
Abstract
The use of medication with anticholinergic properties is widespread among older subjects. Many drugs of common use such as antispasmodics, bronchodilators, antiarrhythmics, antihistamines, anti-hypertensive drugs, antiparkinson agents, skeletal muscle relaxants, and psychotropic drugs have been demonstrated to have an anticholinergic activity. The most frequent adverse effects are dry mouth, nausea, vomiting, constipation, abdominal pain, urinary retention, blurred vision, tachycardia and neurologic impairment such as confusion, agitation and coma. A growing evidence from experimental studies and clinical observations suggests that drugs with anticholinergic properties can cause physical and mental impairment in the elderly population. However, the morbidity and management issues associated with unwanted anticholinergic activity are underestimated and frequently overlooked. Moreover, their possible relation with specific negative outcome in the elderly population is still not firmly established. The aim of the present review was to evaluate the relationship between the use of drugs with anticholinergic activity and negative outcomes in older persons. We searched PubMed and Cochrane combining the search terms “anticholinergic”, “delirium”, “cognitive impairment”, “falls”, “mortality” and “discontinuation”. Medicines with anticholinergic properties may increase the risks of functional and cognitive decline, morbidity, institutionalization and mortality in older people. However, such evidences are still not conclusive probably due to possible confounding factors. In particular, more studies are needed to investigate the effects of discontinuation of drug with anticholinergic properties. Overall, minimizing anticholinergic burden should always be encouraged in clinical practice to improve short-term memory, confusion and delirium, quality of life and daily functioning.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Medication consumption in frail older people is usually high, and several usually prescribed drugs have anticholinergic side effects. Some studies have estimated that in nursing homes more than 30 % of older residents take more than two anticholinergic drugs, and 5 % take more than five [1, 2]. Furthermore, an estimated 51 % of the general population use anticholinergic drugs [3] and nearly one-half of community-dwelling older adults have a clinically relevant anticholinergic cognitive burden score [4].
Anticholinergic drugs act on the muscarinic receptors in the central and peripheral nervous systems and inhibit acetylcholine-mediated responses by competitively binding to these receptors. As a consequence, these drugs are used therapeutically in a wide variety of clinical disorders such as Parkinson’s disease and urinary incontinence. Other classes of drugs utilized for different therapeutic reasons which also have anticholinergic properties are antihistamines and classical antipsychotics (Table 1).
Typical peripheral side effects are gastrointestinal (e.g., dry mouth, nausea, vomiting, constipation, bloated feeling, abdominal pain, taste loss, anorexia) and ophthalmologic symptoms (e.g., blurred vision, diplopia, mydriasis, cycloplegia, increased ocular tension). The most frequent central side effects are dizziness, lightheadedness, tingling, headache, drowsiness, weakness, nervousness, numbness, mental confusion and/or excitement (especially in older persons), dyskinesia, lethargy, syncope, speech disturbance, and insomnia [5, 6]. Figure 1 shows the most common anticholinergic side effects related to a growing anticholinergic burden.

Side effects with increasing anticholinergic activity
The majority of these drugs are likely to have a toxic effect on the aging brain because of augmented permeability of the blood–brain barrier, slower metabolism and drug elimination and age-related deficit in central cholinergic transmission [7]. Furthermore, older people often suffer from multiple diseases and are usually treated with different types of drugs, increasing the probability and severity of cumulative adverse events [8]. For these reasons, they have been considered potentially inappropriate in older subjects [9]. However, anticholinergic side effects are often viewed as “unavoidable” or they are wrongly attributed to the aging process itself [10].
An important risk factor for the prescription of anticholinergic drugs is institutionalization. Potentially inappropriate drug use is common among hospitalized older adults [11, 12]. Some studies have clearly demonstrated that older people in nursing home care use significantly more anticholinergic drugs than those living at home [13, 14]. It has also been reported that among hospitalized people aged above 65 years, the prevalence of anticholinergic prescriptions increases significantly during their hospital stay, although the Geriatric Care Units are more vigilant than others to the use of anticholinergic drugs [15]. Finally, it has been shown that in palliative care, the use of anticholinergic drugs increases as death approaches [16].
Anticholinergic drug burden evaluation
The importance of anticholinergic drugs use, especially in the older population, has led to the development of methods for estimating the overall anticholinergic drug burden in a subject [17]. Both in vitro methods and anticholinergic scales have been developed to predict the risk of peripheral and central adverse events, to reduce the risk of secondary negative brain effects of drug therapy and optimize polypharmacy. However, there is still no consensus on how to define drug exposure and none of these methods has been standardized [18–21].
The serum anticholinergic activity (SAA) is an estimate of the overall anticholinergic activity towards rat brain muscarinic receptors in an individual’s serum. Many factors contribute to the SAA, such as medications, endogenous substances and stress responses. In 2008, Chew et al. [22] dosed the anticholinergic activity (AA) of 107 medications at doses typically administered to older adults. They compared the AA of different drugs within the same therapeutic group to help clinicians to choose between equally efficacious medications. However, the in vitro method used to measure SAA present some limitation in estimating the overall anticholinergic drug burden in the human brain. First of all, SAA is not a measure of the central action of anticholinergic drug but of the peripheral one since it does not reflect the drug concentrations in the brain [23]. Even measuring AA in cerebrospinal fluid would not predict the individual sensitivity of being cognitively affected by the drugs since it would not consider the brain distribution. Indeed, one study found no correlation between SAA and the cerebral cholinergic function measured with electroencephalography [24]. Second, SAA does not make a distinction between medications, endogenous compounds or stress responses to acute illness [25]. It has been proved that the level of SAA increases during acute illness and declines after recovery from it [26]. Also natural substances, such as cortisol, have binding affinity for muscarinic receptors in vitro. Moreover, the binding assay does not distinguish between antagonistic and agonistic activity towards the muscarinic receptors nor between the specific binding to each muscarinic subtype. Finally, the bioassay is not standardized and the range of SAA varies considerably between different reports and the assay methodology varies between different laboratories.
On the other hand, the anticholinergic drug scales are expert-based score models developed to determine the anticholinergic drug burden. Such scales usually rank medication on a four-point scale depending on the anticholinergic potential, ranging from limited or none (0), moderate (1), strong (2), very strong (3) potential [18, 19, 21]. They identify the drugs that might cause adverse effects and suggest which drugs to withdraw to optimize pharmacotherapy for older people.
The Anticholinergic Drug Scale (ADS) was the first scale developed [27] and is based on a three-level anticholinergic classification system of 62 medications. Afterwards, this scale has been modified and extended [28]. It has been shown that ADS was significantly associated with SAA [18]. The Anticholinergic Burden Scale (ACB) assesses the cognitive impact of any anticholinergic drug and is based on literature reviews of the drugs’ anticholinergic potential, whereas the Anticholinergic Risk Scale (ARS) assesses the risk of both peripheral and central anticholinergic adverse effects, taking also into account the dissociation constants for the muscarinic receptors [19]. Drug Burden Index (DBI) includes both sedative and anticholinergic drugs and unlike the other scale is adjusted for dose [20]. In all these scale models, the total anticholinergic burden is determined by the sum of each drug’s anticholinergic score, giving the assumption that the anticholinergic effect of different drugs respects a linear additive model.
Finally, a recent review has developed a new list of 100 anticholinergic drugs based on previously published lists in a first attempt to standardize an anticholinergic scale [29].
Anticholinergic drugs and negative outcomes
The aim of the present review is to collect recent evidences regarding possible adverse outcome linked to the use of medication with anticholinergic effect in the elderly population, with a special focus to cognitive impairment, delirium, falls and mortality.
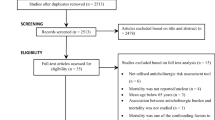
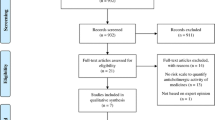
We searched PubMed and Cochrane combining the search terms “anticholinergic”, “delirium”, “cognitive impairment”, “falls”, “mortality”, “discontinuation”. We limited our research to the English language and human studies. The literature review was performed independently by two researchers between August and December 2014. We considered the time frame from January 2000 to December 2014. To identify pertinent studies, we scanned titles and abstracts from each retrieved citation. For selected articles we obtained the full text, when freely available in the University Library. We also retrieved additional pertinent publications using the reference lists and the related article section of PubMed for the identified articles.
Anticholinergic drugs and cognitive impairment
Anticholinergic drugs are a biologically plausible cause of cognitive impairment in older people. Cholinergic deficits may accompany aging and also play a central role in the pathophysiology of Alzheimer’s disease. The older person and those with comorbid medical or psychiatric conditions, such as schizophrenia or dementia, are particularly vulnerable to the more subtle cognitive effects (e.g., attention and memory deficits) of drugs with anticholinergic properties. Age-related peripheral and central pharmacokinetic changes and pharmacodynamic effects on neurotransmission may contribute to the phenomena of increased drug sensitivity in the older people [30, 31], making them particularly susceptible to drug-induced cognitive deficits [32].
Several experimental and clinical studies have demonstrated the detrimental effect of anticholinergic drugs on cognition [7]. In one study of 201 community-based older subjects, a significant association was found between serum anticholinergic activity (SAA) and lower Mini Mental State Exam scores [3]. In a more recent study of 750 persons aged ≥65 years, individuals using drugs with anticholinergic effects were more likely to have cognitive impairment than those using non-anticholinergic medications [33].
Despite their well-known anticholinergic hypersensitivity, older patients with dementia are more frequently exposed to definite anticholinergic drugs than are those without dementia [34–36]. Up to half the people on acetylcholinesterase inhibitors (AChEIs) are also taking drugs that have anticholinergic activity [37–39], with consequent possible reduction of the efficacy of AChEI [40, 41]. Focusing on patient with dementia, one study showed an association between SAA and lower cognitive performance in 26 patients admitted to a gero-psychiatric unit for the treatment of behavioral disturbances associated with moderate-to-severe dementia [42]. Moreover, anticholinergic drug use could be a risk factor for psychosis onset in persons with Alzheimer’s disease [43].
As highlighted in a previous review by Cancelli et al. [44], three cross-sectional population-based studies have investigated the effect of ACH drug intake on cognition [33, 45, 46].
In 2005, Lechevallier-Michel et al. [45] found an association between use of ACH drugs and low cognitive performance (global cognitive functioning, immediate visual memory, verbal fluency) in a non-demented population of 1780 people aged 70 and above. Similar results were found in a subsequent study involving 932 moderately to severely disabled women aged 65 years or more [46]. The results confirmed the presence of a link between ACH drug intake and low MMSE scores. Cancelli et al. [33] confirmed the previous evidence that suggested how anticholinergic drug intake should be regarded as a potentially modifiable risk factor for cognitive impairment in older people. In their study, they enrolled a population of 750 subjects aged 65 years or older and employed the MMSE and the Global Deterioration Scale to evaluate the cognitive impairment. They found that approximately 20 % of the study subjects were ACH drug users and that they were more likely to have cognitive impairment than those using non-ACH drugs.
Two longitudinal studies have been carried out to assess the link between ACH drug intake and cognitive impairment, but they did not achieve a definitive result [47, 48].
Ancelin et al. [47] found that anticholinergic drugs users had significant deficits in cognitive functioning and were highly likely to be classified as mildly cognitively impaired, although they did not have an increased risk for dementia. Similarly, Bottigi et al. [48] found no significant differences between ACH drug users and the non-ACH drug users, after adjusting for age and education.
In recent years, epidemiological and longitudinal observational studies have found that chronic anticholinergic use is associated with ~1.5–2 times greater risk of developing cognitive impairment and dementia in both European and African American samples [49–51]. This risk may be mitigated by discontinuing drugs with antimuscarinic properties [51]. In one study, a high anticholinergic burden increased the cumulative risk of both cognitive impairment and mortality in older patients. The authors suggested that for each one point increase in the ACB total score, a decline in MMSE of 0.33 points over 2 years could be expected and a 26 % increase in the risk of death [52]. Moreover, Pasina et al. [53] demonstrated that drugs with anticholinergic properties identified by the ACB scale and ARS were associated with worse cognitive and functional performance in a population of 1380 inpatient aged 65 or more. The two scales showed a poor overlap and the results suggested that the ARS is more specific but less selective than the ACB in identifying medications that are associated with poorer cognitive outcomes.
Very recently, in a prospective population-based cohort study involving 3434 patients with no dementia at study entry with a mean follow-up of 7.3 years, Gray et al. demonstrated a relationship between 10-year cumulative anticholinergic drug exposure and increased risk of incident dementia [54].
Cumulative anticholinergic drug exposure has been related to deficits in cognitive functioning in a longitudinal study [55]. Conversely, another study did not support the additive properties of the anticholinergic risk scale scores as no progressive decline in cognitive function was observed when the ADS scores increased above three in a nursing home population [56]. In a recent review by Kersten et al. [17], nine studies found no significant relationship between a high anticholinergic burden and poorer cognitive outcomes, whereas ten reported statistically significant relationships.
The major reason why the relationship between cognitive abilities and anticholinergic burden is hard to show in older populations is probably the heterogeneity in cholinergic brain reserves, which causes great differences in the sensitivity to central anticholinergic effects.
Overall, it is good practice to keep the anticholinergic load low in the older people in general and in people with dementia in particular by reducing the total number of drugs with anticholinergic properties used together. Drugs with alternative mechanisms of action should be used where available. Alternatively, choosing drugs with low anticholinergic activity or with high specificity to the site of action and thus minimal central activity is encouraged. Anticholinergic drugs that do not cross the blood–brain barrier may have less effect on cognitive function.
Anticholinergic drugs and delirium
Delirium is a relatively common disorder, especially in older people with acute physical illness; it is correlated to a high morbidity and mortality and is often under-recognized and undertreated [44, 57]. Identifying risk factors for delirium, especially modifiable ones, is of great importance for the effective prevention of this condition. Prescribed medications are the sole cause of delirium in between 12 and 39 % of cases [58]. Both hypo-reactive and hyper-active delirium have been proved to be caused by a reduction in cholinergic signaling due to anticholinergic drugs [59].
In recent decades, an increasing number of studies have examined the risk factors that might predispose, precipitate or perpetuate development and progression of delirium and a growing evidence has been produced suggesting a possible relationship between ACH drug intake and neuropsychiatric manifestation [31]. Indeed, the association between anticholinergic drug intake and delirium has a high biological plausibility. At the moment, the most widely accepted theory is that delirium represents the clinical manifestation of a diffuse imbalance of cerebral neurotransmission. Probably, several neurotransmitters such as serotonin, noradrenaline, dopamine, and c-aminobutyric acid (GABA) are involved in its pathogenesis and any drug interfering with neurotransmission may therefore facilitate delirium onset.
So far, research findings are still controversial, but most published studies considered ACH drug use to be a precipitating factor [31]. Recently, Zimmerman et al. [60] demonstrated that an increase in the ARS from admission through hospital stay was significantly associated to delirium in palliative care inpatients. Best et al. [61] found that DBI was associated with an increased risk of hospital admission for delirium in a retrospective analysis of hospitalized patient. This evidence is in contrast with previous results. An observational cohort study carried out in a population of 65 or older patient with cognitive impairment admitted to a general medical ward failed to find an association between prescription of anticholinergic medication (evaluated through ACB scale) and incident delirium [62]. Also, Luukkanen et al. [63] demonstrated that the use of drugs with anticholinergic properties was not able to predict delirium and mortality in 425 patients in geriatric wards and nursing home. Another longitudinal study on older patients with hip fracture showed uncontrolled SAA levels in patients who developed delirium. Nevertheless, other delirium predisposing factors such as cognitive impairment and IL-6 values were so closely associated with changes in the temporal profile of serum anticholinergic activity that neutralized the previously documented association [64]. Likewise, a prospective cohort study evaluated subjects admitted with hip fracture measuring anticholinergic activity in serum and in cerebrospinal fluid and did not find any difference between patients who developed delirium and those who did not [65].
Several reasons may underlie this discrepancy in the results. First, there is not a uniform measurement of anticholinergic drug exposure between different studies that cannot be compared. Furthermore, the effect of anticholinergic medications on delirium may be confounded by other risk factors, such as cognitive impairment, age or comorbidity. Overall, anticholinergic drugs seem to be a highly plausible risk factor for delirium in older patients. Dementia, polypharmacy, and multiple comorbidity further increase the predisposition of older patients to develop anticholinergic drug-induced delirium.
Anticholinergic drugs and falls
Falls are another possible anticholinergic adverse outcome in older subjects. Anticholinergic drugs side effects that include weakness, mental confusion, lightheadedness and blurred vision can easily explain an increased risk of such a common geriatric syndrome. However, the evidence supporting this association is contrasting.
As a matter of fact, drugs with neurotropic effect such as neuroleptics, sedatives and antidepressants have been associated with falls in different geriatric care settings [66–68].
On one hand, long-acting benzodiazepines, psychotropics and medications with anticholinergic properties have been linked to an increased risk of falling in a prospective cohort study of community-dwelling France population [69].
On the other hand, Fraser et al. [70] investigated the fall and fracture risk associated with anticholinergic drugs in a population-based Canadian cohort in a follow-up of 10 years. Anticholinergic medication use was associated with falls at baseline, at years 5 and 10, but the association was no longer significant after covariate adjustment. Similar results occurred with incident risk fracture and mean change in femoral neck BMD T score. In the same direction, a previous retrospective analysis of patient admitted under the care of the geriatric medicine or rehabilitation teams carried out by Best et al. [61] found no correlation between polypharmacy (defined as the use of more than five regular medication) and DBI and falls, showing instead an increased risk of hospital admission for delirium in exposed population.
In contrast with such results, a recent study demonstrated that polypharmacy and exposure to DBI drugs were independently associated with fall-related hospitalizations, frequency of general practitioner visits, and risk of mortality on a population of ≥65-year-old people living in New Zealand [71].
An observational longitudinal study by Dauphinot et al. [72] focused in particular on the effect of an increased exposure to anticholinergic and sedative medication (measure with BDI) during hospital stay and its relation to in-hospital falls and mortality, finding a significant association with the former, not with the latter.
Moreover, different care setting was investigated. 1490 nursing home residents have been evaluated in a prospective multicenter observational study carried out in 31 facilities on the Italian territory. Their anticholinergic burden was measured through the ARS. A higher score in the ARS scale was related to a higher rate of falls as well as a greater likelihood of functional decline and a higher incidence of delirium in a 1-year follow-up [73]. Similarly, a previous Australian study of a population of older people in residential aged care facilities showed that DBI was significantly and independently associated with falls [74].
Two specific populations were object of study for risk of falls: older people with traumatic brain injuries in residential treatment and older psychiatric inpatient. In both cases, anticholinergic medications were associated with an increased risk of falls [75, 76].
Overall, a definitive demonstration of the connection between falls and anticholinergic drugs is still lacking. This is probably due to the possible confounders that are often associated with anticholinergic prescription such as cognitive impairment, behavioral disorders, incontinence, polypharmacy, poor physical performance that could explain by themselves an increased risk of falling.
Anticholinergic drugs, physical performance and function
A previous study suggested that inappropriate drug use is associated with a worse physical performance among elderly population [77]. In particular, drugs with anticholinergic properties could be implicated in physical impairments [7]. This could be ascribed to their both central and peripheral adverse effects such as mental confusion or excitement, dyskinesia, lethargy, insomnia, lightheadedness, headache or dry mouth, nausea, vomiting, diplopia, mydriasis, cycloplegia, respectively. Furthermore, as mentioned before, in older people these effects are often enhanced as a consequence of polypharmacy: many older people take more than one drug with anticholinergic properties. In addition, the amount of acetylcholine decreases with age and consequently, anticholinergic drugs block a higher percentage of acetylcholine [6].
Based on those findings, many authors investigated the relationship between the use of drugs with anticholinergic properties and measures of physical performance and functional status in older people. Landi et al. [6] evaluated the association between the use of drugs with anticholinergic activity and measures of physical performance (4-m walking test, Short Physical Performance Battery), muscle strength (hand grip strength), and functional status (basic and Instrumental activities of daily living) in 364 persons aged 80 years or older enrolled in the “Invecchiamento e Longevità nel Sirente” study. 40 % of the study sample used drugs with anticholinergic effects. They found a significant association between all physical performance measures and use of anticholinergic drugs, which remained still significant after adjustment for potential confounders. Notably, these associations did not change after excluding the most frequent drugs with anticholinergic properties, such as digoxin and furosemide. Furthermore, in this study, the 4-m walking speed, physical performance battery score, hand grip strength, activities of daily living scale scores showed worsened results among subjects using two or more medications with anticholinergic properties compared with subjects using one or no anticholinergic drugs. These results were confirmed by Lowry et al. [78] who demonstrated that high ARS scores were negatively associated with various components of Barthel Index, in particular bathing, grooming, dressing, transfers, mobility and stairs. In addition, Bostock et al. [79] analyzed the association between different measures of anticholinergic drug exposure and Barthel Index in 271 older hospitalized patients. The results showed an inverse correlation between Barthel Index and use of anticholinergic drugs measured by “anticholinergic risk scale”, “the anticholinergic burden”, number of anticholinergic medications. Other authors investigated the predictive value of different scales to quantify anticholinergic use and amount and its cognitive and functional consequences. A study conducted in 1380 patients aged 65 years or older showed that patients identified with the Anticholinergic Risk Scale had more severe cognitive and physical impairment than patients identified with the Anticholinergic Cognitive Burden scale, with a clear dose–response effect [53]. Furthermore, recent studies available in literature had shown that higher anticholinergic drug exposure on admission independently predicted reduced functional outcomes in older patients undergoing orthopedic rehabilitation [80].
Overall, these findings are important because a poorer outcome in, for instance, gait speed or hand grip strength might predict cognitive decline, frailty and disability, which are of major importance in geriatric risk management.
Anticholinergic drugs and mortality
The impact of the anticholinergic burden on mortality has also been studied, although with inconsistent findings. Fox et al. [52] carried out a 2-year longitudinal study involving 13,004 participants aged 65 or more and demonstrated that 2-year mortality was greater in those taking definite and possible anticholinergics drug measured by means of the ACB Scale. Similarly, in another study, the ARS score predicted 3-month mortality in 71 older hospitalized awaiting surgical repair after hip fractures [81]. On the other hand, more recent studies did not confirm such association. A recent observational longitudinal study conducted among 337 older patients in 3 geriatric hospitals in France quantified the exposure to anticholinergic and sedative medications using DBI. They found that increased exposure to anticholinergic and sedative medications during hospital stay was not associated with mortality while was associated with falls [72]. In a similar manner, there were no significant differences in terms of inpatient mortality between different ACB categories in a retrospective analysis of an oldest old hospitalized population [82].
Moreover, in a prospective, multicentre, cohort study Narbey et al. [83] did not observe any statistically significant relationship between the use of anticholinergic drugs and one-year mortality or nursing home admission in elderly patients hospitalized via the emergency department. Two other different studies found that drugs with anticholinergic properties (DAPs) did not predict mortality in a population of frail inpatients with comorbidities [63] and in older patients with stable cardiovascular disease [84]. Finally, a previous Finnish study did not support that higher ARS scores were associated with mortality in long-term care patients [85].
In general, all these studies suffer from the limitation of their observational design. Randomized controlled trials are required to provide evidence for the presumed relationship between the anticholinergic drug burden and the risk stratification of elderly populations.
Anticholinergic drug discontinuation
Although controversial and not definitively established, the idea of possible negative consequences on health status of anticholinergic drugs in the older population is currently widespread and widely agreed. Therefore, minimizing anticholinergic burden should result in improved short-term memory, confusion and delirium, and may improve the quality of life and daily functioning.
A recent systematic review [86] investigated the impact of discontinuing medicines with anticholinergic properties in older people with a specific focus on cognitive outcomes. The review found two randomized control trials and two prospective cohort studies that met the inclusion criteria. Among them, only the cohort studies [87, 88] demonstrated improvement of cognitive performance after discontinuation of anticholinergic medicines, but both studies were limited by their small sample size (21 hospitalized patient with schizophrenia in the first study [87], 9 inpatient with Parkinson disease in the second one [88]). The first randomized, controlled trial evaluated 34 randomly selected older residents. When the ADS score was reduced from 3.7 to 1.3, improvements in two of the 12 psychometric scales measured were observed but globally no significant improvement in cognitive performance was shown [89]. The second randomized, controlled trial was conducted in 87 long-term residents with an ADS score of greater than or equal to 3 from 22 nursing homes in Norway. A pharmacist-initiated drug review determined a reduction from 4 to 2 in the ADS score but it did not translate into cognitive improvement, reduced SAA or reduced mouth dryness [90]. A successive cohort study by Yeh et al. [91] aimed to reduce anticholinergic drug burden through an educational program for primary care physicians, but the benefit in term of mean Mini Mental State Examination and Barthel Index remained unclear within the first 12 weeks.
Furthermore, a pilot randomized trial that utilized the DBI failed to reduce the anticholinergic drug prescriptions made by general practitioners [92] showing that the DBI is not easily integrated in clinical practice.
Up to day, there are no specific guide lines to orientate drug escalation or adjustment. But in the last decades the issue of appropriate prescribing, especially in the older population, has deserved wide interest and has pushed the development of different criteria for appropriate prescription, the most commonly cited being the Beers criteria [93] and the recently developed STOPP (Screening Tool of Older Person’s Prescription) and START (Screening tool to Alert doctors to Right Treatment) criteria [94].
In the STOPP criteria, anticholinergic drugs are specifically mentioned for their risk of toxicity together with tricyclic antidepressant, phenothiazines, benzodiazepines, neuroleptics and antihistamines.
Finally, a special attention should be paid to the older patient with chronic kidney disease. As clearly shown in a recent review [95], older people with renal function impairment experiment higher rates of adverse drug reaction. Again, anticholinergic drugs are cited among the drugs that should be avoided in such a frial population.
Globally, the impact of anticholinergic discontinuation on cognitive function remains poorly researched and poorly understood. A larger sample size, longer duration of follow-up and better methods of assessing anticholinergic-induced cognitive impairment are needed. Moreover, clinical trials of discontinuation of anticholinergic drugs should also investigate the effect on the other outcomes, i.e., falls, delirium, physical performance and functional status. In the meanwhile, a good clinical practice aimed to minimize anticholinergic load (or reach a tailored anticholinergic prescription) should be encouraged.
Conclusion
The research, up to date, suggested that medicines with anticholinergic properties may increase the risks of functional and cognitive decline, morbidity, institutionalization and mortality in older people. This association is rational since it is based on pharmacodynamic and pharmacokinetic characteristics of these drugs. However, the evidence provided by the studies is still globally inconclusive. More studies are needed to clarify the association between anticholinergic drug use and negative outcome in older adults as well as the potential health benefit obtained with their discontinuation.
References
García-Gollarte F, Baleriola-Júlvez J, Ferrero-López I et al (2012) Inappropriate drug prescription at nursing home admission. J Am Med Dir Assoc 13:83.e9–83.e15
Kolanowski A, Fick DM, Campbell J et al (2009) A preliminary study of anticholinergic burden and relationship to a quality of life indicator, engagement in activities, in nursing home residents with dementia. J Am Med Dir Assoc 10:252–257
Mulsant BH, Pollock BG, Kirshner M et al (2003) Serum anticholinergic activity in a community-based sample of older adults: relationship with cognitive performance. Arch Gen Psychiatry 60:198–203
West T, Pruchnicki MC, Porter K et al (2013) Evaluation of anticholinergic burden of medications in older adults. J Am Pharm Assoc 53:496–504
Morley JE (2011) Anticholinergic medications and cognition. J Am Med Dir Assoc 12:543–555
Landi F, Russo A, Liperoti R et al (2007) Anticholinergic drugs and physical function among frail elderly population. Clin Pharmacol Ther 81:235–241
Mintzer J, Burns A (2000) Anticholinergic side-effects of drugs in elderly people. J R Soc Med 93(9):457–462
Onder G, Landi F, Liperoti R et al (2005) Impact of inappropriate drug use among hospitalized older adults. Eur J Clin Pharmacol 61:453–459
Dilles T, Vander Stichele RH, Van Bortel LM et al (2013) The development and test of an intervention to improve ADR screening in nursing homes. J Am Med Dir Assoc 14:379.e1–379.e6
Tune LE (2001) Anticholinergic effects of medication in elderly patients. J Clin Psychiatry 62(Suppl 21):11–14
Tosato M, Landi F, Martone AM et al (2014) Potentially inappropriate drug use among hospitalised older adults: results from the CRIME study. Age Ageing 43(6):767–773. doi:10.1093/ageing/afu029
Onder G, Landi F, Cesari M et al (2003) Inappropriate medication use among hospitalized older adults in Italy: results from the Italian Group of Pharmacoepidemiology in the Elderly. Eur J Clin Pharmacol 59(2):157–162
Tamura BK, Bell CL, Inaba M et al (2012) Outcomes of polypharmacy in nursing home residents. Clin Geriatr Med 28:217–236
Haasum Y, Fastbom J, Johnell K (2012) Institutionalization as a risk factor for inappropriate drug use in the elderly: a Swedish nationwide register-based study. Ann Pharmacother 46:339–346
Wawruch M, Macugova A, Kostkova L et al (2012) The use of medications with anticholinergic properties and risk factors for their use in hospitalized elderly patients. Pharmacoepidemiol Drug Saf 21(2):170–176. doi:10.1002/pds.2169
Agar M, Currow D, Plummer J et al (2009) Changes in anticholinergic load from regular prescribed medications in palliative care as death approaches. Palliat Med 23:257–265
Kersten H, Wyller TB (2014) Anticholinergic drug burden in older people’s brain—how well is it measured? Basic Clin Pharmacol Toxicol 114(2):151–159. doi:10.1111/bcpt.12140
Carnahan RM, Lund BC, Perry PJ et al (2006) The Anticholinergic Drug Scale as a measure of drug-related anticholinergic burden: associations with serum anticholinergic activity. J Clin Pharmacol 46(12):1481–1486
Rudolph JL, Salow MJ, Angelini MC et al (2008) The anticholinergic risk scale and anticholinergic adverse effects in older persons. Arch Intern Med 168:508–513
Hilmer SN, Mager DE, Simonsick EM et al (2007) A drug burden index to define the functional burden of medications in older people. Arch Intern Med 167(8):781–787
Boustani M, Baker MS, Campbell N et al (2010) Impact and recognition of cognitive impairment among hospitalized elders. J Hosp Med 5(2):69–75. doi:10.1002/jhm.589
Chew ML, Mulsant BH, Pollock BG et al (2008) Anticholinergic activity of 107 medications commonly used by older adults. J Am Geriatr Soc 56(7):1333–1341. doi:10.1111/j.1532-5415.2008.01737.x
Scheife R, Takeda M (2005) Central nervous system safety of anticholinergic drugs for the treatment of overactive bladder in the elderly. Clin Ther 27:144–153
Thomas C, Hestermann U, Kopitz J et al (2008) Serum anticholinergic activity and cerebral cholinergic dysfunction: an EEG study in frail elderly with and without delirium. BMC Neurosci 15(9):86. doi:10.1186/1471-2202-9-86
Carnahan RM, Lund BC, Perry PJ et al (2002) A critical appraisal of the utility of the serum anticholinergic activity assay in research and clinical practice. Psychopharmacol Bull 36(2):24–39
Flacker JM, Lipsitz LA (1999) Serum anticholinergic activity changes with acute illness in elderly medical patients. J Gerontol A Biol Sci Med Sci 54:M12–M16
Summers WK (1978) A clinical method of estimating risk of drug induced delirium. Life Sci 22:1511–1516
Han L, McCusker J, Cole M (2001) Use of medications with anticholinergic effects predicts clinical severity of delirium symptoms in older medical inpatients. Arch Intern Med 161:1099–1105
Durán CE, Azermai M, Vander Stichele RH (2013) Systematic review of anticholinergic risk scales in older adults. Eur J Clin Pharmacol 69(7):1485–1496. doi:10.1007/s00228-013-1499-3
Leon C, Gerretsen P, Uchida H et al (2010) Sensitivity to antipsychotic drugs in older adults. Curr Psychiatry Rep 12(1):28–33. doi:10.1007/s11920-009-0080-3
Uchida H, Mamo DC, Mulsant BH et al (2009) Increased antipsychotic sensitivity in elderly patients: evidence and mechanisms. J Clin Psychiatry 70(3):397–405
Tannenbaum C, Paquette A, Hilmer S et al (2012) A systematic review of amnestic and non-amnestic mild cognitive impairment induced by anticholinergic, antihistamine GABAergic and opioid drugs. Drugs Aging 29(8):639–658. doi:10.2165/11633250-000000000-00000
Cancelli I, Gigli GL, Piani A et al (2008) Drugs with anticholinergic properties as a risk factor for cognitive impairment in elderly people: a population-based study. J Clin Psychopharmacol 28(6):654–659. doi:10.1097/JCP.0b013e31818ce849
Roe CM, Anderson MJ, Spivack B (2002) Use of anticholinergic medications by older adults with dementia. J Am Geriatr Soc 50(5):836–842
Giron MS, Wang HX, Bernsten C et al (2001) The appropriateness of drug use in an older non demented and demented population. J Am Geriatr Soc 49:277–283
Johnell K, Fastbom J (2008) Concurrent use of anticholinergic drugs and cholinesterase inhibitors: register-based study of over 700,000 elderly patients. Drugs Aging 25:871–877
Carnahan RM, Lund BC, Perry PJ et al (2004) The concurrent use of anticholinergics and cholinesterase inhibitors: rare event or common practice? J Am Geriatr Soc 52(12):2082–2087
Modi A, Weiner M, Craig BA et al (2009) Concomitant use of anticholinergics with acetylcholinesterase inhibitors in Medicaid recipients with dementia and residing in nursing homes. J Am Geriatr Soc 57(7):1238–1244. doi:10.1111/j.1532-5415.2009.02258.x
Gill SS, Mamdani M, Naglie G et al (2005) A prescribing cascade involving cholinesterase inhibitors and anticholinergic drugs. Arch Intern Med 165(7):808–813
Lu CJ, Tune LE (2003) Chronic exposure to anticholinergic medications adversely affects the course of Alzheimer disease. Am J Geriatr Psychiatry 11(4):458–461
Sink KM, Thomas J 3rd, Xu H et al (2008) Dual use of bladder anticholinergics and cholinesterase inhibitors: long-term functional and cognitive outcomes. J Am Geriatr Soc 56(5):847–853. doi:10.1111/j.1532-5415.2008.01681.x
Chew ML, Mulsant BH, Pollock BG (2005) Serum anticholinergic activity and cognition in patients with moderate-to-severe dementia. Am J Geriatr Psychiatry 13(6):535–538
Cancelli I, Valentinis L, Merlino G et al (2008) Drugs with anticholinergic properties as a risk factor for psychosis in patients affected by Alzheimer’s disease. Clin Pharmacol Ther 84(1):63–68
Cancelli I, Beltrame M et al (2009) Valente M Drugs with anticholinergic properties: cognitive and neuropsychiatric side-effects in elderly patients. Neurol Sci 30(2):87–92. doi:10.1007/s10072-009-0033-y
Lechevallier-Michel N, Molimard M, Dartigues JF et al (2005) Drugs with anticholinergic properties and cognitive performance in the elderly: results from the PAQUID Study. Br J Clin Pharmacol 59(2):143–151
Cao YJ, Mager DE, Simonsick EM et al (2008) Physical and cognitive performance and burden of anticholinergics, sedatives, and ACE inhibitors in older women. Clin Pharmacol Ther 83(3):422–429
Ancelin ML, Artero S, Portet F et al (2006) Non-degenerative mild cognitive impairment in elderly people and use of anticholinergic drugs: longitudinal cohort study. BMJ 332(7539):455–459
Bottiggi KA, Salazar JC, Yu L et al (2006) Long-term cognitive impact of anticholinergic medications in older adults. Am J Geriatr Psychiatry 14(11):980–984
Campbell NL, Boustani MA, Lane KA et al (2010) Use of anticholinergics and the risk of cognitive impairment in an African American population. Neurology 75(2):152–159. doi:10.1212/WNL.0b013e3181e7f2ab
Jessen F, Kaduszkiewicz H, Daerr M et al (2010) Anticholinergic drug use and risk for dementia: target for dementia prevention. Eur Arch Psychiatry Clin Neurosci 260(Suppl 2):S111–S115. doi:10.1007/s00406-010-0156-4
Carrière I, Fourrier-Reglat A, Dartigues JF et al (2009) Drugs with anticholinergic properties, cognitive decline, and dementia in an elderly general population: the 3-city study. Arch Intern Med 169(14):1317–1324. doi:10.1001/archinternmed.2009.229
Fox C, Richardson K, Maidment ID et al (2011) Anticholinergic medication use and cognitive impairment in the older population: the medical research council cognitive function and ageing study. J Am Geriatr Soc 59(8):1477–1483. doi:10.1111/j.1532-5415.2011.03491.x
Pasina L, Djade CD, Lucca U et al (2013) Association of anticholinergic burden with cognitive and functional status in a cohort of hospitalized elderly: comparison of the anticholinergic cognitive burden scale and anticholinergic risk scale: results from the REPOSI study. Drugs Aging 30(2):103–112. doi:10.1007/s40266-012-0044-x
Gray SL, Anderson ML, Dublin S et al (2015) Cumulative use of strong anticholinergics and incident dementia: a prospective cohort study. JAMA Intern Med. doi:10.1001/jamainternmed.2014.7663
Han L, Agostini JV, Allore HG (2008) Cumulative anticholinergic exposure is associated with poor memory and executive function in older men. J Am Geriatr Soc 56:2203–2210
Kersten H, Molden E, Willumsen T et al (2013) Higher anticholinergic drug scale (ADS) scores are associated with peripheral but not cognitive markers of cholinergic blockade. Cross sectional data from 21 Norwegian nursing homes. Br J Clin Pharmacol 75:842–849
Fleminger S (2002) Remembering delirium. Br J Psychiatry 180:4–5
Alagiakrishnan K, Wiens CA (2004) An approach to drug induced delirium in the elderly. Postgrad Med J 80(945):388–393
Lauretani F, Ceda GP, Maggio M et al (2010) Capturing side-effect of medication to identify persons at risk of delirium. Aging Clin Exp Res. 22(5–6):456–458
Zimmerman KM, Salow M, Skarf LM et al (2014) Increasing anticholinergic burden and delirium in palliative care inpatients. Palliat Med 28(4):335–341
Best O, Gnjidic D, Hilmer SN et al (2013) Investigating polypharmacy and drug burden index in hospitalised older people. Intern Med J. 43(8):912–918. doi:10.1111/imj.12203
Campbell N, Perkins A, Hui S et al (2011) Association between prescribing of anticholinergic medications and incident delirium: a cohort study. Am Geriatr Soc 59(Suppl 2):S277–S281. doi:10.1111/j.1532-5415.2011.03676.x
Luukkanen MJ, Uusvaara J, Laurila JV et al (2011) Anticholinergic drugs and their effects on delirium and mortality in the elderly. Dement Geriatr Cogn Dis Extra 1(1):43–50
van Munster BC, Thomas C, Kreisel SH et al (2012) Longitudinal assessment of serum anticholinergic activity in delirium of the elderly. J Psychiatr Res 46(10):1339–1345
Watne LO, Hall RJ, Molden E et al (2014) Anticholinergic activity in cerebrospinal fluid and serum in individuals with hip fracture with and without delirium. J Am Geriatr Soc 62(1):94–102. doi:10.1111/jgs.12612
Kallin K, Gustafson Y, Sandman PO et al (2004) Drugs and falls in older people in geriatric care settings. Aging Clin Exp Res 16(4):270–276
Sylliaas H, Selbaek G, Bergland A (2012) Do behavioral disturbances predict falls among nursing home residents? Aging Clin Exp Res 24(3):251–256
Stenhagen M, Nordell E, Elmståhl S (2013) Falls in elderly people: a multifactorial analysis of risk markers using data from the Swedish general population study ‘Good ageing in Skåne’. Aging Clin Exp Res 25(1):59–67. doi:10.1007/s40520-013-0015-z
Berdot S, Bertrand M, Dartigues JF et al (2009) Inappropriate medication use and risk of falls-a prospective study in a large community-dwelling elderly cohort. BMC Geriatr 23(9):30. doi:10.1186/1471-2318-9-30
Fraser LA, Adachi JD, Leslie WD et al (2014) Effect of anticholinergic medications on falls, fracture risk, and bone mineral density over a 10-year period. Ann Pharmacother 48(8):954–961
Nishtala PS, Narayan SW, Wang T et al (2014) Associations of drug burden index with falls, general practitioner visits, and mortality in older people. Pharmacoepidemiol Drug Saf 23(7):753–758. doi:10.1002/pds.3624
Dauphinot V, Faure R, Omrani S et al (2014) Exposure to anticholinergic and sedative drugs, risk of falls, and mortality: an elderly inpatient, multicenter cohort. J Clin Psychopharmacol 34(5):565–570
Landi F, Dell’Aquila G, Collamati A et al (2014) Anticholinergic drug use and negative outcomes among the frail elderly population living in a nursing home. J Am Med Dir Assoc. doi:10.1016/j.jamda.2014.08.002
Wilson NM, Hilmer SN, March LM et al (2011) Associations between drug burden index and falls in older people in residential aged care. J Am Geriatr Soc 59(5):875–880. doi:10.1111/j.1532-5415.2011.03386.x
Murphy MP, Carmine H, Kolakowsky-Hayner S (2014) Modifiable and nonmodifiable risk factors for falls after traumatic brain injury: an exploratory investigation with implications for medication use. S Rehabil Nurs 39(3):113–122. doi:10.1002/rnj.89
Aizenberg D, Sigler M, Weizman A et al (2002) Anticholinergic burden and the risk of falls among elderly psychiatric inpatients: a 4-year case- control study. Int Psychogeriatr 14(3):307–310
Landi F, Russo A, Liperoti R et al (2007) Impact of inappropriate drug use on physical performance among a frail elderly population living in the community. Eur J Clin Pharmacol 63(8):791–799 Epub 2007 Jun 14
Lowry E, Woodman RJ, Soiza RL et al (2011) Associations between the anticholinergic risk scale score and physical function: potential implications for adverse outcomes in older hospitalized patients. J Am Med Dir Assoc 12(8):565–572. doi:10.1016/j.jamda.2011.03.006 Epub 2011 Apr 21
Bostock CV, Soiza RL, Mangoni AA (2013) Associations between different measures of anticholinergic drug exposure and Barthel Index in older hospitalized patients. Ther Adv Drug Saf. 4(6):235–245. doi:10.1177/2042098613500689
Koshoedo S, Soiza RL, Purkayastha R et al (2012) Anticholinergic drugs and functional outcomes in older patients undergoing orthopaedic rehabilitation. Am J Geriatr Pharmacother 10(4):251–257. doi:10.1016/j.amjopharm.2012.06.003
Mangoni AA, van Munster BC, Woodman RJ et al (2013) Measures of anticholinergic drug exposure, serum anticholinergic activity, and all-cause postdischarge mortality in older hospitalized patients with hip fractures. Am J Geriatr Psychiatry 21(8):785–793. doi:10.1016/j.jagp.2013.01.012
Kidd AC, Musonda P, Soiza RL et al (2014) The relationship between total anticholinergic burden (ACB) and early in-patient hospital mortality and length of stay in the oldest old aged 90 years and over admitted with an acute illness. Arch Gerontol Geriatr 59(1):155–161. doi:10.1016/j.archger.2014.01.006 Epub 2014 Feb 5
Narbey D, Jolly D, Mahmoudi R et al (2013) Relationship between anticholinergic drug use and one-year outcome among elderly people hospitalized in medical wards via emergency department: the SAFES cohort study. J Nutr Health Aging. 17(9):766–771. doi:10.1007/s12603-013-0349-4
Uusvaara J, Pitkala KH, Kautiainen H et al (2011) Strandberg TE Association of anticholinergic drugs with hospitalization and mortality among older cardiovascular patients: a prospective study. Drugs Aging 28(2):131–138. doi:10.2165/11585060-000000000-00000
Kumpula EK, Bell JS, Soini H et al (2011) Anticholinergic drug use and mortality among residents of long-term care facilities: a prospective cohort study. J Clin Pharmacol 51(2):256–263. doi:10.1177/0091270010368410
Salahudeen MS, Duffull SB, Nishtala PS (2014) Impact of anticholinergic discontinuation on cognitive outcomes in older people: a systematic review. Drugs Aging 31(3):185–192. doi:10.1007/s40266-014-0158-4
Drimer T, Shahal B, Barak Y (2004) Effects of discontinuation of long-term anticholinergic treatment in elderly schizophrenia patients. Int Clin Psychopharmacol 19(1):27–29
Molloy DW, Brooymans M (1988) Anticholinergic medications and cognitive function in the elderly. J Clin Exp Gerontol 10:89–98
Tollefson GD, Montague-Clouse J, Lancaster SP (1991) The relationship of serum anticholinergic activity to mental status performance in an elderly nursing home population. J Neuropsychiatry Clin Neurosci 3:314–319
Kersten H, Molden E, Tolo IK et al (2012) Cognitive effects of reducing anticholinergic drug burden in a frail elderly population: a randomized controlled trial. J Gerontol A Bio Sci Med Sci 68:271–278
Yeh YC, Liu CL, Peng LN et al (2013) Potential benefits of reducing medication-related anticholinergic burden for demented older adults: a prospective cohort study. Geriatr Gerontol Int 13(3):694–700. doi:10.1111/ggi.12000
Gnjidic D, Le Couteur DG, Abernethy DR et al (2010) A pilot randomized clinical trial utilizing the drug burden index to reduce exposure to anticholinergic and sedative medications in older people. Ann Pharmacother 44:1725–1732
Fick DM, Cooper JW, Wade WE et al (2003) Updating the Beers criteria for potentially inappropriate medication use in older adults: results of a US consensus panel of experts. Arch Intern Med. 163(22):2716–2724
Gallagher P, Ryan C, Byrne S et al (2008) STOPP (screening tool of older person’s prescriptions) and START (screening tool to alert doctors to right treatment). Consensus validation. Int J Clin Pharmacol Ther 46(2):72–83
Ponticelli C, Sala G, Glassock RJ (2015) Drug management in the elderly adult with chronic kidney disease: a review for the primary care physician. Mayo Clin Proc. doi:10.1016/j.mayocp.2015.01.016
Conflict of interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Human and animal rights
All procedures performed in studies which involved human participants carried out by any of the authors were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the studies carried out by any of the authors when required.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Collamati, A., Martone, A.M., Poscia, A. et al. Anticholinergic drugs and negative outcomes in the older population: from biological plausibility to clinical evidence. Aging Clin Exp Res 28, 25–35 (2016). https://doi.org/10.1007/s40520-015-0359-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40520-015-0359-7