
Abstract
Objective
The practice of medicine is inherently uncertain. We sought to measure the level of psychological distress among medical students and to ascertain if an intolerance of uncertainty and ambiguity were associated with distress.
Method
The authors conducted a cross-sectional study with a population consisting of 4th year undergraduate medical students at an Irish university. Psychological distress was measured with the GHQ-12 scale. The “tolerance of ambiguity” scale and the “Intolerance of Uncertainty Scale (IUS)-12” were used to measure the respective variables.
Results
One hundred students (class size of 123) participated in this study giving a response rate of 81 %. A total of 27 % of the students met the criteria for psychological distress. Student psychological distress, as measured by GHQ-12 caseness, was associated with a higher intolerance of uncertainty (mean 31.70 (6.18)) compared with those who were not distressed (mean IUS score 26.66 (6.58)) (t (98) = −5.52, p < 0.001).
Conclusion
A relative lack of tolerance for uncertainty may prove to be an important predictor of psychological distress in undergraduates. There is an argument for designing appropriate interventions so that learners can come to recognize and embrace uncertainty rather than its remaining unacknowledged and potentially contributing to psychological morbidity.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Psychological stress can be considered as an unavoidable part of medical education [1]. The level of stress endured by medical undergraduates has been highlighted as a risk factor in the emergence of psychological distress and mental health problems in this population [2–4]. Prevalence studies using the General Health Questionnaire-12 (GHQ-12) have consistently identified increased rates of psychological morbidity in medical student populations with a rate of 52 % reported in one cross-sectional study [5] and a rate of 36 % identified in another [6].
The Role of Uncertainty and Ambiguity in Medical Student Distress
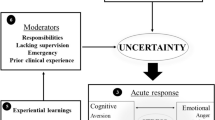
It is within the context of the inherently unpredictable, complex, and uncertain world of medical practice that psychological distress due to an intolerance of uncertainty may be elicited. Medical education has been described as a training for certainty with an overemphasis on unambiguous facts, solvable problems, and correct answers [7, 8], but it is in contrast to the practice of medicine which is fundamentally uncertain. Many of the problems faced by doctors and by medical students point to the uncertainties faced by practitioners in the world of medicine and the fact that a doctor’s role is to exercise judgement in situations of uncertainty [9]. Absolute certainty is unattainable, no matter how much information is gathered by a medical practitioner [10]. It follows that medical education, in which there is a focus on the need for certainty in clinical decision-making, may be a source of increased stress for those students who are more intolerant of the uncertainty which arises in clinically ambiguous situations.
Sources of uncertainty for medical students include technical, personal, and conceptual [11]. The exponential growth of medical knowledge makes it difficult for students to be certain that they have adequate levels of knowledge to perform well in unpredictable clinical situations, contributing to technical uncertainty. Personal uncertainty arises from not knowing a patient’s wishes and from the emotional attachment of the student to a patient. This may lead to the student self-perception that their decision-making is impaired [11]. Conceptual uncertainty arises from the problem of applying abstract criteria to concrete situations [12]. This conceptualization of dimensions of uncertainty implies that the mere accumulation of more knowledge will not lead to an overall improvement in the degree of uncertainty faced by students in their decision-making.
An allied phenomenon to uncertainty in the field of medical education and practice is the intolerance of ambiguity. Intolerance of ambiguity has been defined as the tendency to perceive ambiguous situations as sources of threat. Ambiguous situations can be categorized as those which cannot be adequately structured by an individual and which are characterized by novelty, complexity, or insolubility [13]. It is recognized that individuals who are distressed by ambiguous situations will try to avoid them. The ability of students to tolerate ambiguity and uncertainty in clinical decision-making and their studies would appear to be a protective factor from the development of psychological distress. While intolerance of ambiguity and intolerance of uncertainty share some commonality, they are correctly considered as separate and distinct phenomena [14]. Individuals who are intolerant of ambiguity are unable to tolerate equivocal situations in the present time, while intolerance of uncertainty is the tendency of individuals to consider the possibility of a future negative event occurring as unacceptable, irrespective of the probability of occurrence [15]. An individual who is intolerant of ambiguity will be more likely to interpret a present situation as being full of threat as opposed to one who is intolerant of uncertainty and is increasingly likely to interpret future events as a source of threat [14]. An intolerance of uncertainty has been shown to be a characteristic involved in excessive worry [15], to be strongly associated with generalized anxiety disorder [15, 16], as well as depression and obsessive compulsive disorder [16].
The study described in this paper aims to examine the relationship between the degree of intolerance of uncertainty and ambiguity and student emotional disturbance. It was hypothesized that students’ who demonstrate a higher intolerance of uncertainty and ambiguity will be afflicted by a more significant psychological disturbance.
Method
The study population consists of all students who were enrolled in the 4th year medicine classes in the National University of Ireland, Galway (NUIG), in the academic year 2011–2012. All 123 fourth year medical students were asked to participate and to complete the study questionnaires. The penultimate year of medical studies in NUIG is structured to allow students to rotate through clinical specialties, namely general practice, obstetrics and gynecology, otorhinolaryngology, pediatrics, and psychiatry. They have already completed medical and surgical clinical placements during year 3 of their studies. This period of their undergraduate education has at its core an experiential training program, and students are expected to develop clinical competencies through regular access to patients in clinical settings.
The students received the questionnaires relating to the study during semester 2 of the academic year 2011–2012. The questionnaires were distributed to the students at concurrent time points during the second semester and at such times that their levels of distress would have been minimally influenced by concerns regarding training placements. All responses were anonymous. There were no exclusion criteria.
A cross-sectional study design was used, and self-administered questionnaires were distributed for the data collection.
Demographic data on all of the participants was collected, including their gender, age, and ethnicity.
Data on the level of psychological disturbance among the medical students was collected using the General Health Questionnaire (GHQ)-12 [17]. The GHQ-12 is a well-validated [18], self-administered screening test for general psychiatric morbidity. Each item in the GHQ-12 has four possible response options, and the GHQ-12 two-point response scale scoring method (GHQ method) was used in this study.
Prevalence estimations were assessed with the GHQ-12, in which the item is scored from 0 to 1 (maximum score is 12). This is the standard method recommended by Goldberg [17], whereby a score of 0 is given when either of the first two options in each item is selected and a score of 1 is given when either of the other options is given. Six of the questions are reverse-scored (i.e., 1,1,0,0 or 3, 2, 1, 0) (Appendix B in ESM). A score of 4 or more indicates caseness or pathological levels of distress [17].
A modified version of Budners’ Tolerance for Ambiguity Scale (TAS) [19] (Appendix C in ESM) was presented to the students for completion. This 16-item scale measures the tendency of an individual to perceive ambiguous situations as a source of threat, with higher scores indicating a greater intolerance of ambiguity. The modification of the instrument involves the rewording of four of the items in order to increase their relevance to the medical student population (items 5, 7, 9, and 13). The tolerance for ambiguity scale has demonstrated moderate internal consistency (Cronbachs’ α = 0.64) and moderate reliability (r = 0.64) when respondents are medical students [20], and the modified scale has demonstrated validity [19]. It has been criticized for lacking reliability [21], but it was chosen for this study due to its frequency of prior use in medical student populations [13, 19, 20, 22].
The 12-item Intolerance of Uncertainty Scale (IUS-12) (Appendix D in ESM) [23] is an abridged version of the well-validated 27-item IUS [24]. The IUS-12 has demonstrated excellent internal consistency (Cronbachs’ α = 0.91) [23], has a strong positive correlation with the original scale (r = 0.96) [23], and has been shown to have validity [23]. Each student was asked to respond on a five-point Likert scale. The IUS was further analyzed on the basis of two separate factors, namely prospective anxiety (items 1–7) and inhibitory anxiety (items 8–12). Prospective anxiety relates to items on the scale which represent an active approach to uncertainty in that it motivates an individual to seek sufficient information to increase predictability. Inhibitory anxiety refers to the sense of feeling paralyzed or unable to function when faced with uncertainty [25].
This study was granted ethical approval by the NUIGalway Research Ethics committee.
Statistical analysis was performed using the Statistical Package for Social Sciences 18.0 for Windows (SPSS Inc., Chicago, IL, USA). The student t test for parametric data and the Chi-square (χ 2) test for non-parametric data were employed. All statistical tests were two-sided, and the α-level for statistical significance was 0.05.
The internal consistency of each of the rating scales was determined by calculating a Cronbachs’ alpha.
Results
A sample size of 100 participants was obtained for this study, giving a response rate of 81.3 %. Seventy percent of the study population was female and 30 % was male. Ninety-one percent of female students (n = 77) participated compared to 65 % of male students (n = 46). Seventy percent of students were Irish, 15 % were Malaysian, and 4 % were North American. Eighty-two percent of students were aged from 22 to 25.
Twenty-seven percent (n = 27) of students met the criteria for psychological morbidity (i.e., caseness), as defined by a score of >3 on the GHQ-12 scale. Associations with psychological distress as determined by GHQ-12 caseness are shown in Table 1.
Those students who met the criteria for GHQ caseness had significantly elevated mean inhibitory anxiety scores (mean = 13.70, SD = 3.5) compared to those who did not meet the criteria for GHQ caseness (mean = 10.6, SD = 2.9) (t (98) = −4.51, p < 0.001). There was no significant difference between mean prospective anxiety scores for those who met the criteria for GHQ caseness (mean = 19.08, SD = 3.45) and for those who did not meet the criteria for GHQ caseness (mean = 18.01, SD = 3.1) (t (98) = −1.473, p = 0.144).
There was a high internal consistency on the IUS with a Cronbachs’ alpha of 0.83 demonstrated. The TAS showed a moderate degree of internal consistency with a Cronbachs’ alpha of 0.60. As expected, the IUS had a significant positive correlation with the TAS (r = 0.362, p < 0.001).
The mean GHQ-12 score was 12.5 (SD = 4.80). The mean TAS score was 41.01 (SD = 6.7), and the mean IUS score was 28.83 (SD = 7.37). Associations between the mean TAS and IUS scale scores and demographic correlates are shown in Table 2.
Discussion
The central finding of this study is that 27 % of 4th year medical students demonstrated psychological distress and that a heightened intolerance of uncertainty was associated with psychological distress. A similar level of psychological distress in medical students has been demonstrated in other studies [6], with a comparable rate of 30 % found among 4th year medical students in one [26]. This compares to rates of psychological distress of 28 % in public health workers and contrasts with rates of 18 % in the general population [21] as measured by the GHQ. There were significantly elevated levels of psychological distress in the female student population which has been mirrored in other studies [1, 2].
The significant association between psychological distress and a higher intolerance of uncertainty is a finding which has not been widely assessed for or identified in other studies. Intolerance of uncertainty cannot be considered an adaptive response, and individuals who demonstrate it will worry about how things may turn out, regardless of how they are at the present time, and this may predispose them to worry and distress. Increased distress from uncertainty was higher in students of Asian ethnicity; and again, it is a finding that has not been widely reported or demonstrated consistently in other studies. This should act to provide further impetus to aid this group of students who may find the academic environment already stressful due to the added complexities of the acculturation process to which they are exposed [27].
Inhibitory anxiety was identified as a factor which was associated with psychological distress. It is proposed that this uncertainty paralysis factor represents a sense of feeling unable to act when faced with uncertainty, due to active cognitive avoidance, confounded by difficulties in problem solving [25]. From a medical education and practice perspective, this may be understandable, in that inexperienced medical students require more information before making decisions in ambiguous clinical situations. However, when they are intolerant of uncertainty, they will have even less confidence in their decisions in ambiguous situations, resulting in prolonged anxiety and worry about the implications of their decisions [28]. This intolerance of uncertainty may have further consequences for medical students as it is likely to lead to difficulty in applying problem-solving skills when in uncertain situations, which may lead the individual to feel “stuck” in the uncertainty and unable to move forward.
Students who were older had a higher tolerance of ambiguity than younger students, which is a finding that has been shown in a previous study [29]. This would be expected as older students are likely to be more mature, less conforming and authoritarian, and therefore more likely to have a higher tolerance for ambiguity [19]. This is an encouraging finding in our study, because as students’ age further and move into the clinical realm of their training and away from the more theoretically based pre-clinical years of their education, they encounter patients with novel and complex medical issues. It has been demonstrated that in their adaptation to the increased stress and ambiguity in dealing with more complex patients, students who were more intolerant of ambiguity were found to develop more negative attitudes towards the patients and to experience more stress [22]. Further, intolerance of uncertainty and ambiguity in medical students can have significant implications not only for career choice, with such students preferring more technically focused specialties, such as surgery and radiology [19, 30] but also in their reluctance to look after geriatric and psychiatric patients [31].
The study used a cross-sectional survey design and, as such, does not purport to establish a causal relationship between intolerance of uncertainty and psychological distress. However, the association between psychological distress and intolerance for uncertainty was strong, and it is therefore important that our study is repeated in other student populations. In keeping with the ethical submission for this project, we did not look for information on the current or past psychological history of participants. The low response rate in this study from male students in comparison to females may have been a cofounding factor, as female medical students have previously demonstrated higher levels of distress [1]. We are aware that participant’s mental state at the time of completing questionnaires may have been an important influencing factor in some of their responses to the intolerance of uncertainty and tolerance of ambiguity questionnaires. This may have acted as a confounding factor, as someone who is actively depressed, for example, may display different degrees of tolerance of uncertainty or ambiguity to someone who is anxious or who is highly distressed but without evidence of a clinical disorder. However, this and the bidirectionality between an intolerance of uncertainty and specific mental disorders such as depression and anxiety have not been previously investigated [3], and an investigation of this was beyond the scope of this particular study.
Students who are affected by emotional disturbance due to a high intolerance of uncertainty are more likely to engage in mechanisms to off-set the uncertainty with which they are faced in their studies and future field of practice. If they occur during medical education in order to relieve stress levels, they are likely to continue into their practicing careers and will have important implications for their medical practice, with an intolerance of uncertainty shown to be associated with changes in practice behavior such as excessive investigation [10], over prescribing, and increased rates of hospital admission [32].
There are a number of quantitative and qualitative techniques which are taught and can be utilized in managing uncertainty. These include shared decision-making, meticulous history taking and evaluation, exclusion of worrisome diagnosis, an ability to critically appraise current literature, and the establishment of trust with the patient [30].
The psychological distress which is associated with an intolerance of uncertainty has consequences not only for the physical and mental well-being of students but will also have a detrimental impact on their ability to perform well academically. Medical educators need to communicate more effectively with students when diagnostic uncertainty exists. There is a need to directly acknowledge the uncertainty inherent in clinical practice and the stress which it may cause, in order to diminish the potential for student distress, but also to provide clear structures for collaborative attempts to be initiated to better cope with uncertainty in medical curriculum.
Implications for Educators |
• Twenty seven percent of medical students met the criteria for psychological distress, a level comparable to that identified in previous studies. |
• An intolerance of uncertainty was a significant predictor of psychological distress in this cohort of medical students. |
• This intolerance of uncertainty may have consequences for medical students as it is likely to lead to difficulties in applying problem solving skills and decision making when in uncertain situations. |
• Limitations to this study include a small sample size, a single university setting, the low response rate from male students and the lack of a prospective study design. |
• Additional studies to validate the study findings in larger samples should be pursued, before specific educational interventions can be recommended. |
ᅟ
Implications for Academic Leaders |
• Uncertainty in medical practice and education is an area which merits further study and attention. |
• Given that this single centre study identifies an association between a reduced tolerance for uncertainty and psychological morbidity, replication studies should be pursued in other medical schools. |
• Studies are required to examine techniques to reduce uncertainty in clinical education. |
• Prospective studies are needed to explore further the causal relationship between uncertainty and psychological distress in medical students. |
References
Dyrbye LN, Thomas MR, Shanafelt TD. Systematic review of depression, anxiety, and other indicators of psychological distress among U.S. and Canadian medical students. Acad Med. 2006;81(4):354–73.
Dahlin M, Joneborg N, Runeson B. Stress and depression among medical students: a cross-sectional study. Med Educ. 2005;39(6):594–604.
Baykan Z, Naçar M, Çetinkaya F. Depression, anxiety, and stress among last-year students at Erciyes University Medical School. Acad Psychiatry. 2012;36(1):64–5.
Young C, Fang D, Golshan S, Moutier C, Zisook S. Burnout in premedical undergraduate students. Acad Psychiatry. 2012;36(1):11–6.
Moffat KJ, McConnachie A, Ross S, Morrison JM. First year medical student stress and coping in a problem-based learning medical curriculum. Med Educ. 2004;38(5):482–91.
Guthrie EA, Black D, Shaw CM, Hamilton J, Creed FH, Tomenson B. Embarking upon a medical career: psychological morbidity in first year medical students. Med Educ. 1995;29(5):337–41.
Atkinson P. Training for certainty. Soc Sci Med. 1984;19(9):949–56.
Fox R. Training for certainty. In: Merton R, Reader G, Kendall P, editors. The student–physician: introductory studies in the sociology of medical education. Cambridge: Harvard University Press; 1980.
Coles C. Uncertainty in a world of regulation. Adv Psychiatr Treat. 2006;12(6):397–401.
Kassirer JP. Our stubborn quest for diagnostic certainty. A cause of excessive testing. N Engl J Med. 1989;320(22):1489–91.
Hall KH. Reviewing intuitive decision-making and uncertainty: the implications for medical education. Med Educ. 2002;36(3):216–24.
Beresford EB. Uncertainty and the shaping of medical decisions. Hastings Cent Rep. 1991;21(4):6–11.
Budner S. Intolerance of ambiguity as a personality variable. J Pers. 1962;30:29–50.
Grenier S, Barrette A-M, Ladouceur R. Intolerance of uncertainty and intolerance of ambiguity: similarities and differences. Personal Individ Differ. 2005;39(3):593–600.
Dugas MJ, Gosselin P, Ladouceur R. Intolerance of uncertainty and worry: investigating specificity in a nonclinical sample. Cogn Ther Res. 2001;25(5):551–8.
Gentes EL, Ruscio AM. A meta-analysis of the relation of intolerance of uncertainty to symptoms of generalized anxiety disorder, major depressive disorder, and obsessive-compulsive disorder. Clin Psychol Rev. 2011;31(6):923–33.
Goldberg D, Williams P. A user’s guide to the general health questionnaire. Windsor: NFER-Nelson; 1991.
Goldberg DP, Gater R, Sartorius N, Ustun TB, Piccinelli M, Gureje O, et al. The validity of two versions of the GHQ in the WHO study of mental illness in general health care. Psychol Med. 1997;27(1):191–7.
Geller G, Faden RR, Levine DM. Tolerance for ambiguity among medical students: implications for their selection, training and practice. Soc Sci Med. 1990;31(5):619–24.
Sobal J, DeForge BR. Reliability of Budner’s Intolerance of Ambiguity Scale in medical students. Psychol Rep. 1992;71(1):15–8.
Benjamin A, Riggio R, Mayes B. Reliability and factor structure of Budner’s Tolerance for Ambiguity Scale. J Soc Behav Pers. 1996;11:625–32.
Wayne S, Dellmore D, Serna L, Jerabek R, Timm C, Kalishman S. The association between intolerance of ambiguity and decline in medical students’ attitudes toward the underserved. Acad Med. 2011;86(7):877–82.
Carleton RN, Norton MAPJ, Asmundson GJG. Fearing the unknown: a short version of the Intolerance of Uncertainty Scale. J Anxiety Disord. 2007;21(1):105–17.
Freeston MH, Rhéaume J, Letarte H, Dugas MJ, Ladouceur R. Why do people worry? Personal Individ Differ. 1994;17(6):791–802.
Birrell J, Meares K, Wilkinson A, Freeston M. Toward a definition of intolerance of uncertainty: a review of factor analytical studies of the Intolerance of Uncertainty Scale. Clin Psychol Rev. 2011;31(7):1198–208.
Guthrie E, Black D, Bagalkote H, Shaw C, Campbell M, Creed F. Psychological stress and burnout in medical students: a five-year prospective longitudinal study. J R Soc Med. 1998;91(5):237–43.
Kalra G, Bhugra DK, Shah N. Identifying and addressing stresses in international medical graduates. Acad Psychiatry. 2012;36(4):323–9.
Dugas MJ, Robichaud M. Cognitive-behavioral treatment for generalized anxiety disorder: from science to practice. Routledge: Chapman & Hall; 2007.
DeForge BR, Sobal J. Intolerance of ambiguity in students entering medical school. Soc Sci Med. 1989;28(8):869–74.
Ghosh AK. Understanding medical uncertainty: a primer for physicians. J Assoc Physicians India. 2004;52:739–42.
Merrill JM, Camacho Z, Laux LF, Lorimor R, Thornby JI, Vallbona C. Uncertainties and ambiguities: measuring how medical students cope. Med Educ. 1994;28(4):316–22.
Firth-Cozens J. Medical student stress. Med Educ. 2001;35(1):6–7.
Disclosures
The authors have no competing conflict of interest to report.
Author information
Authors and Affiliations
Corresponding author
Electronic Supplementary Material
Below is the link to the electronic supplementary material.
ESM 1
(DOCX 44 kb)
Rights and permissions
About this article
Cite this article
Lally, J., Cantillon, P. Uncertainty and Ambiguity and Their Association with Psychological Distress in Medical Students. Acad Psychiatry 38, 339–344 (2014). https://doi.org/10.1007/s40596-014-0100-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40596-014-0100-4