
Abstract
Introduction
Anorexia nervosa (AN) is a serious psychiatric disorder that is difficult to treat and often follows a protracted course. A number of theoretical models have been proposed for the etiology and maintenance of AN. Two domains that have received substantial attention in the literature on AN are affect and reward/punishment processes. However, despite an overlap in the nature and implications of these processes, studies of AN addressing these constructs have typically investigated them independently.
Purpose
The purpose of this narrative review is to integrate the literature on the role of affect, reward, and punishment in AN.
Method
We provide a focused narrative overview of the literature relating to the affect, reward, and punishment in AN via a synthesis of recent reviews and meta-analyses.
Results
We first describe several prominent affect and reward/punishment-based conceptualizations of AN, followed by a brief overview of the existing empirical literature in these domains.
Conclusion
We provide a critical discussion of the disparate nature of these literatures in AN, including associated limitations. We then conclude with an extensive discussion of directions for future research that integrate the study of affect and reward/punishment processes in AN.
Level of evidence
Level V, narrative review.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Anorexia nervosa (AN) is a serious psychiatric disorder characterized by restriction of energy intake resulting in significantly low body weight, fear of weight gain, and disturbances in body image [1]. There are two diagnostic subtypes of AN: AN-restricting subtype (AN-R) and AN-binge eating/purging subtype (AN-BP), with only the latter subtype involving recurrent binge eating and/or purging behavior [1]. AN is associated with severe medical complications and psychiatric comorbidities [2, 3], as well as high rates of mortality from suicide and medical complications [4, 5]. Despite the seriousness of AN, effective treatment options are lacking, particularly for adults, and there are high rates of premature treatment termination [6] which may be due in part to the ego-syntonic nature of the disorder. Elucidating the factors that are most relevant to the onset and/or maintenance of AN may aid in the development of more effective prevention and intervention programs.
The etiology of AN involves multiple intersecting biological, psychological, and sociocultural factors [7]. Of particular note, evidence from traditionally separate literatures within the eating disorder field suggests that both affect (i.e., the experience of emotion, either positively or negatively valenced) and reward/punishment (i.e., relating to the positive or negative value that one ascribes to a stimulus, associated with approach or avoidance behaviors, respectively) processes play a crucial role in the onset and maintenance of AN. However, despite an intrinsic link between affect and reward/punishment processes, studies of AN have typically examined these processes separately.
Purpose
The purpose of this review is to provide a narrative overview of research and theory on the role of these processes in AN, and to suggest directions for future research that integrate the study of affect and reward/punishment processes in AN.
Method
We first provide an overview of affect and reward/punishment processes, followed by a description of several prominent theories of AN that relate to these processes. As several recent qualitative and quantitative reviews separately address affect [8, 9] and reward/punishment [10,11,12] processes in AN, we provide a focused narrative summary of the literature in these domains via a synthesis of these recent reviews. We include any reviews or meta-analyses of affect, reward, or punishment in anorexia nervosa. Finally, we discuss the disparate nature of these literatures in AN, including associated limitations, and offer suggestions for future investigations that integrate the study of affect and reward/punishment processes in AN.
Overview of affect and reward/punishment
Broadly, affect encompasses the experience of emotion, which can be either positively or negatively valenced. Positive affect is conceptualized as a subjective experience of pleasant emotions, and is associated with reward-seeking behaviors [13]. Furthermore, high trait positive affect is associated with higher reward sensitivity (i.e., the degree to which rewards lead to positive emotion) [14]. In contrast, negative affect involves states such as fear and anxiety, and high trait negative affect is associated with high punishment sensitivity and avoidance behaviors [14].
The reward system is composed of three distinguishable components, all of which are interlinked with affect: the anticipation of reward (wanting), the consumption of reward (liking), and the learning of reward (learning) [15]. Wanting involves motivation, desire, or craving for reward [15]. Liking involves pleasure experienced during reward consumption [15], and most directly describes affect [16]. Learning involves the formulation of reward-based associations, which ultimately results in habit formation [15]. Pleasure experienced during the consumption of reward directly impacts learning, as individuals learn to continue engaging in behaviors that are pleasurable, and cease behaviors that are not pleasurable or are aversive.
As evidenced by the brief descriptions above, affect, reward, and punishment processes are not entirely distinct. Two core systems have been identified which incorporate these processes: (1) the approach system (i.e., the positive valence system), which motivates actions towards rewards and produces positive affective states, and (2) the avoidance system (i.e., the negative valence system), which motivates punishment avoidance and is linked with negative affective states [17]. It has been argued that positive affect and negative affect are self-reported dimensions of the behavioral approach and inhibition systems (BAS/BIS) [18]. Whereas negative affective states promote avoidance of punishment, positive affective states promote approach behaviors toward potential rewards [18]. For example, when an individual experiences positive affect, he/she is motivated to continue engaging in the activity that results in pleasure/reward, which result in further increases in positive affect [14]. Behavior intended to attain reward and avoid punishment is critical in regulating affect, with rewards and punishers eliciting corresponding emotions [19]. For example, receiving a reward (e.g., food) might result in an increase in positive affective states (e.g., pleasure). Similarly, the removal of punishment (e.g., a painful stimulus) might result in a decrease in negative affective states (e.g., fear).
Affect and reward/punishment-based theories of AN
Affect-based theories of AN
Several theories are focused primarily on the role of eating disorder behaviors in AN as a response to emotions, particularly those that are negatively valenced. For instance, the functional model of emotion avoidance in AN, similar in concept to Heatherton and Baumeister’s [20] escape theory of binge eating, proposes that individuals with AN tend to experience emotions as aversive and uncontrollable, prompting a desire to avoid the experience of these negative affective states. Individuals with AN learn that engaging in disordered eating symptoms can help facilitate such emotion avoidance [21]. Additionally, the transactional model of emotional dysregulation, originally developed for borderline personality disorder [22, 23] has been applied to AN [24] and proposes that individuals with the disorder experience both general emotional vulnerabilities and specific vulnerabilities to food and body-related stimuli and to their starved state. When an individual with AN experiences an emotional event, he/she responds with heightened emotional arousal, and to regulate that emotional state, the individual engages in disordered eating behaviors that temporarily reduce emotional arousal. This model is similar in form to the affect regulation model underlying cognitive-emotional–behavioral therapy for eating disorders [25], which addresses the contribution of an invalidating environment and primary emotional experiences to beliefs about emotions, which in turn produce secondary emotions that promote maladaptive behaviors to regulate emotions. Of note, the major concepts of these theories have been supported by recent reviews and meta-analyses that address the maladaptive nature of emotion generation and regulation in AN [8, 9].
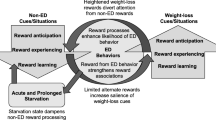
Another affect-based model of AN was described by Selby et al. [26] and focuses on positive emotion differentiation. According to this model, when individuals with AN initiate weight loss and achieve their goals, they experience positive emotions which motivate further weight loss. The effect of weight loss on positive emotions is stronger in individuals with low positive emotion differentiation (i.e., low ability to distinguish between different positive emotions), because several additional positive emotions (e.g., happiness, confidence) in addition to any positive emotion that may naturally result from weight loss (e.g., pride) may be triggered after engaging in eating disorder behaviors, thus positively reinforcing weight loss. In contrast, gaining or failing to lose weight increases negative emotions. Over time, weight-loss behaviors become conditioned to elicit positive emotions, even when the effects of the weight loss become harmful.
Finally, other theories include affect as one of multiple interacting factors that initiate and/or maintain AN. For example, the cognitive interpersonal maintenance model of AN proposes that avoidance of the experience and expression of intense negative emotions, particularly those related to social encounters, is one of the key factors in maintaining AN [27]. Furthermore, the transdiagnostic model of eating disorders proposes that mood intolerance is one of several potential maintaining factors across the eating disorders spectrum, including in AN [28].
Reward/punishment-based theories of AN
Various reward/punishment-related theories of AN have been proposed, many of which emphasize the role of reinforcement processes. For example, Bergh and Södersten (1996) proposed that AN is first initiated, because individuals with AN find it reinforcing to eat less and exercise more given the effects of these behaviors on body weight ands shape [29]. Over time, cue-conditioning (i.e., conditioning to the stimuli that provide reward) becomes the main mechanism responsible for the maintenance of AN. Furthermore, Park et al. (2014) suggest that weight-loss behaviors are initially rewarding and positively reinforced, but over time become compulsive and negatively reinforced [30]. Similarly, Steinglass and Walsh [31] proposed a model, whereby dieting behavior is initially rewarding in AN, leading to repeated practice, which results in the dieting behavior becoming automatic and less dependent on the receipt of reward (i.e., habitual).
Other theories in this domain have been more focused on the underlying neurobiology of reward-related abnormalities in AN. For instance, Davis and Woodside [32] proposed that individuals with AN exhibit hypo-responsive dopamine function, which results in a reduced capacity to experience reward. Zink and Weinberger [33] proposed that stressors (e.g., social rejection) can promote food restriction in certain individuals (e.g., those genetically predisposed to AN or exposed to certain environments), with restriction and associated weight loss promoting alterations in the dopamine-ventral striatal reward system that reinforces self-starvation by associating restriction cues with motivational value. These neurobiological alterations thus reinforce the desire to not eat, resulting in a cycle of starvation. Furthermore, in conceptualizing the neurobiology underlying reward processes in AN, Keating [34] describes the tendency of individuals with AN to confuse aspects of reward with punishment, including a common transition from the experience of disorder-related behaviors as rewarding to punishing over time. These abnormalities are subsequently conceptualized within a framework emphasizing the potential salience of anterior cingulate cortex hypoactivity with respect to altered reward processing in AN.
Synthesizing recent reviews on affect and reward/punishment in AN affect
Two recent reviews/meta-analyses related to affect have been conducted in AN [8, 9]. Oldershaw et al. [9] conducted a review and meta-analysis on emotion generation and regulation processes in individuals with AN, framed around Gross’ process model of emotional regulation [35]. They found that individuals with AN reported: (1) more maladaptive schemata (i.e., more negative beliefs about oneself / others / the environment, which can give rise to negative affect); (2) poorer emotional awareness and recognition; (3) higher negative emotions and lower positive emotions; and (4) a greater use of maladaptive emotion regulation strategies than healthy controls [9]. In contrast, Lavender et al. [8] used Gratz and Roemer’s [36] multidimensional model of emotion regulation and dysregulation as a framework to review the literature on emotion regulation processes in AN. They found that individuals with AN have emotion regulation deficits across the four dimensions identified by Gratz and Roemer [36]: (1) the flexible use of situation adaptive and appropriate strategies to modulate emotion duration / intensity; (2) the ability to successfully inhibit impulsive behavior and maintain goal-directed behavior when distressed; (3) emotional awareness, clarity and acceptance; and (4) the willingness to experience emotional distress to pursue meaningful activities.
Taken together, evidence from both reviews suggests that individuals with AN exhibit a pattern of broad emotion regulation deficits, tend to utilize more maladaptive and less adaptive emotion regulation strategies than healthy controls, and commonly display reduced emotional self-awareness. Furthermore, both reviews noted that, although there are some improvements in emotion regulation among individuals recovered from AN, there is evidence that some difficulties may persist into remission from the illness.
Reward/punishment
Three recent reviews/meta-analyses related to reward /or punishment have been conducted in AN [10,11,12]. In a meta-analysis, Harrison et al. (2010) examined reward and punishment sensitivity in AN, reporting that currently ill and recovered individuals with AN display reduced reward sensitivity/novelty seeking than healthy controls. However, whereas AN-R patients consistently demonstrated lower reduced reward sensitivity / novelty seeking versus healthy controls, results for mixed and recovered AN groups were more variable [10]. They also found that individuals currently ill with or recovered from AN-R or AN-BP exhibited increased sensitivity to punishment, suggesting that there may be a preexisting dispositional bias towards punishment that contributes to AN.
O’Hara et al. [12] examined reward processes in AN through a narrative review, concluding that the reluctance to gain weight in AN promotes an aversive appraisal of food stimuli and subsequent overvaluation of rewards that are related to pursuit of the thin ideal (e.g., thinness, exercise). They further proposed a model in which aberrant cognitions related to eating, weight and shape alter the functioning of reward systems in AN. Finally, Keating et al. [11] provided a qualitative review of reward processing in AN, with a focused on taste-based reward. The authors suggest that the tendency of individuals with AN to exhibit a limited response to typically rewarding stimuli (food) is due to weight/caloric-related fears versus more basic deficits in the experience of reward. As such, the abnormalities are viewed as deficits in wanting versus liking, characterized by an impaired motivational salience for food-related stimuli.
Overall, findings from these three reviews thus support the notion that AN is characterized by a complex pattern of abnormalities in reward and punishment processes. In particular, individuals with AN appear to experience reduced reward responding to conventional rewards, but also overvalue rewards that are related to the thin ideal. Along with this altered reward sensitivity, individuals with AN also seem to exhibit an increased sensitivity to punishment.
Discussion
Disparate literatures
Despite a strong theoretical interlink between affect and reward/punishment, the empirical and theoretical literature in AN has most commonly investigated these processes separately. Several general characteristics of the disparate literatures may represent factors contributing to this separate focus. Perhaps most notably, reward-based research on AN has tended to be more neurobiologically focused, with an emphasis on underlying structural and/or functional abnormalities in brain regions and networks associated with reward processing. In contrast, affect-focused in AN has been more behaviorally focused, emphasizing subjective experience and clinical phenomenology. Furthermore, the role of reward/punishment in AN has most often been investigated from a more static trait/dispositional perspective (e.g., using trait-based self-report measures, or one-time administration of reward tasks), whereas there has been more consistent variability in the approach to investigating affect processes in AN from diagnostic comorbidities (e.g., mood disorders), to dispositional perspectives (e.g., trait anxiety), to state-based perspectives (e.g., momentary emotional precipitants of eating disorder behaviors). As such, the general dissociation of these literatures is likely due to a combination of heterogeneity in methodologies (e.g., clinical interview, questionnaire, computerized task, neuroimaging), level and focus of investigation (e.g., personality, subjective experience, brain function), and underlying conceptualization (e.g., state versus trait).
Clinical implications
A more integrated conceptualization of affect and reward/punishment processes may have clinical implications for AN. For instance, most affect-focused psychotherapies for AN primarily emphasize the reduction of negative affect [37]. However, interventions that also focus directly on both enhancing responsivity to adaptive rewards and increasing the frequency and/or intensity of positive affective states (e.g., behavioral activation) could be particularly beneficial, as increases in hedonic behavior are associated with successful treatment outcomes in AN [38]. For instance, treatments could leverage social activity and adaptive/healthy exercise—which have been shown to be particularly important to positive affect [14]—to increase positive emotions in individuals with AN (see Cook et al. [39] for guidelines on the use of exercise in treating eating disorders). Additionally, strategies focused on reducing emotional and behavioral avoidance tendencies and encouraging individuals with AN to identify and work toward meaningful and valued goals other than the pursuit of thinness may also have promise, as adaptive goal striving can be rewarding and increase positive affect and well-being [40, 41].
Treatments for AN that focused on the characteristic nature of reward and punishment processes in the disorder have also begun to emerge. For example, Kaye et al. [42] describe a temperament-based treatment for AN that targets neurobiologically based traits and temperament variables including anxiety/harm avoidance, reward insensitivity, and interoceptive awareness. Given the empirical evidence supporting the role of such constructs in AN, an increased focus on targeting these processes in the treatment of AN may be warranted. Finally, as novel and/or adapted interventions based on affect and reward/punishment domains are developed and empirically evaluated, including measures of these processes at multiple time points will be important for examining them as predictors, moderators, and mediators of treatment outcome.
Future directions
There are a number potential areas for future integrated investigations of affect and reward/punishment processes in AN. Promising directions may focus on methodological approaches that address gaps in the current literature (e.g., use of prospective and/or longitudinal approaches, applying integrative and multi-method study designs), or on further characterizing the nature of these processes in AN (e.g., exploring between- and within-person variability, exploring transdiagnostic empirical classifications based on these domains). Below we discuss several possible examples for future research in these domains.
One important area for future research is to utilize prospective or longitudinal methods to investigate patterns of dysfunction in affect and reward/punishment processes over time, as the majority of existing studies have been cross section in nature. Longitudinal research would provide the potential for understanding the extent to which abnormalities in these domains (independently or interactivity) function as predisposing factors for AN, consequences of the disorder, or perhaps both. Such research would also allow for an evaluation of the extent the role of these processes in relation to eating disorder symptomatology various across the duration of AN illness. For instance, it is possible that certain processes within these domains are more salient earlier versus later in the course of illness (or vice versa) [31]. Furthermore, studies of mechanisms that maintain maladaptive affective and reward-based reinforcement processes in AN are needed. For example, it is possible that individuals with AN exhibit certain attentional biases that underlie the discrepancy in reward salience between disorder-specific and non-specific stimuli. Additionally, it is likely that these processes interact with other important factors (e.g., culture, personality, cognitions) in their association with eating disorder symptoms. For example, individuals predisposed to AN may have certain personality traits (e.g., perfectionism, obsessionality; [43]) and affective characteristics (e.g., anxiety proneness; [44]) that might enhance the reinforcing nature of restriction.
A second promising direction is the use of multi-method study designs incorporating neurobiological, psychological, and behavioral assessment methods. Studies can integrate functional neuroimaging methods and real-world, real-time assessment approaches (e.g., ecological momentary assessment) to explore how individual differences in neural activity associated with reward processes relate to the naturalistic experience of affect and eating disorder behaviors in AN [45]. For instance, such individual differences in brain function could be related to other traits (e.g., attachment style) [46], affective reactivity to certain stimuli in AN (e.g., meals, social encounters), or with degree of affect-based reinforcement of eating disorder behaviors (e.g., restrictive eating). Such research will be helpful in further elaborating how reward-based propensities relate to the momentary affective experiences in naturalistic settings in AN.
A third key area of future research will be to characterize individual variability in affect- and reward/punishment-based tendencies within the diagnosis of AN, as well as investigating possible empirical classifications based on these processes. Preliminary research suggests that affect intensity and frequency varies depending on AN diagnostic subtype and recovery status, with individuals with AN-BP typically reporting more problematic affect than those with AN-R [47, 48]. There is also evidence suggesting interdiagnostic differences in reward and punishment processes [49, 50]. Moreover, individuals with current AN experience more problematic affect than recovered individuals [51]. There is also evidence for a similar pattern of findings for reward and punishment processes [52]. Finally, given evidence supporting the validity and utility of personality-based subtypes of AN [53, 54], establishing empirically derived subtypes of AN based on propensities within the affect and reward/punishment domains may hold promise (e.g., as potential predictors of treatment response and/or relapse).
Conclusion
The aim of the present article was to demonstrate the disparate nature of the literatures on affect and reward/punishment processes in AN, as well as to discuss related implications and directions for future integrative research on these domains among individuals with AN. Despite an inherent overlap in the nature of affect and reward/punishment processes, the empirical and theoretical literature in AN has most commonly addressed these domains independently. Theoretical conceptualizations and empirical studies that investigate processes across these domains will help to provide a more comprehensive understanding of their role in the development and maintenance of AN, and may also provide guidance on the development or refinement of interventions that will result in better AN treatment outcomes.
References
American Psychiatric Association (2013) Diagnostic and statistical manual of mental disorders, 5th edn. Washington
Katzman DK (2005) Medical complications in adolescents with anorexia nervosa: a review of the literature. Int J Eat Disord 37(S1):S52–S59. https://doi.org/10.1002/eat.20118
Kaye WH, Bulik CM, Thornton L, Barbarich N, Masters K (2004) Comorbidity of anxiety disorders with anorexia and bulimia nervosa. Am J Psychiatry 161:2215–2221. https://doi.org/10.1176/appi.ajp.161.12.2215
Papadopoulos FC, Ekbom A, Brandt L, Ekselius L (2009) Excess mortality, causes of death and prognostic factors in anorexia nervosa. Br J Psychiatry 194(1):10–17. https://doi.org/10.1192/bjp.bp.108.054742
Sullivan PF (1995) Mortality in anorexia nervosa. Am J Psychiatry 152(7):1073–1074. https://doi.org/10.1176/ajp.152.7.1073
Bulik CM, Berkman KA, Brownley KA, Sedway JA, Lohr KN (2007) Anorexia nervosa treatment: a systematic review of randomized controlled trials. Int J Eat Disord 40(4):310–320. https://doi.org/10.1002/eat.20367
Culber KM, Racine SE, Klump KL (2015) Research review: What we have learned about the causes of eating disorders—a synthesis of sociocultural, psychological, and biological research. J Child Psychol Psychiatry 56(11):1141–1164. https://doi.org/10.1111/jcpp.12441
Lavender JM, Wonderlich SA, Engel SG, Gordon KH, Kaye WH, Mitchell JE (2015) Dimensions of emotion dysregulation in anorexia nervosa and bulimia nervosa: a conceptual review of the empirical literature. Clin Psychol Rev 40:111–122. https://doi.org/10.1016/j.cpr.2015.05.010
Oldershaw A, Lavender T, Sallis H, Stahl D, Schmidt U (2015) Emotion generation and regulation in anorexia nervosa: a systematic review and meta-analysis of self-report data. Clin Psychol Rev 39:83–95. https://doi.org/10.1016/j.cpr.2015.04.005
Harrison A, O’Brien N, Lopez C, Treasure J (2010) Sensitivity to reward and punishment in eating disorders. Psychiatry Res 177(1–2):1–11. https://doi.org/10.1016/j.psychres.2009.06.010
Keating C, Tilbrook AJ, Rossell SL, Enticott PG, Fitzgerald PB (2012) Reward processing in anorexia nervosa. Neuropsychologia 50(5):567–575. https://doi.org/10.1016/j.neuropsychologia.2012.01.036
O’Hara CB, Campbell IC, Schmidt U (2015) A reward-centred model of anorexia nervosa: a focussed narrative review of the neurological and psychophysiological literature. Neurosci Biobehav Rev 52:131–152. https://doi.org/10.1016/j.neubiorev.2015.02.012
Forbes EE, Dahl RE (2005) Neural systems of positive affect: Relevance to understanding child and adolescent depression? Dev Psychopathol 17(3):827–850. https://doi.org/10.1017/S095457940505039X
Watson D (2000) Mood and temperament. Guilford Press, New York
Berridge KC, Robinson TE (2003) Parsing reward. Trends Neurosci 26(9):507–513. https://doi.org/10.1016/S0166-2236(03)00233-9
Berridge KC, Kringelbach ML (2008) Affective neuroscience of pleasure: reward in humans and animals. Psychopharmacology 199(3):457–480. https://doi.org/10.1007/s00213-008-1099-6
Gray J (1970) The psychophysiological basis of introversion-extraversion. Behav Res Ther 8(3):249–266. https://doi.org/10.1016/0005-7967(70)90069-0
Watson D, Wiese D, Vaidya J, Tellegen A (1999) The two general activation systems of affect: structural findings, evolutionary considerations, and psychobiological evidence. J Pers Soc Psychol 76(5):820–838. https://doi.org/10.1037/0022-3514.76.5.820
Rolls E (2000) On the brain and emotion. Behav Brain Sci 23(02):219–228. https://doi.org/10.1017/S0140525X00512424
Heatherton TF, Baumeister RF (1991) Binge eating as escape from self-awareness. Psychol Bull 110(1):86–108. https://doi.org/10.1037/0033-2909.110.1.86
Wildes JE, Ringham RM, Marcus MD (2010) Emotion avoidance in patients with anorexia nervosa: initial test of a functional model. Int J Eat Disord 43(5):398–404. https://doi.org/10.1002/eat.20730
Fruzzetti AE, Shenk C, Hoffman PD (2005) Family interaction and the development of borderline personality disorder: a transactional model. Dev Psychopathol 17(4):1007–1030. https://doi.org/10.1017/S0954579405050479
Linehan MM (1993) Dialectical behavior therapy for treatment of borderline personality disorder: Implications for the treatment of substance abuse. In: Onken LS, Blane JD, Boren JJ (eds) National Institute on Drug Abuse research monograph: behavioral treatments for drug abuse and dependence. U.S. Department of Health and Human Services, pp 201–216
Haynos AF, Fruzzetti AE (2011) Anorexia nervosa as a disorder of emotion dysregulation: Evidence and treatment implications. Clin Psychol Sci Pract 18(3):183–202. https://doi.org/10.1111/j.1468-2850.2011.01250.x
Corstorphine E (2006) Cognitive–emotional–behavioural therapy for the eating disorders: working with beliefs about emotions. Eur Eat Disord Rev 14(6):448–461. https://doi.org/10.1002/erv.747
Selby EA, Wonderlich SA, Crosby RD, Engel SG, Panza E, Mitchell JE et al (2014) Nothing tastes as good as thin feels low positive emotion differentiation and weight-loss activities in anorexia nervosa. Clin Psychol Sci 39:870–911. https://doi.org/10.1177/2167702613512794
Schmidt U, Treasure J (2006) Anorexia nervosa: valued and visible. A cognitive-interpersonal maintenance model and its implications for research and practice. Br J Clin Psychol 45(3):343–366. https://doi.org/10.1348/014466505x53902
Fairburn CG, Cooper Z, Shafran R (2003 May) Cognitive behaviour therapy for eating disorders: a “transdiagnostic” theory and treatment. Behav Res Ther 41(5):509–528. https://doi.org/10.1016/S0005-7967(02)00088-8
Bergh C, Södersten P (1996) Anorexia nervosa, self–starvation and the reward of stress. Nat Med 2(1):21–22. https://doi.org/10.1038/nm0196-21
Park RJ, Godier LR, Cowdrey FA (2014) Hungry for reward: How can neuroscience inform the development of treatment for anorexia nervosa? Behav Res Ther 62:47–59. https://doi.org/10.1016/j.brat.2014.07.007
Steinglass JE, Walsh BT (2016) Neurobiological model of the persistence of anorexia nervosa. J Eat Disord 4:19. https://doi.org/10.1186/s40337-016-0106-2
Davis C, Woodside DB (2002) Sensitivity to the rewarding effects of food and exercise in the eating disorders. Compr Psychiatry 43(3):189–194. https://doi.org/10.1053/comp.2002.32356
Zink CF, Weinberger DR (2010) Cracking the moody brain: the rewards of self starvation. Nat Med 16(12):1382–1383. https://doi.org/10.1038/nm1210-1382
Keating C (2010) Theoretical perspective on anorexia nervosa: the conflict of reward. Neurosci Biobehav Rev 34(1):73–79. https://doi.org/10.1016/j.neubiorev.2009.07.004
Gross JJ (1998) The emerging field of emotion regulation: an integrative review. Rev Gen Psychol 2(3):271. https://doi.org/10.1037/1089-2680.2.3.271
Gratz KL, Roemer L (2004) Multidimensional assessment of emotion regulation and dysregulation: development, factor structure, and initial validation of the difficulties in emotion regulation scale. J Psychopathol Behav Assess 26(1):41–54. https://doi.org/10.1023/B:JOBA.0000007455.08539.94
Sala M, Heard A, Black EA (2016) Emotion-focused treatments for anorexia nervosa: a systematic review of the literature. Eat Weight Disord 21(2):147–164. https://doi.org/10.1007/s40519-016-0257-9
Ohmann S, Popow C, Wurzer M, Karwautz A, Sackl-Pammer P, Schuch B (2013) Emotional aspects of anorexia nervosa: results of prospective naturalistic cognitive behavioral group therapy. Neuropsychiatr Klin Diagn Ther Rehabil Organ Ges Osterreichischer Nervenarzte Psychiater 27(3):119–128. https://doi.org/10.1007/s40211-013-0065-7
Cook BJ, Wonderlich SA, Mitchell JE, Thompson R, Sherman R, Mccallum K (2016) Exercise in eating disorders treatment: systematic review and proposal of guidelines. Med Sci Sports Exerc 48(7):1408–1414. https://doi.org/10.1249/MSS.0000000000000912
Diener E, Larsen RJ (1993) The experience of emotional well-being. In: Lewis M, Haviland JM, Lewis M, Haviland JM (eds) Handbook of emotions. Guilford Press, New York, pp 405–415
Myers DG, Diener E (1995) Who is happy? Psychol Sci 6(1):10–19. https://doi.org/10.1111/j.1467-9280.1995.tb00298.x
Kaye WH, Wierenga CE, Knatz S, Liang J, Boutelle K, Hill L et al (2015) Temperament-based treatment for anorexia nervosa. Eur Eat Disord Rev 23(1):12–18. https://doi.org/10.1002/erv.2330
Vitousek K, Manke F (1994) Personality variables and disorders in anorexia nervosa and bulimia nervosa. J Abnorm Psychol 103(1):137–147. https://doi.org/10.1037/0021-843X.103.1.137
Kaye WH, Barbarich NC, Putnam K, Gendall KA, Fernstrom J, Fernstrom M et al (2003) Anxiolytic effects of acute tryptophan depletion in anorexia nervosa. Int J Eat Disord 33(3):257–270. https://doi.org/10.1002/eat.10135
Fischer S, Breithaupt L, Wonderlich J, Westwater ML, Crosby RD, Engel SG et al (2017) Impact of the neural correlates of stress and cue reactivity on stress related binge eating in the natural environment. J Psychiatr Res 92:15–23. https://doi.org/10.1016/j.jpsychires.2017.03.017
Monteleone AM, Cardi V, Volpe U, Fico G, Ruzzi V, Pellegrino F, Castellini G, Monteleone P, Maj M (2018) Attachment and motivational systems: relevance of sensitivity to punishment for eating disorder psychopathology. Psychiatry Res 260:353–359. https://doi.org/10.1016/j.psychres.2017.12.002
Haynos AF, Berg KC, Cao L, Crosby RD, Lavender JM, Utzinger LM et al (2017) Trajectories of higher- and lower-order dimensions of negative and positive affect relative to restrictive eating in anorexia nervosa. J Abnorm Psychol 126(5):495–505. https://doi.org/10.1037/abn0000202
Selby EA, Cornelius T, Fehling KB, Kranzler A, Panza EA, Lavender JM et al (2015) A perfect storm: examining the synergistic effects of negative and positive emotional instability on promoting weight loss activities in anorexia nervosa. Front Psychol 31:6:1260. https://doi.org/10.3389/fpsyg.2015.01260
Matton A, de Jong P, Goosens L, Jonker N, Van Malderen E, Vervaet M et al (2017) Sensitivity for cues predicting reward and punishment in young women with eating disorders. Eur Eat Disorders Rev 25(6):501–511. https://doi.org/10.1002/erv.2541
Murao E, Sugihara G, Isobe M, Noda T, Kawabata M, Matsukawa N et al. Differences in neural responses to reward and punishment processing between anorexia nervosa subtypes: an f MRI study. Psychiatry Clin Neurosci 2017: 71(9): 647–658. https://doi.org/10.1111/pcn.12537
Harney MB, Fitzsimmons-Craft EE, Maldonado CR, Bardone-Cone AM (2014) Negative affective experiences in relation to stages of eating disorder recovery. Eat Behav 15(1):24–30. https://doi.org/10.1016/j.eatbeh.2013.10.016
DeGuzman M, Shott ME, Yang TT, Riederer J, Frank GKW Association of elevated reward prediction error response with weight gain in adolescent anorexia nervosa. Am J Psychiatry 2017:174(6):557–565. https://doi.org/10.1176/appi.ajp.2016.16060671
Lavender JM, Wonderlich SA, Crosby RD, Engel SG, Mitchell JE, Crow SJ et al (2013) Personality-based subtypes of anorexia nervosa: examining validity and utility using baseline clinical variables and ecological momentary assessment. Behav Res Ther 51(8):512–517. https://doi.org/10.1016/j.brat.2013.05.007
Wildes JE, Marcus MD, Crosby RD, Ringham RM, Dapelo MM, Gaskill JA et al (2011) The clinical utility of personality subtypes in patients with anorexia nervosa. J Consult Clin Psychol 79(5):665. https://doi.org/10.1037/a0024597
Acknowledgements
Margarita Sala is supported by the National Science Foundation (NSF) Graduate Research Fellowship under Grant No. DGE-1645420. Amy H. Egbert is supported by the National Science Foundation (NSF) Graduate Research Fellowship. Jason Lavender is supported by National Institute of Health (NIH) grant K23MH101342. Andrea Goldschmidt is supported by NIH grant K23DK105234. Any opinion, findings, and conclusions or recommendations expressed in this material are those of the authors and do not necessarily reflect the views of the NSF or NIH.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed consent
For this type of study, formal consent is not required.
Rights and permissions
About this article

Cite this article
Sala, M., Egbert, A.H., Lavender, J.M. et al. Affect, reward, and punishment in anorexia nervosa: a narrative overview. Eat Weight Disord 23, 731–737 (2018). https://doi.org/10.1007/s40519-018-0588-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40519-018-0588-9