
Abstract
Background
Marriage below the age of 20 brings negative health consequences to female adolescents. Ethiopia is one of the top ten countries with the highest rates of child marriage despite the minimum legal age at first marriage was 18 years.
Objective
To assess the prevalence of adolescent marriage and its associated factors among young women of Delanta District, North-East Ethiopia.
Methods
A community-based cross-sectional study was conducted on 597 adolescent women between the age of 15 and 19. A cluster sampling technique was used for this study. Data were entered and cleaned by EpiData-3.02 and analyzed by SPSS-20.
Results
Around 40% of adolescents were married at the time of the survey. Adolescent marriage was twice higher among girls below the age of 18 (AOR: 2.12, 95%CI (1.15, 3.90)). Lack of comprehensive knowledge on obstetrics fistula prevention increases the risk of adolescent marriage by three folds.
Conclusion
This study indicated that adolescent marriage was higher in the area. Delaying the age at first marriage by implementing the Ethiopian Family Code proclamation is needed
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Background
Adolescent marriage, which is defined as marriage below the age of 20, negatively affects the health of female adolescents. Annually around 21 million women between the age of 15 and 19 years become pregnant in developing countries with 12 million births (Darroch et al., 2016). The minimum age at marriage varies across countries which are 20 years in Nepal (September 8, 2016) and 18 years in most countries. The prevalence of adolescent marriage is higher in sub-Saharan Africa and South Asia. Around 75% of women in Niger, 66% in Bangladesh, 48% in Burkina Faso, 39% in Nigeria, 41% in Ethiopia, 45% in Somalia, 47% in India, 30% in Brazil, and 55% in Mali were married by age 18 (United Nation Population Fund, 2012). In developing countries, nearly 33% and 11% of girls are married by age 18 and 15, respectively, resulting in 39,000 adolescent marriages every day. Twenty percent of child marriage and 40% of adolescent girl marriage were in Africa (Hodgkinson et al., 2016).
Ethiopia is a country having 24% of adolescents between the ages of 10 and 19. The 2016 Ethiopia Demographic and Health Survey (EDHS) reveals that the median age at first marriage in women was 17.1 years and nearly 17% of women aged 15–19 were married (Central Statistical Agency, July 2017) though the minimum age at first marriage for both men and women is 18 years (Nayak BK, July 2013). Ethiopia is one of the top ten countries with the highest rates of child marriage (United Nations Children’s Fund, 2014). It was practiced because of socioeconomic difficulties, cultural values, religious beliefs, and women’s low autonomy in decision-making (Montazeri et al., 2016). Residing in a rural area, having not attended school, being followers of the Muslim religion, residing in the Amhara region, and having uneducated families contributing to the highest rate of adolescent marriage in the country (Erulka, 2013).
Adolescent marriage is a common global problem violating the human rights of individuals. It increases the risk of acquiring sexually transmitted diseases(STIs), cervical cancer, death during childbirth, obstetric fistulas, premature birth (death as neonates, infants, or children) (Nour NM, 2006, Nayak BK, July 2013), marital violence (Raj et al., 2010; Speizer & Pearson, 2011; Yount et al., 2016), uncontrolled fertility (Godha et al., 2011), and education dropout and limits woman’s opportunities (Svanemyr et al., 2012). Globally, around 50,000–100,000 women are affected by obstetric fistula every year as a result of childbirth complications. It is common in sub-Saharan Africa and South Asia, as access to and use of emergency obstetric care is limited (Tebeu et al., 2012). More than 110,000 women in Ethiopia had a vaginal fistula (Ahmed & Tunçalp, 2015). In Ethiopia, around 9000 new cases of obstetrics fistula occur every year. The condition occurs disproportionately among impoverished girls and women, especially those that live far from medical services (DSW, 2011). The most affected groups were 15- to 19-year-old girls (2%). One of the measures to be taken in the prevention of fistula is the prevention of early childbearing by banning adolescent marriage (Kalembo & Zgambo, 2012).
The eligible age range in this study was set between 15 and 19 years following the rationale that they constitute the most affected age group (Adler et al., 2013) having the highest risk for both maternal morbidities and mortalities in the first reproductive life’s of women (Central Statistical Agency, July 2017, Central statistical Agency, 2007) and again obstetric fistula as a result of pregnancies below the age of 20 constitute a large proportion in developing countries (Tebeu et al., 2012). This group of women is understudied because of legal reasons to access informed, written, and voluntary consent from the participant especially those below the age of 18 (Banke-Thomas et al., 2013). There are also research gaps on the prevalence and trends of child marriage and its causes (Svanemyr et al., 2015).
This research was conducted in the Amhara region, where the highest number of early marriages in the country (Inbaraj, 2015). This study aimed to assess the prevalence of adolescent marriage and its associated factors among women aged 15 to 19 years in Delanta District, Northeast Ethiopia.
Methods
Study Area and Period. The study was conducted in Delanta District, which is part of Amhara Regional State of Ethiopia, located in north-east parts of the country. Wogeltena is the town for this particular district and is located in the South Wollo Zone of the Amhara Region and situated on the main road between Dessie and Amba Mariam and Lalibela. It is situated at a distance of 494 km north-east away from Addis Ababa and 325 km east from Bahir Dar. The majority of the inhabitants (90.78%) followed Ethiopian Orthodox Christianity, while 9.21% of the population were Muslim (Central statistical Agency, 2007). The total population of the district reached 142,009, of which 23.58% are women of reproductive age. The district has 6 health centers and 33 health posts (2014/15 annual report of the District). The study was conducted from March 22 to 31, 2016.
Study Design. A community-based cross-sectional study design was conducted.
Populations. All adolescent women of the district between the ages of 15 to 19 were included in this study. Women residing in the area for at least six months before the study were included.
Sample Size Calculation. The sample size was estimated by using a single population proportion formula based on the 30% prevalence of adolescent marriage in Ethiopia (Erulka, 2013) with a level of precision at 95%, taking 5% for non-response rate and with a design effect (Deff) of 2. The final sample size reached 619 after adjustment (N = 3577).
Sampling Procedures (Techniques). In Delanta District, there were 33 rural kebeles and one urban center. They comprised a total of 3577 women between the age of 15 and 19 years (2014/2015 annual report of the District). Rural kebeles of the district were stratified into those having health centers and without the assumption of the presence of health center within the kebele may results in high awareness in health-related consequences of early marriage which further influences marital age. After stratification, six rural kebeles were selected by simple random sampling techniques (lottery method) and the urban center was purposively included. Cluster sampling technique was used to get the desired sample size (n = 619). The survey was conducted 2 weeks before the actual data collection time and a total of 635 eligible women were identified. In case of more than one woman in a household during data collection, only one eligible woman was included by the lottery method (Fig. 1).
Data Collection Tool and Procedure. A structured interviewer-administered questionnaire was first prepared in English and then translated into the local Amharic language and again re-translated to English to maintain consistency in translation. Data was collected from each study subject by using structured Amharic interview questions. The study subjects were interviewed by six trained data collectors.
Study Variables
Dependent variable. Adolescent marriage (ever married/not married).
Independent variables: Age (current age, age at first marriage, and pregnancy), Marital status, religion, residence, women education and occupation, awareness of obstetrics complication, exposure to media, history of contraceptive use, household head education and occupation, history of induced abortion, comprehensive knowledge on obstetrics fistula prevention (OFP), and pregnancy history.
Operational Definitions
Adolescent: Women who belonged to the age between 15 and 19.
Adolescent marriage: Participants were classified as having adolescent marriage if they were married, divorced, and widowed at the time of data collection.
Comprehensive knowledge on OFP: Participants who scored 75% or more on knowledge questions were classified as having comprehensive knowledge while those with a score of less than 75% were classified as having not comprehensive knowledge. The criteria’s used to assess knowledge on OFP found elsewhere (Banke-Thomas et al., 2013).
Access to media: Having access to media was considered if participants had access to one or more of the available medias (radio, television, magazine).
Kebele: The smallest administrative unit in the district.
Awareness on obstetrics complications: If a girl mentioned at least one of the following pregnancy and childbirth complications (hypertension disorder of pregnancy, obstructed labor, bleeding, obstetrics fistula, abortion, ectopic pregnancy, ruptured uterus), she were considered as having an awareness.
Data quality control: Pretest was conducted before the main study on 31 girls and the necessary modifications were made to the instrument to simplify the language but data on pretest were excluded from the main study. Double data entry for 10% of the questionnaire was performed to see consistency in data entry and separately entered data were checked to correct mismatches.
Data processing and analysis: Data were entered and cleaned using EpiDATA version 3.02 and analyzed by SPSS version 20 statistical software. Both descriptive and analytic analyses were computed. A bivariate logistic regression was performed, and variables showing association (p < 0.2) with adolescent marriage were entered into multivariate logistic regression to control the effect of confounding variables. Factors considered significant in the final model were p < 0.05.
Ethical considerations: To conduct the study permission was obtained from Haramaya University College of Health and Medical Science after an ethical review of the contents of the proposal by the University Institutional Health Research Ethics Review Committee (IHRERC). Letter of support was received from Delanta District Administration Office for the necessary facilitation and smooth undertaking of the study. Written, informed, and signed consent were taken from respondents of age 18 and above, and for those aged below 18 years informed, written, and signed consent were taken from their guardian’s (Biological families, caregiver, and husband) before their voluntarism and assent from the participants for interview. Participation in the study was fully voluntary.
Results
Characteristics of Study Participants
A total of 619 contacts were made, whereby 22 declined to participate, making the total number of respondents to be 597 (96.4%). Of the 22 who declined to participate, 2 were from the urban group. The mean age of participants was 17.62 (SD ± 1.36) years old and 98.7% were Orthodox Christianity followers. Among the total sample 28.6% had not received school education and near to half were students (Table 1).
Adolescent Marriage and Behavior
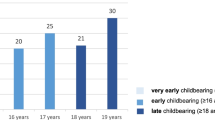
The prevalence of adolescent marriage in the area was 38.9% (95% CI 35, 42.7). Near to 42% of women who have an awareness of obstetrics complications, 18% of under-eighteen girls, and 69% of contraceptive users were married. From all women who had a history of pregnancy, the majorities (60.5%) were pregnant before the age of 18 (Table 1).
Factors Associated with Adolescent Marriage
This study showed a significant association between women’s age and the odds of having a marriage. Women who were under the age of 18 were three times more likely to have a marriage (AOR = 2.62, 95% CI 1.46, 4.71) than those who were 18 and above. Those who had access to media were 66% less likely to engage in marriage (AOR = 0.34, 95% CI 0.17, 0.69). Women who were from families of no formal education had three times more risk of adolescent marriage (AOR = 3.47 95% CI 1.27, 9.48). Women who had no comprehensive knowledge on OFP were three times more likely to marry during their adolescent period (AOR 2.92, 95% CI 1.60, 5.33) (Table 2).
Discussion
The results of this showed that the prevalence of adolescent marriage in Delanta District was 38.9% of which 42.4% were below the age of 18. The finding was lower than studies conducted in Bangladesh (68.9%) (Yount et al., 2016), Serbia (50.4%) (Hotchkiss et al., 2016), Nepal (53.3%) (Sah et al., 2014), India (58%) (Raja et al., July 2010), Sudan (45.9%) (Ali et al., 2014), and Brukinefaso (55%) (Banke-Thomas et al., 2013). These differences could be attributed with the current study were the most recent, difference in study subjects whereby most of the above studies were retrospectively collected from already married women’s above the age of 20, differences in the legal age at first marriage and socio-cultural differences mainly of religion and ethnicity across countries. The result was higher than the national data 17% in 2016 (Central Statistical Agency, July 2017) and 26.7% in 2005 (Central Statistical Agency [Ethiopia] and ORC Macro, 2006). The higher the prevalence could be attributed with the national survey included most urbanized areas whereby adolescent marriage was unlikely. This result exposes the contradiction between situations on the ground and what the law prescribes, whereby the legal age for marriage is set at 18 years for girls in Ethiopia (Ethiopia, 2007). This effectively signifies the importance of reaching out to girls with reproductive health messages.
According to this study, adolescent marriage was higher in rural areas (41.0% in rural vs 27.2% in urban). The practice of child marriage was common among girls who reside in rural locations (Hotchkiss et al., 2016; Ali et al., 2014; United Nations Children’s Fund, 2014). Women living in rural areas could have lower access and exposure to mass media which might further reduce their level of awareness and knowledge on health-related issues. Bringing changes in attitudes, social norms, and behaviors that may lead to positive public health outcomes in rural areas might be challenging (Asp et al., 2014). A study on knowledge about reproductive health among Bangladesh women also showed that rural women had lower knowledge than their urban counterparts (14% vs 75%) (HAUE M et al., 2015). Health knowledge declined as the distance from the nearby health institution increases, which is common in rural areas, and may expose them to adolescent marriage. This urban–rural gap signifies the need for focusing on rural women targeting the reduction of the risks towards early marriage.
In this study, the risk of adolescent marriage was three times higher among women who had no comprehensive knowledge of OFP (AOR 2.92, 95% CI 1.60, 5.33). The reason could be girls might not resist the practice if they have low knowledge of the negative health outcomes of child marriage (Nasrullah et al., 2014). Empowering girls with health information (health and sex education) can increase their self-esteem and improves their sense of self and self-efficacy which further affects the age at first marriage (Olson, November 26, 2014).
Parental education positively contributes to the health of children. In this study women who were from non-educated families had three times more risk of adolescent marriage (AOR 3.39, 95% CI (1.18, 9.74). This was supported by study results showing women from low family education had a greater chance of getting married early (Marchetta & Sahn, 2016). Household decision-making on the choice and timing of marriage could be exclusively preserved for parents if girls are from uneducated families (Adedokun et al., 2016) as they might not be able to predict and evaluate the consequences of early marriage (Montazeri et al., 2016a). In non-educated families, parental control affects a girl’s freedom of expression and forcing them into marriage (Sabbe et al., 2013). Educated families indirectly affect the timing of marriage by taking school as the best alternative than early marriage for girls (Carlson, 1979). Women who had no formal education were 84% less likely to marry (AOR = 0.16, 95% CI 0.08, 0.35)). This finding was not supported by different studies (Ikamari, 2005, Gurmu & Mace, 2013; Erulka, 2013) but the possible reason may be linked with recent changes in social norms in which adolescents believed that “men don’t want to marry an illiterate girl since girls’ economic contribution to make more money and better management of household finances is more with better education” (Jones et al., 2014).
Women below the age of 18 had two times more risk of adolescent marriage (AOR 2.12, 95% CI 1.15, 3.90). The possible justification might be people within the region believed that adolescent marriage is considered as early if it occurred before age 15 for girls (Gage, April 2009). It may also be related to the issue that, the younger a woman had been at the time of her marriage, the more likely she is from parents who had no education (Erulka, 2013).
Based on the result of this study adolescents who had a history of pregnancy were 59% less likely to marry. The cause of the association may be the presence of a high rate of adolescent pregnancies before marriage (35.5%). It could be linked with community perceptions on perceived premarital fertility which is undesirable. Premarital pregnancy may be considered as a loss of parental authority and increasing the freedom of young’s which may result in marital stigma. In most scenarios, pregnancy before marriage was associated with non-contraceptive use and refusal of abortion care for religious reasons which in turn may be associated with a high risk of STIs (Zwang & Garenne, 2008) and may prevent it from marriage. Adolescents who had a history of contraceptive use had 87% less risk of early marriage. This finding was supported by pieces of evidence showing a high rate of contraceptive use among adolescent girls were from unmarried women whose rights of childbearing and age at first marriage were respected (Páez & Ortega, 2016; Marrone et al., 2014). Those who are utilizing contraception methods maybe those who had knowledge about contraception (Okeowo & Olujide, 2014) which may further affect the age at first marriage.
Conclusion
The finding indicated that adolescent marriage was a significant public health problem in Delanta District. Reproductive health programs in the area should target adolescent girls to increase their reproductive health knowledge through health education to tackle adolescent marriage. The district should work to delay age at first marriage by implementing the Ethiopian Family Code proclamation whereby the legal age for marriage should be 18 years and above. Provision of contraception and increases its awareness needs special attention to prevent childbearing at a young age. Attention should be given to increase the educational status of women and school education on adolescent sexual and reproductive health. Research on knowledge of families regarding the health threats of adolescent marriage and existed legal grounds is needed since most risky decisions are made by parents.
Availability of Data and Materials
The data sets used and analyzed for the study are available from the corresponding author on reasonable request. The investigators are responsible for all information provided to the journal.
Abbreviations
- CSA:
-
Central Statistical Agency
- EDHS:
-
Ethiopian Demography and Health Survey
- IHRERC:
-
Institutional Health Research Ethics Review Committee
- STIs:
-
Sexually transmitted infections
- OFP:
-
Obstetric fistula prevention
References
Adedokun, O., Adeyemi, O. & Dauda, C. (2016) Child marriage and maternal health risks among young mothers in Gombi, Adamawa State, Nigeria: Implications for mortality, entitlements and freedoms. African health sciences, 16, 986-999.
Adler, A. J., Ronsmans, C., Calvert, C., & Filippi, V. (2013). Estimating the prevalence of obstetric fistula: A systematic review and meta-analysis. BMC Pregnancy and Childbirth, 13, 246.
Ahmed, S., & Tunçalp, Ö. (2015). Burden of obstetric fistula: From measurement to action. The Lancet Global Health, 3, e243–e244.
Ali, A., Ibrahim, I., Abdelgbar, S., & Elgessim, M. (2014). Socio-demographic factors affecting child marriage in Sudan. J Women’s Health Care, 3, 163.
Asp, G., Pettersson, K. O., Sandberg, J., Kabakyenga, J., & Agardh, A. (2014). Associations between mass media exposure and birth preparedness among women in southwestern Uganda: A community-based survey. Global health action, 7, 22904.
Banke-Thomas, A. O., Kouraogo, S. F., Siribie, A., Taddese, H. B. & Mueller, J. E. (2013). Knowledge of obstetric fistula prevention amongst young women in urban and rural Burkina Faso: A cross-sectional study. PloS One, 8.
Carlson, E. (1979). Family Background, School and Early Marriage. Journal of Marriage and Family, 41.
Central Statistical Agency. (2007). Central Statistical Agency of Ethiopia: population and housing census report.
Central Statistical Agency. (2017). Ethiopia Demographic and Health Survey 2016 The DHS Program ICF, Rockville, Maryland, USA.
Central Statistical Agency [Ethiopia] and Orc Macro. (2006). Ethiopia Demographic and Health Survey 2005 Addis Ababa Central Statistical Agency and ORC Macro Ethiopia and Calverton, Maryland, USA
Darroch, J. E., Woog, V., Bankole, A., Ashford, L. S. & Points, K. (2016). Costs and benefits of meeting the contraceptive needs of adolescents. Guttmacher Institute.
DSW. (2011). German Foundation for World Population: Fight Fistula : Educating and Empowering Women in Ethiopia
Erulka, A. (2013). Early marriage, marital relations and intimate partner violence in Ethiopia. International Perspectives on Sexual and Reproductive Health, 39.
Ethiopia, S. P. (2007). Federal Negarit Gazeta of the Federal Democratic Republic of Ethiopia. Proclamation No. 513/2007. Addis Ababa, 12 February 2007.
Gage, A.J. (2009). Coverage and effects of child marriage prevention activities in Amhara Region, Ethiopia.
Godha, D., Hotchkiss, D., & Gage, A. (2011). The influence of child marriage on fertility, fertility-control, and maternal health care utilization: A multi-country study from South Asia. Chapel Hill, NC: MEASURE Evaluation PRH.
Gurmu, E., & Mace, R. (2013). Determinants of age at first marriage in Addis Ababa, Ethiopia. Journal of Social Development in Africa, 28, 87–110.
Haue M, Hossain S, Ahmed KR, Sultana T, Chowdhury, H. & Akter J. (2015). A comparative study on knowledge about reproductive health among urban and rural women of Bangladesh. Journal of family and reproductive health, 9.
Hodgkinson, K., Koster, W., & Miedema, E. (2016). Understanding and addressing child marriage. Amsterdam: University of Amsterdam.
Hotchkiss, D. R., Godha, D., Gage, A. J., & Cappa, C. (2016). Risk factors associated with the practice of child marriage among Roma girls in Serbia. BMC international health and human rights, 16, 6–6.
Ikamari, L. D. (2005). The effect of education on the timing of marriage in Kenya. Demographic Research, 12, 1–28.
Inbaraj, S. (2015). Married as children, women with obstetric fistulas have no future: Population Reference Bureau
Jones, N., Tefera, B., Stephenson, J., Gupta, T., Pereznieto, P., ... Emire, G. (2014). Early marriage and education: the complex role of social norms in shaping Ethiopian adolescent girls’ lives (pp. 1–103). Country Report: Shaping policy for development.
Kalembo, F. & Zgambo, M. (2012). Obstetric fistula: A hidden publichealth problem in sub-Saharan Africa. Arts and Social Sciences Journal, Vol.ASSJ-41
Marchetta, F., & Sahn, D. E. (2016). The role of education and family background in marriage, childbearing, and labor market participation in Senegal. Economic Development and Cultural Change, 64, 369–403.
Marrone, G., Abdul-Rahman, L., de Coninck, Z., & Johansson, A. (2014). Predictors of contraceptive use among female adolescents in Ghana. African journal of reproductive health, 18, 102–109.
Montazeri, S., Gharacheh, M., Mohammadi, N., & Alaghband Rad, J. & Efterkhar Ardabili, H. (2016). Determinants of early marriage from married girls’ perspectives in Iranian setting: A qualitative study. Journal of environmental and public health, 8615929–8615929.
Nasrullah, M., Zakar, R., Zakar, M. Z., Abbas, S., Safdar, R., Shaukat, M., & Krämer, A. (2014). Knowledge and attitude towards child marriage practice among women married as children-a qualitative study in urban slums of Lahore Pakistan. . BMC Public Health, 14, 1148.
Nayak, B.K. (2013). Child marriage in Ethiopia -A matter of concern. International Journal of Management and Social Sciences Research, 2.
Nour, N.M. (2006). Health Consequences of Child Marriage in Africa. Emerging Infectious Diseases, 12.
Okeowo, T., & Olujide, M. (2014). Attitude, knowledge and utilization of family planning methods among rural women in Ogun State, Nigeria. Agrosearch, 14, 39–53.
Olson, C. (2014). 16 ways of preventing and intervening in child marriages.
Páez, D. A. S. & Ortega, J. A. (2016) Adolescent contraceptive use and its impacts on early marriage and fertility.
Raj, A., Saggurti, N., Lawrence, D., Balaiah, D., & Silverman, J. G. (2010). Association between adolescent marriage and marital violence among young adult women in India. International Journal of Gynaecology and Obstetrics: the official organ of the International Federation of Gynaecology and Obstetrics, 110, 35–39.
Raja, A., Saggurtic, N., Lawrencea, D., Balaiahd, D. & Silvermane, J.G. (2010). Association between adolescent marriage and marital violence among young adult women in India. International Journal of Gynaecology and Obstetrics , 110.
Sabbe, A., Oulami, H., Zekraoui, W., Hikmat, H., Temmerman, M., & Leye, E. (2013). Determinants of child and forced marriage in Morocco: stakeholder perspectives on health, policies and human rights. BMC international health and human rights, 13, 43–43.
Sah, R., Gaurav, K., Baral, D., Subedi, L., Jha, N., & Pokharel, P. (2014). Factors affecting early age marriage in Dhankuta Municipality, Nepal. Nepal Journal of Medical Sciences, 3, 26–30.
September 8, 2016. “Our Time to Sing and Play” child marriage in Nepal: https://www.refworld.org/docid/57d2affd4.html
Speizer, I. S., & Pearson, E. (2011). Association between early marriage and intimate partner violence in India: A focus on youth from Bihar and Rajasthan. Journal of interpersonal violence, 26, 1963–1981.
Svanemyr, J., Chandra-Mouli, V., Christiansen, C. S., & Mbizvo, M. (2012). Preventing child marriages: First international day of the girl child “my life, my right, end child marriage.” Reproductive health, 9, 31–31.
Svanemyr, J., Chandra-Mouli, V., Raj, A., Travers, E., & Sundaram, L. (2015). Research priorities on ending child marriage and supporting married girls. Reproductive health, 12, 80–80.
Tebeu, P. M., Fomulu, J. N., Khaddaj, S., Bernis, L., Delvaux, T., & Rochat, C. H. (2012). Risk factors for obstetric fistula: A clinical review. International Urogynecology Journal, 23, P387-394.
UNITED NATION POPULATION FUND. (2012). Marriying to Young. End Child Marriage: Global & Regional levels and Trends.
UNITED NATIONS CHILDREN’S FUND. (2014). Ending Child Marriage: Progress and prospects. New York: UNICEF.
Yount, K. M., Crandall, A., Cheong, Y. F., Osypuk, T. L., Bates, L. M., Naved, R. T., & Schuler, S. R. (2016). Child marriage and intimate partner violence in rural Bangladesh: A longitudinal multilevel analysis. Demography, 53, 1821–1852.
Zwang, J., & Garenne, M. (2008). Social context of premarital fertility in rural South-Africa. African journal of reproductive health, 12, 98–110.
Acknowledgements
I would like to express my sincere and heartfelt gratitude to Delanta District Administrative Office for the provision of the necessary information that was an important input for the study; the Galladi Health Office for their support in every aspects of the research work. Also, I would like to thank study participants who were devoted their time to participate in the study; the community of selected sites of the district for their cooperation in all aspects they were asked. Finally, my everlasting love and appreciation is to my family especially my brothers Dessalew Adane and Wunete Masresha for their special support and all other family members and friends for their help.
Funding
Haramaya University covered all the costs incurred by the study.
Author information
Authors and Affiliations
Contributions
SAM, MWK, and GDA wrote the proposal and participate in the data collection and entry processes. They analyzed the data, drafted, read, and approved the manuscript.
Corresponding author
Ethics declarations
Ethical Approval
All procedures performed in studies involving human participants were under the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Permission and ethical approval were obtained from Haramaya University College of Health and Medical Science after an ethical review of the contents of the proposal by the University Institutional Health Research Ethics Review Committee (IHRERC). Written, informed, and signed consent were taken from respondents of age 18 and above, and for those aged below 18 years, informed, written, and signed consent were taken from their guardian’s (biological families, caregiver, and husband) before their voluntarism and assent from the participants for interview. We confirmed that the IHRERC approved minor consents for this study. Participation in the study was fully voluntary.
Consent for Publication
This manuscript does not contain any individual/personal data in any form, so it does not need consent for publication.
Conflict of Interest
The authors declare that they have no any conflict of interest.
Appendix
Appendix

Schematic diagram of sampling procedure of adolescent women in Delanta District, 2016
Rights and permissions
About this article

Cite this article
Masresha, S.A., Kassaw, M.W. & Alen, G.D. Adolescent Marriage in Northeast Ethiopia: The Case of Delanta District . Glob Soc Welf 8, 171–179 (2021). https://doi.org/10.1007/s40609-021-00206-7
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40609-021-00206-7