
Abstract
Background
Aging is often accompanied by decline in aspects of cognitive function. Cognitive decline has harmful effects on living independence and general health. Resistance training is seen as a promising intervention to prevent or delay cognitive deterioration, yet the evidence from reviews is less consistent.
Aim
To assess the effect of resistance training on cognition in the elderly with and without mild cognitive impairment and to provide an up-to-date overview.
Methods
A search was conducted using PUBMED, Web of science, MEDLINE, CINAHL, Cochrane Library, EMBASE, Wan Fang, and China National Knowledge Infrastructure. The searches were limited to articles published in English or Chinese from January 2010 to September 2017.
Results
The search returned 2634 records, of which 12 articles were included in the systematic review. Main results showed that resistance training had positive effects on the executive function and global cognitive function of the elderly, and short-term interventions had little positive effect on memory and attention. Secondary results demonstrated that there was a significant benefit of triweekly resistance training in global cognitive function and biweekly in executive function of the elderly.
Conclusions
Resistance training had positive effects on the executive cognitive ability and global cognitive function among the elderly; however, it had a weak-positive impact on memory. No significant improvement was found in attention. Triweekly resistance training has a better effect on general cognitive ability than biweekly. Further studies are needed focusing on the development and application of resistance training among the elderly.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
Aging is a dynamic and progressive process with morphological, functional, biochemical and psychological changes [1] and also an unavoidable phenomenon of a human’s life [2]. Currently, the aging population has become a global problem. According to the World Health Organization, between 2015 and 2050, the number of people over the age of 60 globally has an expected increase from 900 million to 2 billion. With the growth of age, the environmental adaptive capacity, muscle strength and mass of the individual gradually decline [1, 3]. Similarly, the central nervous system (CNS) undergoes changes as people grow older, accompanied by cognitive decline in different aspects, especially attention, executive function and memory [4, 5]. The dependence of old people on others in doing daily activities increases due to the decline of different function systems [6]. These factors may affect the well-being and quality of life of the elderly. Evidence suggested that up to 22% of residents with mild cognitive impairment (MCI) could be restored to normal cognition through early proper intervention [7]. Therefore, it is necessary to pay close attention to cognitive decline of the elderly and early intervention.
Cognitive function is a major element of health-related quality of life in the elderly [8]. Currently, cognitive decline is one of the most serious health problems in the twenty-first century, which not only affects living independence and general health of the elderly [9] but also increases societal burdens. Therefore, alleviating neurocognitive decline among the elderly has become a hot issue around the world. Although drug intervention can effectively alleviate cognitive decline of the elderly, adverse reactions caused by drugs are still controversial [10]. Non-pharmacological interventions may serve to complement drug treatment. The effects of physical activity on cognitive function of the aged have been widely promoted. Previous study indicated that peripheral IGF-1 level was positively correlated with cognitive function of individual [11]. Exercise interventions stimulate the production of peripheral IGF-1 [9] and brain-derived neurotrophic factor (BDNF) [12], a protein of the neurotrophic family involved in the growth, differentiation, and survival of neurons, possibly contributing to improving cognitive function [13, 14].
Previous reviews on the effects of exercise on cognition have revealed that exercise, as a positive lifestyle, might alleviate or delay cognitive decline [15]. Currently, the positive effect of aerobic exercise on cognitive function in older adults appears to be consistent [16]. A systematic review by Zheng et al. [17] showed that aerobic exercise could improve global cognitive ability and had positive effect on memory in people with MCI. A meta-analysis demonstrated that combination of aerobic and resistance training (RT) had a greater effect on cognition than aerobic exercise alone [18]. Therefore, RT may be an important component of exercise programs designed to improve health and cognition [19, 20]. Currently, RT has been confirmed to increase muscle mass, strength, cardiorespiratory capacity, energy expenditure, and body-muscle composition of the elderly. Studies have found that RT improved activities of daily living (ADL) and functional fitness of the healthy older adults or those institutional wheelchair-bound older adults with cognitive impairment [21]. RT may have a positive influence on reducing or preventing cognitive deterioration among the older adults [22, 23]. Some reviews suggested that RT may enhance specific cognitive performances in healthy older adults, while the effect of RT on executive function and memory is still controversial [24, 25]. Moreover, previous reviews only focused on the effects of RT on cognition among the healthy older adults, few took into account the effect of RT on cognition in the elderly with MCI. Since the last relevant review, more than 12 randomized controlled trials investigating the effect of RT on cognition in older adults with or without MCI have been published, underscoring the importance of this topic. Therefore, there is an opportunity to re-evaluate the evidence to date and to further investigate moderators of this effect, such as RT intensity and potential differences. This systematic review of randomized controlled trials seeks to clarify the discrepancies that were observed among recent published RCTs and outline the effects of RT on cognition in the elderly with and without MCI.
Methods
Eligibility criteria
This systematic review included studies that met the following criteria: (a) studies of individuals aged 55 years or older without moderate or severe cognitive impairment and other neurological (e.g., stroke) or mental illnesses (e.g., depression). (b) The study evaluated the effectiveness of resistance training on cognitive function of the elderly. (c) Participants in the control group only maintained their lifestyle as usual or carried out sham exercises (e.g., stretch and balance). (d) Cognitive functions including global cognitive ability, memory, language, attention, executive function or visuospatial ability were measured by cognitive tasks or neuropsychological assessments. (e) The study design must be randomized controlled trials. The articles were excluded if the title and abstract did not follow the inclusion criteria.
Literature search
Systematic searches were conducted according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [26] using the electronic databases PUBMED, Web of science, MEDLINE, CINAHL, Cochrane Library, EMBASE, Wan Fang, and China National Knowledge Infrastructure (CNKI). The databases were searched by either title or title and abstract. Search terms encompassed those related to Resistance Training [MeSH] (Training, Resistance OR Strength Training OR Training, Strength OR Weight-Lifting Strengthening Program OR Strengthening OR Program, Weight-Lifting OR Strengthening Programs, Weight-Lifting OR Weight Lifting Strengthening Program OR Weight-Lifting OR Strengthening Programs OR Weight-Lifting Exercise Program OR Exercise Program, Weight-Lifting OR Exercise Programs, Weight-Lifting OR Weight Lifting Exercise Program OR Weight-Lifting Exercise Programs OR Weight-Bearing Strengthening Program Strengthening Program, Weight-Bearing OR Strengthening Programs, Weight-Bearing OR Weight Bearing Strengthening Program OR Weight-Bearing Strengthening Programs OR Weight-Bearing Exercise Program OR Exercise Program, Weight-Bearing OR Exercise Programs, Weight-Bearing OR Weight Bearing Exercise Program OR Weight-Bearing Exercise Programs), Cognition [MeSH] (Cognitions OR Cognitive Function OR Cognitive Functions OR Function, Cognitive OR Functions, Cognitive), Aged [MeSH] (elderly) were combined with ‘AND’ and searched in ‘All Fields’. We hand-searched included papers’ reference lists and contacted all authors about other relevant studies. The searches were limited to articles published in English or Chinese from January 2010 to September 2017.
Study selection
All searched records were exported to EndNote. After removing duplicates, the studies were selected in two steps. First, two reviewers independently assessed the titles and abstracts of studies according to pre-defined inclusion criteria. In the process of evaluation, the reviewers need to discuss until reaching a consensus when disagreements arise. If the reviewers could not make a final decision according to the titles or abstracts, the full articles need to be assessed. Second, full texts selected were independently reviewed manually by two reviewers. Any disagreement in study selection was resolved by discussion with a third reviewer. PRISMA flow diagram provides detailed information about the screening process of studies.
Risk of bias in individual studies
The quality and level of evidence of 12 RCT studies were assessed by one reviewer and discussed with a second reviewer using the Cochrane Collaboration’s tool for assessing risk of bias for randomized controlled trials [27]. The risk of bias tool consists of six domains of bias: selection bias (random sequence generation, allocation concealment), performance bias (blinding of participants and personnel), detection bias (blinding of outcome assessment), attrition bias (incomplete outcome data), reporting bias (selective reporting), and other bias (anything else, ideally pre-specified). Each item was assigned a judgment of high, low, or unclear risk of material bias independently by two reviewers. When there are discrepancies in assessment between the two reviewers, the reviewers have to discuss. If needed, a third reviewer was involved.
Data extraction and analysis
Data were extracted by one reviewer using the prepared form and checked for accuracy by another reviewer. The following information was extracted from included articles: (a) publication (author, year, country of origin), (b) characteristics of participants (e.g., sample size, cognitive status), (c) the number of participants (enrollment and attrition), (d) experimental and control intervention, duration, frequency, intensity and style of resistance, (e) outcome measures of interest (primary and secondary measures), (f) and main findings. Where authors reported several measured timepoint in the whole intervention, only the first results after resistance intervention was admitted. The authors of the included study were contacted if more information was required. The domains of cognition considered in the included studies were global cognitive function, memory, executive function, and attention. Data extraction and analysis provided a descriptive summary and explanation of results by tables and text. Due to the variety of the research designs and results in the included studies, a narrative approach was applied to synthesize the findings to avoid increased heterogeneity [28]. Therefore, no meta-analysis was performed due to the heterogeneity of study designs and outcomes.
Results
Search results
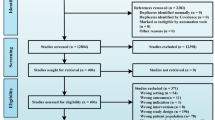
The result of the literature search is 2634 potentially relevant studies. After removing duplicates (N = 1176), 1458 studies remained, which were screened for title and abstracts, leading to exclusion of 1416 studies, potentially relevant 42 full-text articles were reviewed. Finally, 12 articles met the inclusion criteria for this systematic review. Detailed information on the process of search is provided in Fig. 1.

Literature search flow diagram
Characteristics of included studies
The characteristics of these included studies are summarized and available in Table 1. The review included 12 RCT articles, of which 2 articles reported the same trial [29, 30]. Twelve RCTs involved 748 participants, including 126 males and 495 females, excluding 1 study that did not report the gender [31] and 2 studies that reported the gender after the intervention [32, 33]. Four examined the effect of RT on cognitive function in patients with MCI [34,35,36,37], and five in patients with healthy older adults [29,30,31,32, 38], three in older adults with or without MCI [33, 39, 40]. The sample size of participants which completed exercise intervention in included studies ranged from 25 to 155. The mean age of participants varied from 55 to 80 years, excluding two studies that did not report the mean age of participants. All of included studies reported inclusion and exclusion criteria of selecting participants.
The types of RT in the included studies were diverse. The commonly used types were free weight training [29,30,31,32, 35,36,37,38,39,40], elastic band training [33, 34] and dumbbells barbells training [39]. The frequency of RT varied from 1 to 3 training sessions weekly and 30–100 min per session; Percentage of 1-RM (%1-RM) was used to prescribe intensity which ranged from 30 to 100% of 1-RM. Regarding RT volume, six studies used two sets of 6–15 repetitions, and four studies used three sets of 6–15 repetitions. The duration of the intervention was from 6 weeks to 1 year. Among 12 included studies, 5 studies were non-exercise in the control group [30,31,32,33, 40], 5 studies compared RT with Balance and Tone program (BAT) [29, 30, 34,35,36], other studies compared RT with health education [38] or stretching [37]; these activities in the control group did not differ from non-intervention.
Risk of bias
The risk of bias of included studies is summarized in Fig. 2. All included studies reported randomization allocation, but only three of which described the method of randomization sequence generation [29, 39, 40]. If included studies did not describe method of randomization or allocation concealment detail information and were judged as having ‘unclear’ risk of bias for these domains. Seven included studies were judged as having ‘high’ risk of bias because they were neither practical nor possible to blind the participants and therapists [31,32,33,34,35, 39, 40]. Three studies were assessed as low risk for bias because of blinding the outcome assessors [29, 30, 39]. Furthermore, the risk of attrition bias was unclear in two studies because studies did not describe intention-to-treat principles in the data analysis or the reasons of dropouts [36, 37]. Four studies were assessed as ‘unclear’ risk for selective reporting due to the insufficient information [31,32,33, 36].

Risk of bias summary: review authors’ judgements about each risk of bias item for each included study
Main analysis: effect of interventions
Cognitive function outcomes are presented in Table2.
Global cognitive function
Four of included studies reported the effects of RT on global cognitive function among the elderly measured using Mini–Mental State Examination (MMSE) [34], Assessment Scale-cognitive subscale (ADAS-Cog) [37], Korean version of Montreal Cognitive Assessment (K-MoCA) [33, 34], and Montreal Cognitive Assessment (MoCA) [39]. There was heterogeneity between the studies based on study design and outcome measures used. Three studies reported significant positive effects of RT on cognition of the elderly [34, 37, 39]. The study by Smolarek et al. indicated that the RT group showed significant increases in cognitive capacity (F = 3.02, P < 0.05) after 12 weeks [39]. Mavros et al. [37] compared the effects of RT and sham-exercise training on cognitive function of older adults with MCI using double-blind randomized controlled experiment. After 6 months, the difference in the change of ADAS-Cog scores between the RT group and sham-exercise group was statistically significant (P = 0.046). The results indicated that RT can significantly improve global cognitive function of older adults. Yoon et al. [34] reported that cognitive function of the elderly with MCI in the high-speed RT group and low-speed group has significant improvement compared with that before 12-week intervention. However, the control group showed a significant decrease in MMSE score after 12-week. The result demonstrated that high-speed RT had better effects on cognitive performance of the older women with MCI than low-speed RT, although both programs were effective in enhancing cognition. Hong et al. [33] evaluated the effect of RT on cognitive function of the subjects with or without MCI, which has not observed significant differences after 12 weeks.
Memory
The effects of RT on memory measured by Rey 15-Item Memory Test (R15) [33], Logical Memory [37], Memorizing face-scene pairs [36], Verbal Learning Test (VLT) [30] were evaluated in four studies. Nagamatsu et al. [36] evaluated the effects of 6-month RT on memory of the seniors using a single-blind randomized controlled trial. The change of scores from baseline to trial completion for outcome measures were provided in the results, which suggested that compared with BAT, RT significantly improved the associate memory of the elderly with MCI (P = 0.03) after 6-month intervention. The results of study revealed that biweekly RT enhanced long-term memory of the healthy older adults at 2-year follow-up, but this effect was not evident (e.g., 12 months) [30]. In addition, there was no significant positive effect on memory in once-weekly RT group at post-intervention and 2-year follow-up [30]. Hong et al. [33] reported the effects of RT on memory in participants with or without MCI measured using the Rey 15-Item Memory Test (tests of short-term and recognition memory). There was no significant difference between RT and control group in older adults with or without MCI (P > 0.05). The findings reported by Mavros et al. [37] indicated that 6-month RT had no significant effect on the memory domain of the elderly with MCI (P = 0.88).
Executive function
Executive function is a higher order cognitive function that controls basic, underlying cognitive functions for purposeful and goal-directed behavior, involving planning, scheduling, working memory, interference control and task coordination [41, 42]. Stroop Test [29, 30, 32, 35, 36, 40], Trial Making Tests (TMT) [36], Verbal Digits Test (VDT) [36], Digit Span Test [33], Task-Switch Test [38], Wechsler Adult Intelligence(WAIS)-III, Controlled Oral Word Association Test (COWAT), Category fluency [37] were used to assess the executive function. The Stroop Test, consisting of conditions of increasing difficulty, is used to assess a number of executive function components, including selective attention, the ability to shift response/perceptual sets and the ability to inhibit habitual responses [43].
Nine of the included studies reported the effects of RT on executive function of the elderly [29, 30, 32, 33, 35,36,37,38, 40]. Significant benefits were observed for executive function in six studies. Davis et al. [35] reported that RT significantly improved executive function measured by the Stroop Test (P = 0.04) of the elderly with MCI after 6 months. The single-blinded study by Nagamatsu et al. [36] showed that RT had significant positive effects on selective attention and conflict resolution in executive function measured by the Stroop Test in the elderly with MCI. However, no positive effect on set shifting and working memory were observed measured using TMT and VDT, respectively, in the elderly with MCI. Hong et al. [33] reported the effects of RT on working memory in participants with or without MCI measured using the Digit Span Test (the Digit Span Forward (DF) Test and Digit Span Backward (DB) Test). The scores on the DB Test suggested that RT was beneficial to slow the decline of working memory in the elderly with MCI after 12-week intervention. No effect of the intervention was found with regard to working memory in healthy volunteer groups after 12-week. Coetsee et al. [32] reported the effects of RT on executive function measured using Stroop Neutral, Stroop incongruent task and Stroop interference task in healthy participants. The results demonstrated that compared with control group, RT was proved to be better for the enhancement of older individuals’ executive function (P < 0.05). Previous studies indicated that compared with BAT group, once-weekly or biweekly RT had a significantly positive effect on selective attention and conflict resolution measured by the Stroop Test among the healthy older adults after 12-month intervention [29, 30], and the positive impact of once-weekly or biweekly RT persisted at the 2-year follow-up [30], which suggested that RT might have long-term impacts on executive function. However, the results of studies also showed that RT had no positive influence on set shifting and working memory at trial completion.
Among nine studies, three reported no significant effects of RT on executive function. Mavros et al. [37] reported that there was a tendency to improve executive function of the elderly with MCI in RT group. The study reported by Iuliano et al. [40] demonstrated that RT was not effective in improving executive function of the elderly with or without MCI measured by the Stroop Test. A single-blind RCT by Kimura et al. [38] indicated that there was no significant change in the reaction time and correct response rate measured using Task-Switch Test in healthy older adults after 12-week RT.
Attention
Three studies assessed the effects of RT on attention of the subjects, and both results show that there is no significant positive impact [33, 40]. Two studies examined the effect of 12 weeks of RT on the cognition of the elderly with or without MCI. The results indicated that RT did not significantly improve in attention as measured by the Attentive Matrices Test (AMT) [40] or Digit Span Test (DST) [33]. Similarly, Mavros et al. [37] evaluated 6-month RT on cognitive function among the elderly with MCI and found no significant positive changes in attention measured using Symbol Digit Modalities Test (SDMT) after 6 months.
Secondary analysis
Types of resistance training
Ten studies examined the effect of free weights training on cognitive function of the elderly. The results of five studies indicated that RT was beneficial to improve the executive function of the elderly [29, 30, 32, 35, 36]. One study reported that there was a tendency to improve the executive function of the subjects with MCI in the RT group [37]. The results demonstrated no significant changes in the executive function of the participants in the RT group [38, 40]. Two studies indicated that RT could significantly improve global cognitive function of older adults [37, 39]. The results of three studies demonstrated that RT had no significant effect on the memory of the elderly. Two studies indicated that RT significantly improved memory of the elderly [30, 36]. Fragala et al. [31] reported that RT may improve spatial awareness and visual and physical reaction time of the elderly. Two studies examined the effect of elastic band training on cognitive function in the subjects [33, 34]. Yoon et al. [34] showed that elastic band training significantly improved global cognitive ability. Hong et al. [33] demonstrated that it had no significant effect on global cognitive ability and attention of the subjects, but the working memory decline was delayed.
Frequency of resistance training
Eight studies examined the effect of biweekly RT on cognitive function [29,30,31, 33,34,35,36, 38]. Only one of the seven studies confirmed a significant benefit of RT on the general cognitive function [34]; three studies reported that RT promoted executive function of the elderly [30, 35, 36], while one study reported no significant positive effect on executive function [38]; two studies confirmed the positive effect of RT on memory [30, 36]; and one study observed no significant relationship between RT and any of the domains assessed (attention and memory) [33]. Three studies containing 170 participants examined the effect of triweekly RT on cognitive function in the elderly [32, 37, 39]. Two of three studies reported positive effect of RT on global cognitive function of the elderly [37, 39], and a tendency to improve executive function of older adults with MCI [37]; the other study reported that RT improved executive function of healthy older adults [32]. The results demonstrated that triweekly RT has a better effect on general cognitive ability than twice a week.
Discussion
This systematic review examined the effect of different implementation types, frequency and intensity of RT on the cognitive function of the elderly. Significant positive effects of RT on cognition were found in 8 of the 12 included studies, the relationship being most consistent for executive function, intermediate for global cognitive function and weak for memory. No significant improvement was found in attention. Few adverse events related to RT were reported in the included studies. Based on positive results, supervised RT may be a safe physical intervention in older adults to prevent cognitive decline.
Our review supported that RT had inconsistent effect on the general cognition of the elderly. Three of the included studies reported a significant positive association between RT and general cognition of the elderly [34, 37, 39]. One of the included studies showed that RT had no significant impact on general cognition [33]. Previously, studies demonstrated that RT could promote vascularization (both chronic and acute) throughout the body and enhance essential nutrient supply to the brain. Regular RT is a non-pharmacological intervention that is beneficial to the cardiovascular and cognitive function of the elderly [9, 22]. It is plausible that the size of the population in the study and the intensity of intervention were inadequate to show unequivocal changes in cognition. In addition, modest variation in general function may be due to the gender difference of the participants [44], and women’s executive processes may benefit more than men [45]. Further studies should be directed toward identification of potential mechanisms linking adaptations in gender and cognitive function after RT.
Among the included studies, two reported an improvement in memory. Nagamatsu et al. [36] reported that 6-month RT improved the associate memory of the elderly with MCI. Best et al. [30] revealed that RT could significantly improve verbal memory in healthy older adults at 2-year follow-up, the findings were consistent with the results of previous study that RT had long-term positive effect on memory [23] and also confirmed the hypothesis which RT might prevent cognitive decline involving homocysteine [46]. High homocysteine level, identified as a risk factor for cognitive impairment, may decrease performances in tests of immediate and delayed memory in older adults [47, 48]. The peripheral insulin-like growth factor-1 (IGF-1) level was positively correlated with the cognitive function of the elderly [49], and studies showed that RT could improve the hippocampus-dependent memory task with a concomitant increase of IGF-1 level [22, 50]. However, RT were not found to have a positive effect on memory in the other two studies [33, 37]. It is plausible that the duration of the intervention is too short to cause significant positive effects. As such, appropriate intervention duration could confirm more effectively the specific causal relationships.
In included studies, three showed that 12-week RT had no significant positive effect on attention of the elderly [33, 37, 40]. It is possible that the null results were due to the brief period of intervention and the small sample size [51]. Previous studies have shown that some loss of attention, especially vigilance and spatial attention, may be considered a normal part of the aging process and evolved into more serious cognitive impairment [52, 53]. There were only three studies related to the effect of RT on attention and may be insufficient evidence. Future studies with larger sample sizes and high quality should examine the effect of RT on attention of the elderly.
This review found that RT was significantly beneficial to executive function of the elderly, which is inconsistent with the results of previous review [24]. Six of the included studies reported that long-term (> 16 weeks) RT has been shown to be effective in improving executive function of the elderly significantly [29, 30, 32, 33, 35,36,37], especially selective attention and conflict resolution. Among the studies, one demonstrated RT could delay the decline of working memory in the subjects with MCI [33], three reported RT did not improve working memory for the elderly [29, 30, 36]. The results revealed that the benefits of RT on working memory may be more potent among those at greater risk for cognitive impairment. Two of the included studies found that short-term (≤ 12 weeks) RT had no significant improvement on executive function between groups [38, 40]. The findings indicated that duration and dose–response may influence the effect of intervention [54]. In addition, an important point of difference for the included studies finding significant positive associations between RT and executive function was the diverse measurement of executive function. Future RCTs should not be limited to the effectiveness of the intervention, but should improve the prescription of intervention to promote the greatest benefit of cognitive function in the old adults.
The major strengths of this review are that it provides an up-to-date summary of RCTs of RT for cognitive function among the elderly with and without MCI and the detailed analysis of data about intervention content. Not only did we explore the effects of the prescription of interventions on cognitive functions of older adults, but also focus on the effects of different types of RT on cognition. Despite this, there are limitations that must be considered. First, only three studies assessed the effects of RT on attention. Due to the small number of studies, the effect of RT on attention need more evidences. Second, exclusion of studies in languages other than English and Chinese may have led to some relevant studies not being identified, which may be a language bias in this review. Third, the wide variety of cognitive tests militates against comparison between studies. In the 12 included studies, a total of 19 different tests were used to assess cognition. In addition, it is difficult to blind participants in an RT intervention trial; therefore, the performance bias of the included studies may be inevitable.
Conclusions
The findings of this systematic review support that RT is beneficial to improve global cognitive function and executive function of the older adults, whereas RT has a weak-positive impact on the memory domain. No significant improvement was found in attention. The studies showed differences in the types, frequencies and durations of interventions, as well as the limitations in the small sample size of included studies. In the future, high-quality RCTs with larger sample sizes based on a rigorous methodology need to confirm the effect of RT on working memory and attention of the elderly, which are important both scientifically and clinically.
Practical implications
Optimizing cognitive function would contribute positively to improve the quality of life of the elderly, reduce the occurrence of dementia, and alleviate the social and family burden. This systematic review provides clinicians with encouraging evidence that RT enhance some aspects of cognitive function in older adults with or without MCI. Moreover, the review suggests that different training intensity, with realistic frequency and duration of training, produces virtually no adverse effects and RT could be a feasible intervention for the elderly with and without MCI. Evidence of the relationship between RT and cognitive function among the elderly would further support advocacy initiatives for promoting RT in the elderly. Further studies should examine a variety of clinical cohorts using both objective and subjective measures to confirm the efficacy of RT on cognition.
References
Cummings SR (2007) The biology of aging. J Musculoskelet Neuronal Interact 7:340–341
Leger D et al (2008) An international survey of sleeping problems in the general population. Curr Med Res Opin 24:307–317
Roubenoff R (2000) Sarcopenia and its implications for the elderly. Eur J Clin Nutr 54:S40–S47
Carlson MC et al (2009) Executive decline and dysfunction precedes declines in memory: the Women’s Health and Aging Study II. J Gerontol A Biol Sci Med Sci 64:110–117
van Dam PS, Aleman A (2004) Insulin-like growth factor-I, cognition and brain aging. Eur J Pharmacol 490:87–95
Karimi S et al (2016) Surveying the effects of an exercise program on the sleep quality of elderly males. Clin Interv Aging 11:997–1002
Ganguli M et al (2004) Mild cognitive impairment, amnestic type: an epidemiologic study. Neurology 63:115–121
Lox CL et al (2006) The psychology of exercise; integrating theory and practice, 2nd edn. Ringgold
Tsai CL et al (2015) The effects of long-term resistance exercise on the relationship between neurocognitive performance and GH, IGF-1, and homocysteine levels in the elderly. Front Behav Neurosci 9:23
Doody RS et al (2009) Donepezil treatment of patients with MCI: a 48-week randomized, placebo-controlled trial. Neurology 72:1555–1561
Dik MG et al (2003) Insulin-like growth factor I (IGF-I) and cognitive decline in older persons. Neurobiol Aging 24:573–581
Gligoroska JP, Manchevska S (2012) The effect of physical activity on cognition—physiological mechanisms. Mater Sociomed 24:198–202
Erickson KI et al (2011) Exercise training increases size of hippocampus and improves memory. Proc Natl Acad Sci USA 108:3017–3022
Tolwani RJ et al (2002) BDNF overexpression increases dendrite complexity in hippocampal dentate gyrus. Neuroscience 114:795–805
Northey JM et al (2018) Exercise interventions for cognitive function in adults older than 50: a systematic review with meta-analysis. Br J Sports Med 52:154–160
Cai H et al (2017) Effect of exercise on cognitive function in chronic disease patients: a meta-analysis and systematic review of randomized controlled trials. Clin Interv Aging 12:773–783
Zheng G et al (2016) Aerobic exercise ameliorates cognitive function in older adults with mild cognitive impairment: a systematic review and meta-analysis of randomised controlled trials. Br J Sports Med. https://doi.org/10.1136/bjsports-2015-095699
Colcombe S, Kramer AF (2003) Fitness effects on the cognitive function of older adults: a meta-analytic study. Psychol Sci 14:125–130
Williams MA et al (2007) Resistance exercise in individuals with and without cardiovascular disease: 2007 update: a scientific statement from the American Heart Association Council on Clinical Cardiology and Council on Nutrition, Physical Activity, and Metabolism. Circulation 116:572–584
Chang YK et al (2014) Effects of acute resistance exercise on cognition in late middle-aged adults: general or specific cognitive improvement? J Sci Med Sport 17:51–55
Chen M-C et al (2016) Elastic band exercises improved activities of daily living and functional fitness of wheelchair-bound older adults with cognitive impairment: a cluster randomized controlled trial. Am J Phys Med Rehabil 95:789–799
Cassilhas RC et al (2007) The impact of resistance exercise on the cognitive function of the elderly. Med Sci Sports Exerc 39:1401–1407
Perrig-Chiello P et al (1998) The effects of resistance training on well-being and memory in elderly volunteers. Age Ageing 27:469–475
Chang YK et al (2012) Effect of resistance-exercise training on cognitive function in healthy older adults: a review. J Aging Phys Act 20:497–517
Saez de Asteasu, ML et al (2017) Role of physical exercise on cognitive function in healthy older adults: a systematic review of randomized clinical trials. Ageing Res Rev 37:117–134
Moher D et al (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med 151:264–269
Higgins JP et al (2011) The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 343:d5928
Higgins JPT, Green S (2011) Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, London
Liu-Ambrose T et al (2010) Resistance training and executive functions a 12-month randomized controlled trial. Arch Intern Med 170:170–178
Best JR et al (2015) Long-term effects of resistance exercise training on cognition and brain volume in older women: results from a randomized controlled trial. J Int Neuropsychol Soc 21:745–756
Fragala MS et al (2014) Resistance exercise may improve spatial awareness and visual reaction in older adults. J Strength Cond Res 28:2079–2087
Coetsee C, Terblanche E (2017) The effect of three different exercise training modalities on cognitive and physical function in a healthy older population. Eur Rev Aging Phys Act 14:13
Hong SG, Kim JH, Jun TW (2017) Effects of 12-week resistance exercise on electroencephalogram patterns and cognitive function in the elderly with mild cognitive impairment: a randomized controlled trial. Clin J Sport Med. https://doi.org/10.1097/JSM.0000000000000476
Yoon DH et al (2017) Effect of elastic band-based high-speed power training on cognitive function, physical performance and muscle strength in older women with mild cognitive impairment. Geriatr Gerontol Int 17:765–772
Davis JC et al (2013) An economic evaluation of resistance training and aerobic training versus balance and toning exercises in older adults with mild cognitive impairment. PLoS One 8:e63031
Nagamatsu LS et al (2012) Resistance training promotes cognitive and functional brain plasticity in seniors with probable mild cognitive impairment. Arch Intern Med 172:666–668
Mavros Y et al (2017) Mediation of cognitive function improvements by strength gains after resistance training in older adults with mild cognitive impairment: outcomes of the study of mental and resistance training. J Am Geriatr Soc 65:550–559
Kimura K et al (2010) The influence of short-term strength training on health-related quality of life and executive cognitive function. J Physiol Anthropol 29:95–101
Smolarek Ade C et al (2016) The effects of strength training on cognitive performance in elderly women. Clin Interv Aging 11:749–754
Iuliano E et al (2015) Effects of different types of physical activity on the cognitive functions and attention in older people: a randomized controlled study. Exp Gerontol 70:105–110
Etnier JL, Chang YK (2009) The effect of physical activity on executive function: a brief commentary on definitions, measurement issues, and the current state of the literature. J Sport Exerc Psychol 31:469–483
Lindwall M, Rennemark M, Berggren T (2008) Movement in mind: the relationship of exercise with cognitive status for older adults in the Swedish National Study on Aging and Care (SNAC). Aging Ment Health 12:212–220
Rivera D et al (2015) Stroop Color-Word Interference Test: normative data for the Latin American Spanish speaking adult population. NeuroRehabilitation 37:591–624
Al-Delaimy WK, von Muhlen D, Barrett-Connor E (2009) Insulin like growth factor-1, insulin like growth factor binding protein-1, and cognitive function in older men and women. J Am Geriatr Soc 57:1441–1446
Barha CK et al (2017) Sex differences in exercise efficacy to improve cognition: a systematic review and meta-analysis of randomized controlled trials in older humans. Front Neuroendocrinol 46:71–85
Liu-Ambrose T, Donaldson MG (2009) Exercise and cognition in older adults: is there a role for resistance training programmes? Br J Sports Med 43:25–27
Ford AH et al (2012) Homocysteine, methylenetetrahydrofolate reductase C677T polymorphism and cognitive impairment: the health in men study. Mol Psychiatry 17:559–566
Ford AH et al (2013) Homocysteine, depression and cognitive function in older adults. J Affect Disord 151:646–651
Aleman A et al (1999) Insulin-like growth factor-I and cognitive function in healthy older men. J Clin Endocrinol Metab 84:471–475
Cassilhas RC et al (2012) Resistance exercise improves hippocampus-dependent memory. Braz J Med Biol Res 45:1215–1220
Greblo Jurakic Z et al (2017) Effects of feedback-based balance and core resistance training vs. Pilates training on cognitive functions in older women with mild cognitive impairment: a pilot randomized controlled trial. Aging Clin Exp Res 29:1295–1298
McGaughy J, Eichenbaum H (2002) It’s time to pay attention to attention in aging. Learn Mem 9:151–152
Montero-Odasso M et al (2009) Quantitative gait analysis under dual-task in older people with mild cognitive impairment: a reliability study. J Neuroeng Rehabil 6:35
Chang YK, Etnier JL (2009) Exploring the dose-response relationship between resistance exercise intensity and cognitive function. J Sport Exerc Psychol 31:640–656
Funding
This research is funded by Natural Science Foundation of Jilin Province (20160101215JC).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed consent
For this type of study, formal consent is not required.
Rights and permissions
About this article

Cite this article
Li, Z., Peng, X., Xiang, W. et al. The effect of resistance training on cognitive function in the older adults: a systematic review of randomized clinical trials. Aging Clin Exp Res 30, 1259–1273 (2018). https://doi.org/10.1007/s40520-018-0998-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40520-018-0998-6