
Abstract
Background and aims
For older adults, an Emergency Department (ED) visit represents a period of vulnerability that extends beyond the visit itself. This study aimed to determine the impact of the role of caregiver, and geriatric conditions of patients on early unplanned rehospitalization (EUR) within 3 months after an ED visit.
Methods
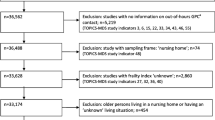
This prospective longitudinal experimental study included consecutively 173 patients aged 75 and older admitted in an ED over a 2-week period (18.7 % of the total visits). Only older patients having a caregiver were analyzed (78.0 %, n = 135). Medical conditions and a comprehensive geriatric assessment were recorded for each patient. All caregivers were interviewed about their tasks and emotional impact using the short Zarit Burden Inventory. Three months after, patients or their caregivers were called about the vital status, and EUR of patients.
Results
Among the patients included, 64.2 % had an EUR and 28.9 % of their caregivers reported a high level of burden. EUR was strongly associated with a high caregiver burden (OR 8.7, 95 % CI 1.5–49.8). No association was found for patient’s medical or geriatric status. Caregivers reported a significantly high burden when patients were malnourished, or were at risk of adverse health outcomes based on the ISAR scale, and when they had greater disabilities in IADLs and ADLs, or cognitive impairments.
Conclusions
Many hospital readmissions after an ED visit may be preventable by identifying caregiver’s high burden. Reasons that lead to this high burden should be checked at the first visit.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
With the aging populations in western countries, more and more caregivers need to cope with older relatives, most of whom suffer from chronic diseases or terminal illness. In 2011, a French national survey established that nearly 80 % of older persons living at home had regular care from close relatives, and 69 % had a single caregiver [1].
Most studies on caregivers focus on older persons with chronic diseases such as dementia, stroke or cancer [2–5], or who receive end-of-life caregiving [6]. Only recently, caregiver burden or poor health is considered as a predictive factor of poor outcome or associated with poor quality of life for the caregiver and care recipient [2, 6–8]. ED admissions of older patients are currently increasing in developed countries, accounting for approximately 20 % of all ED visits [9]. Older people with atypical symptoms and/or multiple comorbidities are at high risk of ED readmission, unplanned hospitalization or death [10, 11]. Thus, several assessment tools have been developed to identify older patients at risk for adverse outcomes after an ED visit or early unplanned hospitalization (EUR) [12]. However, none of them includes social items related to living conditions at the time of the ED visits, while some ED visits are indeed motivated by their social situation [13]. However, few studies focus on the impact of the patient’s environment leading to the ED visit and adverse outcomes. The “SAFE” study included only older patients hospitalized after an ED visit and focused on the patient’s health and living conditions, but caregivers and their characteristics contributing to readmission after an ED visit were not studied [14, 15].
In routine clinical practice, measuring caregiver burden at the time of the ED visit of the care recipient could be a relevant variable for the ED care of older patients and adverse health outcomes after their discharge. We hypothesized that a high caregiver burden is associated with adverse patient outcome and EUR in particular. Thus, we conducted a longitudinal study to better understand the impact of caregiver burden on the EUR and the determinants of caregiver burden.
Methods
Study design and population
This secondary data analysis used the database of a previous study conducted in an older population admitted to the ED with a 3-months follow-up [16]. In the previous study, we conducted a prospective cohort study in the ED of Sainte Marguerite Hospital in Marseille, France. Baseline data (T1) were obtained from June 2, 2009, to June 16, 2009, and one survey was conducted 3 months after the ED visit (T3). This previous study considered only patients aged 75 years and older who were consecutively admitted to the ED between 8 a.m. and 12 p.m., regardless of their chief complaint (n = 157) [16].
For the purpose of the present study, only older patients who came with a caregiver were analyzed, as defined by Van Durme et al. (“the person who spends most of the time with the elder and/or from whom the older person declares that he/she is his/her main informal caregiver, for care or support of care”) [17].
Informed consent was required to enter the study by each willing patient or their caregiver. Patients and caregivers could refuse to take part in the study or to withdraw from it at any time. This study was approved by two national authorities, the Advisory Committee on Health Research Information (“Comité Consultatif sur le Traitement de l’Information en matière de Recherche dans le domaine de la Santé”) and the National Commission on Informatics and Freedom (“Commission Nationale Informatique et Liberté”) [18].
Data collection and measurements
The study was conducted in two steps. First, upon ED admission, four trained geriatric physicians who were independent from ED usual care interviewed older patients and their caregivers with a face-to-face questionnaire (T1). Second, all older patients or their caregivers were called 3 months later (T3).
Assessment of caregivers
At baseline, information on age, sex, marital status, employment, relationship to the patient, and self-reported number of hours per week caring for the patient was collected about the primary caregiver. Caregiver tasks were identified according to previous survey [16] providing transportation, preparing meals, shopping, doing chores, managing business, legal, and financial matters, and dressing/bathing the patient. These tasks were scored as yes (1)/no (0).
Emotional impact on the primary caregiver was evaluated by the French Short version of the Zarit Burden Inventory (ZBI) [19], with two added questions: “Do you feel like you are having more difficulty than usual in providing care to the patient?” and “Have you recently experienced a stressful event?”. The ZBI is one of the most widely used instruments to assess caregiving burden and consists of 40 questions originally designed to evaluate five broad aspects of caregiver burden in caregivers of patients with dementia [20, 21]. The ZBI short form (ZBI-SF) is extensively validated for measuring the impact of informal caregiving in the older population [22]. This scale includes 7 questions measuring potential stress (e.g., emotional distress and overall burden) answered on a 3-point Likert scale. The items were scored 0 (never), 0.5 (sometimes) and almost always (1), and added to give a total score ranging from 0 to 7. For analytical purposes, a dichotomous variable of high burden was created, defined as a score above the 75th percentile (moderate to very high burden, score >3).
Assessment of older patients
Information on patient age, sex, marital status, living situation, social support and ED visit circumstances was collected, and a comprehensive geriatric assessment was carried out [16]. The patient initial assessment consisted of:
-
1.
The Cumulative Illness Rating Scale in Geriatrics (CIRS-G) to measure comorbidities. Each of the 14 body systems is scored from 0 (no impairment) to 4 (extremely severe), calculated by the total score (0–56) [23, 24],
-
2.
The Identification of Seniors At Risk (ISAR), a 6-item self-report questionnaire with a yes/no response. This screening tool identifies ED older patients at risk of subsequent functional decline (total scale range of 0–6 with risk of functional decline defined as a score ≥3) [25];
-
3.
A standardized geriatric assessment including:
-
The nutritional status using the Mini Nutritional Assessment Short Form (MNA-SF), a 6-item questionnaire. Scores are defined as malnutrition (score ≤7/14 defined malnutrition [26]);
-
the occurrence of any fall in the previous year
-
depression using the Mini Geriatric Depression Scale (Mini-GDS), a 4-item yes/no self-rating scale (ranging from 0 to 4), with a cut-off score of 1 defining the risk of depression [27];
-
cognitive or behavioral status assessed by geriatric physicians;
-
current medications (number of medications per day);
-
dependency assessed by
-
the Katz’s Activities of Daily Living (ADL) scale (with dependency defined as the inability to perform bathing, toileting, feeding, dressing, continence, and transferring, each item assessed on a 3-point scale: independent (1 point), partially dependent (0.5 point), and fully dependent (0), with a total range of 0–6; dependent status defined as a score ≤3 [28, 29];
-
the Instrumental Activities of Daily Living (IADL) scale to assess the ability to perform four activities including finances, taking medications, using the telephone and transportation [4-item scale, where each item was assessed on a 2-point scale: independent (1 point) and partially or fully dependent (0 point); dependent status defined as a score ≤3] [30].
-
-
Follow-up and outcome assessments
Three months after the ED visit (T3), two trained research assistants called all patients included at T0, or their caregivers. This assessment explored vital status (death/alive) and EUR within 3 months after the ED visit.
Statistical analysis
Data were analyzed on Spss 20.0 using proportions or means, and standard deviations of all variables. Two univariate analyses were performed using the Chi-square test for binomial and ordinal variables, and the Student’s t test for continuous variables. First, we examined the strength of the association between independent variables and the caregiver burden, and secondly, the strength of the association between independent variables and the EUR.
Multivariable analysis by logistic regression was performed to identify factors significantly associated with EUR of older patients within 3 months after the ED visit. Significant variables from the univariate analyses were selected using a forward stepwise (likelihood ratio) method, with the level of significance set at 0.20 for addition of the variable to predict the outcome. p values, adjusted odds ratios and 95 % confidence levels were reported to determine the strength of contribution from each predictor towards EUR of older patients within 3 months after the ED visit. For all analyses, tables show only variables with p value <0.20.
Results
Out of the 173 patients aged 75 and older admitted to the ED (18.7 % of all 924 ED visits during the study period), 135 patients identified a primary caregiver (78 % of the study population). Patients with or without caregivers did not differ on sociodemographic and environmental characteristics.
Older patient characteristics
Description of patients’ characteristics is summarized in Table 1. Out of the 135 older patients admitted to the ED, 57 % were female and the mean age was 83.8 ± 5.4 years old, and 45.2 % of patients were aged 85 years and over. Older patients had several comorbidities with a CIRS-G mean total score of 10.1 ± 6.1; 71.2 % of the patients were affected by more than three comorbidities. Also, depression was diagnosed in 52.6 % of all patients. Patients took a mean of 5.9 ± 3.5 medications per day. At the time of admission, nearly 68.9 % were dependent according to the IADL scale and 70.4 % according to the ADL scale, and 68.1 % were at high risk of subsequent functional decline (ISAR). Overall, 28.1 % of patients were malnourished according to the nutritional assessment using the MNA-SF (average total score of 9.1 ± 2.8).
Caregiver burden
Characteristics of the 135 caregivers are summarized in Table 1. Out of the 135 caregivers, 48.1 % were younger than 60 years, 21.5 % were 75 years and older.
Table 1 also shows the frequency and percentages of the items with the answer modalities “sometimes” and “almost always”. The items 3, 5 and 6 were the most frequently cited, even if we only analyzed the answers with the modality “almost always “.
In our caregiver population, ZBI-SF total score ranged from 0 (no burden) to 7 (intense burden). The average global score of burden using the ZBI-SF was 2.3 ± 1.8, with a median score of 2. Among the 135 caregivers, 28.9 % had a ZBI-SF score at the upper quartile (score >3), with mean score of 4.7 ± 1.1 versus 1.3 ± 0.9 for those with a score ≤3 (low burden).
A higher burden was more frequent for women caregivers; for those making specific tasks (preparing the meals and taking care of home chores), when the number of tasks increased; when caregivers had a recent personal stressful event; and when they felt higher difficulties for caring their relative (p < 0.05) (Table 2). However, burden was not associated with the caregiver’s age, marital status, employment status, relationship to patient, and the week duration of caregiving.
According to the patient’s health status at the ED admission (T1), caregivers reported a significantly high burden when patients were malnourished, when they were at risk of adverse health outcomes based on the ISAR scale, when they had greater disabilities in IADLs and ADLs, or cognitive impairments (p < 0.05) (Table 2). There were not differences related with some characteristics of the patients: age, sex, living environment, comorbidities (CIRS-G), depression (Mini-GDS) and polymedication.
At 3 months of after the ED visit
At 3 months of follow-up, 87 older patients (64.4 %) had an EUR, 22 of them died (16.3 %).
By univariate analysis (Table 3), EUR patients were more likely malnourished and had disabilities in ADLs (p < 0.05). Moreover, EUR within the 3 months was significantly associated with caregiver high burden (p < 0.05). The demographic profile of the caregiver was not significantly associated with EUR, only the score Zarit and the component items 1 and 2 were associated.
In our previous article [16], we identified two factors associated with the occurrence of “death”: malnutrition [Odds ratio (OR) 20.2, 95 % confidence interval (CI) 95 % 5.74–71.35] and comorbidities (OR 1.1, CI 95 % 1.01–1.22 for at least one comorbidity at level 2 severity).
Among the EUR patients, caregiver high burden was similar between those who died and those who were still alive at 3 months (36.4 % deceased versus 36.9 % alive, p = 0.59).
In multivariate analysis, we tested older patients and caregivers characteristics including the caregiver burden potentially associated to EUR. A high caregiver burden was the only independent predictive factor positively associated with older patients’ EUR (OR 8.7, 95 % CI 1.5–49.8).
Discussion
This study aimed to demonstrate the predictive factors that lead older patients to EUR taking into account not only the patient medical and geriatric status, but also with the aspect of the caregiver characteristics and burden. All of these patients had an ED visit with their caregivers in the previous 3 months. Our main result showed that a high caregiver burden is a determinant predictive factor of EUR. Malnutrition and disability on the ADL were also associates with a higher rate of EUR but disappeared in the multivariate analysis as these two variables were also associated to a high caregiver burden. Most of the studies about caregiver burden were conducted in specific chronic and stressful medical conditions as dementia [2, 31, 32], cancer [4] or advance illness [7] with specific programs to improve their burden [33]. But very few studies about caregiver burden were conducted in older patients with usual complex medical conditions. In our study, we purposefully included all older patients who were consecutively admitted in ED, independently from their chronic diseases and chief complaints to try to be close to real-life conditions of ED admissions. Although our study was monocentric with a small sample size, our patients are representative of the older population usually admitted in ED [10, 11].
Our results about caregiver burden showed no association between usual comorbid conditions assessed by the CIRS-G and the caregiver burden, contrary to the literature, but an association between complex care needs and high caregiver burden has been highlighted [7]. Indeed, geriatric conditions and particularly functional disability and malnutrition were associated to a high burden. Moreover, most of the older patients were at risk of adverse outcomes according to the ISAR score; this rate was higher when the caregiver reported a high burden. And at the same time, the majority of caregivers were afraid about the future holds of their relatives [34].
Sometimes, given the lack of specific complaints, ED visits by older people seem to be a “sentinel event” reflecting often insufficient environmental/social support [9] or may reflect a serious medical problem related to a social problem [35]. Our results suggest that a greater attention to the caregiver burden at the time of a first ED visit of the patient could have a positive effect on the patient medical use. In a busy ED, nurses and physicians tend to underestimate the lack of social support. Yet, some of the early rehospitalizations are consequences of a previous hospitalization with unplanned discharge [34].
Because of time constraints, health ED professionals usually neglect the interview of the caregiver. Yet, among the old patients admitted in the ED during the study period, most of them had a caregiver reflecting their involvement in the care of their patients. Despite the small sample size, our caregiver’s characteristics were similar to those reported in the literature [36, 37]. Nearly half of our caregiver was less than 60-year old, that is they were mainly children of the elders; and more than 40 % of our caregivers were still working. These characteristics reflect what is called the “parent sandwich” generation, who take care of their older parents and of their children or grand children” [38] with specific needs and multiple care involvements that increase the risk of burden.
In addition to the complex care needs related to the medical condition of the older patient, we identified some relevant variables that were associated to burden caregiver, such as recent stressful events, the number of tasks and specific tasks as preparing meals or doing the home cores. We did not assess the caregiver’s quality of life, neither their health status which time consuming and hardly feasible in ED. This could have helped in the interpretation of the determinants of the burden even if a recent review showed a lower mortality in caregivers compared to non-caregivers [8].
More than half of the caregivers reported an adverse effect of the caring on their personal health. Indeed, according to the literature, a high burden is associated to a higher risk of physical fatigue, depression or anxiety [39–41]. This should also be checked with the caregiver at the time of admission to elicit further information and design a social or health plan for patients. Moreover, the caregiver with a high level of burden should be monitored for depressive symptoms [41].
But caregiving is a complex personal situation and two-thirds of our caregivers felt no high burden caring their relative. In fact, caregiving can also be associated with positive aspects, as when the caregiver feels a high self-efficacy [42], an enhanced relationship with the care-receiver, the feeling of being rewarded, a sense of personal growth, and a perception of personal satisfaction which are associated with a better quality of life for the caregiver [43].
Our results raise the question of the optimal orientation after an ED visit for these patients. If specific programs have been developed for the caregivers in specific disease (i.e. dementia), or psychosocial programs to relieve the burden of informal caregivers [44], this is not yet generalized in general older population despite the increasing number of older patients. In other words, old patients medical conditions should be completed with a comprehensive geriatric assessment and a measure of a high caregiver burden and its determinants. This could lead to a personal intervention plan established before patient ED discharge. Interventions should include family education, and communication between healthcare workers and family [34]. Of course, looking for all of these aspects and perspectives is unfeasible during the ED visit; but a prescreening at the time of admission could help to better target patients and caregivers that need more complete socio-environmental investigation to geriatrician (mobile team, consultation or geriatric wards).
The efficiency of this organization in hierarchy (screening, diagnosis, personal plan) including family and caregivers should be tested in further studies.
Conclusion
For older adults, an ED visit represents a period of extreme vulnerability that extends beyond the visit itself. The occurrence of early rehospitalization within 3 months after the ED visit underscores broader problems in the health system’s ability to meet the needs of older adults and their caregivers, as well as the importance of the ED in identifying those needs to refer the patient to the appropriate service. Many hospital readmissions after an ED visit may be preventable. Additional efforts by ED healthcare professionals must be performed to screen for caregiver burden and identify its determinants to better refer the patient to the appropriate service and/or better planned the hospital discharge.
References
Soullier N, Weber A (2011) L’implication de l’entourage et des professionnels auprès des personnes âgées à domicile. Etudes et résultats. http://www.drees.sante.gouv.fr/l-implication-de-l-entourage-et-des-professionnels-aupres-des-personnes-agees-a-domicile,9279.html. Accessed 26 Feb 2014
Thomas P, Ingrand P, Lalloue F, Hazif-Thomas C, Billon R, Viéban F, Clément JP (2004) Reasons of informal caregivers for institutionalizing dementia patients previously living at home: the Pixel study. Int J Geriatr Psychiatry 19:127–135 [PubMed:14758578]
Takai M, Takahashi M, Iwamitsu Y, Ando N, Okazaki S, Nakajima K, Oishi S, Miyaoka H (2009) The experience of burnout among home caregivers of patients with dementia: relations to depression and quality of life. Arch Gerontol Geriatr 49:e1–e5. doi:10.1016/j.archger.2008.07.002
Bevans M, Sternberg EM (2012) Caregiving burden, stress, and health effects among family caregivers of adult cancer patients. JAMA 307:398–403. doi:10.1001/jama.2012.29
Visser-Meily JM, Post MW, Riphagen II, Lindeman E (2004) Measures used to assess burden among caregivers of stroke patients: a review. Clin Rehabil 18:601–623 [PubMed:15473113
McGuire DB, Grant M, Park J (2012) Palliative care and end of life: the caregiver. Nurs Outlook 60:351–356. doi:10.1016/j.outlook.2012.08.003
Garlo K, O’Leary JR, Van Ness PH, Fried TR (2010) Burden in caregivers of older adults with advanced illness. J Am Geriatr Soc 58:2315–2322. doi:10.1111/j.1532-5415.2010.03177.x
Vlachantoni A, Evandrou M, Falkingham J, Robards J (2013) Informal care, health and mortality. Maturitas 74:114–118. doi:10.1016/j.maturitas.2012.10.013
Samaras N, Chevalley T, Samaras D, Gold G (2010) Older patients in the emergency department: a review. Ann Emerg Med 56:261–269. doi:10.1016/j.annemergmed.2010.04.015
Ballabio C, Bergamaschini L, Mauri S, Baroni E, Ferretti M, Bilotta C, Vergani C (2008) A comprehensive evaluation of elderly people discharged from an Emergency Department. Intern Emerg Med 3(245–9):18. doi:10.1007/s11739-008-0151-1
Aminzadeh F, Dalziel WB (2002) Older adults in the emergency department: a systematic review of patterns of use, adverse outcomes, and effectiveness of interventions. Ann Emerg Med 39:238–247 [PubMed:11867975]
Bissett M, Cusick A, Lannin NA (2013) Functional assessments utilised in emergency departments: a systematic review. Age Ageing 42:163–172. doi:10.1093/ageing/afs187
Rutschmann OT, Chevalley T, Zumwald C, Luthy C, Vermeulen B, Sarasin FP (2005) Pitfalls in the emergency department triage of frail elderly patients without specific complaints. Swiss Med Wkly 135:145–150 [PubMed:15832233]
Lanièce I, Couturier P, Dramé M, Gavazzi G, Lehman S, Jolly D, Voisin T, Lang PO, Jovenin N, Gauvain JB, Novella JL, Saint-Jean O, Blanchard F (2008) Incidence and main factors associated with early unplanned hospital readmission among French medical inpatients aged 75 and over admitted through emergency units. Age Ageing 37:416–422. doi:10.1093/ageing/afn093
Dramé M, Lang PO, Novella JL, Narbey D, Mahmoudi R, Lanièce I, Somme D, Gauvain JB, Heitz D, Voisin T, de Wazières B, Gonthier R, Ankri J, Saint-Jean O, Jeandel C, Couturier P, Blanchard F, Jolly D (2012) Six-month outcome of elderly people hospitalized via the emergency department: the SAFES cohort. Rev Epidemiol Sante Publique 60:189–196. doi:10.1016/j.respe.2011.11.004
Gentile S, Lacroix O, Durand AC, Cretel E, Alazia M, Sambuc R, Bonin-Guillaume S (2013) Malnutrition: a highly predictive risk factor of short-term mortality in elderly presenting to the emergency department. J Nutr Health Aging 17:290–294. doi:10.1007/s12603-012-0398-0
Van Durme T, Macq J, Jeanmart C, Gobert M (2012) Tools for measuring the impact of informal caregiving of the elderly: a literature review. Int J Nurs Stud 49:490–504. doi:10.1016/j.ijnurstu.2011.10.011
Commission Nationale de l’Informatique et des Libertés (2012). http://www.cnil.fr/vos-responsabilites/declarer-un-fichier/. Accessed 31 Jan 2012
Revel Da Rocha V, Harit Chabalet I, Kervinio C et al (2002) Construction d’une échelle simplifiée pour la détection en médecine générale du fardeau de l’aidant d’une personne âgée dépendante. L’année gérontologique. vol 16, Tome 1
Zarit SH, Reever KE, Bach-Peterson J (1980) Relatives of the impaired elderly: correlates of feelings of burden. Gerontologist 20:649–655
Zarit SH, VandenBos GR (1990) Effective evaluation of memory in older persons. Hosp Community Psychiatry 41(9–10):16 [PubMed: 2403966]
Higginson IJ, Gao W, Jackson D, Murray J, Harding R (2010) Short-form Zarit Caregiver Burden Interviews were valid in advanced conditions. J Clin Epidemiol 63:535–542. doi:10.1016/j.jclinepi.2009.06.014
Parmelee PA, Thuras PD, Katz IR, Lawton MP (1995) Validation of the Cumulative Illness Rating Scale in a geriatric residential population. J Am Geriatr Soc 43:130–137 [PubMed:7836636]
Salvi F, Miller MD, Grilli A, Giorgi R, Towers AL, Morichi V, Spazzafumo L, Mancinelli L, Espinosa E, Rappelli A, Dessì-Fulgheri P (2008) A manual of guidelines to score the modified cumulative illness rating scale and its validation in acute hospitalized elderly patients. J Am Geriatr Soc 56:1926–1931. doi:10.1111/j.1532-5415.2008.01935.x
McCusker J, Bellavance F, Cardin S, Trepanier S, Verdon J, Ardman O (1999) Detection of older people at increased risk of adverse health outcomes after an emergency visit: the ISAR screening tool. J Am Geriatr Soc 47:1229–1237 [PubMed:10522957]
Kaiser MJ, Bauer JM, Ramsch C, Uter W, Guigoz Y, Cederholm T, Thomas DR, Anthony P, Charlton KE, Maggio M, Tsai AC, Grathwohl D, Vellas B, Sieber CC, MNA-International Group (2009) Validation of the Mini Nutritional Assessment short-form (MNA-SF): a practical tool for identification of nutritional status. J Nutr Health Aging 13:782–788 [PubMed: 19812868]
Clément JP, Nassif RF, Léger JM, Marchan F (1997) Development and contribution to the validation of a brief French version of the Yesavage Geriatric Depression Scale. Encephale 23:91–99 [PubMed: 9264935]
Katz S, Ford AB, Moskowitz RW, Jackson BA, Jaffe MW (1963) Studies of illness in the aged. The index of ADL: a standardized measure of biological and psychosocial function. JAMA 185:914–919 [PubMed:14044222]
Collège National des enseignants de gériatrie, Module 5 (2010) Masson, Paris
Lawton MP, Brody EM (1969) Assessment of older people: self-maintaining and instrumental activities of daily living. Gerontologist 9:179–186 [PubMed:5349366]
Covinsky KE, Newcomer R, Fox P, Wood J, Sands L, Dane K, Yaffe K (2003) Patient and caregiver characteristics associated with depression in caregivers of patients with dementia. J Gen Intern Med 18:1006–1014 [PubMed:14687259]
Lilly MB, Robinson CA, Holtzman S, Bottorff JL (2012) Can we move beyond burden and burnout to support the health and wellness of family caregivers to persons with dementia? Evidence from British Columbia, Canada. Health Soc Care Community 20:103–112. doi:10.1111/j.1365-2524.2011.01025.x
De Rotrou J, Cantegreil I, Faucounau V, Wenisch E, Chausson C, Jegou D, Grabar S, Rigaud AS (2011) Do patients diagnosed with Alzheimer’s disease benefit from a psycho-educational programme for family caregivers? A randomised controlled study. Int J Geriatr Psychiatry 26:833–842. doi:10.1002/gps.2611
Bauer M, Fitzgerald L, Haesler E, Manfrin M (2009) Hospital discharge planning for frail older people and their family. Are we delivering best practice? A review of the evidence. J Clin Nurs 18:2539–2546. doi:10.1111/j.1365-2702.2008.02685.x
Durand AC, Gentile S, Devictor B, Palazzolo S, Vignally P, Gerbeaux P, Sambuc R (2011) ED patients: how nonurgent are they? Systematic review of the emergency medicine literature. Am J Emerg Med 29:333–345. doi:10.1016/j.ajem.2010.01.003
Soullier N (2012) L’aide humaine auprès des adultes à domicile : l’implication des proches et des professionnels. Etudes et Résultats. http://www.drees.sante.gouv.fr/IMG/pdf/er827.pdf. Accessed 26 Feb 2014
Guillemin P, Gauthier AM, Bret G, Gonthier R (2014) Caractéristiques des aidants ayant à charge un proche en perte d’indépendance sévère à domicile : enquête départementale auprès de 971 aidants. Revue de Gériatrie (La) 39:497–508
Künemund H (2006) Changing Welfare States and the “Sandwich Generation”: Increasing Burden for the Next Generation? Int J Ageing Later Life 1:11–29. Accessed 15 Jan 2014
Carretero S, Garcés J, Ródenas F, Sanjosé V (2009) The informal caregiver’s burden of dependent people: theory and empirical review. Arch Gerontol Geriatr 49:74–79. doi:10.1016/j.archger.2008.05.004
Soullier N (2012) Aider un proche à domicile: la charge ressentie. Etudes et Résultats, 799. http://www.drees.sante.gouv.fr/aider-un-proche-age-a-domicile-la-charge-ressentie,10861.html. Accessed 26 February 2014
Sherwood PR, Given CW, Given BA, von Eye A (2005) Caregiver burden and depressive symptoms: analysis of common outcomes in caregivers of elderly patients. J Aging Health 17:125–147 [PubMed:15750048]
Semiatin AM, O’Connor MK (2012) The relationship between self-efficacy and positive aspects of caregiving in Alzheimer’s disease caregivers. Aging Ment Health 16:683–688. doi:10.1080/13607863.2011.651437
Kate N, Grover S, Kulhara P, Nehra R (2013) Positive aspects of caregiving and its correlates in caregivers of schizophrenia: a study from north India. East Asian Arch Psychiatry 23:45–55 [PubMed:23807629]
Garcés J, Carretero S, Ródenas F, Alemán C (2010) A review of programs to alleviate the burden of informal caregivers of dependent persons. Arch Gerontol Geriatr 50:254–259. doi:10.1016/j.archger.2009.04.012
Conflicts of interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Ethical standards
This study involved human participants and has been approved by two national ethics committees, the Advisory Committee on Health Research Information (“Comité Consultatif sur le Traitement de l’Information en matière de Recherche dans le domaine de la Santé”) and the National Commission on Informatics and Freedom (“Commission Nationale Informatique et Liberté”) and performed in accordance with ethical standards.
Informed consent
All patients and their caregiver signed informed consent before inclusion to the procedure.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Bonin-Guillaume, S., Durand, AC., Yahi, F. et al. Predictive factors for early unplanned rehospitalization of older adults after an ED visit: role of the caregiver burden. Aging Clin Exp Res 27, 883–891 (2015). https://doi.org/10.1007/s40520-015-0347-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40520-015-0347-y