
Abstract
Objectives
Immigrants to the USA have disparate access to health insurance coverage and healthcare services. We evaluate the effects of gaining insurance following the January 2014 Affordable Care Act’s (ACA) key provisions implementation on health services use among foreign- (FB) and US-born (USB) adults.
Methods
Longitudinal data from two panels (2013/2014 and 2014/2015) of the Medical Expenditure Panel Survey on FB and USB adults, ages 26–64 (unweighted n = 15,232), and difference-in-differences analysis using generalized estimating equations were used to estimate the effects of insurance gain. The primary outcomes were five measures of healthcare utilization including yearly routine care appointment, annual number of physician office visits, annual number of prescription medications filled or refilled, use of the emergency department (ED) during the year, and having an inpatient hospital stay during the year.
Results
Immigrants were more likely to gain health insurance between 2013 and 2015 relative to USB adults (6.3% vs. 4.4%) but remained much more likely to be continuously uninsured by 2015 (20.8% vs. 6.4%). Controlling for sociodemographic and health characteristics, FB and USB adults who gained insurance increased their use of health services, including routine care (absolute change ΔFB = 15.7%; p < 0.001 and ΔUSB = 11.7%; p < 0.001), office-based doctor visits (ΔFB = 1.3; p < 0.001 and ΔUSB = 0.6; p < 0.001), prescribed medications (ΔFB = 2.5; p < 0.001 and ΔUSB = 1.6; p = 0.016), and inpatient hospitalizations (ΔFB = 3.6%; p = 0.017 and ΔUSB = 3%; p < 0.001). ED use increased only among the FB (ΔFB = 4.8%; p < 0.001). Gaining insurance eliminated the differences in health services use for all considered outcomes among the FB relative to the continuously insured USB.
Conclusions
US immigrants had notable gains in health insurance after the ACA provisions took full effect, but major disparities in coverage persist. If insurance continues to expand among immigrants, then the gains may reduce longstanding disparities in health services use and enhance primary and preventive healthcare.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The Affordable Care Act (ACA) was designed to substantially reduce the number of uninsured in the United States of America (USA). In January 2014, the bulk of the ACA’s regulatory mandates took effect. These mandates include rules governing the structure of private health insurance policies nationwide, the creation of health insurance exchanges to serve individuals and small businesses sponsoring health insurance, the extension of Medicaid in many states to low-income individuals, the creation of federally funded premium subsidies for low-income individuals buying health insurance in the exchanges and tax credits for small businesses sponsoring employment-based insurance plans, and most importantly, federal requirements and penalties linked to having health insurance. [1] The ACA, however, maintains limitations in coverage (e.g., Medicaid restrictions, and years of residence-waiting periods) for certain immigrant groups, requires verifications for citizenship and legal documentation for federal coverage, and entirely excludes the undocumented. [2,3,4] Recent political pressures in the USA foretell a potentially more restrictive policy environment targeting this population.
Immigrants now comprise 13.3% of the US population and the Census Bureau projects this share will grow to close to 20% by 2050. [5] Un-insurance and under-insurance have been longstanding problems among immigrants to the USA. [6,7,8] Independent of time spent in the USA, employment status, ethnic background, and legal status, many immigrants face barriers to obtaining health insurance and sustaining such coverage. [6,7,8,9,10,11] Despite known disparities in health insurance coverage, access to both preventive and non-preventive services, and the receipt of care among immigrants, [9, 12,13,14,15,16,17] to date, no studies have looked at the effects of the ACA on immigrants using longitudinal data. Such data, collected from the same individuals over time, is critical for establishing causal inference, and can be especially important for testing change consequent to a systemic shock, such as the one introduced by the ACA.
Cross-sectional studies indicate that the ACA has, so far, had numerous beneficial effects for several segments of the US population. Among young adults, for example, its dependent coverage provisions have led to major coverage gains and improved physical and mental health. [18,19,20] Among low-income adults, coverage became more affordable and use of emergency departments (EDs) declined. Medicaid expansion in states such as Kentucky substantially improved health among low-income adults, relative to comparable low-income adults in neighboring states, such as Texas, that did not expand Medicaid. These health improvements were attributed to more primary care visits, a greater focus on prevention, improved care management for chronic conditions, and reductions in the inefficient use of EDs. [20, 21] Early findings regarding the ACA’s effects within the general population are also encouraging. Analyses of data from state and federal surveys, such as the Behavioral Risk Factor Survey and the National Health Interview Survey, as well as data from Gallup (e.g., the Gallup Healthways Well-Being Index), reveal that the ACA’s 2014 reforms increased insurance coverage, and that those coverage gains were associated with improvements in health, better primary care, greater access to prescription medications, and improvements in the affordability of care. [20, 22, 23]
The overarching goal of this study is to examine three important aspects of how coverage and healthcare use among foreign- (FB) vs. US-born (USB) adults changed following the 2014 reforms. We used longitudinal data from two consecutive panels from the Medical Expenditure Panel Survey (MEPS) to [1] examine how health insurance coverage changed among immigrants and USB adults, [2] test how gaining insurance coverage changed healthcare utilization between the two groups, and [3] consider whether the changes in insurance and healthcare utilization have reduced disparities between the two groups.
Methods
Data
We analyzed data from the 2013–2015 Medical Expenditure Panel Survey (MEPS) longitudinal files. Each year, MEPS collects survey data from a panel of individuals who are followed over 2 years. MEPS respondents are a nationally representative subsample of respondents to the National Health Interview Survey. The 2013–2015 MEPS includes data from two consecutive panels, gathered from n = 16,714 individuals in 2013–2014 and n = 15,898 in 2014–2015, and is the most comprehensive source of information on healthcare utilization and expenditures in the USA. Additionally, MEPS collects detailed information on participants’ health, medical conditions, and demographic and socioeconomic characteristics. The MEPS data files and their documentations are de-identified to ensure participant’s privacy and publicly available from the Agency for Healthcare Research and Quality (AHRQ; https://meps.ahrq.gov/). Research using publicly available de-identified data are exempt from review as determined by the Institutional Review Board following Department of Health and Human Services Regulations.
Analytic Subpopulation
We focused on adults ages 26 years and older in 2013 and 2014, our baseline years, and younger than 65 years by 2014 and 2015, correspondingly our follow-up years (n = 15,773). MEPS data are longitudinally weighted for target population representation. We exclude adults under age 26 because, beginning in 2010, the ACA allowed parents to extend dependent coverage to their children ages 18–25. We further exclude n = 541 participants with missing values on any of the model covariates. Our unweighted analytic sample consists of npanel18 = 7752 and npanel19 = 7480 individuals (the weighted equivalent of 156 million adults represented in each panel), np18 = 2429 and np19 = 2384 (the weighted equivalent of 30.4 million adults represented in each panel) of whom are FB.
Change in Health Insurance Coverage
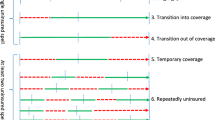
We operationalized insurance coverage based on multiple sources including private, TRICARE, Medicaid or SCHIP, Medicare, and other public sources. Our insurance indicator summarizes information from all these sources and conservatively assigns participants to the “uninsured” category if they had no coverage from any of these sources for the entire year. We constructed a 4-category indicator to distinguish between respondents who (1) were continuously uninsured over the baseline and follow-up years in each panel, (2) were continuously insured over both years, (3) lost insurance in the follow-up year, and (4) gained insurance in the follow-up year.
Yearly Use of Health Services
We examined (1) whether the respondent scheduled any appointment(s) for routine care, (2) total number of reported visits to an office-based physician, (3) total prescription medications filled, (4) whether they reported any visits to an emergency department (ED), and (5) whether they reported any overnight hospital stay(s). The first three suggest an efficient use of resources (in line with the primary care model), whereas the fourth and fifth may signal inefficiency. It should be noted that current US laws prohibit EDs from discriminating in the provision of care based on insurance status.
Nativity
Whether the respondent was born in or outside the USA (0 = FB; 1 = USB) was measured based on self-reported information (immigrant and FB are used interchangeably in text to refer to participants born outside the USA).
Covariates
We adjusted for an individual’s gender, ethnicity/race (non-Hispanic White, Hispanic, non-Hispanic Black, and non-Hispanic other), and educational attainment (less than high school (HS), HS or equivalent, some college, or a college degree). Our time-varying indicators included age in years, census region (Northeast, South, Midwest, or West) of residence, annual household income relative to the federal poverty level (FPL) (poor or < 100%, near poor or 100 ≤ 125%, low income or 125 ≤ 200%, middle income or 200 ≤ 400%, and high income > 400%), whether the individual was employed during the year, and self-reported general health and mental health, both measured on a five-point scale (excellent, very good, good, fair, or poor). We also controlled for a dichotomous fixed effect panel indicator (0 = 18, 1 = 19) to account for unobserved period-specific differences.
Analysis
To ensure that our results do not reflect secular trends, we calculated, tested, and plotted time changes in the probabilities of continuous un-insurance (i.e., being uninsured over both years in each panel) and continuous insurance (i.e., being insured over both years in each panel) over 4 MEPS panels (2 preceding, 1 overlapping with, and 1 following the 2014 ACA implementation) stretching over the years 2011–2015 (SF1).
All following analyses focused on data from panels 18 (2013/2014) and 19 (2014/2015). We first compared FB and USB adults ages 26–64 on variables used in the analysis, and subsequently tested for statistically significant differences in characteristics between the groups (Table 1). For categorical variables, we used Rao-Scott survey-adjusted chi-squared tests, and for continuous variables, we used t tests. Panel-specific characteristics by nativity status are presented in (ST1).
Second, using data from the combined panels, we examined how change in insurance status varied depending on the baseline characteristics of individuals, and plotted these variations for the foreign and USB groups (Fig. 1). Detailed estimates are provided in ST2. Additionally, we re-examined variations in insurance status change by these characteristics independently within each panel to assess whether insurance gains were sustained or have slowed down differentially over time. Panel-specific estimates for the foreign and USB groups are included in ST3 and SF2.

Prevalence of continuous un-insurance and insurance gains. Prevalence of continuous un-insurance and insurance gains following the Affordable Care Act implementation across nativity groups and by baseline characteristics. Change in status is from the baseline years (2013 and 2014) to year 2 (2014 and 2015) in panels 18 and 19 of the Medical Expenditure Panel Survey (MEPS). Results are based on participants ages 26+ years at baseline to < 65 years in year 2 from the longitudinal files of the MEPS. 1FB = foreign born, USB = US born. 2NH White = non-Hispanic White. 3LTHS = less than high school, GED/HS = high school or GED. 4Poverty status is based on income to poverty ratios as created by the Agency for Healthcare Research and Quality: < 100% of poverty level = poor; 100 ≤ 125% = near poor; 125 ≤ 200% = low income; 200 ≤ 400% = middle income; and 400%+ = high income. 5SRG = self-reported general health. 6SRM = self-reported mental health
Third, we estimated a series of differences-in-differences (DD) models using multinomial logistic regressions to test how nativity status relates to insurance status after controlling for various individual characteristics. Five models were estimated, which incrementally accounted for nativity status and panel (M1), additionally adjust for age, gender, and census region (M2), for race/ethnicity (M3), for education, household income, and employment (M4), and for health status (M5). In a sensitivity analysis (M6), we also controlled for 4 measures that probe an individual’s preference for healthcare and insurance, and their attitudes towards risk-taking based on agreements to the following statements: (1) Do not need health insurance; (2) health insurance not worth cost; (3) more likely to take risks; and (4) can overcome health issues without help; all measured on a 5-point scale (1 = disagree strongly–5 = agree strongly). For each model, we reported the estimated differences between US and FB adults in marginal probabilities of classification in each of the four insurance groups and their 95% confidence intervals (CIs) (Fig. 2). [24] We provide the estimated odds ratios of a USB vs. an FB adult being in each of the insurance categories and the estimated differences in probabilities resulting from these models along with 95% CIs for the estimates in ST4 and ST5, respectively. To examine whether these estimated group differences varied over panels, we estimated differences-in-differences-in-differences (DDD) by refitting all regression models detailed above to include interactions between the panel indicator and model covariates. This is similar to estimating multinomial logistic regression models independently in each panel yet allowed us to directly test changes in estimates between FB and USB groups over panels. Odds ratios and marginal estimates from DDD models are provided in ST6 and ST7, respectively, and plotted in SF3 and SF4.

Estimated differences in marginal probabilities of insurance status between US and foreign-born adults. Results are based on estimates from multinomial logit model (reference outcome set to continuously insured) data using participants ages 26+ years at baseline to < 65 years in year 2 from the longitudinal files of the Medical Expenditure Panel Survey (2013–2015). Model 1 (M1) is crude, M2 adjusts for age and sex, M3 = M2+ race/ethnicity, M4 = M3+ poverty status, education, and employment, M5 = M4+ self-reported general and mental health, and M6 (sensitivity model) = M5+ attitudes about insurance and health risk taking (do not need health insurance; health insurance not worth cost; more likely to take risks; can overcome health issues without help) are all measured on a 5-point scale (1 = disagree strongly–5 = agree strongly). Δ (USB−FB) is the difference in estimated marginal probability of a specific insurance status between USB and FB adults. The lines represented through the markers represent 95% confidence intervals
Fourth, we fit generalized estimation equations (GEEs) to examine the associations between gaining insurance and healthcare utilization measures and test for differential utilization effects by nativity status. [24] GEEs are population average analytic techniques that account for the dependence in outcome measurements (here time nested within participants) through pre-specified covariance structures. GEEs have good properties in large samples, such as MEPS, are robust to misspecification of working covariance structures, and can accommodate multiple outcome distributions and link functions. [24, 25] For each of the five utilization measures, we estimated (1) a “crude” model that adjusts only for the main and interaction effects of nativity, insurance, and survey year, and (2) a covariate-adjusted model that also adjusts for time invariant (gender, ethnicity/race, education) and time-varying measures (age, region, income, employment, and self-rated general and mental health). For the binary utilization measures—scheduled an appointment for routine care, had an ED visit, and had an inpatient stay—we adopted a binomial family and logit link, and for the count measures—number of office visits and number of prescriptions filled—we adopted a negative binomial family. For sensitivity analyses, we also considered a Poisson family; the results from Poisson family models were quantitatively and qualitatively consistent with the negative binomial findings. All models assumed an unstructured covariance matrix.
After fitting the models, we examined multiple ANOVA-style contrasts to determine and test time-specific group differences in marginal means/probabilities of the outcomes as well as other conditional effects. The estimated marginal means and probabilities of healthcare services use pre- and post-gaining insurance by nativity status are plotted with their 95% confidence intervals in Fig. 3. The estimated absolute change in healthcare services use, resulting from the tested contrasts, and the differences in change by nativity status are plotted in Fig. 4 and detailed in ST8.

Estimated marginal probabilities and means of healthcare services use. The estimated marginal probabilities and means of healthcare services use are for uninsured respondents in who became insured post-ACA enactment by nativity status. Results are based on Generalized Estimation Equation (GEE) models fit to test the longitudinal association between insurance status and five health services use outcomes using data on ages 26+ years at baseline to <65 years in year 2 from the longitudinal files of the Medical Expenditure Panel Survey (2013–2015). Adjusted models control for sex, race/ethnicity, education, and time-varying measures of age in years, poverty status, employment, and self-reported general and mental health. Estimated values are included over the bars. Upper 95% confidence intervals values are represented by the lines attached to each bar

Fully adjusted estimates of absolute change (%) and difference in change in healthcare services use. The fully adjusted estimates of absolute change (%) in healthcare services use, and difference in change for uninsured respondents who became insured post-ACA enactment by nativity status. Results are based on generalized estimation equation (GEE) models fit to test the longitudinal association between insurance status and five health services use outcomes using data on ages 26+ years at baseline to < 65 years in year 2 from the longitudinal files of the Medical Expenditure Panel Survey (2013–2015). ΔFB is the absolute change in use (marginal mean for count outcomes and percent for binary outcomes) for uninsured foreign-born respondents at baseline who became insured in year 2 for a specific health service due to gaining insurance. ΔUSB is the absolute change in use (marginal mean for count outcomes and percent for binary outcomes) for uninsured US-born respondents at baseline who became insured in year 2 for a specific health service due to gaining insurance. ΔUSB−ΔFB is the difference in absolute change (as defined above) in use (marginal mean for count outcomes and percent for binary outcomes) from the baseline year to year 2 for a specific health service due to gaining insurance between US-born and foreign-born adults. Adjusted models control for age, sex, race/ethnicity, education, and time-varying measures of poverty status, employment, and self-reported general and mental health. The values of the estimated absolute change for each service are included in the bar. Upper 95% confidence interval values are represented by the lines attached to each bar
As with step 2 above, we also examined whether the estimated differences varied over panels by refitting all GEE models detailed above to include an additional interaction with the panel indicator. Doing so allowed us to test whether the cohorts of newly insured individuals in the baseline and second year following implementation differed in their healthcare use patterns and whether those differences varied by nativity status. Panel-specific estimates of marginal probabilities are plotted in SF5, and DDD estimates and their associated F tests and p values are provided in ST9.
Finally, to examine whether and to what extent gaining insurance coverage affected disparities in use of health services between the FB and USB, we tested differences in rates and means of health services use, derived from the GEE models, among FB individuals that gained insurance relative to USB individuals that were continuously insured. These estimated ANOVA-style contrasts, their p values, and 95% confidence intervals are presented in Table 2. To provide context for interpreting the increase in health services use among those who gained insurance, we plotted the baseline and year 2 rates of use for the continuously insured, where no change in use would be expected (SF6).
Results
Estimates of insurance changes over time (SF1) indicated that rates of continuous un-insurance did not differ in the 2 panels preceding the ACA and declined significantly afterwards. Additionally, the probability for being continuously insured, a lagging indicator, did not differ in the first 3 panels but became significantly so in the panel following implementation (2014/2015). These results hold for both USB and FB groups and provide support that observed changes are systemic rather than reflective of secular data trends.
Descriptive statistics at the baseline years for the overall sample and by nativity status are reported in Table 1. Immigrants were less likely to be non-Hispanic White or non-Hispanic Black or to reside in the Midwest, and more often had less than a high school education and a household income below 200% of the poverty level. Immigrants were slightly less likely to report very good or excellent general health, but slightly more likely to report very good or excellent mental health. There were no differences in the distribution of gender, age, or employment between immigrants and those born in the USA. Largely similar characteristics were observed in both panels (ST1).
Insurance Coverage
Between 2013 and 2015, 6.3% and 4.4% of FB and USB participants, respectively, gained insurance. Between 2013 and 2014, 5.7% of adults, ages 26–64, gained health insurance, and immigrants were more likely to gain coverage relative to those born in the USA (6.9–5.5%, the weighted equivalent of 2.1 and 6.9 million adults, respectively). Rates of insurance gains decreased slightly between 2014 and 2015 to 5.7% and 3.4% (the weighted equivalent of 1.8 and 4.2 million adults) among the FB and USB, respectively. Despite these gains, immigrants were much more likely to remain continuously uninsured, relative to the USB, with rates of continuous un-insurance among the FB decreasing from 25.2% (vs. 9% for USB) in 2013/2014 to 20.8% (vs. 6.4% for USB) in 2014/2015. Within subgroups of the immigrant and USB populations, we found substantial variations both in the percentage who gained coverage and those who remained uninsured (Fig. 1; also, ST2 for detailed numbers). Immigrants with household incomes just above the poverty level (i.e., low income or 125 ≤ 200% FPL) and immigrants with poor physical health were most likely to gain coverage, whereas among USB adults, those in households with incomes less than 125% of poverty were most likely to gain coverage. A plurality of immigrants from Hispanic backgrounds (37%), immigrants with less than a high school education (42%), and immigrants with household incomes less than 125% of poverty (46.4% of poor and 42.4% of near poor) were continuously uninsured over the 2013–2015 period. Rates of insurance gains slowed down consistently for all considered FB and USB subgroups between 2014 and 2015 relative to the first year of implementation (2013 to 2014; SF2 and ST3).
Multinomial logit models (ST3) for insurance status over 2 years indicated that nativity differences in the likelihood of being continuously uninsured (Δ = − 15.3%; 95% CI = (− 18.1; − 12.5)) were attenuated but remained statistically significant after controlling for demographic, socioeconomic, and health indicators (Δ = − 6.3%; 95% CI = (− 8.4; − 4.3)) (Fig. 2; ST4 and ST5). Nativity differences in insurance gains (Δ = − 1.9%; 95% CI = (− 2.9; − 0.9)) were explained by controlling for race/ethnicity (p = 0.112). Additional controls for socioeconomic factors, physical and mental health status, and individual preferences for medical care and risk-taking (in sensitivity analyses) did not substantively change differences in insurance gains by nativity status. DDD models (ST6) and difference tests indicated that similar patterns were evident in both panels (ST7; SF3 and SF4).
Health Services Use
Estimates of use of health services among participants before and after gaining insurance are presented in Fig. 3. After gaining insurance 45.3% (95% CI = 38.3.4; 52.2) and 50.1% (95% CI = 44.4; 55.8) of FB and USB adults, respectively, reported at least one routine care visit. Moreover, FB (95% CI = 1.5; 2.6) and USB (95% CI = 1.7; 2.4) adults, respectively, had an average of 2 office-based (outpatient) physician visits, and 5.8 (95% CI = 3.9; 7.7) and 9 (95% CI = 7.4; 10.6) prescription medications filled or refilled. Finally, 12.6% (95% CI = 8.9; 16.2) and 16.2% (95% CI = 12.4; 20.0) of FB and USB adults had an ED visit, and 6.1% (95% CI = 3.3; 8.8) and 7% (95% CI = 6.8; 9.4) had an inpatient hospital stay. These patterns remained consistent and robust to controlling for the time-invariant and time-varying model covariates (Fig. 3).
Our DD results point to a clear and substantial increase in use of services particularly for measures associated with the standard clinical care model. Estimates and tests of absolute change in health services use are provided in Fig. 4 (also detailed in ST8). Among immigrants and USB adults, the absolute change in the probability of scheduling at least one appointment for routine care following gaining insurance was ΔFB = 15.7% (p < 0.001) and ΔUSB = 11.7% (p < 0.001), respectively, after adjusting for differences in population characteristics. The difference in group differences (ΔFB−ΔUSB = 4.0%; p = 0.3964) was not statistically distinguishable from zero suggesting equivalent rates of change in this service for both groups.
The annual number of office-based physician visits also increased. It rose by 1.3 (p < 0.001) and 0.6 (p < 0.001) visits, respectively, among immigrants and USB adults, and the difference between the groups was significant (ΔFB−ΔUSB = 0.7; p = 0.035). The annual number of filled medication prescriptions also rose by 2.5 (p < 0.001) and 1.6 (p < 0.001), respectively, among FB and USB adults. The difference in the increase between the groups was not statistically significant (p = 0.3813).
FB but not USB adults who gained health insurance also increased their ED use. Among the FB, the probability of any ED use during the year close to doubled, increasing by 4.8% (p = 0.0145) in absolute terms, reaching the same levels reported among the USB whose rates pre and post insurance gains remained unchanged. The probability of having an inpatient hospital discharge during the year also increased substantially among both FB and USB adults, by 3.6% (p = 0.017) and 3% (p = 0.016), respectively. The difference in the probability of inpatient hospitalization did not differ significantly between the two groups (p value = 0.7695). The estimates of absolute change were statistically equivalent in both panels when tested separately. These results are detailed in ST9 and plotted in SF5.
Finally, the contrasts between the estimated health services use levels among the FB gaining insurance and the levels of use among the referent continuously insured USB group are presented in Table 2. These results indicated that gaining insurance was sufficient to eliminate differences in health services use for all considered outcomes. All differences were statistically indistinguishable from zero, and consistently so in both crude and covariates adjusted models.
Discussion
Three major findings emerge from our analysis. First, between 2013 and 2015, the ACA increased the prevalence of health insurance among US adults 26–64 years old. Larger gains in coverage occurred among immigrants than among USB adults, but substantial variations in gains occurred within these groups. Second, despite the gains for immigrants, as a group, they remained nearly 3 times as likely as USB adults to be chronically uninsured. Among immigrants, 1 out of every 4 lacked health insurance for all of 2013 and 2014, compared with less than 1 in 10 among USB adults. These rates continued to decline in 2014/2015 where one of every five immigrants lacked health insurance compared with slightly more than 1 in 20 USB adults. As such, major disparities in health insurance access by nativity status remained. Third, the gains in health insurance that occurred over this period translated into important changes in healthcare consumption and eliminated disparities in use among those gaining insurance irrespective of nativity. Among immigrants, the percentage who scheduled at least one appointment for routine care rose by 16%, the annual number of physician visits increased by 1.3 visits, the annual number of medication prescriptions filled rose by about 2.5 prescriptions, the percentage of immigrants making an ED visit during the year rose by close to 5%, and the percentage having a hospital stay rose by 3.6%.
These findings underscore the importance of health insurance for the use of healthcare, particularly among under-covered immigrant populations. Middle-aged immigrants, who might be particularly vulnerable to lack of access to care, were most likely to benefit from insurance gains. However, our results underscore the persistence of coverage disparities based on one’s nativity status, even after implementation of the ACA where a quarter of the population remained uninsured.
Our findings on how the ACA affected immigrants echo available evidence on how the 2006 Massachusetts health reforms (MHRs) affected Hispanics and the poor in that state. Maxwell and colleagues found that MHRs led to significant increases in insurance coverage and in “having a personal provider” among Hispanics. [26] Their insurance coverage rose 11% post-MHRs, and having a personal provider rose 15.2%, compared with 4.8% and 1.8%, respectively, among non-Hispanic Whites. Yet, despite these gains, 21% of Hispanics remained uninsured post-MHR, compared with about 4% of non-Hispanic Whites. Likewise, Tinsley and colleagues analyzed data for the Boston area and found that despite the MHR explicitly targeting the working poor, it has not reduced disparities in insurance between the poor and non-poor, which has important implications for the ACA. [27] A few researchers have examined why so many immigrants in Massachusetts still lack health insurance post–MHR. Joseph and colleagues found that even in Boston’s permissive regulatory environment, immigrants’ worries about anti-immigrant sentiments, documentation status, and fear of deportation remain major impediments to obtaining coverage. [28] Language and cultural barriers also contribute to lack of coverage and reduced access to care. [26] Immigrants have concerns about paying premiums and affording care, as well as obtaining insurance information in their primary language. [29] Many of these barriers to coverage and healthcare require direct policy interventions, over and above what the ACA offers, in order to reduce disparities.
We found that extending coverage was especially linked to better use of efficient resources in line with the primary preventive care model. [30, 31] Individuals gaining insurance had substantial increase in routine care, office-based physician care, and increase in subscription medications filled. These findings echo work on the effects of extending insurance coverage from the Oregon Medicaid experiment, [32] Massachusetts healthcare reform, [33, 34] and early evidence from the ACA Medicaid expansion. [1, 20, 35] The absolute effect of access on use of these services was largely similar among the foreign and US born after controlling for differences in population characteristics. However, the relative increase among the FB, given their much lower baseline, was larger, suggesting that if sustained and expanded, these increases have the potential to effectively reduce existing disparities between the two groups. In Oregon’s Medicaid experiment, those that gained and maintained coverage had increased their utilization of health center services to rates similar to those who were continuously insured. [36] While no work has looked at the effects of reform among immigrants, our findings are concordant with work that examined other vulnerable populations targeted by reform, including the poor and near poor, minorities, the near-elderly, and women. [37,38,39,40]
Insurance gains were also associated with higher use of ED services among the FB and higher hospital discharges among both USB and FB participants that gained insurance. The lack of change in use of ED services as a result of gaining health insurance among the USB is likely due to higher awareness of legal mandates for ED visits to provide services for individual seeking care irrespective of their insurance status. This is less likely to be the case for the FB, which provides an explanation for the increase in the level of use among FB respondents. Importantly, the level of use after gaining insurance among the FB increased to a level that matched those reported among those born in the USA. Available evidence on the effects of coverage gains on ED use and hospitalizations are somewhat mixed, and largely non-existent for immigrants. While some have reported that the MHR has led to efficiencies in health services use as a result of reductions in ED visits and hospital inpatient stays, [41] mostly attributed to reduction in non-urgent visits, [42] several other studies have found that ED use increased among people who gained insurance, as did hospital admissions. [43,44,45] Research on ED use suggest that use patterns reflect issues other than need alone and are influenced by closeness to point of access, time allocation issues, and health literacy with regard to treatment options and symptom recognition. We found that both the absolute and relative rates of change resulting from insurance access were similar among US and FB adults. The use of ED and hospitalizations is not always intrinsically inefficient and future research should focus on quantifying the effects of insurance gains on relative spending on services as well as overall gains in the long-term health, costs, and quality of life.
Our findings have important policy implications. We provided evidence that the ACA mandates have improved access to insurance in the US population overall, and among immigrants in particular. If this expansion is long-lasting and undisrupted by counteractive judicial, legislative, or executive actions, reductions in healthcare access disparities can yield important improvements in realized access to healthcare and health outcomes among immigrants. Reducing disparities could lead to vital population health corrections in the USA. However, several fundamental issues remain. First, the political uncertainty and precariousness of the policy environment around the ACA can lead to stagnation and even losses in attained gains. These losses are likely to affect the most vulnerable and at-risk subpopulations and as such could reverse any attained reductions in disparities regarding health outcomes. Second, our results point to an increase in realized access to healthcare secondary to insurance gains. However, access to care, as shown by decades of research on underserved populations, does not equate to health improvement or reduction in health disparities. Complimentary policies and programs to diminish the under-insurance or high-sharing cost plans, enhance care quality, increase health literacy, improve system-patient and provider-patient communication, and ensure care continuity, among many others, are needed to sustain this realized access. Finally, our results most critically indicate that a major proportion of US immigrants, and to a lesser extent US-born groups, remain uninsured. These groups are most vulnerable to health shocks and adverse health risks. Unless these groups are covered, the US society and the public health system will continue to run the risk of having a resident health underclass. This has grave implications for health equity.
Several limitations deserve attention. First, MEPS does not gather information on immigrants’ documentation status, so we were unable to isolate the ACA’s effects on undocumented immigrants and other non-citizens who legally reside in the USA. Second, we were unable to distinguish between urgent and non-urgent ED use and preventable and non-preventable hospital stays. Third, we were also unable to control for the effects of other factors known to influence willingness to obtain insurance or seek healthcare services, e.g., an individual’s perceptions about and trust in providers. [46, 47] Although, we controlled for a set of proxy indicators that measure participant’s perception of usefulness and worth of health insurance and propensity for risk taking. Fourth, we are unable to attribute with certainty that the gains in insurance are completely due to the ACA. In our models, however, we controlled for time-varying socioeconomic, employment, and health indicators, which are probable confounders for obtaining insurance and the results we obtained were largely unchanged through these adjustments. Fifth, we did not adjust for a comorbidity index (e.g., Charlson). However, our models adjusted for self-reported physical and mental health status, which are good proxies for assessment of health needs across groups. Future studies with more granular medical condition data should more precisely account for differences in health risk profiles between US- and foreign-born groups and adjust for underlying differences in comorbid conditions. Sixth, as with any household survey, many data elements in MEPS are self-reported, which could be subject to recall as well as other biases. However, studies done to validate self-reports have shown overall validity. [48,49,50] Finally, the timeline and data used in this work might have been too constrained to detect all the changes introduced by the ACA insurance mandates. The ACA was passed in 2010, with phased changes occurring over time, but the major mandates going into effect in 2014. As such, the 2013/2014 panel might have underreported health insurance coverage. Future work should consider a longer observation period to validate our findings and assess the longer term, and longer lasting, changes derived from the ACA.
Conclusion
Our analysis of MEPS data covering 2013 to 2015 reveals that health insurance coverage among adult immigrants increased following the ACA, and that immigrant gains were larger than those among USB adults. However, a much higher percentage of immigrants remained uninsured in both 2014 and 2015. Both immigrants and the USB increased their use of healthcare following the ACA, including their use of routine care, office-based doctor visits, prescription medications, and inpatient hospitalizations. Although major disparities in health insurance coverage persisted into 2015, if coverage continues to expand among immigrants, then disparities in health services use between immigrants and USB adults will likely continue to diminish.
References
French MT, Homer J, Gumus G, Hickling L. Key provisions of the Patient Protection and Affordable Care Act (ACA): a systematic review and presentation of early research findings. Health Serv Res. 2016;51(5):1735–71.
Warner DC. Access to health services for immigrants in the USA: from the Great Society to the 2010 Health Reform Act and after. Ethn Racial Stud. 2012;35(1):40–55.
Sommers BD, Parmet WE. Health care for immigrants-implications of Obama’s executive action. N Engl J Med. 2015;372(13):1187–9.
Zuckerman S, Waidmann TA, Lawton E. Undocumented immigrants, left out of health reform, likely to continue to grow as share of the uninsured. Health Aff. 2011;30(10):1997–2004.
Colby LS, Ortman MJ. Projections of the size and composition of the US population: 2014 to 2060, Current Population Reports, P25–1143, U.S. Census Bureau, Washington, DC, 2014.: U.S. Census Bureau; 2015.
Carrasquillo O, Carrasquillo AI, Shea S. Health insurance coverage of immigrants living in the United States: differences by citizenship status and country of origin. Am J Public Health. 2000;90(6):917–23.
Derose KP, Escarce JJ, Lurie N. Immigrants and health care: sources of vulnerability. Health Aff. 2007;26(5):1258–68.
Derose KP, Bahney BW, Lurie N, Escarce JJ. Review: immigrants and health care access, quality, and cost. Med Care Res Rev. 2009;66(4):355–408.
Tarraf W, Miranda PY, González HM. Medical expenditures among immigrant and nonimmigrant groups in the United States: findings from the Medical Expenditures Panel Survey (2000–2008). Med Care. 2012;50(3):233–42.
Parmet WE. Holes in the safety net-legal immigrants’ access to health insurance. N Engl J Med. 2013;369(7):596–8.
Ye J, Mack D, Fry-Johnson Y, Parker K. Health care access and utilization among US-born and foreign-born Asian Americans. J Immigr Minor Health. 2012;14(5):731–7.
Goldman DP, Smith JP, Sood N. Immigrants and the cost of medical care. Health Aff. 2006;25(6):1700–11.
Tarraf W, Vega W, González HM. Emergency department services use among immigrant and non-immigrant groups in the United States. J Immigr Minor Health. 2013:1–12.
Tarraf W, Jensen GA, González HM. Impact of Medicare age eligibility on health spending among US and foreign-born adults. Health Serv Res. 2016;51(3):846–71.
Xu KT, Borders TF. Does being an immigrant make a difference in seeking physician services? J Health Care Poor Underserved. 2008;19(2):380–90.
Lebrun LA, Shi L. Nativity status and access to care in Canada and the U.S.: factoring in the roles of race/ethnicity and socioeconomic status. J Health Care Poor Underserved. 2011;22(3):1075–100.
Lebrun LA, Dubay LC. Access to primary and preventive care among foreign-born adults in Canada and the United States. Health Serv Res. 2010;45(6p1):1693–719.
Chua K-P, Sommers BD. Changes in health and medical spending among young adults under health reform. Jama. 2014;311(23):2437–9.
Antwi YA, Moriya AS, Simon K, Sommers BD. Changes in emergency department use among young adults after the Patient Protection and Affordable Care Act’s dependent coverage provision. Ann Emerg Med. 2015;65(6):664–72. e2.
Sommers BD. Why health insurance matters-and why research evidence should too. Acad Med. 2017;92:1228–30.
Sommers BD, Blendon RJ, Orav EJ, Epstein AM. Changes in utilization and health among low-income adults after Medicaid expansion or expanded private insurance. JAMA Intern Med. 2016;176(10):1501–9.
Sommers BD, Maylone B, Nguyen KH, Blendon RJ, Epstein AM. The impact of state policies on ACA applications and enrollment among low-income adults in Arkansas, Kentucky, And Texas. Health Affairs. 2015;34(6):1010–8.
Sommers BD, Maylone B, Blendon RJ, Orav EJ, Epstein AM. Three-year impacts of the affordable care act: improved medical care and health among low-income adults. Health Aff. 2017;36(6):1119–28.
Hardin JW, Hilbe JW. Generalized linear models and extensions: Stata Press books; 2012.
Fitzmaurice GM, Laird NM, Ware JH. Applied longitudinal analysis: Wiley; 2012.
Maxwell J, Cortes DE, Schneider KL, Graves A, Rosman B. Massachusetts’ health care reform increased access to care for Hispanics, but disparities remain. Health Aff (Millwood). 2011;30(8):1451–60.
Tinsley LJ, Hall SA, McKinlay JB. Has Massachusetts health care reform worked for the working poor? Results from an analysis of opportunity. Ann Epidemiol. 2014;24(4):312–8.
Benitez JA, Adams EK, Seiber EE. Did health care reform help Kentucky address disparities in coverage and access to care among the poor? Health Serv Res. 2017.
Kang YJ, McCormick D, Zallman L. Affordability of and access to information about health insurance among immigrant and non-immigrant residents after Massachusetts health reform. J Immigr Minor Health. 2017;19(4):929–38.
Davis K, Abrams M, Stremikis K. How the Affordable Care Act will strengthen the nation’s primary care foundation. J Gen Intern Med. 2011;26(10):1201–3.
Fiscella K. Health care reform and equity: promise, pitfalls, and prescriptions. Ann Fam Med. 2011;9(1):78–84.
Gold R, Bailey SR, O’Malley JP, Hoopes MJ, Cowburn S, Marino M, et al. Estimating demand for care after a Medicaid expansion: lessons from Oregon. J Ambul Care Manage. 2014;37(4):282–92.
Ku L, Jones E, Shin P, Byrne FR, Long SK. Safety-net providers after health care reform: lessons from Massachusetts. Arch Intern Med. 2011;171(15):1379–84.
Okoro CA, Dhingra SS, Coates RJ, Zack M, Simoes EJ. Effects of Massachusetts health reform on the use of clinical preventive services. J Gen Intern Med. 2014;29(9):1287–95.
Mulcahy AW, Eibner C, Finegold K. Gaining coverage through Medicaid or private insurance increased prescription use and lowered out-of-pocket spending. Health Aff (Millwood). 2016;35(9):1725–33.
Hatch B, Bailey SR, Cowburn S, Marino M, Angier H, Devoe JE. Community health center utilization following the 2008 Medicaid expansion in Oregon: implications for the Affordable Care Act. Am J Public Health. 2016;106(4):645–50.
Okoro CA, Zhao G, Fox JB, Eke PI, Greenlund KJ, Town M. Surveillance for health care access and health services use, adults aged 18–64 years-Behavioral Risk Factor Surveillance System, United States, 2014. MMWR Surveill Summ. 2017;66(7):1–42.
Martinez ME, Ward BW. Health care access and utilization among adults aged 18–64, by poverty level: United States, 2013-2015. NCHS Data Brief. 2016(262):1–8.
Courtemanche CJ, Zapata D. Does universal coverage improve health? The Massachusetts experience. J Policy Anal Manage. 2014;33(1):36–69.
Simon K, Soni A, Cawley J. The impact of health insurance on preventive care and health behaviors: evidence from the first two years of the ACA Medicaid expansions. J Policy Anal Manage. 2017;36(2):390–417.
Long SK, Stockley K, Dahlen H. Massachusetts health reforms: uninsurance remains low, self-reported health status improves as state prepares to tackle costs. Health Aff (Millwood). 2012;31(2):444–51.
Miller S. The effect of insurance on emergency room visits: an analysis of the 2006 Massachusetts health reform. J Public Econ. 2012;96(11–12):893–908.
Lee J, Ding R, Zeger SL, McDermott A, Habteh-Yimer G, Chin M, et al. Impact of subsidized health insurance coverage on emergency department utilization by low-income adults in Massachusetts. Med Care. 2015;53(1):38–44.
Niedzwiecki MJ. Does health insurance coverage encourage more efficient use of medical care? Evidence from the Massachusetts health reform. 2014.
Lasser KE, Hanchate AD, McCormick D, Manze MG, Chu C, Kressin NR. The effect of Massachusetts health reform on 30 day hospital readmissions: retrospective analysis of hospital episode statistics. BMJ. 2014;348:g2329.
Afilalo J, Marinovich A, Afilalo M, Colacone A, Léger R, Unger B, et al. Nonurgent emergency department patient characteristics and barriers to primary care. Acad Emerg Med. 2004;11(12):1302–10.
Newton MF, Keirns CC, Cunningham R, Hayward RA, Stanley R. Uninsured adults presenting to US emergency departments. JAMA. 2008;300(16):1914–24.
Zuvekas SH, Olin GL. Validating household reports of health care use in the medical expenditure panel survey. Health Serv Res. 2009;44(5p1):1679–700.
Zuvekas SH. The effects of recall length and reporting aids on household reporting of health care events in the medical expenditure panel survey. J Econ Soc Meas. 2011;36(4):321–43.
Zuvekas SH. Accuracy of Medicare expenditures in the medical expenditure panel survey. Inquiry (Chicago). 2009;46(1):92–108.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Tarraf, W., Jensen, G.A., Li, Y. et al. Changes in Insurance Coverage and Healthcare Use Among Immigrants and US-Born Adults Following the Affordable Care Act. J. Racial and Ethnic Health Disparities 8, 363–374 (2021). https://doi.org/10.1007/s40615-020-00790-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40615-020-00790-y