
Abstract
Background
Certain features of the social environment could maintain and even improve not only psychological well-being, but also health and cognition of the elderly.
Aims
We tested the association between social network characteristics and the number of chronic diseases in the elderly.
Methods
A randomized sample of the elderly population of Brescia, Italy, was evaluated (N = 200, age ≥65 years). We performed a comprehensive geriatric assessment, including information on socio-demographic variables (family, friendships, and acquaintance contacts). We measured each person’s social network, i.e., degree, efficiency, and variety.
Results
The sample included 118 women and 82 men, mean age 77.7 years. The mean number of chronic diseases was 3.5. A higher social network degree, i.e., more social connections, was associated with fewer diseases. We also found that having more contacts with people similar to each other or intense relationships with people who do not know each other were associated with fewer diseases.
Conclusion
More healthy people tend to share certain characteristics of social networks. Our study indicates that it is important to look at diseases and health as complex phenomena, which requires integrating different levels of analysis.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The number of elderly in the world has gradually increased from ten million in 1900 to 420 million in 2000. According to the latest estimates made by the United Nations Population Division, the elderly population will probably reach two billion by 2050 and they will account for about a fifth of world population [1]. According to the Italian National Institute of Statistics Data [2], people over 65 years, who now account for 20.8% of the country population, will reach 36.3% by 2050. This constitutes a population change without precedent in human history, which will have important social, economic, and cultural implications.
Income growth and progress in nutrition, education, sanitation, and medicine in advanced countries has increased life expectancy and improved general health conditions. Chronic diseases have replaced infectious diseases as the dominant health care burden, giving rise to the so-called “epidemiological transition” [3]. On the one hand, this implies that the majority of older people (ranging from 55 to 98%) are affected by multimorbidity, i.e., two or more co-occurring chronic diseases [4]. On the other hand, the minimization of the expected growth of health care and long-term care costs due to chronic diseases requires innovative primary and secondary prevention. This will also include checks for several risk factors as well as the impact of lifestyles and social contexts on health.
Research suggests that social support has a positive impact on health. For social support, we mean “everyday behaviors that, whether directly or indirectly, communicate to an individual that she or he is valued and cared for by others” [5]. According to Uchino [6], social support may have four functions: emotional (e.g., provision of affect, acceptance, encouragement, and trust [7]), informative (e.g., provision of advice and guidance), companionship (e.g., sense of belonging), and tangible (e.g., provision of financial assistance, material goods, or services). It may come from both social relationships or public institutions (e.g., care from governments or public institutions).
Here, it is important to note that given the recent reduction of public investments on healthcare not only in Italy [8], but also in many other countries [9], private forms of social support that come from a person’s social relationships are now of paramount importance. Indeed, according to the second European Quality of Life Survey, almost a quarter of adults in EU27 provide care of an older relative and about 8% do so on a daily basis [10]. In Italy, family is a key factor for elderly care [11]. Quattrini et al. [12] estimated that in Italy, about 11% of the over 50-year-old population provide care to an older relative, i.e., about 2,350,000 persons.
Furthermore, it is acknowledged that the social contexts in which the elderly live (e.g., the amount and the type of informal care provided by their family, friends, and contacts) may influence their lifestyles. However, there is still a need for a close examination of which features of these social contexts really do matter. For instance, while recent studies have examined health as a consequence of education, occupation, and income, only a few have thoroughly analyzed the impact of social networks on health in the elderly by looking at network characteristics. Social networks are social structures made up of a set of individuals connected through different ties, but they also have different characteristics which could have important implications for elderly status and behavior.
Indeed, it is probable that people with few social contacts, typically restricted to family members, may have little knowledge about healthy behavior, have problems in the self-management of chronic diseases and do not use preventive services sufficiently. It is well known, for instance, that social isolation is a major health problem among community-dwelling older adults, leading to numerous detrimental health conditions, including a higher risk of death [13]. In short, social isolation has serious implications for health, well-being, and quality of life for numerous older adults [14]. For instance, Mazzella et al. [15] looked at the effect of social support and comorbidity on 12-year mortality in a sample of 1332 elders from the “Osservatorio Geriatrico Regione Campania”, which was a cross-sectional study performed in 1992 in Campania, a Region in Southern Italy. Findings showed that higher mortality was associated with low social support of the elderly and that this effect was stronger in case of high levels of comorbidity.
Many studies have shown that a rich social network could maintain and even improve, not only psychological well-being, but also health and cognition at different ages [16, 17]. For instance, Rizzuto et al. [18] showed that the median survival of the elderly with a low risk profile (healthy lifestyle behavior, participation in at least one leisure activity, and a rich or moderate social network) was 5.4 years longer than those with a high risk profile (unhealthy lifestyle behavior, no participation in leisure activities, and a limited or poor social network). They found that this effect was similar even among the oldest subjects. Another Swedish study found significant associations between social capital and cause-specific mortality, including cancer and stroke in the elderly [19].
However, only an in-depth analysis that looks at the type of social contacts and resources that people have due to their social connections can help to examine the interplay of health and social life. Indeed, social networks can have positive consequences on individual health by facilitating access to health-enhancing services and amenities as well as via the psychological process of providing effective support [16]. Possible mechanisms explaining the association between a rich social network and better health include higher resilience and better neuro-endocrine responses to stress by the elderly [20]. The social environment can also trigger better lifestyles, such as physical activity, assistance when needed, cognitive and affective resources, not to mention access to relevant information for disease prevention [21–23].
However, it is still uncertain what are the advantage of specific links compared to others (e.g., spouses, children, and friendships) as well as that of the entire social network of the elderly. Social relationships are multi-faceted and different social network components can operate by different processes to influence well-being. For example, does a cohesive and closed family with strong affective relationships matter more than enjoying a large network of unrelated friends and acquaintances? If we consider the importance of information for prevention and how much people’s behavior is influenced by the exposure to the behavior of others, especially of relevant people, it is important to understand if people benefit more from having social contacts among similar or different kinds of people.
Answering these questions requires looking at each person’s social network in close detail, by measuring a subject’s connections on a micro scale, the characteristics of the contacts and the type of relationships they have. To do so, we constructed a prospective population-based study through a randomized sample of the elderly in Brescia, Italy. We performed a comprehensive geriatric assessment, including information on socio-demographic variables (family, friendship and acquaintance contacts) and measured each person’s social network through a list of questions that allowed us to comprehensively map the characteristics of ties and their mutual relationships. We measured the degree, efficiency, and variety of each person’s network (detail below), so that we could compare each person involved in the sample.
Older people who are more socially isolated could be penalized by lower access to relevant information, lower chances to self-regulate their lifestyles through social control offered by contacts, and lack of cognitive stimuli from participating in a vibrant social environment, e.g., connections with similarly educated friends. We wanted to verify whether a larger network of contacts, higher intensity of contacts, or a higher variety of social contacts in terms of education could be associated with fewer chronic diseases.
Methods
Study design
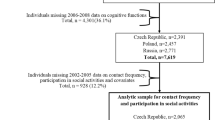
‘ANZIANI IN-RETE’ was designed as a prospective population-based study. A sample of 816 people was randomly selected by age cohort (from 65 to 74, from 75 to 84, and ≥85 years) and by gender. Subjects were living in three districts (Brescia Antica, Centro Storico Nord, and Centro Storico Sud) located in the city center of Brescia, Italy. We requested address contacts of eligible subjects from the municipal register. We sent a letter describing the study design and aims. We then contacted each eligible subject by phone to schedule an appointment for the examination. The examinations were performed at the subjects’ home or in the Geriatric Ward of the Spedali Civili, Brescia. Of the original 816 people invited to participate, 372 (45.5%) were not eligible (i.e., they had no phone contact information). Of the remaining 444, 15 (3.4%) died before the beginning of the study, and 8 (1.8%) moved their home residence. Among the remaining (421), 221 (52.4%) persons refused to participate, while 200 (47.5%) accepted. Of the latter, 167 had valid data on social networks (see Online Resource 1, Table S1). It is important to note that the sample included not only the data of 167 subjects but also information on their contacts, so that the whole sample actually included 964 persons and 1984 social ties.
Comparisons between the group with no contact information and those who were contacted showed no statistically significant differences according to mean age and gender. The same was true for those who accepted and those who refused to participate. The examination took place during a 5-month period (April 2014–August 2014). A written informed consent was obtained from all individual participants included in the study. All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008.
The study was approved by the Ethical committee of the Local Health Unit (ASL) of Brescia, Italy (reference number 0144116).
General objectives
The general aims of the study ‘ANZIANI IN-RETE’ were as follows: (1) to investigate somatic health, cognition, affective status, and functional domains of a sample of the elderly living in Brescia, Italy; (2) to map the social network of this sample; (3) to understand the relationship between social variables and global health status, and (4) to derive public policy principles to improve quality of social networks of the elderly as part of a health policy.
Data collection
Data collection consisted of a face-to-face, structured interview and a clinical examination. The whole process took about 1 h. The interviews were conducted by trained physicians using an online application on a tablet computer. Information was also collected on people living with the interviewee and caregivers. Previous medical reports and drug boxes were checked, if available. All data were collected by means of a structured questionnaire based on the domains of the InterRAI Home Care Assessment System (HC), a validated and standardized third-generation multi-dimensional evaluation tool developed by interRAI, a scientific international not-for-profit corporation [24]). We included the following indicators: health status number and category of chronic diseases, sensory impairments, number and type of prescribed drugs, presence of adverse events (i.e., falls, hospitalization, etc) during the previous 3 months, presence and characteristics of pain, skin conditions, and malnutrition. Furthermore, we also included functional, affective and cognitive status, adherence to screening and prevention programs, and life styles, such as smoking, alcohol, diet habits, and physical activity. Physical tests included basic anthropometry (body-mass index), measurement of blood pressure, and heart rate.
Social networks evaluation
By following a person’s (ego) network approach [e.g., 16–18], we mapped social networks of each individual interviewee (ego) by listing a set of questions that included important resources typically needed by the elderly and personal contacts that could help him/her access them [19, 20]. These included: (a) help in house work (e.g., gardening, wall painting, and moving furniture); (b) a lift to the pharmacy or municipality offices to run personal errands; (c) a loan of small amounts of cash for unforeseen personal expenses; (d) personal advice on health, affective or relational problems; (e) personal advice on savings, life insurance or pensions; (f) a place (a room, flat or house) to stay in case of need, due to house work or eviction [25]. The interviewee was asked to indicate the name and surname of each person (i.e., alter) to which he/she could ask for the resource needed, his/her alter’s status (i.e., family member, friend, or acquaintance) and the intensity of his/her relationship with his/her alter (i.e., the frequency of their encounters on daily, weekly, monthly, and yearly bases [26]). The interviewee was also asked to indicate whether each alter in his/her list of contacts knew each other. Finally, he/she was asked to provide the educational qualification of each contact (see Online Resource 2).
To understand the quality of the social network of each interviewee (i.e., ego), we first measured the network degree, i.e., the size of ego’s social network in terms of number of alters and the frequency with whom each ego usually met his/her alters. Second, we measured the network efficiency [27], i.e., a structural indicator that looks at inter-alter connectedness in each ego network. The principle here is that the more alters are connected with each other, the higher the probability that they come from the same social circle and so that they provide ego with similar information and experience. Vice versa, an efficient network is one in which ego’s alters are poorly connected with each other, and therefore, each one provides different informations and possibly heterogeneous new contacts for the ego. The network efficiency held values from zero (maximum connectedness between ego’s alters) to one (minimum connectedness between ego’s alters). Finally, we measured the network variety by considering the heterogeneity of the educational qualification of each ego’s alters. We considered the education heterogeneity as a proxy of the level of cognitive variety and stimuli that each ego had by being exposed to his/her alters. The assumption was that the higher the heterogeneity of the education profile of a person’s contacts, the higher the variety of stimuli a person was exposed to. We followed the heterogeneity index proposed by Blau [28], which holds values from zero (=minimum heterogeneity) to one (=maximum variety).
Figure 1a, b, c shows the different types of social networks that were detected in the sample. Figure 1a represents an example of a ‘closed’ social network: i.e., where almost each alter knew each other. While the presence of strong links may provide subjects with time, resources, and love shared by his/her contacts, this type of networks cannot guaranteed ego access to new information, because his/her alters tend to have similar information. Figure 1b shows an example of an ‘open’ social network: i.e., where the ego was the only common tie among his/her alters who did not know each other. While this type of networks is beneficial in allowing ego access to a variety of information and so ideally exploit different resources from different unrelated alters, they have poor affective value. Finally, Fig. 1c shows an example of a ‘mixed’ social network: i.e., where the ego had a network that included different kinds of links and so could balance access to a variety of information and affective components.

a Example of a ‘closed’ social network. b Example of an ‘open’ social network. c Example of a ‘mixed’ social network
Statistics
Regression models were run to measure the effect of social variables on the total number of diseases (GLM regression). We built a GLM regression model on the following variables: gender, age, marital status, network degree, network efficiency, education-level heterogeneity of ego’s alters, and frequency of ego’s relationship with his/her alters. To look at the association between network structure (i.e., network degree and efficiency) and the characteristics of the social ties (i.e., the intensity of relations and the heterogeneity of contacts), we included two interaction terms (see Table 2). Interaction effects allowed us to understand if the effect of a group of independent variables (i.e., network structure) on the total number of diseases varied as a function of a second group of independent variables (i.e., characteristics of the social ties). All p values <0.10 were considered significant. For the statistical analysis, we used the following software packages: Stata (version 12), E-Net (version 0.41), and R (version3.2.2).
Results
Comparisons of demographic characteristics showed that the mean age of the original randomized sample was 77.6 years (SD 8.4) vs. 77.7 years (SD 7.6) of those who accepted to participate (p = 0.860). The percentage of women in the original sample was 63.9 and 59.0% for those included (p = 0.202).
The sample included 118 women (59%) and 82 men (41%). The youngest participant was 66, while the oldest was 102 years; 40 (20%) participants were 85+ years. Ninety-seven participants (47.5%) were still married, while 53 (26.5%) were widows. The mean number of chronic diseases was 3.5, median 3, ranging from 0 (12 cases) to 11 (two cases). The most frequent diseases were as follows: hypertension (n = 108, 52.4%), malignancy (n = 41, 19.9%), diabetes (n = 24, 11.7%), hypothyroidism (n = 23, 11.2%), chronic obstructive pulmonary disease (n = 20, 9.7%), and stroke (n = 18, 8.7%).
Table 1 shows baseline characteristics of the whole sample and age groups.
Social network and number of chronic diseases
Table 2 shows a GLM regression model that considered the association between social network characteristics and the number of chronic diseases. While being older (75 or more years) was associated with a higher number of chronic diseases, a higher social network degree was associated with fewer chronic diseases. The higher the number of contacts in a person’s network, the lower the number of chronic diseases. This effect was moderated by network variety as higher network variety decreased the impact of the degree on chronic diseases. Network efficiency also had a significant impact on the number of chronic diseases. On the one hand, an efficient network with low intensity of relationships was associated with a high number of chronic diseases. However, having efficient networks with high intensity of the relationships was associated with less chronic diseases.
Discussion
Our findings show that some characteristics of social networks are associated with health in the elderly. This would confirm recent findings on networks and diseases by Li and Zhang [29] and Steptoe et al. [30] and suggest that the effect of social networks is significant also on chronic diseases [31]. In particular, we found that a higher social degree of network was associated with a lower number of chronic diseases. This effect was moderated by network variety, i.e., the higher the network variety, the lower the impact of the degree on the number of chronic diseases was. This would indicate that subjects benefit from more contacts, especially when these contacts are similar. Furthermore, network efficiency had a significant impact on the number of chronic diseases. On the one hand, having efficient networks, when the intensity of the relationships was low, was associated with more chronic diseases. On the other hand, we found fewer chronic diseases when persons had efficient networks and high intensity of the relationships. This would indicate the complex mix of effects that certain network characteristics have on the health of the elderly [32].
In general, similar to Rafnsson et al. [33], we found two combinations of positive network effects on our sample, that is more contacts similar to each other and more intense relationships between unrelated contacts. This meant that, on the one hand, certain social network characteristic could have more important effects. On the other hand, we also found that different combinations of network characteristics might trigger a similarly positive effect. For example, it seems beneficial to have a dense network of similar contacts for the elderly, which probably ensures close attention to symptoms, prevention and guaranteed help, or intense relationships with unrelated contacts, which probably ensures access to a high variety of information and cognitive stimuli (e.g., [34, 35]).
Strengths and limitations
The main limitations of this study are the cross-sectional analysis and the small sample size. Indeed, the small size of our sample could reflect a selection bias due to several reasons. While selection bias is hard to control in all research, whose samples depend on participant decision, obviously a larger sample could help to reduce it. Despite we cannot completely rule out that refusals were sicker than participants, the two groups did not differ by age, and thus, it is unlikely that they had a very different number of comorbidities which are strongly related to age. Our low rate could be explained by a variety of other different mechanisms, including the fact that not all subjects were prone to share data on their social networks. Finally, the sample is considerably large when we consider the typical sample of social network analysis. As regards to the association between social network and health variables, longitudinal data of the study will be analyzed as soon as available. On the other hand, the strength of our study lies in the fact that each person was evaluated by trained physicians, so that participants or their caregivers gave information directly.
Conclusions
Our study indicates that it is important to look at diseases and health as complex phenomena, which requires integrating different levels of analysis [36]. People do not live in isolation. It is not simply the social structure of how everyday life is embedded which has important consequences on cognitive stimuli, prevention, and lifestyles. Access to relevant information and learning by observing others’ behavior requires good social connections. It also potentially hosts important resources, e.g., emotive support, information, and relevant contacts that a complexity-friendly health policy should try to activate to protect old persons from diseases [37]. This is an important message as only a new alliance between medicine and social sciences can help develop policies that truly reflect the complexity of health and explore innovative ways to respond to the needs of an aging society.
References
P. D. United Nations, Department of Economic and Social Affairs (2015) World population prospects: the 2015 revision, key findings and advance tables, Work. Pap. No. ESA/P/WP.241
ISTAT (2014) Annuario statistico italiano 2014
Omran AR (1971) The epidemiologic transition. A theory of the epidemiology of population change. Milbank Mem Fund Q 49:509–538
Marengoni A, Angleman S (2011) Aging with multimorbidity: a systematic review of the literature. Ageing Res Rev 10:430–439
Barnes MK, Duck S (1994) Everyday communicative contexts for social support. Sage Publications, Inc., New York
Uchino B (2004) Social support and physical health: understanding the health consequences of relationships. Yale University Press, New Haven
Langford CP, Bowsher J, Maloney JP et al. (1997) Social support: a conceptual analysis. J Adv Nurs 25:95–100
de Belvis AG, Ferrè F, Specchia ML et al. (2012) The financial crisis in Italy: implications for the healthcare sector. Health Policy (New York) 106:10–16
Karanikolos M, Mladovsky P, Cylus J et al (2013) Financial crisis, austerity, and health in Europe. Lancet 381:1323–1331
Anderson R, Mikuliç B, Vermeylen G et al (2009) Second European quality of life survey—overview, Office for Official Publications of the European Communities, Luxembourg (ISBN 9789289708470)
Karp A, Ebrahimi R, Marengoni A and Fratiglioni L (2010) Informal care and voluntary assistance: a systematic literature review of quantitative and qualitative aspects of assistance to elderly persons in Sweden, Italy, the United Kingdom and Canada. Swedish Government Inquiries, Social Council, Stockholm
Quattrini BCS, Melchiorre MG (2003) Studio Europeo ESAW: la condizione dei carers familiari di persone anziane in Italia. In: 48° conference of the Italian Society of gerontology and geriatrics
Holt-Lunstad J, Smith TB, Baker M et al. (2015) Loneliness and social isolation as risk factors for mortality: a meta-analytic review. Perspect Psychol Sci 10:227–237
Nicholson N (2012) A review of social isolation: an important but underassessed condition in older adults. J Prim Prev 33:137–152
Mazzella F, Cacciatore F, Galizia G, et al. (2010) Social support and long-term mortality in the elderly: role of comorbidity. Arch Gerontol Geriatr 51:323–328
Iwase T, Suzuki E, Fujiwara T et al. (2012) Do bonding and bridging social capital have differential effects on self-rated health? A community based study in Japan. J Epidemiol Community Health 66:557–562
Windsor TD, Rioseco P, Fiori KL et al. (2016) Structural and functional social network attributes moderate the association of self-rated health with mental health in midlife and older adults. Int Psychogeriatr 28:49–61
Rizzuto D, Orsini N, Qiu C et al. (2012) Lifestyle, social factors, and survival after age 75: population based study. Br Med J 345:e5568
Sundquist K, Hamano T, Li X et al (2014) Linking social capital and mortality in the elderly: a Swedish national cohort study. Exp Gerontol 55:29–36
Martire LM, Franks MM (2014) The role of social networks in adult health: introduction to the special issue. Heal Psychol 33:501–504
Seeman TE (1996) Social ties and health: the benefits of social integration. Ann Epidemiol 6:442–451
Krueger KR, Wilson RS, Kamenetsky JM et al. (2009) Social engagement and cognitive function in old age. Exp Aging Res 35:45–60
Wald C (2016) Social networks: better together. Nature 531:S14–S15
Bernabei R, Landi F, Onder G et al. (2008) Second and third generation assessment instruments: the birth of standardization in geriatric care. J Gerontol A Biol Sci Med Sci 63:308–313
Steverink N, Lindenberg S (2006) Which social needs are important for subjective well-being? What happens to them with aging? Psychol Aging 21:281–290
Van Der Gaag M, Snijders TAB (2005) The resource generator: social capital quantification with concrete items. Soc Netw 27:1–29
Burt RS (2009) Structural holes: the social structure of competition. Harvard University Press, Cambridge
Blau P (1977) Inequality and heterogeneity: a primitive theory of social structure. Free Press, New York
Li T, Zhang Y (2015) Social network types and the health of older adults: Exploring reciprocal associations
Steptoe A, Shankar A, Demakakos P et al. (2013) Social isolation, loneliness, and all-cause mortality in older men and women. Proc Natl Acad Sci USA 110:5797–5801
Vassilev I., Rogers A, Blickem C et al. (2013) Social networks, the ‘work’ and work force of chronic illness self-management: a survey analysis of personal communities. PLoS One 8:e59723
Ellwardt L, Van Tilburg TG, Aartsen MJ (2015) The mix matters: complex personal networks relate to higher cognitive functioning in old age”. Soc Sci Med 125:107–115
Rafnsson SB, Shankar A, Steptoe A (2015) Longitudinal influences of social network characteristics on subjective well-being of older adults: findings from the ELSA study. J Aging Health 27:919–934
Fratiglioni L, Wang HX, Ericsson K et al. (2000) Influence of social network on occurrence of dementia: a community-based longitudinal study. Lancet 355:1315–1319
Ellwardt L, Aartsen M, Deeg D et al. (2013) Does loneliness mediate the relation between social support and cognitive functioning in later life? Soc Sci Med 98:116–124
Squazzoni F (2013) A social science-inspired complexity policy: beyond the mantra of incentivization. Complexity 19:5–13
Smith KP, Christakis NA (2008) Social networks and health. Annu Rev Sociol 34:405–429
Acknowledgements
This work received official support by the Municipality of Brescia and Province of Brescia. The authors are grateful to Leonardo Pedroni for his help with the data input.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
This work was supported by a grant of Fondazione EULO and the University of Brescia (Grant: ANZIANI IN-RETE) and a grant of Senior Italia Federanziani. The funding agencies had no role in the study design, data analysis, preparation, or approval of the manuscript.
Conflict of interest
The authors do not have any conflict of interest to disclose.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the Ethical committee of the Local Health Unit (ASL) of Brescia (Italy) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Bianchetti, L., Squazzoni, F., Casnici, N. et al. Social networks and health status in the elderly: the ‘ANZIANI IN-RETE’ population-based study. Aging Clin Exp Res 29, 1173–1179 (2017). https://doi.org/10.1007/s40520-017-0726-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40520-017-0726-7