
Abstract
Background
Total hip replacements (THRs) are the sixth most common surgical procedure performed in the USA. Readmission rates are estimated at between 4.0 and 10.9%, and mean costs are between $10,000 and $19,000. Readmissions are influenced by the quality of care received. We sought to examine differences in readmissions by insurance payer, race and ethnicity, and income status.
Methods
We analyzed all THRs from 2007 to 2011 in California, Florida, and New York from the State Inpatient Databases, Healthcare Cost and Utilization Project, Agency for Healthcare Research and Quality. Primary outcomes were readmission at 30 and 90 days after THR. Descriptive statistics were calculated, and multivariate logistic regression analysis was used to estimate adjusted odds ratio (OR) for readmissions. Statistical significance was evaluated at the < 0.05 alpha level.
Results
A total of 274,851 patients were included in the analyses. At 30 days (90 days), 5.6% (10.2%) patients had been readmitted. Multivariate logistic regression analysis showed that patients insured by Medicaid (OR 1.23, 95%CI 1.17–1.29) and Medicare (OR 1.58, 95%CI 1.44–1.73) had increased odds of 30-day readmission, as did patients living in areas with lower incomes, Black patients, and patients treated at lower volume hospitals. Ninety-day readmissions showed similar significant results.
Conclusions
The present study has shown that patients on public insurance, Black patients, and patients who live in areas with lower median incomes have higher odds of readmission. Future research should focus on further identifying racial and socioeconomic disparities in readmission after THR with an eye towards implementing strategies to ameliorate these differences.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Total hip replacements (THRs) are the sixth most common surgical procedure performed in the USA, with annual national spending exceeding $17 billion [1]. In 2011 alone, more than 305,000 THR surgeries were performed. While THR is a routine procedure that provides a marked improvement in the quality of life and return to function for patients [2], it is not without risk [3]. Effective healthcare and resource utilization may help reduce the risk of morbidity and mortality associated with the procedure, including reducing hospital readmissions [4]. Hospital readmission rates for THR are estimated at 4.0 to 10.9% and mean readmission costs vary between $10,000 and $19,000 [4,5,6,7,8,9,10].
Readmission rates are influenced by the quality of inpatient and outpatient care; differences in readmission rates suggest differences in quality and transition of care [11]. Under the Hospital Readmission Reduction Program (HRRP), a provision of the Affordable Care Act (ACA) enacted in Fiscal Year 2015, Medicare initiated the implementation of incentives to reduce 30-day hospital readmissions for elective THR through the use of penalties for hospitals with readmission rates that exceed a risk-adjusted calculated national average [12,13,14,15,16,17]. The focus on readmission rates extends to Medicare’s bundled payment system for orthopedic surgeries where participating hospitals are accountable for total episode payments (initial hospitalization and Medicare-covered services during 90 days following discharge). This serves to highlight the importance of hospitals identifying reasons for unplanned 30- and 90-day readmissions and finding modifiable risk factors [18,19,20].
Previous research has identified clinical and non-clinical risk factors associated with readmissions across various orthopedic surgeries. These include increased age, a larger number of patient comorbidities, longer postoperative length of stay, having the procedure performed at a hospital with a low surgical volume, and non-routine discharge status [5, 21,22,23,24,25,26,27,28,29]. Studies also show that not having private insurance and being non-White may increase the likelihood of readmission after orthopedic surgeries [5, 7]. However, these studies were limited to single institutions, limited geographic areas or single states, or to exclusively Medicare populations [7, 21]. Few studies have focused extensively on socioeconomic factors affecting the risk of readmission in THR, and even fewer have been dedicated to exploring readmission by insurance payer status in THR surgeries specifically [7, 30, 31]. Research to address disparities by these sociodemographic categories in THR readmissions is necessary because of its status as one of the most commonly performed procedures.
The present study used hospital discharge data from a multistate inpatient, all-payer database for California, Florida, and New York for the years 2007–2011. We examined differences in 30- and 90-day readmissions after THR by insurance payer, race and ethnicity, and quartile of median income. We hypothesized that patients’ socioeconomic characteristics, including being on Medicaid or uninsured, having lower median income, and being non-White, are all independently associated with increased hospital readmissions after THR.
Methods
Study Database and Population
We examined retrospective inpatient hospitalization and discharge records of adults aged 18 years or older using data from California, Florida, and New York from January 2007 to December 2011 from the State Inpatient Databases (SID), Healthcare Cost and Utilization Project (HCUP), Agency for Healthcare Research and Quality (AHRQ) [32]. The Weill Cornell Medicine Institutional Review Board approved all study activities; because the data used in this study was sufficiently de-identified before analysis, this project was deemed exempt from review by the IRB. The SID contains all inpatient records, regardless of primary payer, from non-federal, non-psychiatric hospitals, representing about 97% of all US community hospital discharges [32]. Data is coded so each inpatient hospital admission corresponds to one individual record. SID data uses a unique discharge identifier, VisitLink, to facilitate the linking of the initial inpatient admission to a subsequent readmission record and to provide information on the postdischarge timing of readmission. Readmissions are able to be identified if they occur in the same state in which the THR occurred, irrespective of the hospital to which the patient was readmitted. All HCUP data are subject to quality control procedures to assess the validity of values and their internal consistency [33].
Using International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) procedure codes, we retrospectively identified records for patients (aged ≥ 18 years) who underwent a THR (ICD-9-CM code 81.51). Patients were excluded if they were aged < 18 years, had missing data on gender, experienced inpatient mortality during the index hospital stay, had missing information on hospital length of stay (LOS) or days to readmission data, had insufficient follow-up time, or lacked primary insurance status information.
Variables and Endpoints
Variables abstracted for each admission include patient-, surgical-, and hospital-related factors. Patient-related factors include demographic characteristics, comorbidities as noted by ICD-9-CM present-on-admission (POA) indicators for each diagnosis, procedure codes, postoperative complications, residence in quartiles of median state household income, insurance status (or expected primary insurance payer), hospital length of stay (LOS), admission and discharge dates, and discharge disposition. POA indicators facilitate disentangling preexisting medical comorbidities from perioperative complications. POA comorbidities were selected from the Elixhauser comorbidity index [34]. Postoperative complications are defined as medical diagnoses coded for a patient at hospital discharge that occurred during their initial hospitalization for THR surgery. Patients were grouped by insurance type (expected payer): Medicare (includes both fee-for-service and managed care Medicare patients), Medicaid (includes both fee-for-service and managed care Medicaid patients), uninsured (includes no charge reported or self-pay status), other (includes Worker’s Compensation, CHAMPUS, CHAMPVA, Title V, and other government programs), or private insurance (includes Blue Cross/Blue Shield, commercial carriers, and private HMOs and PPOs). Surgical and hospital-related factors include year and state in which the surgery was performed, core based statistical area (CBSA) for the hospital, and surgical volume for THR at each hospital.
Outcomes
The primary outcomes of our study were unadjusted rates and adjusted odds of 30- and 90-day hospital readmissions. We were specifically concerned with these outcomes for patients as they varied across racial/ethnic and socioeconomic lines, as measured by insurance payer, race and ethnicity, and median income by geographic location. Secondary outcomes of our study included reasons for readmissions, cohorted by insurance type.
Statistical Analysis
Demographic characteristics and POA comorbidities were compared for all patients who underwent THR by readmission status for 30 and 90 days, respectively. Counts of patients readmitted up to 90 days also included those who were admitted up to 30 days postoperatively. Categorical variables were compared using Pearson’s χ2 tests or Fisher’s exact tests; continuous variables were compared using analysis of variance (ANOVA) or Kruskal-Wallis tests, for non-normally distributed variables, as appropriate.
To examine the effect of markers of racial and socioeconomic disparities on readmissions, we conducted separate multivariate logistic regression analyses for 30- and 90-day readmissions, controlling for other demographic variables, comorbidities, postoperative complications, hospital LOS, discharge disposition status, and other potential confounders. Adjusted odds ratios (ORs) with robust 95% confidence intervals were calculated. Models included variables with differences at an alpha level of 0.25 or below in bivariate analyses, or variables selected a priori as potential confounders (age, gender, race, median income, expected insurance payer, state of surgery, year of surgery). Our multivariate regression models were also rerun in a series of models with outcomes of interest (30-, 90-day readmission) stratified by insurance type, race/ethnicity, and median income, separately, to examine the independent associations of these social determinants of health on outcomes when variables of interest are homogeneous among patients. Models were additionally stratified by individual state (California, Florida, and New York) to account for the differences in access to and provisions of Medicaid among individual states.
Additionally, we conducted multivariate logistic regression models to restrict our analysis to only elective THR to account for the newly instituted provision of the Affordable Care Act (ACA), the Readmissions Reduction Program (HRRP), which applies to elective procedures only [12,13,14,15,16,17]. Though our data does not temporally coincide with the introduction of the HRRP, the restricted analyses were used to identify risk factors specific to elective procedures [12]. California state data did not indicate elective surgery and therefore analysis was performed only for the states of Florida and New York.
We performed sensitivity analyses to account for any potential unmeasured confounders that could cause specious findings. Our models for 30- and 90-day readmissions were separately re-estimated after removing the most statistically significant covariate as measured by the Wald statistic (found to be age in years for both models); as long as the originally observed effect was not substantially attenuated (which would be indicated by the estimated odds of each outcome being reduced by less than 10%) and remained statistically significant after re-estimation, the potential for specious results is reduced, thus validating the findings of the original model [3, 35].
Model assumptions of normality and linearity were assessed graphically and statistically; goodness-of-fit testing was performed. Model discrimination was evaluated using the area under the receiver operating characteristics curve (AUC), where AUC values of 0.5 indicate results equal to chance and values of 1.0 indicate perfect discrimination between outcome groups as measured with the C-statistic. All P values are two-sided with statistical significance evaluated a priori at < 0.05 alpha level. Statistical tests and analyses were performed using SAS version 9.3 (SAS Institute, Cary, NC).
Results
Patient and Hospital Characteristics
Patients Admitted up to 30 Days Postoperatively
During the 5-year study period from 2007 to 2011, a total of 297,103 patients underwent a THR in California, Florida, and New York, with 295,579 patients being ages ≥ 18 years old. A total of 274,851 patients had non-missing primary insurance payer and data on readmission status allowing for inclusion in the analysis. Within 30 days, 15,273 (5.6%) patients were readmitted, including 7.7% of Medicaid patients, 6.8% of Medicare patients, and 3.5% of patients with private insurance. After 30-day readmission, 271 patients (1.8%) died inhospital. Table 1 shows results of the bivariate analysis for patient demographic characteristics and POA comorbidities, surgical- and hospital-related characteristics, and initial hospital stay characteristics compared by 30-day readmission status.
Patients readmitted within 30 days were more likely to be older, be Black or Hispanic, live in the poorest quartile of median household income in their respective ZIP code, have Medicare and Medicaid as insurance providers, and have greater numbers of comorbidities as defined by the Elixhauser index [34] than those not readmitted within 30 days. Their surgery was more likely to be emergent and performed in hospitals with a low volume of annual THR surgeries. Their initial hospital course was more likely to have a longer length of stay and have greater total hospital charges than those not readmitted up to 30 days postoperatively. Additionally, readmitted patients were more likely to have suffered cardiovascular, pulmonary, infectious, and intraoperative complications during their initial postoperative hospitalization.
The incidence of 30-day readmission was lowest in the privately insured group, and as such, we compared the incidence of specific POA reasons for readmission in other insurance categories to private insurance. The most common reasons for 30-day readmissions were wound infection (15.7% Private insurance; 19.3% Uninsured), atrial fibrillation (5.9% Private insurance; 18.4% Medicare), urinary tract infection (6.3% Private insurance; 13.3% Medicare), and pneumonia (3.4% Private insurance; 6.9% Medicare) (Table 2).
Patients Admitted up to 90 Days Postoperatively
Of the 274,851 patients aged ≥ 18 with non-missing insurance payer and readmission variables who underwent surgery for THR, 28,075 (10.2%) were readmitted within 90 days postoperatively, including 14.5% of Medicaid patients, 11.9% of Medicare patients, and 7.3% patients with private insurance. After 90-day readmission, 432 (1.5%) died inhospital. Patient demographics for those readmitted up to 90 days postoperatively were more likely to be on public insurance (Medicare/Medicaid), older, live in geographic areas with poorer median household incomes, be Black or Hispanic, have longer hospital lengths of stay, higher hospital charges, and be treated in hospitals performing fewer THRs (Table 1).
The most common reasons for 90-day readmission compared to private insurance were atrial fibrillation (5.5% Private insurance; 16.9% Medicare), urinary tract infection (4.5% Private insurance; 12.0% Medicare), wound infection (9.3% Private insurance; 10.7% Other Insurance), and pneumonia (2.7% Private insurance; 6.2% Medicare) (Table 2).
Multivariate Results
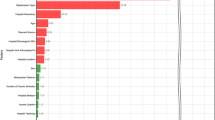
In multivariate logistic regression models (Table 3), patients insured by Medicare (OR 1.23, 95% CI 1.17–1.29) and Medicaid (OR 1.58, 95% CI 1.44–1.73) had higher likelihoods of being readmitted up to 30 days postoperatively than patients with private insurance. Similarly, patients insured by Medicare (OR 1.20, 95% CI 1.16–1.25) and Medicaid (OR 1.52, 95% CI 1.42–1.62) also had higher likelihoods of being readmitted up to 90 days postoperatively than patients with private insurance.
Patients living in geographic areas with the highest median household income values of their state were less likely to be readmitted 30 and 90 days postoperatively than those living in the poorest income quartiles of their state (30-day OR 0.89, 95% CI 0.85–0.94; 90-day OR 0.91, 95% CI 0.87–0.94, Table 3). Blacks were more likely than Whites to be admitted up to 30 and 90 days postoperatively (30-day OR 1.20, 95% CI 1.11–1.29; 90-day OR 1.08, 95% CI 1.02–1.14). Patients treated at hospitals in the highest quartile of THR surgery volume in their state were also less likely to be readmitted up to 30 days postoperatively (OR 0.76, 95% CI 0.72–0.80). In addition, a larger number of POA comorbidities, longer postoperative length of stay, and occurrence of cardiovascular, pulmonary, intraoperative, and infectious complications postoperatively were associated with increased odds of 30- and/or 90-day readmissions (Table 3).
Results from the series of exploratory stratified models (stratified by insurance payer, race and ethnicity, and median income) largely supported our initial findings; however, some models were likely statistically underpowered due to small subpopulation numbers.
Primary Insurance Payer Effects on Readmissions
Medicare and Medicaid insurance continued to be a predictor of 30-day readmissions among Black and Hispanic populations, save for Hispanic Medicaid patients at 30 days; White Medicare and Medicaid patients also had higher odds of readmission (Supplementary Table 1). The two government insurers also predicted readmission by individual stratified quartile of median income, save for 30-day readmission in the highest income quartile (Supplementary Table 2).
Median Income Effect on Readmissions
Living in the highest versus lowest quartile of median income was significantly associated with a reduced rate of readmissions in patients with Medicare and other types of insurance; however, this finding was not observed in Medicaid patients living in the highest median income quartile, nor in patients with other insurance (90 days only) (Supplementary Table 3). Additionally, residing in the highest versus lowest income quartile continued to be a predictor for reduced risk of readmission for White and Black patient populations individually at 30 days, and in a White patient population at 90 days as well (Supplementary Table 1).
Race and Ethnicity Effects on Readmissions
Black patients continued to have increased odds of readmission compared to White patients among most insurance groups, except in the populations with private insurance or the uninsured (Supplementary Table 3). Hispanics were now found to have higher odds of 30-day readmission in the Medicare-only population (compared to Whites), yet those with other types of insurance had lower odds. The odds of readmission were found to be significantly increased for Black patients compared to White patients in the first quartile of median income and at 30 days for the third quartile of median income (Supplementary Table 2).
Our main results did not differ in separate multivariate sub-analyses by state, by elective procedures only, or within our sensitivity analysis omitting age (unpublished data).
Discussion
Using retrospective discharge data from the State Inpatient Databases (SID) of California, Florida, and New York for the years 2007–2011, we showed that markers of socioeconomic, racial, and ethnic disparities resulted in increased odds of 30- and 90-day hospital readmissions after THR. Specifically, Blacks (as compared to Whites), living in an area with a lower median income, and being on Medicaid (versus private insurance) were all independently associated with higher rates of readmission. This association remained significant after adjustment for patient demographic factors and medical history, postoperative complications, initial hospital length of stay, state, temporal, surgical, and hospital-related factors, when our analysis was performed by stratification by individual state and by a subgroup analysis of elective procedures only (to account for the 2015 HRRP provision), and when subjected to a sensitivity analysis to adjust for possible missing confounders (unpublished data). Additionally, our primary findings were compared to results from a series of stratification models by individual social determinants of health (insurance type, race/ethnicity, and median income level, separately) to help clarify independence, confounding, and interdependence between these variables of interest. Collectively, our results point to the robustness of our findings.
Our findings are consistent with previous literature that has identified race, ethnicity, and/or markers of socioeconomic inequality as risk factors for broader healthcare disparities and for hospital readmission after THR. As evidenced by our statistical multivariate and stratified analyses, these factors are all interconnected with confounding associations; this too is reflected in the reviewed literature. According to the United States Census Bureau, in 2015, insurance coverage among different racial and ethnic groups was as follows: Whites (93.3%), Blacks (88.9%), Asians (92.5%), and Hispanics (83.8%) [36]. At 51.6%, Hispanics were also found to have the lowest rate of private health insurance converge, compared to Blacks (55.9%), Whites (73.6%), and Asians (75.5%) [36]. In addition, there is a persistent and growing gap in income between racial groups, with the median income of Whites being disproportionately higher than that of Blacks or Hispanics [37].
Oronce et al. showed that Blacks and those with non-private insurance had a greater incidence of 30-day readmissions in California during the years 2009–2011 [7]. In a meta-analysis examining orthopedic surgeries, Bernatz et al. found that in over 75% of the studies analyzed, patients on Medicare or Medicaid (when compared to private insurance) were more likely to be admitted up to 30 days postoperatively after THR [5]. Girotti et al. found that Black patients were significantly more likely to be readmitted after THR than White patients [38]. Racial disparities have also been shown to exist within Medicare enrollees after general surgery. Using national Medicare data, Joynt et al. found that 30-day readmissions were more likely with Black patients than that with White patients and patients treated at hospitals primarily serving racial minorities after hospitalization for myocardial infarction, congestive heart failure, and pneumonia than with White patients and patients treated at primarily non-minority serving hospitals [30]. Tsai et al. found that among Medicare beneficiaries, Black patients and patients served at a minority-serving hospital had a greater rate of 30-day readmissions after six major surgeries including THR [39]. In light of these findings, government regulators must ensure that hospitals providing services to certain sociodemographic populations are not disproportionately penalized due to HRRP or Medicare bundled payment systems [7].
Though our primary results were not significant for increased readmissions for members of the Hispanic ethnicity, our stratified analysis by insurance type showed mixed results. Hispanic patients have been found to undergo many different surgical procedures at lower surgical volume hospitals compared to White patients, which would suggest poorer outcomes [40, 41]; however, Adelani et al. found no significant disparity in readmissions after hip arthroplasty when adjusting for hospital surgical volume, which corroborates our reported findings [42]. Our findings are also in line with previous orthopedic literature that has shown mixed results concerning disparities in outcome measures for Hispanic patients [42, 43].
To our knowledge, our study features the most currently available and up-to-date data on disparities in 30- and 90-day readmissions after THR. We included 274,851 patients from three states in our multivariate logistic regression models; the population of these states collectively represents 24.6% of the US population [44]. Prior research focused on healthcare disparities and readmissions after THR as a primary or well-defined outcome only included single institutions or hospital systems, single states, or only the Medicare patient population [7, 21]. In addition to our primary findings, we found that patient age, medical comorbidities, postoperative course (as measured by LOS and complications), and hospital procedure volume were found to be important predictors of hospital readmissions in our models. The most common reasons for hospital readmissions in our dataset population were infection (surgical site infection, pneumonia, UTI) and medical complications (atrial fibrillation and DVT). These findings replicate previous studies identifying risks, factors, and reasons for hospital readmission after THR [5, 45, 46].
Our results show that markers of racial, ethnic, and socioeconomic disparities were associated with an increase in both 30- and 90-day readmissions. The increased rates of readmissions for Blacks, patients living in poorer areas, and patients on Medicaid serve as markers of the continuing and persistent disparities in healthcare quality [3, 31, 47,48,49].
Previous research has identified preoperative, intraoperative, and postoperative examples of disparities in health status and care provided to minority and socioeconomically disadvantaged patients [3, 47,48,49]. Non-Whites have been shown to have more comorbidities [50], and those on Medicaid or not insured have difficulties accessing care, including undergoing surgery at low-quality and high-cost hospitals [51, 52]. Intraoperatively, Black patients and those insured with Medicaid are less likely to be treated with neuraxial anesthesia [53, 54], a clinical technique shown to result in improved postoperative outcomes [55,56,57,58]. Postoperatively, racial minorities have been shown to be undertreated for pain [59], have barriers to accessing pain management specialists [60], and receive less postacute rehabilitation care than Whites [61].
The analysis of sociodemographic disparities is an imperative in research, especially because many studies of orthopedic surgeries assessing predictors of patient-related outcomes often fail to even analyze race, ethnicity, or insurance payer status [62]. Programs to ameliorate healthcare disparities among racial, ethnic, and socioeconomic groups and thus optimizing the level of care provided should be implemented. Targeted initiatives to decrease global readmission rates for THR should be enacted, addressing modifiable risk factors and channeling patients to undergo surgery in high-volume surgical centers or Centers for Excellence. While some research has indicated that these readmission reduction initiatives may not be effective for patients after THR with an even less benefit for socioeconomically disadvantaged patients [63], more research needs to be performed to identify potential mechanisms for these discrepancies [64, 65].
There are important limitations to our study, which must be addressed to provide important context for the interpretation of our results [3]. One limitation of this study is the confounding nature between patient comorbidities (POA indicators) and postsurgical outcomes. Despite our best efforts to account for these differences through statistical adjustment, the confounding and mediating effect of a patient’s medical history cannot be understated. Research has shown that Medicaid beneficiaries are poorer, have poorer health profiles, and have greater risk factors, including THR preoperative risk factors, compared to the privately insured [51, 52, 66, 67].
Moreover, the accuracy of an administrative dataset is reliant upon complete and accurate clinical coding. The potential exists for coding errors, including miscoded and misclassified data. Variables lacking coding of relevant qualitative clinical data prevents grading of severity of comorbidities or adverse perioperative outcomes. Intraoperative data is not available in the HCUP dataset and therefore the choice of anesthetic cannot be elicited. There are no patient identifiers in the SID database. Follow-up postdischarge can only be performed for patients who are readmitted to the hospital within the same state of patient discharge; events occurring outside the hospital or in hospitals in other states cannot be followed or analyzed. As a result, longitudinal follow-up for non-admitted patients and patients admitted to out of state hospitals was not possible and we could not assess some postdischarge outcomes; such a methodology may underestimate the rate of adverse outcomes after THR.
A major strength of this study is its statistical power achieved through analysis of a large number of patient records. This allows for statistical means to control for a substantial range of potentially confounding patient and non-patient variables. The use of the HCUP administrative datasets provides data that is widely generalizable across hospitals and insurance payer types and the resultant findings are not restricted to specialized, experienced Centers of Excellence only (likewise as a limitation, findings from administrative database research may not be directly applicable to individual institutions or centers of care).
The present study has shown that patients with Medicaid insurance, Black patients, and patients living in geographic areas with household median incomes in the poorest quartile of the state have higher unadjusted and adjusted odds of 30- and 90-day readmissions. Caution must be used in interpreting our results because they show only associations; causality is not to be inferred. Future research should focus on further defining the problem of racial, ethnic, and socioeconomic disparities in readmissions after THR and helping to better identify and implement strategies to lessen their incidence.
References
HCUPnet. A tool for identifying, tracking, and analyzing national hospital statistics. Rockville, MD. 2013. https://hcupnet.ahrq.gov/#setup. Accessed 10 Sept 2013.
Ethgen O, Bruyere O, Richy F, Dardennes C, Reginster JY. Health-related quality of life in total hip and total knee arthroplasty. A qualitative and systematic review of the literature. J Bone Joint Surg Am. 2004;86-A(5):963–74.
Xu HF, White RS, Sastow DL, Andreae MH, Gaber-Baylis LK, Turnbull ZA. Medicaid insurance as primary payer predicts increased mortality after total hip replacement in the state inpatient databases of California, Florida and New York. J Clin Anesth. 2017;43:24–32. https://doi.org/10.1016/j.jclinane.2017.09.008.
Rosenthal JA, Lu X, Cram P. Availability of consumer prices from us hospitals for a common surgical procedure. JAMA Intern Med. 2013;173(6):427–32. https://doi.org/10.1001/jamainternmed.2013.460.
Bernatz JT, Tueting JL, Anderson PA. Thirty-day readmission rates in orthopedics: a systematic review and meta-analysis. PLoS One. 2015;10(4):e0123593. https://doi.org/10.1371/journal.pone.0123593.
Weiss A, Elixhauser A, Steiner C. Readmissions to US hospitals by procedure, 2010: statistical brief# 154. Rockville: Agency for Health Care Policy and Research (US); 2006.
Oronce CIA, Shao H, Shi L. Disparities in 30-day readmissions after total hip arthroplasty. Med Care. 2015;53(11):924–30. https://doi.org/10.1097/mlr.0000000000000421.
Kiridly DN, Karkenny AJ, Hutzler LH, Slover JD, Iorio R, Bosco JA 3rd. The effect of severity of disease on cost burden of 30-day readmissions following total joint arthroplasty (TJA). J Arthroplast. 2014;29(8):1545–7. https://doi.org/10.1016/j.arth.2014.03.035.
Bosco JA 3rd, Karkenny AJ, Hutzler LH, Slover JD, Iorio R. Cost burden of 30-day readmissions following Medicare total hip and knee arthroplasty. J Arthroplast. 2014;29(5):903–5. https://doi.org/10.1016/j.arth.2013.11.006.
Nichols CI, Vose JG. Clinical outcomes and costs within 90 days of primary or revision total joint arthroplasty. J Arthroplast. 2016;31(7):1400–6.e3. https://doi.org/10.1016/j.arth.2016.01.022.
Benbassat J, Taragin M. Hospital readmissions as a measure of quality of health care: advantages and limitations. Arch Intern Med. 2000;160(8):1074–81. https://doi.org/10.1001/archinte.160.8.1074.
Federal Register/Vol. 78, No. 160. Government Publishing Office. 2013. http://www.gpo.gov/fdsys/pkg/FR-2013-08-19/pdf/2013-18956.pdf. Accessed 2 June 2017.
Federal Register/Vol. 76, No. 160. 2011. https://www.gpo.gov/fdsys/pkg/FR-2011-08-18/pdf/2011-19719.pdf. Accessed 2 June 2017.
Boccuti C, Casillas G. Aiming for fewer hospital U-turns: the Medicare hospital readmission reduction program. Henry J Kaiser Fam Found. 2015:1–10.
National Quality Measures C. Total hip arthroplasty (THA) and/or total knee arthroplasty (TKA): hospital-level 30-day, all-cause, risk-standardized readmission rate (RSRR) following elective primary THA and/or TKA. Agency for Healthcare Research and Quality (AHRQ), Rockville MD. 2015. https://www.qualitymeasures.ahrq.gov/summaries/summary/49200/total-hip-arthroplasty-tha-andor-total-knee-arthroplasty-tka-hospitallevel-30day-allcause-riskstandardized-readmission-rate-rsrr-following-elective-primary-tha-andor-tka.
The Patient Protection and Affordable Care Act. Washington, DC.
Federal Register/Vol. 77, No. 170. 2012. http://www.gpo.gov/fdsys/pkg/FR-2011-08-18/pdf/2011-19719.pdf. Accessed 10 Sept 2013.
Dummit LA, Kahvecioglu D, Marrufo G, Rajkumar R, Marshall J, Tan E, et al. Association between hospital participation in a Medicare bundled payment initiative and payments and quality outcomes for lower extremity joint replacement episodes. JAMA. 2016;316(12):1267–78. https://doi.org/10.1001/jama.2016.12717.
Bundled Payments for Care Improvement (BPCI) Initiative: general information. https://innovation.cms.gov/initiatives/Bundled-Payments/index.html. Accessed 29 Aug 2015.
Press MJ, Rajkumar R, Conway PH. Medicare’s new bundled payments: design, strategy, and evolution. JAMA. 2016;315(2):131–2. https://doi.org/10.1001/jama.2015.18161.
Paxton EW, Inacio MC, Singh JA, Love R, Bini SA, Namba RS. Are there modifiable risk factors for hospital readmission after total hip arthroplasty in a US healthcare system? Clin Orthop Relat Res. 2015;473(11):3446–55. https://doi.org/10.1007/s11999-015-4278-x.
Ricciardi BF, Oi KK, Daines SB, Lee YY, Joseph AD, Westrich GH. Patient and perioperative variables affecting 30-day readmission for surgical complications after hip and knee arthroplasties: a matched cohort study. J Arthroplast. 2017;32(4):1074–9. https://doi.org/10.1016/j.arth.2016.10.019.
Clement RC, Derman PB, Graham DS, Speck RM, Flynn DN, Levin LS, et al. Risk factors, causes, and the economic implications of unplanned readmissions following total hip arthroplasty. J Arthroplast. 2013;28(8 Suppl):7–10. https://doi.org/10.1016/j.arth.2013.04.055.
Saucedo JM, Marecek GS, Wanke TR, Lee J, Stulberg SD, Puri L. Understanding readmission after primary total hip and knee arthroplasty: who's at risk? J Arthroplast. 2014;29(2):256–60. https://doi.org/10.1016/j.arth.2013.06.003.
Pugely AJ, Callaghan JJ, Martin CT, Cram P, Gao Y. Incidence of and risk factors for 30-day readmission following elective primary total joint arthroplasty: analysis from the ACS-NSQIP. J Arthroplast. 2013;28(9):1499–504. https://doi.org/10.1016/j.arth.2013.06.032.
Schairer WW, Sing DC, Vail TP, Bozic KJ. Causes and frequency of unplanned hospital readmission after total hip arthroplasty. Clin Orthop Relat Res. 2014;472(2):464–70. https://doi.org/10.1007/s11999-013-3121-5.
Tayne S, Merrill CA, Smith EL, Mackey WC. Predictive risk factors for 30-day readmissions following primary total joint arthroplasty and modification of patient management. J Arthroplast. 2014;29(10):1938–42. https://doi.org/10.1016/j.arth.2014.05.023.
Mednick RE, Alvi HM, Krishnan V, Lovecchio F, Manning DW. Factors affecting readmission rates following primary total hip arthroplasty. J Bone Joint Surg Am. 2014;96(14):1201–9. https://doi.org/10.2106/jbjs.m.00556.
Inneh IA, Lewis CG, Schutzer SF. Focused risk analysis: regression model based on 5,314 total hip and knee arthroplasty patients from a single institution. J Arthroplast. 2014;29(10):2031–5. https://doi.org/10.1016/j.arth.2014.05.007.
Joynt KE, Orav E, Jha AK. Thirty-day readmission rates for Medicare beneficiaries by race and site of care. JAMA. 2011;305(7):675–81. https://doi.org/10.1001/jama.2011.123.
Singh JA, Lu X, Rosenthal GE, Ibrahim S, Cram P. Racial disparities in knee and hip total joint arthroplasty: an 18-year analysis of national Medicare data. Ann Rheum Dis. 2014;73(12):2107–15. https://doi.org/10.1136/annrheumdis-2013-203494.
HCUP. Overview of the state inpatient databases. Healthcare cost and utilization project. Agency for Healthcare Research and Quality, Rockville, MD. https://www.hcup-us.ahrq.gov/sidoverview.jsp. Accessed 4 Feb 2017.
HCUP. HCUP quality control procedures. Agency for Healthcare Research and Quality, Rockville, MD. 2016. https://www.hcup-us.ahrq.gov/db/quality.jsp. Accessed 20 Nov 2017.
Quan H, Sundararajan V, Halfon P, Fong A, Burnand B, Luthi JC, et al. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med Care. 2005;43(11):1130–9. https://doi.org/10.1097/01.mlr.0000182534.19832.83.
LaPar DJ, Bhamidipati CM, Mery CM, Stukenborg GJ, Jones DR, Schirmer BD, et al. Primary payer status affects mortality for major surgical operations. Ann Surg. 2010;252(3):544–51. https://doi.org/10.1097/SLA.0b013e3181e8fd75.
Barnett JC, Vornovitsky MS. Health insurance coverage in the United States: 2015. US Census Bureau, Current Population Reports, Report 2016 (P60–257).
Parker K, Horowitz J, Mahl B. On views of race and inequality, blacks and whites are worlds apart. Pew Research Center. Retrieved from http://www.pewsocialtrends.org/files/2016/06/ST_2016; 2016.
Girotti ME, Shih T, Revels S, Dimick JB. Racial disparities in readmissions and site of care for major surgery. J Am Coll Surg. 2014;218(3):423–30. https://doi.org/10.1016/j.jamcollsurg.2013.12.004.
Tsai TC, Orav EJ, Joynt KE. Disparities in surgical 30-day readmission rates for Medicare beneficiaries by race and site of care. Ann Surg. 2014;259(6):1086–90. https://doi.org/10.1097/SLA.0000000000000326.
Zhang W, Lyman S, Boutin-Foster C, Parks ML, Pan TJ, Lan A, et al. Racial and ethnic disparities in utilization rate, hospital volume, and perioperative outcomes after total knee arthroplasty. J Bone Joint Surg Am. 2016;98(15):1243–52. https://doi.org/10.2106/jbjs.15.01009.
Ravi P, Sood A, Schmid M, Abdollah F, Sammon JD, Sun M, et al. Racial/ethnic disparities in perioperative outcomes of major procedures: results from the National Surgical Quality Improvement Program. Ann Surg. 2015;262(6):955–64. https://doi.org/10.1097/sla.0000000000001078.
Adelani MA, Keller MR, Barrack RL, Olsen MA. The impact of hospital volume on racial differences in complications, readmissions, and emergency department visits following total joint arthroplasty. J Arthroplast. 2017; https://doi.org/10.1016/j.arth.2017.09.034.
Nwachukwu BU, Kenny AD, Losina E, Chibnik LB, Katz JN. Complications for racial and ethnic minority groups after total hip and knee replacement: a review of the literature. J Bone Joint Surg Am. 2010;92(2):338–45. https://doi.org/10.2106/jbjs.i.00510.
J. J. Utah is nation’s fastest-growing state, Census Bureau Reports. US Census Bureau. http://www.census.gov2017/. Accessed 8 Feb 2017.
Avram V, Petruccelli D, Winemaker M, de Beer J. Total joint arthroplasty readmission rates and reasons for 30-day hospital readmission. J Arthroplast. 2014;29(3):465–8. https://doi.org/10.1016/j.arth.2013.07.039.
Kurtz SM, Lau EC, Ong KL, Adler EM, Kolisek FR, Manley MT. Which hospital and clinical factors drive 30- and 90-day readmission after TKA? J Arthroplast. 2016;31(10):2099–107. https://doi.org/10.1016/j.arth.2016.03.045.
Shaparin N, White R, Andreae M, Hall C, Kaufman A. A longitudinal linear model of patient characteristics to predict failure to attend an inner-city chronic pain clinic. J Pain. 2014;15(7):704–11. https://doi.org/10.1016/j.jpain.2014.03.004.
Andreae MH, White RS, Chen KY, Nair S, Hall C, Shaparin N. The effect of initiatives to overcome language barriers and improve attendance: a cross-sectional analysis of adherence in an inner city chronic pain clinic. Pain Med. 2016;18(2):265–74. https://doi.org/10.1093/pm/pnw161.
Andreae MH, Gabry JS, Goodrich B, White RS, Hall C. Antiemetic prophylaxis as a marker of health care disparities in the National Anesthesia Clinical Outcomes Registry. Anesth Analg. 2017;126(2):1–599. https://doi.org/10.1213/ane.0000000000002582.
Slover JD, Walsh MG, Zuckerman JD. Sex and race characteristics in patients undergoing hip and knee arthroplasty in an urban setting. J Arthroplast. 2010;25(4):576–80. https://doi.org/10.1016/j.arth.2009.03.002.
Warth LC, Callaghan JJ, Wells CW, Liu SS, Klaassen A, Gao Y, et al. Demographic and comorbid disparities based on payer type in a total joint arthroplasty cohort: implications in a changing health care arena. Iowa Orthop J. 2011;31:64–8.
Martin CT, Callaghan JJ, Liu SS, Gao Y, Warth LC, Johnston RC. Disparity in total joint arthroplasty patient comorbidities, demographics, and postoperative outcomes based on insurance payer type. J Arthroplast. 2012;27(10):1761–5.e1. https://doi.org/10.1016/j.arth.2012.06.007.
Fleischut PM, Eskreis-Winkler JM, Gaber-Baylis LK, Giambrone GP, Faggiani SL, Dutton RP, et al. Variability in anesthetic care for total knee arthroplasty: an analysis from the anesthesia quality institute. Am J Med Qual. 2015;30(2):172–9. https://doi.org/10.1177/1062860614525989.
Cozowicz C, Poeran J, Memtsoudis SG. Epidemiology, trends, and disparities in regional anaesthesia for orthopaedic surgery. Br J Anaesth. 2015;115(Suppl 2):ii57–67. https://doi.org/10.1093/bja/aev381.
Liu J, Ma C, Elkassabany N, Fleisher LA, Neuman MD. Neuraxial anesthesia decreases postoperative systemic infection risk compared with general anesthesia in knee arthroplasty. Anesth Analg. 2013;117(4):1010–6. https://doi.org/10.1213/ANE.0b013e3182a1bf1c.
Basques BA, Toy JO, Bohl DD, Golinvaux NS, Grauer JN. General compared with spinal anesthesia for total hip arthroplasty. J Bone Joint Surg Am. 2015;97(6):455–61. https://doi.org/10.2106/jbjs.n.00662.
Atchabahian A, Andreae M. Long-term functional outcomes after regional anesthesia: a summary of the published evidence and a recent Cochrane review. Refresh Course Anesthesiol. 2015;43(1):15–26. https://doi.org/10.1097/ASA.0000000000000033.
Memtsoudis SG, Sun X, Chiu YL, Stundner O, Liu SS, Banerjee S, et al. Perioperative comparative effectiveness of anesthetic technique in orthopedic patients. Anesthesiology. 2013;118(5):1046–58. https://doi.org/10.1097/ALN.0b013e318286061d.
Hoffman KM, Trawalter S, Axt JR, Oliver MN. Racial bias in pain assessment and treatment recommendations, and false beliefs about biological differences between blacks and whites. Proc Natl Acad Sci. 2016;113(16):4296–301. https://doi.org/10.1073/pnas.1516047113.
Wiznia DH, Zaki T, Maisano J, Kim CY, Halaszynski TM, Leslie MP. Influence of medical insurance under the affordable care act on access to pain management of the trauma patient. Reg Anesth Pain Med. 2017;42(1):39–44. https://doi.org/10.1097/aap.0000000000000502.
Freburger JK, Holmes GM, L-JE K, Cutchin MP, Heatwole-Shank K, Edwards LJ. Disparities in post-acute rehabilitation care for joint replacement. Arthritis Care Res (Hoboken). 2011;63(7):1020–30. https://doi.org/10.1002/acr.20477.
Goodman SM, Parks ML, McHugh K, Fields K, Smethurst R, Figgie MP, et al. Disparities in outcomes for African Americans and Whites undergoing total knee arthroplasty: a systematic literature review. J Rheumatol. 2016;43(4):765–70. https://doi.org/10.3899/jrheum.150950.
Keeney JA, Nam D, Johnson SR, Nunley RM, Clohisy JC, Barrack RL. Socioeconomically disadvantaged CMS beneficiaries do not benefit from the readmission reduction initiatives. J Arthroplast. 2015;30(12):2082–5. https://doi.org/10.1016/j.arth.2015.06.031.
Keeney JA, Nam D, Johnson SR, Nunley RM, Clohisy JC, Barrack RL. The impact of risk reduction initiatives on readmission: THA and TKA readmission rates. J Arthroplast. 2015;30(12):2057–60. https://doi.org/10.1016/j.arth.2015.06.007.
Jordan CJ, Goldstein RY, Michels RF, Hutzler L, Slover JD, Bosco JA 3rd. Comprehensive program reduces hospital readmission rates after total joint arthroplasty. Am J Orthop (Belle Mead NJ). 2012;41(11):E147–51.
Jiang HJ, Boutwell AE, Maxwell J, Bourgoin A, Regenstein M, Andres E. Understanding patient, provider, and system factors related to Medicaid readmissions. Jt Comm J Qual Patient Saf. 2016;42(3):115–21. https://doi.org/10.1016/S1553-7250(16)42014-3.
Coughlin TA, Long SK, Clemans-Cope L, Resnick D. What difference does medicaid make? Assessing cost effectiveness, access, and financial protection under Medicaid for low-income adults. Kaiser Commission Medicaid and the Uninsured. 2013.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
The Weill Cornell Medicine Institutional Review Board approved all study activities.
Conflict of Interest
The authors declare that they have no conflict of interest.
Electronic Supplementary Material
Rights and permissions
About this article

Cite this article
White, R.S., Sastow, D.L., Gaber-Baylis, L.K. et al. Readmission Rates and Diagnoses Following Total Hip Replacement in Relation to Insurance Payer Status, Race and Ethnicity, and Income Status. J. Racial and Ethnic Health Disparities 5, 1202–1214 (2018). https://doi.org/10.1007/s40615-018-0467-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40615-018-0467-0