
Abstract
There is an increasing incidence of skin cancer across the world. The World Health Organization reports that the global incidence of melanoma will continue to rise with increasing depletion of the ozone layer and consequent UV irradiation. The natural product sandalwood oil from genus Santalum (Family Santalaceae) and its constituent alpha-santalol have been reported to exert chemopreventive effects against skin cancers as well as prostate, head and neck, and breast cancers. The anticancer effects are mediated via modulation of MAPK, AP-1, beta-catenin and PI3K/Akt pathways, upregulation of p21, and activation of caspases/PARP. Furthermore, sandalwood oil exerts anti-inflammatory activities via prostaglandin E2, IL-1beta, inhibition of NF-kappaB, and 5-lipoxygenase. Other therapeutic activities in eczema, psoriasis, radiation dermatitis, antifungal, etc. have also been reported. Sandalwood oil has acceptable safety and is well-tolerated. Taken together, given the chemopreventive potential of sandalwood oil, future clinical trials are warranted to investigate its use as an adjunct to chemotherapy or immunotherapy for skin cancers.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Skin cancer is the most prevalent form of cancer leading to several deaths within the USA each year [1]. In England, melanoma occurrence has risen from 9.3 to 14.7 per 100,000 people [2]. The melanoma incidence is estimated to be 1,222,023 people in the USA in 2015 whereas 5.3% new cases and 1.5% of deaths are estimated in 2018. According to the statistics of the NCI’s Surveillance, Epidemiology, and End Results (SEER) Registry, the survival rate was 91.8% for melanoma skin cancer for the years 2008–2014 [3]. In non-melanoma carcinoma, including basal cell cancer (BCC) and squamous cell cancer (SCC), SCC is found to be the second most prevalent form of skin carcinoma. About 4.3 million cases of BCC and 1 million cases of SCC are reported every year in the USA respectively [4, 5]. Globally, the incidence is estimated to be 132,000 for melanoma and 2–3 million for non-melanoma skin cancer every year [6]. The mortality rate per 100,000 for skin cancer is estimated to be 0.43 in India [7]. However, this is expected to rise with increased ozone layer depletion and consequent ultraviolet (UV) irradiation. Across the globe, the incidence is highest in Australia and New Zealand due to the highest exposure to UV radiation [8]. In Australia, melanoma skin cancer ranks third amongst all the other cancers and more than 750,000 are treated for non-melanoma skin cancer every year [9]. Other regions with high risk of skin cancer include England, Switzerland, Slovenia, Netherlands, Canada, China, India, and South Africa.
The ozone layer depletion leads to the loss of the protective function of the atmosphere allowing the UVB rays to reach the earth’s surface. These rays cause skin cancer through genetic alteration or DNA damage [10]. It has been shown that chemical- and UVB-induced skin carcinoma was inhibited by sulforaphane through nuclear factor erythroid 2-related factor 2 (Nrf2) [11]. The global incidence of melanoma cases is about to rise to 4500 and for non-melanoma cases to 300,000 with 10% increase in the ozone layer depletion [6]. Melanoma at “low-risk” (stage 0 and 1) is treated by surgical resection. Indeed, several surgical approaches in the treatment of melanoma carcinoma are excisional surgery, Moh’s surgery, and lymph node dissection [12]. Interestingly, the “high-risk” (stage 2, stages 3 and 4) melanomas are treated by new promising strategies such as targeted drug therapy, vaccines, and immunotherapy [13]. Immunotherapy treatment works on the principle of activating the person’s immune system to identify and cause the self-destruction of the melanoma cells. This treatment involves immune checkpoint blockades, such as programmed death 1 (PD-1) inhibitors and CTLA-4, oncolytic virus treatment, and cytokines [13]. Few drugs such as nivolumab (anti-PD-1) and ipilimumab (anti-CTLA-4) belonging to the class of checkpoint inhibitors are effective in and approved by USFDA for the treatment of melanoma skin carcinoma when given either alone or in combination with other immunotherapy or targeted class of drugs [14]. A combination of dabrafenib and trametinib is given to treat stage 3 melanoma skin cancer thereby effectively decreasing the risk by more than 50% [15]. Olaratumab alone or in combination with doxorubicin has received accelerated approval in the USA and Europe for the treatment of soft tissue malignant tumor [16]. In addition, non-melanoma skin cancers are also treated through various surgeries, radiotherapy, topical, systemic, and targeted therapies [17].
Phytochemistry of Sandalwood Oil
Sandalwood belonging to the genus Santalum (family Santalaceae) is a semiparasitic tree and is the most expensive tree after African Blackwood [18]. A large number of sandalwood varieties exist from which sandalwood oil (essential oil) can be extracted. From these varieties, Santalum album (East Indian Sandalwood) and Santalum spicatum (West Australian Sandalwood) were approved as standards by the International Organization for Standardization (ISO) [19]. Table 1 shows some of the global varieties of sandalwood along with their chemical constituents, geographical distribution, and historical uses. Amongst these, the two most common varieties in India are White sandalwood (Santalum album) and Red sandalwood (Pterocarpus santalinus) which are depicted in Fig. 1 a and b respectively. Furthermore, the active constituents in the White sandalwood variety include 41–55% of α-santalol and 16–24% of β-santalol as shown in Fig. 2 a and b respectively.

a White Sandalwood (Santalum album): also known as East Indian Sandalwood and is the most common variety of Sandalwood found in India. The major chemical constituents are α-santalol and β-santalol. b Red Sandalwood (Pterocarpus santalinus): also known as Red saunders/Raktachandana which is the second most common variety found in India after White Sandalwood

a Chemical structure of α-santalol: It is a constituent (41–55%) of the White Sandalwood variety. b Chemical structure of β-santalol: It is a constituent (16–24%) of the White Sandalwood variety

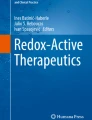
Molecular pathway for skin cancer chemoprevention with sandalwood oil and alpha-santalol:α-santalol may induce apoptosis through activation of various caspase cascades in the death receptor pathway. In particular, α-santalol may be responsible for the activation of caspase-3 and cleavage of poly (ADP-ribose) polymerase (PARP) by activating the upstream caspase-8 and caspase-9. In addition, α-santalol may also trigger the release of cytochrome c from the mitochondria into the cytosol. Further, it may also inhibit the PI3K/Akt pathway. Moreover, α-santalol may upregulate the levels of p53 and p21 resulting in the induction of apoptosis and cell cycle arrest at G2/M phase respectively. Sandalwood oil may inhibit the production of cytokines and elevate the production of IL-1β resulting in the inhibition of the downstream NF-κB pathway. Sandalwood oil also inhibits AP-1. Furthermore, sandalwood oil may also increase the levels of Interleukin-6 (IL-6) exhibiting anti-inflammatory activity
Sandalwood oil content was found to be 0.2–2% in heartwood of the young trees whereas 2–6.2% in heartwood of the mature trees [29]. The widely utilized method for isolating sandalwood oil is steam distillation because of its ability to generate high quality and yield of sandalwood oil. The other methods are absolute extraction, supercritical carbon dioxide extraction, and the traditionally used hydro-distillation method. In steam distillation, steam liberates sandalwood oil from the heartwood. Sandalwood oil shows several therapeutic activities such as anticancer, anti-inflammatory, and antimicrobial (antibacterial/antiviral) [19]. Other constituents present in sandalwood include hydrocarbons (santene, nortricyclo-ekasantalene), α- and β-santalenes, alcohols (santenol, teresantalol), aldehydes (nor-tricyclo-kasantalal), α- and β-santalic acids, and teresantalic acids. Two minor components namely cyclosantalal (0.21–2.26%) and isocyclo-santalal (0.11–1.47%) were also reported [29].
Molecular Aspects of Skin Cancer Chemoprevention with Sandalwood Oil
α-Santalol, a major phytoconstituent of sandalwood oil, is a sesquiterpene useful for chemoprevention in skin cancer either by initiation of caspase-mediated cell death or through cell growth prohibition [30]. Dickinson et al. [31] evaluated the impact of East Indian sandalwood oil treatment on cell multiplication, cell death, and changes in UV-induced signal transduction pathways such as MAPK, PI3K/Akt, and AP-1 in HaCaT cells. It was demonstrated that East Indian sandalwood oil inhibited multiplication of cells by hindering the cell cycle at G2/M phase in proliferating cells rather than in quiescent cells. Further, this study showed that the UVB-initiated signaling pathways such as MAPK and PI3K/Akt were not inhibited whereas the AP-1 signaling pathway was inhibited by 0.0005% East Indian sandalwood oil in a concentration-dependent manner. East Indian sandalwood oil treatment initiates autophagy through stimulation of microtubule-associated protein 1 light chain 3 (LC3). Interestingly, increased concentration of α-santalol (about 25–75 μM) resulted in enhanced cell death and activation of apoptotic proteins such as caspase-8 and caspase-9 resulting in the cleavage of poly (ADP-ribose) polymerase (PARP) and further activating caspase-3 protein upon α-santalol treatment in human epidermoid carcinoma A431 cells [32].
α-Santalol elevated the cyclin A/Cdk2 expression and suppressed the cyclin B/Cdc2 binding expression in p53 mutated A431 cells and p53 wild-type UACC-62 skin cancer cell lines resulting in the arrest of the cell cycle at metaphase stage and depolymerization of microtubules respectively [33]. α-Santalol at 50–100 μM concentration showed suppression of cell growth whereas 50–75 μM concentration of α-santalol arrested the cell cycle at G2/M phase respectively. In addition, α-santalol upregulated p21 and downregulated mutated-p53 in A431 cells, whereas it upregulated p53 wild-type in UACC-62 cells [33].
In Vivo Skin Cancer Chemopreventive Efficacy of Sandalwood Oil and α-Santalol
There have been several pre-clinical studies that demonstrate the efficacy of sandalwood oil and α-santalol in skin cancer chemoprevention. Dwivedi et al. [34] demonstrated the significance of α-santalol, a chemopreventive agent, in SENCAR and CD1 mice throughout the DMBA (7,12-dimethylbenz(a)anthracene)-induced and TPA (12-O-tetradecanoyl phorbol-13-acetate)-promoted stage as well as TPA-initiated ornithine decarboxylase (ODC) and 3-H thymidine activity in skin cancer prevention. Treatment with 0.1 mL of 5% of α-santalol in acetone retarded the growth and multiplication of papilloma during the promotion stage and TPA-initiated ODC event whereas 3-H thymidine incorporation in epidermal DNA was inhibited. In another study in CD-1 mice, the influence of 100 μL of sandalwood oil on DMBA-induced and TPA-promoted skin papilloma and also TPA-induced ODC activity was investigated [35]. The study reported reduced papilloma occurrence, multiplicity, and TPA-induced ODC activity by 67%, 96%, and 70% respectively.
Chemopreventive effect was observed by the application of 0.1 mL of 5% w/v of α-santalol in acetone two times a week for 30 weeks topically in hairless SKH-1 mice induced with skin cancer through exposure to UVB radiation. Skin cancer incidence and multiplicity was found to decrease in UVB-initiated and TPA-promoted group; DMBA-initiated and UVB-promoted group; and UVB-initiated and UVB-promoted group whereas UVB-induced ODC activity was also inhibited [36]. Arasada et al. [37] used a UVB-exposed skin cancer model to study the impact of α-santalol on the caspase 3, 8 and p53 levels in SKH-1 mice. They reported a delay in the development of tumors, elevated levels of caspase 3, caspase 8, and upregulation of p53 levels when pre-treated with 0.1 mL of 5% w/v of α-santalolin acetone 1 h prior to exposure to UVB radiation two times a week for 30 weeks. Santha et al. [38] reported downregulation in the levels of cyclin-dependent kinase (CDK) and cyclins A, B1, D1, and D2 expression whereas elevated expression of p53 levels for skin cancer induced by UVB in hairless SKH-1 mouse model after treatment with 0.1 mL of 10% w/v of α-santalol in acetone for 5 days a week for 30 weeks. It further showed induction of caspase 3 and PARP and inhibition of epidermal thickness, hypergenesis (a result of cell proliferation), inflammation markers, and COX-2 when pre-treated with 0.1 mL of 10% w/v of α-santalol in acetone. Chilampalli et al. [39] analyzed the effect of α-santalol, magnolol and honokiol alone, or α-santalol in combination with honokiol or magnolol, on viability, multiplication of cells and on apoptosis in human epidermoid carcinoma A431 cells. A 90% reduction in cell proliferation was observed on combination treatment with 50 μM α-santalol and 50 μM honokiol or 100 μM magnolol showing the efficacy of these compounds in skin cancer prevention. Banerjee et al. [40] showed an increase in the sulphydryl and GST (glutathione-S-transferase) levels upon oral gavage of 5 μL sandalwood oil for 10 days and 15 μL for 20 days every day in male Swiss albino mice.
Chemopreventive Efficacy of Sandalwood Oil in Other Cancers
Saraswati et al. [41] reported a study in which 10–40 μM of α-santalol was found to be an effective inhibitor of angiogenesis by acting on vascular endothelial growth factor (VEGF) and VEGF receptor (VEGFR2) which further inhibited the growth of prostate cancer. Experiments conducted on HUVEC and PC-3 cells showed that 20 μM of α-santalol inhibits protein kinase B pathway, extracellular-signal-related-kinase and other kinases in HUVEC, PC-3, and LNCaP cells and it also showed a decrease in the induced cell death and cell viability, particularly in PC-3 cells. Furthermore, a decrease in the number and mass of solid tumors was seen in a tumor xenograft model in immunodeficient nude mice. Ortizet al. [42] evaluated the genotoxicity and cytotoxicity of sandalwood oil in MCF-7 and MCF-10A breast cancer cell lines. The findings from this study suggest that 6 μg/mL and 8 μg/mL of sandalwood oil show both genotoxic and cytotoxic activity in MCF-7 cells but only cytotoxic activity in MCF-10A cells. It was also demonstrated that sandalwood oil is efficient at initiating breaks in single- and double-stranded DNA in MCF-7 cells. Using LC/MS-based quantitative proteomics approach, the proteins such as EPHX1, Ku70, Ku80, and 14–3-3ζ were found to be associated with sandalwood oil genotoxicity.
Dave et al. [43] administered 25% v/v of α-santalol in a phospholipid microemulsion transdermally through the skin and nipples of the breast of small animals to evaluate the efficacy of breast cancer prevention. Penetration in female Sprague-Dawley rats and porcine model, tissue localization in rats, and efficacy studies in carcinogenesis model were investigated. The results obtained from this study showed that microemulsion of α-santalol had the maximum penetration amongst the other formulations through the skin and nippleof the breast, whereas α-santalol was found to be widely distributed throughout the mammary glands when delivered by both nipples and breast skin than through nipples or breast skin alone [43]. Lee et al. [44] proved that East Indian sandalwood oil and its phytoconstituents α-santalol and β-santalol inhibited tubulin polymerization by directly binding to tubulin and also showed cytotoxic effects in head and neck squamous cell cancer (HNSCC) cells. Dozmorov et al. [45] reported the induction of selective apoptosis by frankincense oil and non-selective apoptosis by sandalwood oil on both UROtsa and J82 human bladder cells. They also showed the activation of stress and histone proteins by frankincense oil and GPCR (G protein-coupled receptors) by sandalwood oil respectively. Bommareddy et al. [46] reported that treatment with 20 μM and 40 μM of α-santalol prevented breast tumor growth through the β-catenin pathway that β-catenin translocation from the cytoplasm to the nucleus was hindered in MDA-MB-231 cells.
Sandalwood Oil Exerts Anti-inflammatory Activities
Li et al. [47] investigated a study in Sprague-Dawley rats to understand the effects of 8% sandalwood seed oil administered for 8 weeks on the inflammatory activity and fatty acid levels. The result showed a marked increase in docosahexaenoic acid (DHA), n-3 polyunsaturated fatty acid (PUFA), and inflammatory factors such as interleukin-1β (IL-1β) and prostaglandin E2 (PGE2). A study was conducted to assess the activity of East Indian sandalwood oil or Western Australian sandalwood oil on inflammatory activities in LPS-induced dermal fibroblast or keratinocyte co-culture. The results showed an increase in IL-6, CXCL-5 and MCP-1 levels, and IL-8 levels in LPS-stimulated dermal fibroblast and keratinocyte cultures respectively as well as suppression in the thromboxane B2 and PGE2 levels [48].
Sharma et al. [49] conducted a phase 2 trial in patients with eczema and psoriasis and demonstrated that East Indian sandalwood oil administered at a concentration of 0.001% and 0.002% applied topically for 8 weeks showed anti-inflammatory activity through inhibition of phosphodiesterase, nuclear factor kappa B (NF-κB), and production of cytokines. A 50% decrease was seen in eczema severity when East Indian sandalwood oil was topically applied. An open-label, single-center, phase 2 clinical study in psoriasis patients demonstrated that 10% w/w of East Indian sandalwood oil applied topically two times a day for 28 days showed a reduction in the generation of cytokines and suppression of Ki67, psoriasin, and inflammatory markers [50]. Baylac et al. [69] reported the anti-inflammatory activity of sandalwood oil in an in vitro study by inhibiting 5-lipoxygenase.
Other Therapeutic Activities of Sandalwood Oil and Its Constituents
Effects in Radiation Dermatitis
Pallatyet al. [51] conducted an investigator-blinded, single-center clinical trial to evaluate the efficacy of sandalwood oil and turmeric containing cream in the prevention of radiation dermatitis after topical application 5 times a day for 2 weeks in 50 patients with neck and head cancer undergoing radiation treatment. This study showed reduced incidence of grade 3 radiation dermatitis in cohorts applying a proprietary turmeric cream (containing 5% sandalwood oil) as compared to cohorts applying a commercially available baby oil, with no adverse reactions or allergies in both the groups. Further, Rao et al. [52] conducted an investigator-blinded randomized trial on a proprietary turmeric cream (comprised of 16% turmeric and 5% sandalwood oil) applied topically 5 times a day for 5 weeks to assess radiation dermatitis prevention in 40 patients with breast cancer. It was observed from this study that topical application of turmeric plus sandalwood oil cream reduced the occurrence and delayed the appearance of grades 1, 2, and 3 dermatitis when compared to the study group applying commercial baby oil. In addition, grade 4 radiation dermatitis did not develop in both groups. Both these studies suggest that more extensive double-blind, randomized trials should be conducted to further understand and assure the effectiveness of turmeric plus sandalwood oil cream in the treatment of ionizing radiation initiated dermatitis in patients with neck, head, and breast cancer undergoing radiation therapy.
Antibacterial Effects
A study was conducted in which inhibitory effect was shown by 30 μL of sandalwood oil along with 90 essential and 64 blended essential oils against Methicillin-resistant Staphylococcus aureus (MRSA) infection [53].
Another study showed the considerable efficacy of sandalwood oil (non-diluted) and other essential oils against gram-negative as well as gram-positive bacterial strains [70].
Effects in Eczema and Psoriasis
A phase 2 study was conducted to examine the potency, tolerability, and safety of a cream containing 5% and 10% East Indian sandalwood oil in eczema patients [71]. A multi-center, double-blind, randomized, phase 2 clinical trial has currently enrolled 69 plaque psoriasis patients who were treated by the application of a serum containing 10% East Indian sandalwood oil so as to assess the tolerability, potency, and efficacy [72]. A single-center, phase 2 clinical study is ongoing in 72 plaque psoriasis patients who are administered topically with 10% East Indian sandalwood oil contained in a serum [73]. An ongoing study is a randomized, phase 2 trial in 72 atopic dermatitis patients treated with a cream containing 5% East Indian sandalwood oil containing cream [74].
Antiviral Effects
Paulpandi et al. [58] investigated an antiviral (anti-influenza) effect of β-santalol which showed inhibition of viral mRNA synthesis and 86% of anti-influenza activity in MDCK cells at a 100 μg/mL concentration. Koch et al. [59] conducted an in vitro study showing an inhibition of Type-2 Herpes Simplex Virus by 0.0015% of sandalwood and other essential oils in RC-37 (African green monkey kidney cells). Benencia et al. [75] reported inhibition of replicas of Type 1 and Type 2 Herpes Simplex Virus thus demonstrating the antiviral activity of sandalwood oil.
Effects on Warts
A clinical trial has investigated the efficacy and safety profile after topical administration of an ointment comprising 10%, 20%, and 30% of East Indian sandalwood oil in Verruca vulgaris (common warts) patients [76]. A multi-center, randomized, phase 2 study evaluated 27 pediatric patients with Molluscum contagiosum (water warts) for safety and efficacy of a cream containing 10% of East Indian sandalwood oil [77]. However, this study was terminated for reasons unknown. Another ongoing open-label, phase 2 trial in external venereal warts patients investigated for the potency, tolerability, and safety of a cream that comprises 10% East Indian sandalwood oil [78].
Antifungal Effects
An investigation on ringworms (fungal) and yeast infection that included Candida, Escherichia coli, Trichophyton, and Microsporum strains showed efficacious effects with 0.06%, > 2%, 25 μg/mL, and > 10% of sandalwood oil respectively [63,64,65,66].
Effects on Physiological and Behavioral Parameters
Hongratanaworakit et al. [67] initiated a clinical trial in 36 healthy human volunteers to evaluate whether the physiological and behavioral (emotional and mental) parameters are modulated by East Indian sandalwood oil. Behavioral aspects were measured by the visual analog scale. A reduction in the systolic blood pressure, eye blink rate, and arousal was observed when α-santalol was administered transdermally.
Effects on Cholinesterases and Tyrosinases
Misra et al. [79] reported that 50 μg/mL of α-santalol acts as a strong cholinesterase and tyrosinase inhibitor in an in vitro study.
Effects in Oral Mucositis
An open-label, phase 2 clinical study was carried out in radiation-induced mouth sores (oral mucositis) patients to examine the efficacy, tolerability, and safety of a mouth rinse containing 0.25% East Indian sandalwood oil [15].
Effects in Chronic Angina Pectoris
An ongoing randomized, early phase 1 clinical trial by Chengdu University of Traditional Chinese Medicine has enrolled 200 participants to evaluate the safety and potency of a mixture of Traditional Chinese herbal medicine, containing santalum and other herbs, upon acupoint application in chronic angina pectoris patients [80].
Table 2 summarizes various clinical trials on East Indian sandalwood oil containing formulations in various diseases for the benefit of the reader.
Safety Profile of Sandalwood Oil
α-Santalol, the major phytoconstituent of sandalwood oil, was found to have an acute oral lethal dose (LD50) of 3.8 g/kg in rats and an acute dermal lethal dose (LD50) of more than 5 g/kg in rabbits [81]. Similarly, acute oral lethal dose (LD50) of 5.58 g/kg and an acute dermal lethal dose (LD50) of more than 5 g/kg of sandalwood oil was reported in rats and rabbits respectively [81]. Concentrated sandalwood oil upon application to the rear surface of the hairless mouse skin was reported to be slightly irritating whereas sandalwood oil was not photoirritating [81]. Sandalwood oil was reported to show irritation when it was applied to the whole or undamaged skin of rabbit [81]. Sandalwood oil of Santalum album variety was found to be allergic in 0.1–2.4% of the population [19]. Rudzkiet al. [82] reported that 5 subjects out of 450 subjects with dermatitis showed positive results (sensitive to essential oil) with sandalwood oil when 35 essential oils and their standards were tested. Hayakawa et al. [83] investigated 10% of sandalwood oil in petrolatum and reported a loss of pigmentation and dermatitis when a patch test was conducted. This was observed due to the sandalwood fragrance volatilized from the joss stick that comes in contact with the skin. A 24- and 48-h patch study conducted in 18 human volunteers showed that there was no irritating effect upon application of concentrated sandalwood oil and 10% sandalwood oil in petrolatum respectively. Furthermore, 20% of α-santalol in petrolatum was also found to be non-irritant to the skin [81]. A reported study by Larsen et al. conducted in North American and Central European patients showed that 1.8% population had irritation whereas 6.6% had an allergy to sandalwood oil when patch test was carried out [84].
Conclusions and Future Perspectives
Sandalwood oil and α-santalol have been reported to show beneficial effects in the chemoprevention of primarily skin cancer as well as various other cancers. The molecular basis for such anticancer effects may be attributed to changes in critical cancer signaling pathways such as MAPK, AP-1, β-catenin, and PI3K/Akt pathways as well as activation of caspases/PARP and upregulation of p21. Sandalwood oil also exerts anti-inflammatory activity via PGE2, IL-1β, and inhibition of the NF-κB pathway and 5-lipoxygenase. In addition, sandalwood oil and its constituents exhibit other therapeutic activities in eczema/psoriasis, radiation dermatitis, antifungal, antibacterial, antiviral, etc. Table 3
summarizes the non-clinical and clinical efficacy of sandalwood oil and α-santalol in various diseases including the dose and routes of administration. Sandalwood oil has an acceptable safety profile and is generally well-tolerated. Clinical trials have majorly focused on the other therapeutic activities mentioned above. Further efforts devoted to clinical trials of sandalwood oil as an adjunct to chemotherapy for skin cancers or immunotherapy for melanoma will likely shed more light on the chemopreventive potential of sandalwood oil in melanoma/non-melanoma skin cancers.
Abbreviations
- A431 cells:
-
Human epidermoid carcinoma cell line
- AP-1:
-
Activator protein 1
- BCC:
-
Basal cell carcinoma
- COX-2:
-
Cyclooxygenase-2
- DHA:
-
Docosahexenoic acid
- DMBA:
-
7,12-Dimethylbenz(a) anthracene
- GPCR:
-
G protein-coupled receptor
- GST:
-
Glutathione-S-transferase
- HaCaT:
-
Cultured human keratinocyte cells
- HUVEC:
-
Human umbilical vein endothelial cells
- IL:
-
Interleukin
- J82:
-
Human bladder carcinoma cell line
- LC3:
-
Microtubule-associated protein 1 light chain 3
- LD50 :
-
Lethal dose (in 50% of population)
- LNCaP:
-
Lymph node carcinoma of the prostate (prostate cancer cells)
- LPS:
-
Lipopolysaccharide
- MAPK:
-
Mitogen-activated protein kinase
- MCF-7:
-
Michigan Cancer Foundation-7 (breast cancer cells)
- MCF-10A:
-
Normal mammary epithelial cells
- MDA-MB 231 cells:
-
Triple-negative breast cancer cell line
- MDCK:
-
Madin-Darby canine kidney cells
- ODC:
-
Ornithine decarboxylase
- p53:
-
Tumor suppressor protein
- PC-3:
-
Prostate cancer cell line
- PI3K:
-
Phosphatidylinositol-3-kinase
- PUFA:
-
Polyunsaturated fatty acid
- SCC:
-
Squamous cell carcinoma
- TPA:
-
12-O-tetradecanoyl phorbol-13-acetate
- UV:
-
Ultraviolet
- UROtsa:
-
Human urothelial cell line
- VAS:
-
Visual analog scale
- VEGF:
-
Vascular endothelial growth factor
- VEGFR2:
-
Vascular endothelial growth factor receptor 2
References
Goh KJ, Tan CT, Chew NK, Tan PS, Kamarulzaman A, Sarji SA, et al. Clinical features of Nipah virus encephalitis among pig farmers in Malaysia. N Engl J Med. 2000;342(17):1229–35.
Hsu VP, Hossain MJ, Parashar UD, Ali MM, Ksiazek TG, Kuzmin I, et al. Nipah virus encephalitis reemergence, Bangladesh. Emerg Infect Dis. 2004;10(12):2082–7.
Sazzad HM, Hossain MJ, Gurley ES, Ameen KM, Parveen S, Islam MS, et al. Nipah virus infection outbreak with nosocomial and corpse-to-human transmission, Bangladesh. Bangladesh. Emerg Infect Dis. 2013;19(2):210–7.
Ang BSP, Lim TCC,Wang L. Nipah virus infection. J Clin Microbiol 2018; 56(6):
Rogers HW, Weinstock MA, Feldman SR, Coldiron BM. Incidence estimate of nonmelanoma skin cancer (keratinocyte carcinomas) in the U.S. population, 2012. JAMA Dermatol. 2015;151(10):1081–6.
Hassan MZ, Sazzad HMS, Luby SP, Sturm-Ramirez K, Bhuiyan MU, Rahman MZ, et al. Nipah virus contamination of hospital surfaces during outbreaks, Bangladesh, 2013-2014. Emerg Infect Dis. 2018;24(1):15–21.
Nahar N, Paul RC, Sultana R, Sumon SA, Banik KC, Abedin J, et al. A controlled trial to reduce the risk of human Nipah virus exposure in Bangladesh. Ecohealth. 2017;14(3):501–17.
Prasad N, Radhiga T, Agilan B, Muzaffer U, Karthikeyan R, Kanimozhi G, et al. Phytochemicals as modulators of ultraviolet-b radiation induced cellular and molecular events: a review. Journal of Radiation and Cancer Research 2016; 7(1).
Chadha MS, Comer JA, Lowe L, Rota PA, Rollin PE, Bellini WJ, et al. Nipah virus-associated encephalitis outbreak, Siliguri, India. Emerg Infect Dis. 2006;12(2):235–40.
Cohuet S, Marquer C, Shepherd S, Captier V, Langendorf C, Ale F, et al. Intra-household use and acceptability of ready-to-use-supplementary-foods distributed in Niger between July and December 2010. Appetite. 2012;59(3):698–705.
Saw CL, Huang MT, Liu Y, Khor TO, Conney AH, Kong AN. Impact of Nrf2 on UVB-induced skin inflammation/photoprotection and photoprotective effect of sulforaphane. Mol Carcinog. 2011;50(6):479–86.
Cortes MC, Cauchemez S, Lefrancq N, Luby SP, Jahangir Hossain M, Sazzad HMS, et al. Characterization of the spatial and temporal distribution of Nipah virus spillover events in Bangladesh, 2007-2013. J Infect Dis. 2018;217(9):1390–4.
Isanaka S, Guesdon B, Labar AS, Hanson K, Langendorf C, Grais RF. Comparison of clinical characteristics and treatment outcomes of children selected for treatment of severe acute malnutrition using mid upper arm circumference and/or weight-for-height Z-score. PLoS One. 2015;10(9):e0137606.
Nair S. Pharmacometrics and systems pharmacology of immune checkpoint inhibitor nivolumab in cancer translational medicine. Advances in Modern Oncology Research 2016; 2(1).
Islam MS, Sazzad HM, Satter SM, Sultana S, Hossain MJ, Hasan M, et al. Nipah virus transmission from bats to humans associated with drinking traditional liquor made from date palm sap, Bangladesh, 2011-2014. Emerg Infect Dis. 2016;22(4):664–70.
Nair S, Iyer A, Vijay V, Bandlamudi S, Llerena A. Pharmacokinetics and systems pharmacology of monoclonal antibody olaratumab for inoperable soft tissue sarcoma. Advances in Modern Oncology Research 2017; 3(3).
Gurley ES, Montgomery JM, Hossain MJ, Bell M, Azad AK, Islam MR, et al. Person-to-person transmission of Nipah virus in a Bangladeshi community. Emerg Infect Dis. 2007;13(7):1031–7.
Arunkumar AN, Joshi GY, Mohan Ram H. Sandalwood: History, uses, present status and the future, 2012.
Moy RL, Levenson C. Sandalwood album oil as a botanical therapeutic in dermatology. J Clin Aesthet Dermatol. 2017;10(10):34–9.
Moniodis J, Jones CG, Renton M, Plummer JA, Barbour EL, Ghisalberti EL, et al. Sesquiterpene Variation in West Australian Sandalwood (Santalum spicatum). Molecules 2017; 22(6):
Bulle S, Reddyvari H, Nallanchakravarthula V, Vaddi DR. Therapeutic potential of Pterocarpus santalinus L.: an update. Pharmacogn Rev. 2016;10(19):43–9.
Brophy JJ, Fookes CJR, Lassak EV. Constituents of Santalum spicatum (R.Br.) A. DC. Wood Oil. J Essent Oil Res. 1991;3(6):381–5.
Valder C, Neugebauer M, Meier M, Kohlenberg B, Hammerschmidt F-J,Braun N: Western Australian sandalwood oil - new constituents of santalum spicatum (R. Br.) A. DC. (Santalaceae), 2003.
Braun NA, Sim S, Kohlenberg B, Lawrence BM. Hawaiian sandalwood: oil composition of Santalum paniculatum and comparison with other sandal species. Nat Prod Commun. 2014;9(9):1365–8.
Page T, Southwell I, Russell M, Tate H, Tungon J, Sam C, et al. Geographic and phenotypic variation in heartwood and essential-oil characters in natural populations of Santalum austrocaledonicum in Vanuatu. Chem Biodivers. 2010;7(8):1990–2006.
Harbaugh DT, Baldwin BG. Phylogeny and biogeography of the sandalwoods (Santalum, Santalaceae): repeated dispersals throughout the Pacific. Am J Bot. 2007;94(6):1028–40.
Rached W, Calhelha RC, Fernandes Â, Carvalho AM, Bennaceur M, Marouf A, et al. Phytochemical characterization and bioactive properties of Osyris quadripartita Salzm. ex Decne. leaves from Algeria. RSC Adv. 2016;6(76):72768–76.
Kreipl AT, Konig WA. Sesquiterpenes from the east African sandalwood Osyris tenuifolia. Phytochemistry. 2004;65(14):2045–9.
Bossart KN, Wang LF, Flora MN, Chua KB, Lam SK, Eaton BT, et al. Membrane fusion tropism and heterotypic functional activities of the Nipah virus and Hendra virus envelope glycoproteins. J Virol. 2002;76(22):11186–98.
Zhang X, Dwivedi C. Skin cancer chemoprevention by alpha-santalol. Front Biosci (Schol Ed). 2011;3:777–87.
Dickinson SE, Olson ER, Levenson C, Janda J, Rusche JJ, Alberts DS, et al. A novel chemopreventive mechanism for a traditional medicine: East Indian sandalwood oil induces autophagy and cell death in proliferating keratinocytes. Arch Biochem Biophys. 2014;558:143–52.
Kaur M, Agarwal C, Singh RP, Guan X, Dwivedi C, Agarwal R. Skin cancer chemopreventive agent, {alpha}-santalol, induces apoptotic death of human epidermoid carcinoma A431 cells via caspase activation together with dissipation of mitochondrial membrane potential and cytochrome c release. Carcinogenesis. 2005;26(2):369–80.
Zhang X, Chen W, Guillermo R, Chandrasekher G, Kaushik RS, Young A, et al. Alpha-santalol, a chemopreventive agent against skin cancer, causes G2/M cell cycle arrest in both p53-mutated human epidermoid carcinoma A431 cells and p53 wild-type human melanoma UACC-62 cells. BMC Res Notes. 2010;3:220.
Dwivedi C, Guan X, Harmsen WL, Voss AL, Goetz-Parten DE, Koopman EM, et al. Chemopreventive effects of alpha-santalol on skin tumor development in CD-1 and SENCAR mice. Cancer Epidemiol Biomarkers Prevent : Public Am Assoc Cancer RES Cosponsored Am Soc Prevent Oncol. 2003;12(2):151–6.
Dwivedi C, Abu-Ghazaleh A. Chemopreventive effects of sandalwood oil on skin papillomas in mice. Eur J Cancer Prev. 1997;6(4):399–401.
Dwivedi C, Valluri HB, Guan X, Agarwal R. Chemopreventive effects of alpha-santalol on ultraviolet B radiation-induced skin tumor development in SKH-1 hairless mice. Carcinogenesis. 2006;27(9):1917–22.
Arasada BL, Bommareddy A, Zhang X, Bremmon K, Dwivedi C. Effects of alpha-santalol on proapoptotic caspases and p53 expression in UVB irradiated mouse skin. Anticancer Res. 2008;28(1A):129–32.
Santha S, Dwivedi C. Alpha-santalol, a skin cancer chemopreventive agent with potential to target various pathways involved in photocarcinogenesis. Photochem Photobiol. 2013;89(4):919–26.
Chilampalli C, Zhang X, Kaushik RS, Young A, Zeman D, Hildreth MB, et al. Chemopreventive effects of combination of honokiol and magnolol with alpha-santalol on skin cancer developments. Drug Discov Ther. 2013;7(3):109–15.
Banerjee S, Ecavade A, Rao AR. Modulatory influence of sandalwood oil on mouse hepatic glutathione S-transferase activity and acid soluble sulphydryl level. Cancer Lett. 1993;68(2–3):105–9.
Saraswati S, Kumar S, Alhaider AA. alpha-santalol inhibits the angiogenesis and growth of human prostate tumor growth by targeting vascular endothelial growth factor receptor 2-mediated AKT/mTOR/P70S6K signaling pathway. Mol Cancer. 2013;12:147.
Ortiz C, Morales L, Sastre M, Haskins WE, Matta J. Cytotoxicity and genotoxicity assessment of sandalwood essential oil in human breast cell lines MCF-7 and MCF-10A. Evid Based Complement Alternat Med. 2016;2016:3696232.
Dave K, Alsharif FM, Islam S, Dwivedi C, Perumal O. Chemoprevention of breast cancer by transdermal delivery of alpha-santalol through breast skin and mammary papilla (nipple). Pharm Res. 2017;34(9):1897–907.
Lee B, Bohmann J, Reeves T, Levenson C, Risinger AL. Alpha- and beta-santalols directly interact with tubulin and cause mitotic arrest and cytotoxicity in oral cancer cells. J Nat Prod. 2015;78(6):1357–62.
Dozmorov MG, Yang Q, Wu W, Wren J, Suhail MM, Woolley CL, et al. Differential effects of selective frankincense (Ru Xiang) essential oil versus non-selective sandalwood (Tan Xiang) essential oil on cultured bladder cancer cells: a microarray and bioinformatics study. Chin Med. 2014;9:18.
Bommareddy A, Knapp K, Nemeth A, Steigerwalt J, Landis T, Vanwert AL, et al. Alpha-santalol, a component of sandalwood oil inhibits migration of breast cancer cells by targeting the beta-catenin pathway. Anticancer Res. 2018;38(8):4475–80.
Li G, Singh A, Liu Y, Sunderland B, Li D. Comparative effects of sandalwood seed oil on fatty acid profiles and inflammatory factors in rats. Lipids. 2013;48(2):105–13.
Sharma M, Levenson C, Bell RH, Anderson SA, Hudson JB, Collins CC, et al. Suppression of lipopolysaccharide-stimulated cytokine/chemokine production in skin cells by sandalwood oils and purified alpha-santalol and beta-santalol. Phytother Res. 2014;28(6):925–32.
Sharma M, Levenson C, Browning JC, Becker EM, Clements I, Castella P, et al. East Indian sandalwood oil is a phosphodiesterase inhibitor: a new therapeutic option in the treatment of inflammatory skin disease. Front Pharmacol. 2018;9:200.
Sharma M, Levenson C, Clements I, Castella P, Gebauer K, Cox ME. East Indian Sandalwood Oil (EISO) alleviates inflammatory and proliferative pathologies of psoriasis. Front Pharmacol. 2017;8:125.
Palatty PL, Azmidah A, Rao S, Jayachander D, Thilakchand KR, Rai MP, et al. Topical application of a sandal wood oil and turmeric based cream prevents radiodermatitis in head and neck cancer patients undergoing external beam radiotherapy: a pilot study. Br J Radiol. 2014;87(1038):20130490.
Rao S, Hegde SK, Baliga-Rao MP, Lobo J, Palatty PL, George T, et al. Sandalwood oil and turmeric-based cream prevents ionizing radiation-induced dermatitis in breast cancer patients: clinical study. Medicines (Basel) 2017; 4(3).
Chao S, Young G, Oberg C, Nakaoka K. Inhibition of methicillin-resistant Staphylococcus aureus (MRSA) by essential oils 2008; 23(6):444–449.
ClinicalTrials.gov: ClinicalTrials.gov (2018). A Trial of a Botanical Drug Containing East Indian Sandalwood Oil (EISO) For Treatment of Atopic Dermatitis, 2018.
ClinicalTrials.gov: ClinicalTrials.gov (2018). A trial of a botanical drug containing East Indian Sandalwood Oil (EISO) for treatment of mild-to-moderate plaque psoriasis., 2018.
ClinicalTrials.gov: ClinicalTrials.gov (2018). A trial of a botanical drug containing East Indian Sandalwood Oil (EISO) for treatment of plaque psoriasis in adults., 2018.
ClinicalTrials.gov: ClinicalTrials.gov (2017). A trial of a botanical drug product containing East Indian Sandalwood Oil (EISO) For Treatment of Atopic Dermatitis, 2017.
Paulpandi M, Kannan S, Thangam R, Kaveri K, Gunasekaran P, Rejeeth C. In vitro anti-viral effect of beta-santalol against influenza viral replication. Phytomedicine. 2012;19(3–4):231–5.
Koch C, Reichling J, Schneele J, Schnitzler P. Inhibitory effect of essential oils against herpes simplex virus type 2. Phytomedicine. 2008;15(1–2):71–8.
ClinicalTrials.gov: ClinicalTrials.gov (2017). A trial of a botanical drug containing East Indian Sandalwood Oil (EISO) for treatment of common warts., 2017.
ClinicalTrials.gov: ClinicalTrials.gov (2017). A trial of a botanical drug containing East Indian Sandalwood Oil (EISO) for the treatment of Molluscum Contagiosum., 2017.
ClinicalTrials.gov: ClinicalTrials.gov (2017). A trial of a botanical drug containing East Indian Sandalwood Oil (EISO) for the treatment of external genital warts., 2017.
Hammer KA, Carson CF, Riley TV. Antimicrobial activity of essential oils and other plant extracts. J Appl Microbiol. 1999;86(6):985–90.
Hammer KA, Carson CF, Riley TV. In-vitro activity of essential oils, in particular Melaleuca alternifolia (tea tree) oil and tea tree oil products, against Candida spp. J Antimicrob Chemother. 1998;42(5):591–5.
Inouye S, Uchida K, Abe S. Vapor activity of 72 essential oils against a Trichophyton mentagrophytes. J Infect Chemother. 2006;12(4):210–6.
Nardoni S, Giovanelli S, Pistelli L, Mugnaini L, Profili G, Pisseri F, et al. In vitro activity of twenty commercially available, plant-derived essential oils against selected dermatophyte species. Nat Prod Commun. 2015;10(8):1473–8.
Hongratanaworakit T, Heuberger E, Buchbauer G. Evaluation of the effects of East Indian Sandalwood Oil and alpha-santalol on humans after transdermal absorption. Planta Med. 2004;70(1):3–7.
ClinicalTrials.gov: ClinicalTrials.gov (2017). A trial of a botanical drug containing East Indian Sandalwood Oil (EISO) for the treatment of oral mucositis., 2017.
Baylac S, Racine P. Inhibition of 5-lipoxygenase by essential oils and other natural fragrant extracts. Int J Aromather. 2003;13(2):138–42.
Warnke PH, Becker ST, Podschun R, Sivananthan S, Springer IN, Russo PA, et al. The battle against multi-resistant strains: renaissance of antimicrobial essential oils as a promising force to fight hospital-acquired infections. J Cranio-maxillo-facial surgery : Off Public Eur Assoc Cranio-Maxillo-Facial Surg. 2009;37(7):392–7.
Naser AM, Hossain MJ, Sazzad HM, Homaira N, Gurley ES, Podder G, et al. Integrated cluster- and case-based surveillance for detecting stage III zoonotic pathogens: an example of Nipah virus surveillance in Bangladesh. Epidemiol Infect. 2015;143(9):1922–30.
Hahn MB, Epstein JH, Gurley ES, Islam MS, Luby SP, Daszak P, et al. Roosting behaviour and habitat selection of Pteropus giganteus reveals potential links to Nipah virus epidemiology. J Appl Ecol. 2014;51(2):376–87.
Nahar N, Mondal UK, Hossain MJ, Khan MS, Sultana R, Gurley ES, et al. Piloting the promotion of bamboo skirt barriers to prevent Nipah virus transmission through date palm sap in Bangladesh. Glob Health Promot. 2014;21(4):7–15.
Sazzad HM, Luby SP, Stroher U, Daszak P, Sultana S, Afroj S, et al. Exposure-based screening for Nipah virus encephalitis. Bangladesh Emerg Infect Dis. 2015;21(2):349–51.
Benencia F, Courreges MC. Antiviral activity of sandalwood oil against herpes simplex viruses-1 and -2. Phytomedicine. 1999;6(2):119–23.
Chakraborty A, Sazzad HM, Hossain MJ, Islam MS, Parveen S, Husain M, et al. Evolving epidemiology of Nipah virus infection in Bangladesh: evidence from outbreaks during 2010-2011. Epidemiol Infect. 2016;144(2):371–80.
Parveen S, Islam MS, Begum M, Alam MU, Sazzad HM, Sultana R, et al. It’s not only what you say, it’s also how you say it: communicating nipah virus prevention messages during an outbreak in Bangladesh. BMC Public Health. 2016;16:726.
Hegde ST, Sazzad HM, Hossain MJ, Alam MU, Kenah E, Daszak P, et al. Investigating rare risk factors for Nipah virus in Bangladesh: 2001-2012. Ecohealth. 2016;13(4):720–8.
Misra BB, Dey S. TLC-bioautographic evaluation of in vitro anti-tyrosinase and anti-cholinesterase potentials of sandalwood oil. Nat Prod Commun. 2013;8(2):253–6.
Nahar N, Paul RC, Sultana R, Gurley ES, Garcia F, Abedin J, et al. Raw sap consumption habits and its association with knowledge of Nipah virus in two endemic districts in Bangladesh. PLoS One. 2015;10(11):e0142292.
Opdyke DLJ: Monographs on fragrance raw materials, Pergamon Press, 1974.
Rudzki E, Grzywa Z. Balsam of Peru as screening agent for essential oils sensitivity. Dermatologica. 1977;155(2):115–21.
Hayakawa R, Matsunaga K, Arima Y. Depigmented contact dermatitis due to incense. Contact Dermatitis. 1987;16(5):272–4.
Warshaw EM, Zug KA, Belsito DV, Fowler JF Jr, DeKoven JG, Sasseville D, et al. Positive patch-test reactions to essential oils in consecutive patients from North America and Central Europe. Dermatitis. 2017;28(4):246–52.
Acknowledgments
The authors thank Viral Bakhai of ViralAnimationz (https://viralanimationz.wixsite.com/website) for his assistance in drawing the electronic version of Fig. 3.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Cancer Chemoprevention
Rights and permissions
About this article

Cite this article
Jain, R., Nair, S. Sandalwood Oil for the Chemoprevention of Skin Cancer: Mechanistic Insights, Anti-inflammatory, and In Vivo Anticancer Potential. Curr Pharmacol Rep 5, 345–358 (2019). https://doi.org/10.1007/s40495-019-00195-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40495-019-00195-4