
Abstract
Introduction
Approximately one-half of patients with epidermal growth factor receptor (EGFR) mutation-positive advanced/metastatic non-small-cell lung cancer (NSCLC) develop resistance to first- or second-generation EGFR tyrosine kinase inhibitors (TKIs) due to a secondary T790M mutation. This study investigated the pattern of T790M testing after EGFR TKI treatment in a real-world setting in Japan.
Method
This prospective observational study enrolled patients with EGFR mutation-positive advanced/metastatic NSCLC who reported disease progression during treatment with first- or second-generation EGFR TKIs. Data regarding sampling methods for T790M mutation testing (plasma sample, cytology or tissue biopsy) and the treatment strategies after disease progression were recorded prospectively.
Results
A total of 236 patients were included in the study (female, 67.4%; median age, 73.0 years), and 205 patients (86.9%) underwent rebiopsy by any of the three possible methods: plasma sampling in 137 patients (58.1%) and tissue/cytology sampling in 68 patients (28.8%) during the first rebiopsy. Overall, 80.6% of the tissue/cytology samples contained tumor cells, and 40% of these samples were positive for the T790M mutation. T790M mutations were detected in only 19.7% of plasma samples. Of the 199 patients who underwent T790M testing, 61 (30%) tested positive, and 56 (91.8%) subsequently received osimertinib.
Conclusion
Among the 87% of Japanese patients who underwent rebiopsy after progressing on treatment with a first- or second-generation EGFR TKI, approximately 30% tested positive for the T790M mutation and were eligible to receive osimertinib. Although plasma sampling is non-invasive, this rebiopsy method is less sensitive for T790M detection compared with tissue or cytology sampling (UMIN identifier: UMIN000024928).
Funding
AstraZeneca Japan.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
For patients with advanced/metastatic non-small-cell lung cancer (NSCLC), identification of optimal therapy requires access to molecular diagnostic testing to guide selection of a therapy with demonstrated effectiveness against the molecular defects relevant to each individual patient. Currently, patients with NSCLC and epidermal growth factor receptor (EGFR) mutations that render them sensitive to tyrosine kinase inhibitors (TKIs) are treated with first- or second-generation EGFR TKIs as first-line therapy [1, 2]. EGFR TKI-sensitizing mutations, such as exon 19 deletion and L858R, are common in patients with advanced/metastatic NSCLC, with an incidence of over 50% in Asian populations [3]. Despite high tumor response rates with first-line EGFR TKIs, disease progression occurs in most patients after 9–13 months of treatment with EGFR TKIs [4,5,6,7,8,9]. The most common mechanism of resistance to EGFR TKI therapy, reported in about 50% of patients, is the development of a secondary mutation in EGFR, specifically an amino acid substitution from the original threonine to methionine at position 790 (EGFR T790M) [10,11,12].
Third-generation EGFR TKIs that selectively target the EGFR T790M mutation are in development to overcome this resistance [13,14,15]. Osimertinib is a third-generation, irreversible EGFR TKI that selectively inhibits both EGFR TKI-sensitizing and EGFR T790M resistance mutations [16]. Based on the positive results of the AURA clinical trial program, osimertinib is currently approved in many countries for the treatment of patients with EGFR T790M mutation-positive NSCLC who experience disease progression during or after first-line therapy with first- or second-generation EGFR TKIs [17,18,19]. In the confirmatory phase III study conducted in patients with T790M mutation-positive advanced NSCLC who had disease progression after first-line EGFR TKI therapy, progression-free survival was significantly longer with second-line osimertinib than with second-line standard chemotherapy (median progression-free survival, 10.1 versus 4.4 months; hazard ratio, 0.30; p < 0.001) [19]. The recent FLAURA study also showed that first-line osimertinib was more effective than standard EGFR TKIs for prolonging progression-free survival in untreated patients with EGFR TKI-sensitizing mutation-positive advanced NSCLC [20].
Detection of the EGFR T790M mutation in patients is necessary before initiating osimertinib. Currently, the cobas® EGFR Mutation Test v2 (Roche Molecular Diagnostics, Basel, Switzerland) is approved as a companion diagnostic test for the detection of EGFR mutations and is widely used in Japan [21]. However, identification of patients who have developed EGFR TKI resistance as a result of the T790M mutation is complicated by several factors. Tissue/cytology sampling is invasive and may not always be feasible because of the difficulty of accessing certain tumor sites [22]. Furthermore, tissue/cytology samples do not always contain adequate amounts of tumor cells for detection [23]. Although it is feasible to obtain blood samples in almost all patients for use in liquid biopsy, a noninvasive detection technique that relies on circulating tumor DNA (ctDNA), the sensitivity of liquid biopsy is lower compared with the use of tissue samples, and not all tumors shed ctDNA in the plasma [24, 25]. For example, cobas® testing of plasma samples has a sensitivity of 41–64% for T790M mutation detection when compared with cobas® testing of tissue samples and a concordance of 57–86% with tissue samples [24].
Currently, limited data are available on the proportion of patients identified as T790M positive after EGFR TKI treatment in the real-world clinical setting, particularly from studies conducted after marketing approval of the third-generation EGFR TKI osimertinib. The present study aimed to demonstrate the real-world identification of T790M mutation-positive patients by investigating the pattern of rebiopsy and T790M testing among patients with EGFR mutation-positive advanced/metastatic NSCLC who experienced disease progression during EGFR TKI treatment in Japan. This study also describes patient treatment after T790M testing results.
Methods
Study Design
This prospective multicenter observational study conducted at 49 medical centers in Japan (UMIN-Clinical Trial Registry ID: UMIN000024928) enrolled patients with EGFR mutation-positive advanced/metastatic NSCLC who reported disease progression during treatment with first- or second-generation EGFR TKIs. The study included patients aged ≥ 20 years with EGFR mutation-positive advanced/metastatic NSCLC in whom disease progression had been reported with first- or second-generation EGFR TKIs and who were able to provide written informed consent. Patients were excluded from the study if they had been previously treated with T790M-targeted EGFR TKI therapy if they received EGFR TKI therapy with more than two different TKIs (except for patients who switched TKIs because of toxicity) or if the patient’s medical history before disease progression was unavailable. At enrollment, information regarding diagnosis and treatment of NSCLC was collected retrospectively from patients’ medical charts. Data regarding sample collection, T790M testing and subsequent treatment were recorded prospectively using electronic case report forms. Patients who were enrolled in an early access program that provided access to liquid biopsy testing for the T790M mutation without financial cost to the patient were also eligible to participate in the current study. In National Hospital Organization centers, the study protocol was approved by the central review board. In other study centers, the study protocol was approved by the ethics committee/institutional review board at each study center. The study was conducted in accordance with the ethical principles of the Declaration of Helsinki, International Conference on Harmonisation guidelines for Good Clinical Practice and the ethical guidelines for epidemiologic research in Japan and/or ethical guidelines for clinical research in Japan for noninterventional studies, and ethical guidelines for medical and health research involving humans. All patients included in the study provided written informed consent.
Study Measures
The primary objectives of the study were to determine the tissue/cytology/plasma rebiopsy rate among patients with disease progression during treatment with EGFR TKIs, reason for selection of each sample, T790M testing rate, T790M detection rate and treatment pattern by T790M test result. Secondary objectives included determination of the tissue/cytology rebiopsy status (sampling lesion, sampling method and success rate) and T790M detection rate by prior therapy. Sampling success was defined as having obtained tumor cells in the tissue or cytology samples.
Statistical Analysis
All analyses were descriptive in nature. Categorical study measures (e.g., sex) were reported using frequency and proportions, and continuous measures (e.g., age) were reported using median and range (minimum to maximum value). No statistical power calculation was undertaken because of the descriptive nature of this study, but we had expected to enroll approximately 300 patients between 6 January and 31 May 2017, based on a preliminary feasibility survey in a respiratory cancer group in the National Hospital Organization. However, the enrollment was slower than expected, so the recruitment period was extended to 31 August 2017. At this time, a decision was made to proceed with the study with the existing patient cohort rather than continue to extend the recruitment period.
Results
Patients
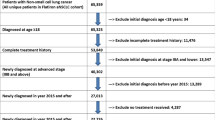
A total of 243 patients were enrolled at 44 medical centers in Japan from 6 January 2017 to 31 August 2017, but 7 patients were excluded because they did not meet the study eligibility criteria (Fig. 1); therefore, 236 patients [female, 67.4%; median age, 73.0 years (range 40–93)] were included in the full analysis set (FAS) (Table 1). Instead of enrolling the patients after disease progression before sample collection for T790M testing, 11 patients were enrolled after availability of the T790M result because of procedural error. Nonetheless, all of them met the eligibility criteria and were included in the FAS based on the predefined statistical analysis plan. All 236 patients included in the FAS were positive for EGFR TKI-sensitizing mutations, and 1 patient was also positive for the T790M mutation at initial diagnosis (Table 1). Most patients (n = 173/236) were enrolled during the early access program that allowed access to liquid biopsy testing for the T790M mutation (Table S1). Information on subsequent treatment was collected for 213 patients (Fig. 1).

Overview of patient status for patients enrolled in the study (N = 243) and included in the full analysis set (N = 236). EGFR epidermal growth factor receptor, NSCLC non-small-cell lung cancer, TKI tyrosine kinase inhibitor. T790M+ indicates positive for T790M mutation; T790M− indicates no T790M mutation. aIncluding 11 patients identified retrospectively; bT790M testing was not performed in 13 patients because no tumor cells were obtained; cT790M testing was not performed in eight patients because no tumor cells were obtained
Rebiopsy Rate and Sample Type
Rebiopsy after disease progression, including “liquid biopsy” using plasma sampling, occurred in 205 (86.9%) of the 236 patients (Table 2). Of the 236 patients in the study, the samples selected for initial rebiopsy most commonly were plasma (58.1%) followed by tissue (17.4%) and cytology specimens (11.4%). No samples were collected from 31 patients (13.1%). The proportion of patients in whom plasma sampling occurred was 67.1% for patients enrolled during the period of the early access program and 33.3% for patients enrolled after the program’s conclusion (Table S1). Sample collection rate and sample type by sex, age at disease progression and Eastern Cooperative Oncology Group performance status are shown in Table 2.
Second and third rebiopsies were conducted in 50 and 8 patients, respectively, based on T790M-negative or unknown results in 156 patients after a first rebiopsy (Fig. 1). Among the 46 patients with T790M-negative/unknown results who initially provided tissue/cytology samples, 13 (28.3%) underwent additional sampling, and T790M mutations were detected in 3 (23.1%). Of the remaining ten patients, three underwent a third rebiopsy, and one of these biopsies was positive for a T790M mutation. Of the 110 patients with T790M-negative results who initially provided plasma samples, 37 (33.6%) underwent additional sampling, and T790M mutations were detected in 6 (16.2%). Five of the 31 patients with a negative or unknown T790M result on the second rebiopsy underwent a third rebiopsy, of which 2 were positive for T790M mutation (Fig. 1). Therefore, 12 patients with negative T790M results on the first rebiopsy had a mutation detected on the second or third rebiopsy. Overall, rebiopsies using tissue/cytology samples were conducted 108 times including repeated sampling, and tumor cells were successfully obtained in 80.6% of the 108 total tissue/cytology rebiopsy samples collected (Table 3).
The most common reason cited for the use of tissue/cytology samples for T790M mutation assay was concern regarding the sensitivity of the plasma test (tissue samples, 82.9%; cytology samples, 81.5%), while the most common reason cited for the selection of plasma samples was concern regarding the use of invasive sampling techniques (64.2%). The reasons given for no sample collection included no appropriate lesion for tissue/cytology sampling (45.2%), patient refusal of tissue/cytology sampling (9.7%), T790M testing before enrollment (9.7%), rapid disease progression (6.5%), continuation of first- or second-generation EGFR TKI treatment after disease progression (6.5%), or selection of best supportive care after disease progression (6.5%).
T790M Mutation Testing Rate and Detection Rate
T790M mutation testing occurred in 199 of the 236 patients included in the FAS; 31 patients did not have a sample collection, and 6 additional patients had a tissue/cytology rebiopsy, but no tumor cells were detected in the sample. The proportion of patients who were identified as positive for the T790M mutation was 30.7% among patients tested for T790M mutation (Table 4). A T790M-positive result occurred in 23.9% of patients at first rebiopsy (Table 4). T790M mutation was detected at first rebiopsy in 13/33 patients who were tested using tissue samples and had successful tumor cell collection (39.4%), 9/22 patients who provided cytology samples and had tumor cell collection (40.9%), and 27/137 patients who were tested using plasma samples (19.7%). Importantly, no EGFR mutations were detected in 77 patients (56.2%) during the first rebiopsy with plasma samples (Table S2). T790M detection rate by previous EGFR TKI treatment is shown in Table S3 and was 23.1% in patients previously treated with afatinib, 30.7% with gefitinib and 36.4% with erlotinib.
The most commonly used testing method, employed in 87.4% of patients, was the cobas® EGFR Mutation Test v2, followed by the peptide nucleic acid-locked nucleic acid polymerase chain reaction clamp [26] and cycleave polymerase chain reaction [27] methods (3.5 and 2.5%, respectively).
Subsequent Treatment
Of the 61 patients who underwent rebiopsy and were positive for the T790M mutation, 56 patients (91.8%) received osimertinib (monotherapy, n = 55; combination with chemotherapy, n = 1) as subsequent treatment (Table 5). Approximately one-half of the patients with negative test results or with no sample collected continued receiving first- or second-generation EGFR TKI therapy. Two patients in whom no samples were collected during the study received osimertinib, as these patients had tested positive for the T790M mutation before enrollment. Therefore, of the 236 patients included in the FAS, 58 patients received osimertinib treatment as T790M-targeted therapy.
Discussion
The present study is a prospective multicenter observational study that demonstrates real-world use of rebiopsy and T790M mutation testing among patients with advanced/metastatic NSCLC and disease progression after treatment with first- or second-generation EGFR TKIs. In the present study, the proportion of patients who could be identified as positive for the T790M mutation was approximately 31% in the patients tested for it. Liquid biopsy was used for T790M testing in 58.1% of patients. The T790M detection rate was 19.7% with plasma samples and approximately 40.0% with adequate tissue/cytology samples, consistent with previous data that mutation testing of plasma samples has lower sensitivity for T790M mutation detection compared with tissue samples [24].
In previous studies conducted among patients with NSCLC who experienced disease progression with EGFR TKI therapy, the prevalence of the T790M mutation ranged from 49 to 65% when tissue/cytology samples were used [10, 11, 19, 23, 28,29,30]. In contrast, the prevalence of the T790M mutation was 30.7% in the present study. Numerically more plasma samples than tissue/cytology samples were used to test for the T790M mutation, presumably to avoid invasive sampling methods. The T790M mutation detection rate was ~ 40% in tissue/cytology samples when only the successful tissue/cytology samples that contained sufficient amounts of tumor cells were considered compared with the ~ 20% detection rate in plasma samples. Therefore, the relatively low overall T790M mutation detection rate observed in the present study may be a result of the frequent reliance on plasma samples, which appear to be less sensitive for T790M detection.
Tumor detection in plasma samples, also known as liquid biopsy, is gaining popularity in EGFR mutation testing because of the small amounts of blood required and the relative ease and minimal invasiveness with which blood samples can be obtained [31]. However, the sensitivity of T790M testing using plasma samples is lower than that with tissue samples because ctDNA is often absent. In the present study, no EGFR mutation was detected in 56.2% of patients who underwent liquid biopsy. Such patients have been referred to as “ctDNA non-shedders,” and, for this patient population, plasma testing can be considered uninformative [25, 32]. When only patients with a detectable EGFR mutation in plasma ctDNA were considered, the proportion of T790M mutation-positive patients increased from 19.7 to 45.0%. Based on these findings, tissue/cytology samples appear to be preferable for T790M mutation testing compared with plasma samples.
Among patients who tested negative for the T790M mutation during initial rebiopsy, as well as those whose biopsy sample contained no tumor cells, repeat sampling and testing identified 12 additional patients with the T790M mutation. This finding highlights the need for repeat testing in patients with advanced/metastatic NSCLC who have previously tested negative for the T790M mutation and for patients with unknown mutation status. This is particularly true for patients who have an initially negative T790M result on a plasma sample. It is noteworthy that 9 of the 12 positive T790M results on second or third rebiopsy were identified in tissue or cytology samples, and none of the 5 positive T790M results on third biopsy were seen in plasma samples.
Our study also found that no specific EGRF TKI was associated with a greater probability of a T790M mutation compared with any other EGFR TKI in our pretreated patient cohort, consistent with previous findings by other researchers [33, 34]. Matsuo and colleagues found that the duration of previous EGFR TKI treatment was a significant predictor of T790M mutation presence, whereas the type of EGFR TKI was not [34].
Currently, the American Society of Clinical Oncology clinical practice guidelines strongly recommend osimertinib therapy for patients with disease progression after first- or second-generation EGFR TKI treatment and the presence of the T790M mutation based on the results of the AURA clinical trial program [35]. In the present study, approximately 90% of patients who could be identified as positive for the T790M mutation received osimertinib therapy. This finding indicates that osimertinib is widely used in a real-world setting as a standard of care for T790M mutation-positive patients in Japan.
In the present study, only about one-quarter of the patients eventually, after several steps (i.e., sample collection, T790M testing and T790M-positive results), became eligible for osimertinib treatment following disease progression on first- or second-generation EGFR TKIs. Although direct comparisons between studies are not possible, the proportion of patients who received osimertinib treatment in the present study is similar to that observed in the FLAURA trial (ClinicalTrials.gov identifier: NCT02296125), which compared osimertinib with first-generation EGFR TKIs among patients with previously untreated EGFR TKI-sensitizing mutation-positive NSCLC [20]. In the FLAURA study, patients assigned to the first-generation EGFR TKI group were allowed to cross over to the osimertinib group if they experienced disease progression and tested positive for the T790M mutation. Of the 192 patients who were initially assigned to the first-generation EGFR TKI group and experienced disease progression without death, 55 patients (28.6%) crossed over to receive osimertinib as T790M-targeted therapy [20]. These findings suggest that the proportion of patients who can receive osimertinib as T790M-targeted therapy is limited in the real world, although the proportion was previously presumed to be higher based on the earlier reported T790M-positive rate of approximately 50%.
The present study has several limitations. First, the sample collection procedure and type of sample used for T790M testing could have been affected by the type of participating study site. Both medical facilities highly specialized in the treatment of lung cancer, such as clinical oncology departments, and facilities with a more general focus, such as respiratory departments, participated in the study. Medical facilities specialized in lung cancer may be more adept at tissue/cytology sample collection compared with those with a general focus.
Second, approximately 70% of the patients were enrolled in the present study during the time period of the early access program, which made liquid biopsy testing for the T790M mutation available without financial cost to the patient; this scenario would be unusual in a real-world context. The finding that a greater proportion of samples was derived from plasma for patients enrolled in the present study during the early access program than after its conclusion suggests that, in a true real-world context, the proportion of plasma samples might be less than that observed in the present study. However, no firm conclusion can be reached because of the limited number of patients enrolled in the present study after the end of the early access program.
Third, the FAS included 11 patients who were retrospectively recruited after the results of the T790M testing became available in violation of the protocol, which could potentially have affected the results, particularly the T790M detection rate. The T790M detection rate may have been greater than otherwise would have been anticipated because of the retrospective enrollment. To address the potential for these data to bias the results, we conducted a sensitivity analysis that excluded these patients. This analysis showed that, after exclusion of the 11 retrospectively enrolled patients, the T790M detection rate was consistent with the results in the FAS (data not shown).
Conclusion
In our study, approximately 87% of patients with EGFR mutation-positive NSCLC underwent rebiopsy when their disease progressed during first- or second-generation EGFR TKI treatment. Of the 68 tissue or cytology samples, 55 contained tumor cells (80.8%) and could be tested for T790M mutation status, and 40% were positive for this mutation. In contrast, only 20% of plasma samples were positive for T790M mutation. Fifty patients underwent second rebiopsy and 8 had third rebiopsy, which led to T790M mutation detection in an additional 12 patients. Our data highlight the importance of conducting rebiopsies and T790M mutation testing among patients who progressed during treatment with first- or second-generation EGFR TKI to identify those who may benefit from treatment with osimertinib. This study also indicates that tissue or cytology sampling should be the preferred method of rebiopsy in this setting because plasma sampling is less sensitive and may produce false-negative results.
References
Pirker R. What is the best strategy for targeting EGF receptors in non-small-cell lung cancer? Future Oncol. 2015;11:153–67.
Keedy VL, Temin S, Somerfield MR, et al. American Society of Clinical Oncology provisional clinical opinion: epidermal growth factor receptor (EGFR) mutation testing for patients with advanced non–small-cell lung cancer considering first-line EGFR tyrosine kinase inhibitor therapy. J Clin Oncol. 2011;29:2121–7.
Shi Y, Au JS-K, Thongprasert S, et al. A prospective, molecular epidemiology study of EGFR mutations in Asian patients with advanced non–small-cell lung cancer of adenocarcinoma histology (PIONEER). J Thorac Oncol. 2014;9:154–62.
Maemondo M, Inoue A, Kobayashi K, et al. Gefitinib or chemotherapy for non–small-cell lung cancer with mutated EGFR. N Engl J Med. 2010;362:2380–8.
Mitsudomi T, Morita S, Yatabe Y, et al. Gefitinib versus cisplatin plus docetaxel in patients with non-small-cell lung cancer harbouring mutations of the epidermal growth factor receptor (WJTOG3405): an open label, randomised phase 3 trial. Lancet Oncol. 2010;11:121–8.
Zhou C, Wu Y-L, Chen G, et al. Erlotinib versus chemotherapy as first-line treatment for patients with advanced EGFR mutation-positive non-small-cell lung cancer (OPTIMAL, CTONG-0802): a multicentre, open-label, randomised, phase 3 study. Lancet Oncol. 2011;12:735–42.
Rosell R, Carcereny E, Gervais R, et al. Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): a multicentre, open-label, randomised phase 3 trial. Lancet Oncol. 2012;13:239–46.
Sequist LV, Yang JC, Yamamoto N, et al. Phase III study of afatinib or cisplatin plus pemetrexed in patients with metastatic lung adenocarcinoma with EGFR mutations. J Clin Oncol. 2013;31:3327–34.
Wu YL, Zhou C, Hu CP, et al. Afatinib versus cisplatin plus gemcitabine for first-line treatment of Asian patients with advanced non-small-cell lung cancer harbouring EGFR mutations (LUX-Lung 6): an open-label, randomised phase 3 trial. Lancet Oncol. 2014;15:213–22.
Oxnard GR, Arcila ME, Chmielecki J, Ladanyi M, Miller VA, Pao W. New strategies in overcoming acquired resistance to epidermal growth factor receptor tyrosine kinase inhibitors in lung cancer. Clin Cancer Res. 2011;17:5530–7.
Yu H, Arcila ME, Rekhtman N, et al. Analysis of mechanisms of acquired resistance to EGFR TKI therapy in 155 patients with EGFR-mutant lung cancers. Clin Cancer Res. 2013;19:2240–7.
Camidge DR, Pao W, Sequist LV. Acquired resistance to TKIs in solid tumours: learning from lung cancer. Nat Rev Clin Oncol. 2014;11:473.
Nan X, Xie C, Yu X, Liu J. EGFR TKI as first-line treatment for patients with advanced EGFR mutation-positive non-small-cell lung cancer. Oncotarget. 2017;8:75712.
Walter AO, Sjin RTT, Haringsma HJ, et al. Discovery of a mutant-selective covalent inhibitor of EGFR that overcomes T790M-mediated resistance in NSCLC. Cancer Discov. 2013;3:1404–15.
Tan CS, Kumarakulasinghe NB, Huang YQ, et al. Third generation EGFR TKIs: current data and future directions. Mol Cancer. 2018;17:29.
Cross DA, Ashton SE, Ghiorghiu S, et al. AZD9291, an irreversible EGFR TKI, overcomes T790M-mediated resistance to EGFR inhibitors in lung cancer. Cancer Discov. 2014;4:1046–61.
Goss G, Tsai C-M, Shepherd FA, et al. Osimertinib for pretreated EGFR Thr790Met-positive advanced non-small-cell lung cancer (AURA2): a multicentre, open-label, single-arm, phase 2 study. Lancet Oncol. 2016;17:1643–52.
Yang JCH, Ahn MJ, Kim DW, et al. Osimertinib in pretreated T790M-positive advanced non–small-cell lung cancer: AURA study phase II extension component. J Clin Oncol. 2017;35:1288–96.
Mok TS, Wu Y-L, Ahn M-J, et al. Osimertinib or platinum–pemetrexed in EGFR T790M–positive lung cancer. N Engl J Med. 2017;376:629–40.
Soria J-C, Ohe Y, Vansteenkiste J, et al. Osimertinib in untreated EGFR-mutated advanced non-small-cell lung cancer. N Engl J Med. 2018;378:113–25.
Yver A. Osimertinib (AZD9291)-a science-driven, collaborative approach to rapid drug design and development. Ann Oncol. 2016;27:1165–70.
Kawamura T, Kenmotsu H, Taira T, et al. Rebiopsy for patients with non-small-cell lung cancer after epidermal growth factor receptor-tyrosine kinase inhibitor failure. Cancer Sci. 2016;107:1001–5.
Nosaki K, Satouchi M, Kurata T, et al. Re-biopsy status among non-small cell lung cancer patients in Japan: a retrospective study. Lung Cancer. 2016;101:1–8.
Li X, Zhou C. Comparison of cross-platform technologies for EGFR T790M testing in patients with non-small cell lung cancer. Oncotarget. 2017;8:100801–18.
Lin CC, Shih JY, Yu CJ, et al. Outcomes in patients with non-small-cell lung cancer and acquired Thr790Met mutation treated with osimertinib: a genomic study. Lancet Respir Med. 2018;6:107–16.
Nagai Y, Miyazawa H, Tanaka T, et al. Genetic heterogeneity of the epidermal growth factor receptor in non-small cell lung cancer cell lines revealed by a rapid and sensitive detection system, the peptide nucleic acid-locked nucleic acid PCR clamp. Cancer Res. 2005;65:7276–82.
Yatabe Y, Hida T, Horio Y, Kosaka T, Takahashi T, Mitsudomi T. A rapid, sensitive assay to detect EGFR mutation in small biopsy specimens from lung cancer. J Mol Diagn. 2006;8:335–41.
Arcila ME, Oxnard GR, Nafa K, et al. Rebiopsy of lung cancer patients with acquired resistance to EGFR inhibitors and enhanced detection of the T790M mutation using a locked nucleic acid-based assay. Clin Cancer Res. 2011;17:1169–80.
Sequist LV, Waltman BA, Dias-Santagata D, et al. Genotypic and histological evolution of lung cancers acquiring resistance to EGFR inhibitors. Sci Transl Med. 2011;3:75ra26.
Kuiper J, Heideman D, Thunnissen E, et al. Incidence of T790M mutation in (sequential) rebiopsies in EGFR-mutated NSCLC-patients. Lung Cancer. 2014;85:19–24.
Kwapisz D. The first liquid biopsy test approved. Is it a new era of mutation testing for non-small cell lung cancer? Ann Transl Med. 2017;5:46.
Oxnard GR, Thress KS, Alden RS, et al. Association between plasma genotyping and outcomes of treatment with osimertinib (AZD9291) in advanced non-small-cell lung cancer. J Clin Oncol. 2016;34:3375–82.
Jenkins S, Chih-Hsin Yang J, Janne PA, et al. EGFR mutation analysis for prospective patient selection in two phase II registration studies of osimertinib. J Thorac Oncol. 2017;12:1247–56.
Matsuo N, Azuma K, Sakai K, et al. Association of EGFR exon 19 deletion and EGFR-TKI treatment duration with frequency of T790M mutation in EGFR-mutant lung cancer patients. Sci Rep. 2016;6:36458.
Hanna N, Johnson D, Temin S, et al. Systemic therapy for stage IV non-small-cell lung cancer: American Society of Clinical Oncology clinical practice guideline update. J Clin Oncol. 2017;35:3484–515.
Acknowledgements
We thank the patients and their families as well as the investigators and staff at all trial sites.
Funding
The study was funded by AstraZeneca Japan. All authors had full access to all of the data in this study and take complete responsibility for the integrity of the data and accuracy of the data analysis.
Medical Writing, Editorial and Other Assistance
Editorial assistance in the preparation of this article was provided by Nishad Parkar, PhD, and Elizabeth Strickland, PhD, CMPP, of inScience Communications, Springer Healthcare. Support for this assistance, as well as journal processing fees, were funded by AstraZeneca.
Authorship
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole and have given their approval for this version to be published.
Disclosures
Takashi Seto has received grants from Astellas Pharma, AstraZeneca, Bayer Yakuhin, Chugai Pharmaceutical, Daiichi Sankyo, Eli Lilly Japan, Eisai, Kissei Pharmaceutical, Merck Serono, Merck Sharp & Dohme, Nippon Boehringer Ingelheim, Novartis, Pfizer Japan, Verastem and Yakult Honsha and honoraria from Astellas Pharma, AstraZeneca, Bristol-Myers Squibb, Chugai Pharmaceutical, Daiichi Sankyo, Eli Lilly Japan, Kissei Pharmaceutical, Kyowa Hakko Kirin, Merck Sharp & Dohme, Mochida Pharmaceutical, Nippon Boehringer Ingelheim, Nippon Kayaku, Ono Pharmaceutical, Pfizer Japan, Roche Singapore, Sanofi, Showa Yakuhin Kako, Taiho Pharmaceutical, Takeda Pharmaceutical and Yakult Honsha. Naoyuki Nogami has received grants from AstraZeneca and Meiji Seika Pharma and personal fees from Boehringer Ingelheim, Chugai Pharmaceutical, Eli Lilly Japan, Kyowa Hakko Kirin, Merck Sharp & Dohme KK, Ono Pharmaceutical, Pfizer and Taiho Pharmaceutical. Nobuyuki Yamamoto has received grants from Boehringer Ingelheim, Chugai Pharmaceutical, Eli Lilly and Merck Sharp & Dohme and personal fees from AstraZeneca, Boehringer Ingelheim, Bristol-Myers Squibb, Chugai Pharmaceutical, Daiichi Sankyo, Eli Lilly, Merck Sharp & Dohme, Novartis, Ono Pharmaceutical and Pfizer. Shinji Atagi has received grants from Boehringer Ingelheim, Chugai Pharmaceutical, Eli Lilly, Merck Serono, Ono Pharmaceutical, Pfizer and Taiho Pharmaceutical and personal fees from AstraZeneca, Boehringer Ingelheim, Bristol-Myers Squibb, Chugai Pharmaceutical, Ono Pharmaceutical and Taiho Pharmaceutical. Naoki Tashiro is an employee of AstraZeneca KK. Yoko Yoshimura is an employee of AstraZeneca KK. Yutaka Yabuki is an employee of AstraZeneca KK. Hideo Saka has received grants from AstraZeneca, Bayer, Boehringer Ingelheim Japan, Bristol-Myers Squibb, Chugai Pharmaceutical, Daiichi Sankyo, Eli Lilly Japan, Eisai, Kyowa Hakko Kirin, Merck Serono, Merck Sharp & Dohme, Novartis, Olympus, Ono Pharmaceutical, Quintiles Transnational Japan, Sanofi, Taiho Pharmaceutical and West Japan Oncology Group and personal fees for lectures from Astellas Pharma, AstraZeneca, Becton, Dickinson and Company, Boehringer Ingelheim Japan, Boston Scientific, Chugai Pharmaceutical, Chunichi Shimbun, Covidien Japan, Eli Lilly Japan, Japan Society for Respiratory Endoscopy, Kyorin Pharmaceutical, Nagoya Pharmaceutical, Nobelpharma, Olympus Medical Systems, Ono Pharmaceutical and Taiho Pharmaceutical.
Compliance with Ethics Guidelines
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
Open Access
This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
Author information
Authors and Affiliations
Corresponding author
Additional information
Enhanced Digital Content
To view enhanced digital content for this article, go to https://doi.org/10.6084/m9.figshare.6931199.
Electronic Supplementary Material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Seto, T., Nogami, N., Yamamoto, N. et al. Real-World EGFR T790M Testing in Advanced Non-Small-Cell Lung Cancer: A Prospective Observational Study in Japan. Oncol Ther 6, 203–215 (2018). https://doi.org/10.1007/s40487-018-0064-8
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40487-018-0064-8