
Abstract
Background
Age-related change of spinal alignment in the standing position is known to be associated with decreases in walking speed, and alteration in muscle quantity (i.e., muscle mass) and muscle quality (i.e., increases in the amount of intramuscular non-contractile tissue) of lumbar back muscles. Additionally, the lumbar lordosis angle in the standing position is associated with walking speed, independent of lower-extremity muscle strength, in elderly individuals. However, it is unclear whether spinal alignment in the standing position is associated with walking speed in the elderly, independent of trunk muscle quantity and quality. The present study investigated the association of usual and maximum walking speed with age, sagittal spinal alignment in the standing position, muscle quantity measured as thickness, and quality measured as echo intensity of lumbar muscles in 35 middle-aged and elderly women.
Methods
Sagittal spinal alignment in the standing position (thoracic kyphosis, lumbar lordosis, and sacral anterior inclination angle) using a spinal mouse, and muscle thickness and echo intensity of the lumbar muscles (erector spinae, psoas major, and lumbar multifidus) using an ultrasound imaging device were also measured.
Results
Stepwise regression analysis showed that only age was a significant determinant of usual walking speed. The thickness of the lumbar erector spinae muscle was a significant, independent determinant of maximal walking speed.
Conclusions
The results of this study suggest that a decrease in maximal walking speed is associated with the decrease in lumbar erector spinae muscles thickness rather than spinal alignment in the standing position in middle-aged and elderly women.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Walking speed decreases with aging [1], which leads to a decline of daily activities [2], falls [3], and survival prognosis [4]. Therefore, it is important to identify the risk factors of decreased walking speed to prevent the decline of walking ability in elderly individuals.
Sagittal spinal alignment in the standing position also changes with age-related increased kyphosis [5, 6] and pelvic posterior inclination [5]. It has been demonstrated that changes of spinal alignment in the standing position is associated with a decrease in trunk extensor strength [7], but not with trunk flexor strength [8], in middle-aged and elderly women. Thus, previous studies suggested that age-related changes of spinal alignment in the standing position may be associated with back muscles rather than abdominal muscles.
Recently, it was determined that muscle quantity or muscle mass can be assessed from muscle thickness (MT) [9] using a non-invasive ultrasound imaging device. A non-invasive ultrasound imaging device is plausible for use in muscle thickness measurements to estimate muscle mass and in muscle echo intensity (EI) measurements to estimate the amount of intramuscular non-contractile tissue [10, 11] (i.e., adipose and fibrous tissue). It has been verified that muscle mass and the amount of intramuscular non-contractile tissue on ultrasound imaging are associated with muscle strength in middle-aged and elderly women [12]. Furthermore, our previous study [13] using an ultrasound imaging device has demonstrated that an increase in thoracic kyphosis in the standing position is associated with a decrease in the mass of the lumbar erector spinae muscle. Our study also has demonstrated that an increase in pelvic posterior inclination is associated with a decrease in the mass of the psoas major muscle and an increase in the amount of non-contractile tissue within the lumbar multifidus muscle.
It has been demonstrated that age-related decreases in the lumbar lordosis angle and decreases in lower-extremity muscle strength, such as knee extensor strength, are both independent variables associated with decreases in maximal walking speed in elderly individuals [14]. However, there have been no studies that have focused on whether spinal alignment in the standing position and trunk muscle quantity and quality are independently associated with walking speed. Therefore, it is unclear whether spinal alignment in the standing position, such as increased kyphosis and pelvic posterior inclination, or quantitative and qualitative changes in lumbar back muscles, such as decreases in muscle mass and increases in the amount of non-contractile tissue, influence walking speed in elderly individuals. Furthermore, it is also unclear which quantitative or qualitative change in individual muscles of lumbar back muscles are associated with decreased walking speed.
Therefore, the aims of present study are to investigate the association of walking speed with sagittal spinal alignment in the standing position, muscle mass, and the amount of non-contractile tissue of lumbar back muscles measured using an ultrasound imaging device in middle-aged and elderly women.
Materials and methods
Participants
The subjects were 35 healthy middle-aged and elderly women (mean age 72.9 ± 7.4 years) who were living independently in Kyoto, Japan. The subjects’ characteristics are presented in Table 1. Participants were excluded if they had ongoing low back pain or a history of low back pain lasting 3 months or more in the past; orthopedic, neurological, respiratory, or circulatory disorders; or previous spinal surgery.
The protocol was approved by the Ethics Committee of the Kyoto University Graduate School and Faculty of Medicine. All participants provided written informed consent.
Measurement of walking speed
The usual and maximal walking speeds were determined over a 6-m distance. Participants were provided with 2 m to accelerate and decelerate before and after the test distance. The walking time of the 6-m distance was recorded using a stopwatch, and walking speed (m/s) was calculated. The participants were not allowed to use canes or walkers.
Measurement of spinal alignment in the standing position
Sagittal spinal alignment in the standing position (thoracic kyphosis, lumbar lordosis, and sacral anterior inclination angle) was measured using the Spinal Mouse (Index Ltd., Tokyo, Japan), based on a previous study [13]. The Spinal Mouse was guided along the midline of the spine, starting at the C7 spinous process and finishing at S3. The thoracic kyphosis angle was calculated from the sum of 11 segmental angles from Th1/2 to Th11/12. The lumbar lordosis angle was calculated from the sum of six segmental angles from Th12/L1 to L5/S1. The sacral anterior inclination angle was calculated from the difference between the sacral angle and the vertical plane. Spinal alignment was measured three times, and the mean value was used for analyses.
Ultrasound measurement
MT and EI were measured to evaluate muscle mass and the amount of intramuscular non-contractile tissue, respectively. MT and EI of lumbar back muscles were measured using a B-mode ultrasound imaging device (LOGIQ Book Xp; GE Healthcare Japan, Tokyo, Japan) with an 8-MHz linear array probe, as described previously [13]. Longitudinal ultrasound images of the lumbar erector spinae and psoas major muscles and transverse ultrasound images of the lumbar multifidus muscle were taken bilaterally in the prone position. The measurement sites were defined as 7 cm lateral from the L3 spinous process for the lumbar erector spinae and psoas major muscles, and 2 cm lateral to the L4 spinous process for the lumbar multifidus muscle. A 58-dB gain, 69-Hz dynamic range, and time gain compensation with the neutral position were used for all measurements of lumbar back muscles. Dynamic focus depth was set to the depth of the lumbar back muscles.
From the obtained images, EI was determined using image processing software (ImageJ; National Institutes of Health, Bethesda, MD, USA). Regions of interest were set at a depth of 2.0–3.5 cm for the lumbar erector spinae muscle, 1.5–2.5 cm for the lumbar multifidus muscle, and 3.5–5.0 cm for the psoas major muscle, avoiding the surrounding fascia.
The mean EI of the region was assessed by computer-assisted 8-bit gray-scale analysis and was expressed as a value between 0 (black) and 255 (white). Enhanced EI indicated an increase in the amount of intramuscular non-contractile tissue (i.e., adipose and fibrous tissue) within the muscle. The mean values of the thickness and EI for the right and left muscles were used for analyses.
A previous study has shown a high degree of intrarater reliability of the ultrasound technique for measuring the MT and EI of lumbar back muscles [13].
Statistical analyses
Statistical analyses were performed using SPSS version 17.0 (IBM Japan; Tokyo, Japan). Partial correlations between usual and maximal walking speeds and spinal alignment, MT, and EI with age as a control variable were investigated after normality of the variable was evaluated using Shapiro–Wilk tests. Stepwise regression analysis was employed to investigate the associations with walking speed, using spinal alignment in the standing position, MT, EI, and age as the independent variables. The variance inflation factor (VIF) was examined to monitor for a multicollinearity effect. P values of <0.05 were considered significant.
Results
Results of walking speeds, spinal alignment in the standing position, MT, and EI are presented in Table 1.
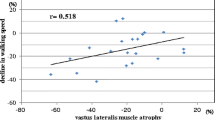
Table 2 indicates the partial correlation coefficients between walking speed and spinal alignment, MT, and EI with age as a control variable. Usual walking speed showed no significant correlations with any of variables. Maximal walking speed showed a significant positive correlation with the thickness of the lumbar erector spinae muscle, i.e., maximal walking speed decreased with decreased thickness of the lumbar erector spinae muscle.
Stepwise regression analysis revealed that only age was a significant and independent determinant of usual walking speed, i.e., usual walking speed decreased with aging. The VIF value was 1.00, which had no multicollinearity effect in a regression equation. In the stepwise regression analysis for maximal walking speed, only the thickness of the lumbar erector spinae muscle was a significant and independent determinant, i.e., maximal walking speed decreased with a decrease in the thickness of the lumbar erector spinae muscle. The VIF value was 1.01, which had no multicollinearity effect (Table 3).
Discussion
Investigating the risk factors of decreased walking speed is important for preventing a decline of walking ability in middle-aged and elderly individuals. To the best of our knowledge, this is the first study examining whether spinal alignment in the standing position and MT or EI of lumbar back muscles are independent variables for walking speed. It is also the first study clarifying whether spinal alignment in the standing position, or MT or EI of lumbar back muscles have greater influence on walking speed in middle-aged and elderly women.
As a result of having examined the factors associated with walking speed, stepwise regression analysis showed that usual walking speed decreased with aging, and that maximal walking speed decreased with a decrease in the thickness of the lumbar erector spinae muscle. Chiu et al. [15] has demonstrated that changes in electromyographic activities in the lumbar spinae, biceps femoris, and medial gastrocnemius muscles showed a marked increase with an increase in walking speed. Anders et al. [16] has also demonstrated that the electromyography (EMG) of the lumbar erector spinae muscle changed in activity amplitude, but not in activity pattern, with an increase in walking speed in healthy subjects. Furthermore, Thorstensson et al. [17] has documented with electromyographic analysis that the main function of the lumbar erector spinae muscle is to restrict excessive trunk movements during walking. The erector spinae muscle may be important in controlling the sagittal and frontal movements on the trunk dynamically during walking, because this muscle has a large moment arm of extension and lateral flexion on the spine [18]. The present study showed the association of the thickness of the lumbar erector spinae muscle with maximal walking speed, not with usual walking speed. This is probably because more swift control of trunk movement is required for maximal walking compared with usual walking.
The present study showed that the thickness of the lumbar multifidus muscle was not associated either with usual or maximal walking speeds. The deep muscles of the back such as the lumbar multifidus muscle contribute to lumbar spine stability [19–21]. It has been demonstrated that the EMG activity of the lumbar multifidus muscle increased with an increase in walking speed in healthy subjects [16, 22], which suggests that the lumbar multifidus muscle has an important role in walking. However, in a previous study [23] examining age-related changes of the back muscles using an ultrasound imaging device in elderly women who were able to perform activities of daily living independently, an age-related atrophy was observed in the erector spinae muscle, but not in the multifidus muscle. Therefore, the lumbar multifidus muscle might not be associated with walking speed due to its lesser age-related atrophy.
In addition to the lumbar multifidus muscle, the psoas major muscle also contributes to lumbar spine stability [24–26]. The psoas major muscle is known to show a marked age-related atrophy [27]. Although the EMG activity of the psoas major muscle increases with an increase in walking speed [28], the thickness of the psoas major muscle has shown no difference between elderly women who were able to walk at a maximum walking speed of more than 1 m/s and elderly women who were not able to walk fast [29]. These previous studies suggest that despite the remarkable age-related atrophy observed in the psoas major muscle, there is only a minor influence of its muscle mass on walking speed among elderly individuals. Therefore, it is confirmed that no correlation was observed between the thickness of the psoas major muscle and walking speed in this study.
In our study, there was no significant association between walking speed and EI in either of the lumbar back muscles, which suggests that walking speed may be influenced by age-related decreases in muscle mass rather than age-related increases in the amount of intramuscular non-contractile tissue within lumbar back muscles.
Furthermore, our results showed that there was no association between maximal walking speed and spinal alignment in the standing position, which is inconsistent with the results of a previous study [14] indicating the association between maximal walking speed and lumbar lordosis angle in elderly individuals. The inconsistency of these results might be influenced by the small sample size in our study.
The present study had several limitations. First, the measurements of MT and EI targeted only the lumbar back muscles. Second, we did not measure muscle strength in the lower extremities, such as knee extensor strength, which is known to be associated with walking speed in elderly individuals. Third, the amount of age-related change in spinal alignment, such as increased kyphosis, was slight in the participants of our study. Further studies are required to clarify the association of walking speed with spinal alignment in the standing position, and quantity and quality of lumbar back muscles in middle-aged and elderly women who have increased kyphosis.
The present study suggests that resistance training targeting the lumbar erector spinae muscles may be important to improve maximal walking speed in middle-aged and elderly women. It has been demonstrated that resistance training on lower extremities was effective for improving walking speed in elderly individuals [30, 31]. However, the effect of resistance training of trunk muscles on walking speed in elderly individuals is unclear. Further study is needed to clarify whether improvement in quantity and quality of the trunk muscles, especially lumbar back muscles, leads to improvement in walking speed for middle-aged and elderly women.
Conclusions
The results of the present study suggest that maximal walking speed is associated with the mass of the lumbar erector spinae muscles rather than spinal alignment in the standing position or age-related increases in the amount of intramuscular non-contractile tissue within lumbar back muscles in middle-aged and elderly women.
References
Lauretani F, Russo CR, Bandinelli S et al (1985) Age-associated changes in skeletal muscles and their effect on mobility: an operational diagnosis of sarcopenia. J Appl Physiol 95:1851–1860
Shinkai S, Watanabe S, Kumagai S et al (2000) Walking speed as a good predictor for the onset of functional dependence in a Japanese rural community population. Age Ageing 29:441–446
Luukinen H, Koski K, Laippala P et al (1995) Risk factors for recurrent falls in the elderly in long-term institutional care. Public Health 109:57–65
Cesari M, Pahor M, Lauretani F et al (2009) Skeletal muscle and mortality results from the InCHIANTI Study. J Gerontol A Biol Sci Med Sci 64:377–384
Takeda N, Kobayashi T, Atsuta Y et al (2009) Changes in the sagittal spinal alignment of the elderly without vertebral fractures: a minimum 10-year longitudinal study. J Orthop Sci 14:748–753
Kado DM, Huang MH, Karlamangla AS et al (2013) Factors associated with kyphosis progression in older women: 15 years’ experience in the study of osteoporotic fractures. J Bone Miner Res 28:179–187
Sinaki M, Itoi E, Rogers JW et al (1996) Correlation of back extensor strength with thoracic kyphosis and lumbar lordosis in estrogen-deficient women. Am J Phys Med Rehabil 75:370–374
Kim HJ, Chung S, Kim S et al (2006) Influences of trunk muscles on lumbar lordosis and sacral angle. Eur Spine J 15:409–414
Miyatani M, Kanehisa H, Ito M et al (2004) The accuracy of volume estimates using ultrasound muscle thickness measurements in different muscle groups. Eur J Appl Physiol 91:264–272
Reimers K, Reimers CD, Wagner S et al (1993) Skeletal muscle sonography: a correlative study of echogenicity and morphology. J Ultrasound Med 12:73–77
Pillen S, Tak RO, Zwarts MJ et al (2009) Skeletal muscle ultrasound: correlation between fibrous tissue and echo intensity. Ultrasound Med Biol 35:443–446
Fukumoto Y, Ikezoe T, Yamada Y et al (2012) Skeletal muscle quality assessed from echo intensity is associated with muscle strength of middle-aged and elderly persons. Eur J Appl Physiol 112:1519–1525
Masaki M, Ikezoe T, Fukumoto Y et al (2015) Association of sagittal spinal alignment with thickness and echo intensity of lumbar back muscles in middle-aged and elderly women. Arch Gerontol Geriatr 61:197–201
Miyazaki J, Murata S, Horie J et al (2013) Lumbar lordosis angle (LLA) and leg strength predict walking ability in elderly males. Arch Gerontol Geriatr 56:141–147
Chiu MC, Wang MJ (2007) The effect of gait speed and gender on perceived exertion, muscle activity, joint motion of lower extremity, ground reaction force and heart rate during normal walking. Gait Posture 25:385–392
Anders C, Wagner H, Puta C et al (2007) Trunk muscle activation patterns during walking at different speeds. J Electromyogr Kinesiol 17:245–252
Thorstensson A, Carlson H, Zomlefer MR et al (1982) Lumbar back muscle activity in relation to trunk movements during locomotion in man. Acta Physiol Scand 116:13–20
Lin YH, Chen CS, Cheng CK et al (2001) Geometric parameters of the in vivo tissues at the lumbosacral joint of young Asian adults. Spine (Phila Pa 1976) 26:2362–2367
Panjabi MM (1992) The stabilizing system of the spine. Part I. Function, dysfunction, adaptation, and enhancement. J Spinal Disord 5:383–389 (discussion 397)
Panjabi MM (1992) The stabilizing system of the spine. Part II. Neutral zone and instability hypothesis. J Spinal Disord 5:390–396 (discussion 397)
Wilke HJ, Wolf S, Claes LE et al (1995) Stability increase of the lumbar spine with different muscle groups. A biomechanical in vitro study. Spine (Phila Pa 1976) 20:192–198
Lee HS, Shim JS, Lee ST et al (2014) Facilitating effects of fast and slope walking on paraspinal muscles. Ann Rehabil Med 38:514–522
Ikezoe T, Mori N, Nakamura M et al (2012) Effects of age and inactivity due to prolonged bed rest on atrophy of trunk muscles. Eur J Appl Physiol 112:43–48
Penning L (2000) Psoas muscle and lumbar spine stability: a concept uniting existing controversies. Critical review and hypothesis. Eur Spine J 9:577–585
Jemmett RS, Macdonald DA, Agur AM (2004) Anatomical relationships between selected segmental muscles of the lumbar spine in the context of multi-planar segmental motion: a preliminary investigation. Man Ther 9:203–210
Blemker SS, Delp SL (2005) Three-dimensional representation of complex muscle architectures and geometries. Ann Biomed Eng 33:661–673
Ikezoe T, Mori N, Nakamura M et al (2011) Age-related muscle atrophy in the lower extremities and daily physical activity in elderly women. Arch Gerontol Geriatr 53:e153–e157
Andersson EA, Nilsson J, Thorstensson A (1997) Intramuscular EMG from the hip flexor muscles during human locomotion. Acta Physiol Scand 161:361–370
Ikezoe T, Mori N, Nakamura M et al (2011) Atrophy of the lower limbs in elderly women: is it related to walking ability? Eur J Appl Physiol 111:989–995
Boshuizen HC, Stemmerik L, Westhoff MH et al (2005) The effects of physical therapists’ guidance on improvement in a strength-training program for the frail elderly. J Aging Phys Act 13:5–22
Protas EJ, Tissier S (2009) Strength and speed training for elders with mobility disability. J Aging Phys Act 17:257–271
Acknowledgments
The authors would like to thank Saori Shibuta, Natsuki Yamakami, and Kosuke Saida (Human Health Sciences, Graduate School of Medicine, Kyoto University) for their practical and technical assistance. The authors also thank all of the individuals who participated in the present study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
No funding sources were disclosed for the study.
Conflict of interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Masaki, M., Ikezoe, T., Fukumoto, Y. et al. Association of walking speed with sagittal spinal alignment, muscle thickness, and echo intensity of lumbar back muscles in middle-aged and elderly women. Aging Clin Exp Res 28, 429–434 (2016). https://doi.org/10.1007/s40520-015-0442-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40520-015-0442-0