conduct additional baseline sessions after an FA has been completed). For similar reasons, this approach has the potential to decrease caregiver objection to essential pretreatment activities. Specifically, it allows practitioners to spend less time determining the degree to which problem behavior occurs given the presence of counter-therapeutic contingencies, relevant establishing operations (EO; Laraway et al. 2003), and discriminative stimuli (SD), potentially reducing the need to justify this difficult-to-understand yet important practice.
Another way that practitioners might decrease caregiver objection to important pretreatment activities is by selecting a variation of traditional FA methodology that requires fewer instances of problem behavior to establish functional relationships. For instance, latency-based FAs occasion a small fraction of the problem behavior commonly seen during traditional FAs but produce results whose interpretations closely align with those of traditional FAs (Thomason-Sassi et al. 2011).
Latency-based FA data allows practitioners to say with confidence that, in the absence of treatment, specific EOs and SDs will evoke problem behavior within (for instance) 40 s of their initial presentation. Thus, if practitioners continue to track latency to first response per unit of time during treatment, then they can determine how exposure to said treatment alters these latencies across time.
Generating latency-based measures of progress during treatment requires only slight changes to baseline session protocol. Whereas therapists end sessions contingent upon the first occurrence of problem behavior during latency-based FAs, therapists continue to conduct sessions for a prespecified period of time (e.g., the maximum session duration of the latency-based FA) during treatment and only end data collection after the first instances of relevant dependent variables.
To date, no research has used latency-based FA outcomes as baseline for latency-based measures of treatment effectiveness. Although the process for collecting latency-based measures during treatment is relatively straightforward, it is unclear whether practitioners would draw the same conclusions about treatment effectiveness when analyzing latency-based treatment data as they do when analyzing rate-based treatment data. Thus, the purpose of this study was to track various dimensions of dependent variables during a multiphase treatment to determine whether visual analysis of graphical representations of each would lead to similar conclusions regarding treatment effectiveness.
Alison was a 5-year-old girl diagnosed with an autism spectrum disorder who could respond appropriately to, and emit, vocal verbal communication. Alison’s vocabulary appeared to be age appropriate and she often participated in intraverbal exchanges with others. She was referred to a university-based outpatient behavior clinic for aggression. Appointments occurred twice weekly in an empty room of Alison’s home. Graduate students studying special education served as observers and therapists for all study phases.
We defined aggression as any forceful physical contact between Alison (or an object controlled by Alison) and another individual as well as any attempt to damage objects in the surrounding environment. We defined a mand as any instance in which Alison independently combined the words “break” and “please” in a single sentence and/or touched a therapist with a corresponding picture card. We defined compliance as the successful completion of a requested task within 10 s of its initial presentation (e.g., prior to manual guidance). We defined noncompliance as the non-completion of a requested task within 10 s of its initial presentation (regardless of whether a reinforced mand followed the initial demand).
Trained observers collected data on dependent variables during all study phases using handheld computers with ABC Data Pro® software. We evaluated interobserver reliability of rate-based measures by averaging mean count-per-interval (10 s) scores for all relevant responses. Mean rate-based reliability was 94.9 % (range 90.9–98.4) across 29 % of sessions. We calculated reliability scores for latency-based data by comparing raw data streams generated by each observer. If latency to first response fell within ±10 s across observers, we scored an agreement. Otherwise, we scored a disagreement. We then divided agreements by agreements plus disagreements and multiplied by 100. Mean reliability for latency-based measures was 93.4 % (range 66.7–100) across 39.5 % of sessions. We evaluated therapist fidelity to programmed procedures using yes/no checklists during 62.5 % of all sessions. Therapist fidelity was 100 %.
Prior to treatment, we alternated escape and ignore conditions (Kahng and Iwata 1998) of a latency-based FA to test a hypothesized escape function of Alison’s aggression. Maximum session duration was 5 min, and therapists did not initiate a new session until a full minute had passed without aggression. During the escape condition, the therapist presented a continuous series of demands using a three-step prompting procedure (i.e., vocal, model, manual guidance). Compliance produced praise and a new demand. Aggression produced a 30-s break and session termination. During the ignore condition, therapists ignored all subject behavior and aggression did not terminate sessions. Sessions from the escape condition served as baseline during the subsequent treatment evaluation.
We implemented functional communication training (FCT; Carr and Durand 1985) during the initial phase of treatment. All sessions lasted 5 min yet differed from the escape condition in a number of ways. First, therapists provided Alison with a contingency review prior to each session (e.g., “If you hurt me you will have to keep working. If you need a break, say, ‘break please’”). Second, therapists placed aggression on extinction and reinforced mands with 30-s breaks. Third, a second therapist manually guided Alison to exchange her picture card if she did not independently mand within the allotted time frame. Specifically, during the first session of FCT, the therapist prompted a picture exchange immediately following every demand presentation. After each subsequent session, the prompt delay increased by 5 s. Once Alison independently manded at least once during each of three consecutive sessions in which aggression did not occur, we returned to baseline’.
Baseline’ was identical to the escape condition with one exception. Sessions lasted 5 min and did not end following the first instance of aggression. Alison remained in baseline’ until a counter-therapeutic trend in aggression was observed. Then, we re-implemented FCT and again eliminated aggression.
Signaling schedule changes with distinct stimulus conditions can bring rapid control of these schedules over behavior (e.g., Hanley et al. 2001) and can facilitate the systematic leaning of initially dense reinforcement schedules without weakening response-reinforcer contingencies in appropriate contexts (e.g., Fisher et al. 1998).
Thus, following FCT, therapists conducted discrimination training using a two-component chained schedule to help Alison distinguish contexts in which mands would be reinforced with breaks (SD components) from those in which mands would be placed on extinction and compliance was required (S∆ components; Lambert et al. submitted for publication). Therapists signaled S∆ components by wearing a red silicone bracelet and saying, “bracelet is on, you need to work.” Therapists signaled SD components by taking the bracelet off and saying, “bracelet is off, you can ask for a break.” We displayed the time remaining in current components using a visual timer on an iPad® with TimeTimer® software.
Each session started in the SD component. During SD, we placed aggression and noncompliance on extinction and reinforced each mand with a 30-s break. Transition from SD to S∆ occurred on a fixed-time (FT) 60 s. During S∆, we placed mands, noncompliance, and aggression on extinction and transitioned from S∆ back to SD following the successful completion of a single 40-s resetting DRO interval. That is, we transitioned to the SD component following 40 consecutive seconds of compliance in the absence of aggression. If aggression or noncompliance occurred during S∆, a therapist reset the visual timer while stating “I’m resetting the timer.”
Following sessions in which no aggression occurred, we increased the value of each component by 50 % until reaching a terminal value of 300 s within a 10-min session (we switched to 10-min sessions to compensate for increased component durations).
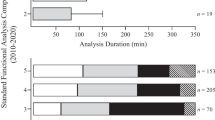
The top panel of Fig. 1 shows latency-based measures of aggression, manding, and compliance during Alison’s FA, FCT, and discrimination training. The middle panel shows rate-based measures of aggression and manding during FCT and discrimination training. The bottom panel shows compliance depicted as a percentage of opportunities (i.e., compliance/[compliance + noncompliance] × 100) during discrimination training. During the FA, shorter latencies in escape relative to ignore conditions indicated an escape function of Alison’s aggression. FCT suppressed aggression and increased mands. Discrimination training brought mands under the control of “bracelet off” and compliance under the control of “bracelet on.”

Latency-based measures of aggression, manding, and compliance during Alison’s FA, FCT, and discrimination training (top panel). Rate-based measures of aggression and manding during FCT and discrimination training (middle panel). Compliance depicted as a percentage of opportunities during discrimination training (bottom panel)
As has been noted in previous research on latency-based FAs (e.g., Thomason-Sassi et al. 2011) short and long latencies to Alison’s behavior corresponded with high and low rates of said behavior. Additionally, trends and variability in latency-based data corresponded to trends and variability in rate-based data. Thus, our results suggest that graphical representations of latencies to the first response of important dependent variables during treatment can lead practitioners to draw similar conclusions about the effectiveness of that treatment to those drawn when analyzing graphical representations of more traditional forms of data.
One important distinction between baseline sessions and treatment sessions must be made. Whereas baseline (FA) sessions ended after the first instance of problem behavior, treatment sessions did not. Rather, treatment sessions typically ended after 5 min elapsed. By programming data collection to occur at the onset of each 5 (or 10)-min block of therapy, we were able to ensure the client had adequate opportunities to contact therapeutic contingencies while simultaneously producing the structure from which to derive valid samples of client progress across time. That is, by predetermining session duration, it was possible for us to track the cumulative effect that each 5 (or 10)-min block of therapy had on the latencies to behavior from the onset of relevant EOs and SDs.
Two limitations of this study should be noted. First, we did not collect data on latency to mands or compliance during our FA. Tracking these variables during baseline in future research or practice has the potential of providing a more streamlined record of progress. Second, only one subject participated in this study and so the generality of our findings is unknown.
Notwithstanding, this study provides an applied example of how data collection during treatment might be structured in order to allow latency-based FA results to function as baseline data. Similarly, our results show that latency-based measures of dependent variables can generate conclusions about treatment efficacy similar to those generated by more traditional measures. One potential benefit of collecting latency-based data during treatment is that they require less effort to obtain than rate-based data. Thus, practitioners may opt to track latency instead of rate when they must collect their own data and treatment is effortful.
References
Baker, J. C., Hanley, G. P., & Mathews, R. M. (2006). Staff-administered functional analysis and treatment of aggression by an elder with dementia. Journal of Applied Behavior Analysis, 39, 469–474. doi:10.1901/jaba. 2006.80-05.
Carr, E. G., & Durand, V. M. (1985). Reducing behavior problems through functional communication training. Journal of Applied Behavior Analysis, 18, 111–126. doi:10.1901/jaba. 1985.18-111.
Fisher, W. W., Kuhn, D. E., & Thompson, R. H. (1998). Establishing discriminative control of responding using functional and alternative reinforcers during functional communication training. Journal of Applied Behavior Analysis, 31, 543–560. doi:10.1901/jaba. 1998.31-543.
Hanley, G. P., Iwata, B. A., & Thompson, R. H. (2001). Reinforcement schedule thinning following treatment with functional communication training. Journal of Applied Behavior Analysis, 34, 17–38. doi:10.1901/jaba. 2001.34-17.
Iwata, B. A., Dorsey, M. F., Slifer, K. J., Baumen, K. E., & Richman, G. S. (1982/1994). Towards a functional analysis of self-injury. Journal of Applied Behavior Analysis, 27, 197-209. doi:10.1901/jaba.1994.27-197.
Kahng, S. W., & Iwata, B. A. (1998). Play versus alone conditions as controls during functional analyses of self-injurious escape behavior. Journal of Applied Behavior Analysis, 31, 669–672. doi:10.1901/jaba. 1998.31-669.
Lambert, J. L., Doyle, A. M., Barrows, S. B., & Houchins-Juarez, N. J. (submitted for publication). Two variations of traditional FA methodology for assessing the function of noncompliance: with treatment evaluation. Journal of Applied Behavior Analysis.
Laraway, S., Snycerski, S., Michael, J., & Poling, A. (2003). Motivating operations and terms to describe them: some further refinements. Journal of Applied Behavior Analysis, 36, 407–414. doi:10.1901/jaba. 2003.36-407.
Lloyd, B. P., Wehby, J. H., Weaver, E. S., Goldman, S. E., Harvey, M. N., & Sherlock, D. R. (2014). Implementation and validation of trial-based functional analyses in public elementary school settings. Journal of Behavioral Education. doi:10.1007/s10864-014-9217-5.
Thomason-Sassi, J., Iwata, B. A., Neidert, P. L., & Roscoe, E. M. (2011). Response latency as an index of response strength during functional analyses of problem behavior. Journal of Applied Behavior Analysis, 44, 51–67. doi:10.1901/jaba. 2011.44-51.
Acknowledgments
We would like to thank Gounah Choi and Destiney Young for their assistance with the conceptualization and implementation of this project. We also thank the Treatment and Research Institute for Autism Spectrum Disorders (TRIAD) for providing clinic space.
Compliance with Ethical Standards
This manuscript is not under review, nor has it been published, elsewhere. This submission has been approved by all authors and by the responsible authorities where the work was carried out. The participant’s guardian provided informed consent for her daughter’s participation in this study before we initiated study-related activities.
Author information
Authors and Affiliations
Corresponding author
Additional information
Implications for Practitioners
• Decrease probability of high rates of problem behavior during assessment
• Potentially decrease caregiver objection to pretreatment activities
• Increase efficiency of service delivery
• Decrease effort of meaningful data collection
Rights and permissions
About this article

Cite this article
Caruthers, C.E., Lambert, J.M., Chazin, K.M. et al. Latency-Based FA as Baseline for Subsequent Treatment Evaluation. Behav Analysis Practice 8, 48–51 (2015). https://doi.org/10.1007/s40617-015-0046-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40617-015-0046-3