
Abstract
Purpose of Review
Prosocial behavior and depression are related constructs that both increase during adolescence and display gender-specific effects. The current review surveys literature examining the association between depressive symptoms and prosociality, measured with behavioral economic paradigms, across development and proposes a theoretical model explaining a mechanism through which adolescent girls have higher risk for depression than boys.
Recent Findings
Relative to healthy controls, prosocial behavior is reduced in adults with major depressive disorder (MDD) but may be increased in adolescents with MDD. The relationship between non-clinical levels of depressive symptoms and prosocial behavior remains to be studied experimentally; however, self-reported prosocial behavior is negatively associated with depressive symptoms in non-clinical adolescents, which may suggest a shift in the relation of prosocial behavior and depressive symptoms across the non-clinical (i.e., negative) to clinical range (i.e., positive).
Summary
The effect of gender on these developmental and clinical status shifts has not been studied but could have important implications for understanding the emergence of higher rates of depression in girls than boys during adolescence. We propose that girls are at heightened risk for depression due to higher social-evaluative concern and other-oriented prosocial motivation that emphasize the needs of others over the self, leading to more altruistic prosocial behavior (despite personal cost) and a higher burden that enables depressive symptoms.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Disruptions to social processing and decision-making are features of major depressive disorder (MDD) that may precede diagnosis [1]. Indeed, prosocial behavior, defined most simply as a voluntary action intended to benefit others, has been shown to correlate negatively with depressive mood in non-clinical samples [2,3,4,5,6]. This finding supports the theory that people engage in prosocial behavior because they take pleasure in helping others [7], which, in turn, increases their happiness [8]. However, previous literature has largely ignored the motivations behind prosocial behavior when reporting associations with depressive symptoms. Prosocial motivation includes other-oriented (i.e., selfless; altruistic) and self-oriented (i.e., selfish; egoistic) motives, which can lead to similar behavioral outcomes under certain circumstances. However, individuals who are motivated by the needs of others are more likely to behave prosocially even when there is the potential for personal cost [9], which can create substantial burden [10•] and lead to higher depressive symptoms [11]. Therefore, the association between prosocial behavior and depressive symptoms maybe more nuanced than previously assumed.
Important developmental and gender differences in prosocial behavior may affect its relationship to depressive symptomatology. Compared to adulthood, adolescence is characterized by heightened peer affiliation and salience of social information, rooted in the development of endocrine, neural, and social systems [12]. In fact, prosocial behavior increases across adolescence and then decreases and plateaus in early adulthood [13]. Moreover, the adolescent period is marked by a substantial increase in the onset of depressive disorders, which predominantly impacts girls versus boys [14]. The onset of puberty triggers not only a rise in sex hormone levels, such as testosterone, which not only differentiate girls and boys but also triggers a re-organization of neural oxytocin binding sites, representing a refinement of the social brain [15]. These endocrine changes contribute to the maturation of neural networks involved in key aspects of prosocial behavior, including reward, cognitive control, and social cognition neural networks [16, 17]. The convergence of puberty, brain development, and social development places adolescents in a context where prosociality becomes more important for affiliation but may include a cost for individuals who sacrifice their own needs for those of others, increasing the risk for depressive symptoms.
Due to the increased relevance of peers and relationships to define self-identity and self-worth, adolescents, particularly female adolescents, display more social-evaluative concern or concern with negative social evaluation [18]. In females, heightened psychological investment in relationships manifests in more worry about judgment of peers, closer interpersonal connections, and more self-reported prosocial behavior [19]. Importantly, adolescent girls are more likely to report other-oriented concerns (e.g., fear of disapproval from peers), while boys are more likely to report self-oriented prosocial motivations (e.g., helping others to achieve a sense of self-satisfaction) [20]. These gender differences in motivation for prosocial behavior may help to explain the higher prevalence of depression in girls than boys, beginning in adolescence. Indeed, social-evaluative concern, specifically concern about disapproval from peers, is not only linked with altruistic prosocial behavior [21•] but also predicts depressive symptoms [18]. Thus, other-oriented motivations for prosocial behaviors in adolescent girls may underlie the link between these behaviors and depressive symptoms.
Importantly, the associations between prosocial behavior and depressive symptoms may be more complex in individuals diagnosed with MDD, as social functioning tends to decline during episodes [22]. Patients with MDD often display anhedonia—the inability or reduced ability to feel pleasure—and may not readily experience the pleasure accompanying prosociality, which will result in less helping behavior. Alternatively, individuals with MDD may seek opportunities to behave prosocially if they want to relieve negative symptoms of depression. In addition, individuals with MDD, particularly females, often display excessive interpersonal dependence—a reliance on other people for emotional and social support—in response to loneliness and fear of rejection [23]. Therefore, individuals with MDD may display either more or less prosocial behavior than healthy controls, which may depend on the gender of the individual.
We present a theoretical model based on the emergence of gender differences in motivations for prosocial behavior that may explain adolescent gender differences in the risk for depressive symptoms (Fig. 1). Specifically, we propose that higher social-evaluative concern in girls translates into more other-oriented prosocial motivations, leading to more altruistic prosocial behavior. Engaging in altruistic prosocial behavior that prioritizes the needs of others over the self can, in turn, lead to burden that perpetuates the expression of depressive symptoms. In a current state of depression, adolescent girls may fear rejection further and demonstrate more social-evaluative concern, which perpetuates the cycle. Importantly, this proposed mechanism is not exclusive to females, but it may be less common in males since they tend to report less social-evaluative concern, other-oriented prosocial motivation, altruistic prosocial behavior, and fewer depressive symptoms.

Theoretical model of adolescent gender differences in depressive symptom expression. Girls experience heightened social-evaluative concern, which supports increased other-oriented prosocial motivations and altruistic prosocial behavior, which is further supported by engagement of the social cognitive network and reduced engagement of the reward and cognitive control networks. The burden created by prioritizing the needs of others at the expense of the self may then perpetuate depressive symptoms, which are further supported by higher oxytocin and lower testosterone levels. SCN social cognition network, CCN cognitive control network, RN reward network
The current manuscript will review studies that measure prosocial behavior, using behavioral economic paradigms, in relation to depression, defined as both depressive symptoms and MDD diagnosis. The behavioral economic approach combines mathematical theory and rigorous experimental paradigms from game theory (and may also include neural activity measured with neuroimaging methods—e.g., neuroeconomics) to predict effects of cognitive and emotional factors (e.g., social-evaluative concern) on (prosocial) individual choices [24] including those that are costly to the individual. Research conducted in adults and adolescence (defined as 12–19 years old) will be presented to delineate developmental differences in prosocial behavior in MDD and non-clinical populations. The neural correlates of prosocial behavior and the relationships between prosocial behavior and gender, testosterone, and oxytocin will be discussed as well. Finally, a discussion of the reviewed literature in the context of the proposed theoretical model will be included and future directions will be provided.
Operationalizing Prosocial Behavior
Behavioral economic paradigms offer an ecologically valid means to study complex social behaviors—such as altruistic punishment, cooperation and reciprocity—by modeling interactions between two or more individuals in a variety of contexts (reviewed by [25•]). The behavioral economic paradigms most frequently studied in the context of depression include the Ultimatum Game, the Trust Game, and the Prisoner’s Dilemma (reviewed by [26•]). Other types of prosocial games include the Dictator and Public Goods Games (Table 1). Manipulation of task conditions to promote or discourage prosocial outcomes is common; however, only the most basic task parameters will be discussed below.
The Ultimatum Game is used to measure altruism. Briefly, player 1 (proposer) proposes how to divide a fixed amount of money and player 2 (responder) decides to accept or reject this proposal without negotiation. If the proposal is accepted, the proposed split is realized, but if it is rejected neither player receives money. Proposing a more generous split of the money, although potentially confounded by strategic concerns and risk aversion (e.g., determining the lowest possible offer while avoiding rejection), is indicative of higher prosociality. Responders typically reject unfair proposals even though they stand to benefit from accepting any offer. More fair-minded (i.e., justice-oriented) individuals tend to reject unfair offers and accept zero payment for both themselves and the proposer as a form of punishment (i.e., altruistic punishment) meant to encourage the proposer to make more fair offers in subsequent trials played against the responder and/or other future responders. Altruistic punishment may be interpreted as prosocial behavior or a failure of self-control (to inflict punishment).
The Trust Game is used to study reciprocal exchanges: first, a trustor decides if and how much money to invest in a trustee and if invested the money is multiplied by some factor; second, the trustee has the option to return any proportion of the multiplied amount to the trustor. Both parties stand to gain more money by reciprocating trust, and typically both the trustor and trustee choose to invest and return money, respectively. The trustor’s behavior is more reflective of trust and risk aversion, and the trustee’s behavior indicates degree of altruism, reciprocity, and trustworthiness; more trust and reciprocity reflect more prosocial behavior. The trustee’s choice to return a portion of an investment (or not) mirrors the choice of the proposer in the Dictator Game. In the Dictator Game, the proposer makes an offer to be split between himself/herself and a receiver, who has no choice but to accept the offer. Even though the proposer faces no monetary repercussions for unfair behavior, they tend to make fair offers, which serves as a measure of altruism.
Finally, the Prisoner’s Dilemma and Public Goods Games are used to measure cooperative behavior. In the Prisoner’s Dilemma, two players are confronted with the same option to cooperate or defect and there are four possible outcomes for a given trial. Payout for a trial is determined by the interaction between both players, such that the largest payout for a player occurs when he or she defects and the partner cooperates and the worst outcome occurs when the player cooperates while the partner defects. The largest payout is brought upon by mutual cooperation, while mutual defection yields a smaller payout to each player. More cooperation represents higher prosociality. In the Public Goods Game, multiple players decide how many tokens to privately put into a public pot. The amount in the pot is multiplied by a factor (greater than 1 and less than the number of players) and evenly divided among players. In addition, players keep the tokens they do not contribute. Total payoff is maximized when everyone in the group contributes all of their tokens. Those who contribute below average are termed defectors or free riders, in contrast to cooperators who make above-average contributions to the public pot.
Adult Prosocial Behavior and Depression
Recent studies examining linear associations between prosocial behavior and depressive symptoms in non-clinical adults report mixed results (Table 2). Positive associations between depressive symptoms and prosocial behavior, as indicated by more cooperation in the Prisoner’s Dilemma [27, 28] and Public Goods Game [28], have been reported. However, Brendan Clark and colleagues [28] also show that depressive symptoms are not correlated with behavior on the Trust or Ultimatum Games. Furthermore, another study reports that higher depression scores are negatively correlated with cooperation on the Prisoner’s Dilemma [29]. Only one study reported a full range of participant depressive symptoms [27]; therefore, the association between prosocial behavior and depressive symptoms may be underestimated. Overall, there is no clear association between depressive symptoms and prosocial behavior in healthy adults, which stands in contrast to previous research that has used self-report measures of prosocial behavior showing a negative association [6].
Studies comparing prosocial behavior of adults with MDD and healthy or non-clinical adults also demonstrate mixed results, although on balance studies tend to report that MDD is associated with less prosocial behavior (Table 2). Using the Prisoner’s Dilemma, Pulcu and colleagues [30] report less cooperation by adults diagnosed with MDD compared to healthy controls. Similarly, Zhang and colleagues [31] show that adults with MDD engage in less reciprocity during a Trust Game than non-clinical adults. Finally, using the Ultimatum Game, Radke and colleagues [32] show that adults with MDD reject more (fair and unfair) offers in the role of responder, compared to healthy controls. However, five studies show no difference in prosocial behavior by adults with MDD compared to healthy or non-clinical controls using a variant of the Dictator Game [30], the Prisoner’s Dilemma [33•], an Ultimatum Game in the role of proposer [30] and responder [30, 34] and a Trust Game in the roles of trustor and trustee [35•, 36]. Shao and colleagues [35•] also measured the correlation between reciprocity and depressive symptoms in adults with MDD; however, the association was not statistically significant. Finally, three other studies report more prosocial behavior (measured with the Ultimatum Game) in adult patients with MDD compared to healthy and non-clinical controls in both the roles of proposer [37] and responder [37,38,39]. However, latter studies measured altruistic punishment (i.e., rejection of unfair offers), which may also represent failures of self-control. Therefore, the data are in favor of a negative or null effect of MDD diagnosis on prosocial behavior.
In sum, non-clinical adults do not show a significant association between prosocial behavior and depressive symptoms, but the onset of MDD seems to alter prosocial behavior, such that adults with MDD demonstrate less prosociality than healthy controls. A state of depression may heighten sensitivity to social signals and rejection, which encourages individuals to retreat to avoid rejection [40]. In contrast, it is possible that anhedonia plays a role in decreasing the salience of prosocial behavior. Although causality cannot be determined without longitudinal investigation of these factors, prosocial neural activation studies provide some support for the latter interpretation.
Neural Correlates of Prosocial Behavior in Adult MDD
Several studies report aberrant activation of reward and cognitive control networks in adults with MDD during behavioral economic paradigms designed to engage prosocial behavior. The reward network includes the ventral striatum, which mediates (social) reward processing, reinforcement, and motivational salience [41], while the cognitive control network includes the dorsolateral prefrontal cortex (DLPFC) and mediates executive functions, including inhibitory control (of selfish behavior) [42]. Gradin and colleagues [33•] report weaker activation of the reward network during prosocial behavior (i.e., cooperation during the Prisoner’s Dilemma) and weaker activation of the cognitive control network during proself behavior (i.e., defection by self or partner), in patients with MDD, compared to healthy controls. The same group replicate part of these findings using the Ultimatum Game in the role of responder: patients with MDD show weaker activation of the reward network during prosocial behavior, compared to healthy controls. Furthermore, activation of the ventral striatum was negatively correlated with anhedonia [34•], lending support to the interpretation that MDD diagnosis, via anhedonia, decreases the salience and rewarding properties of prosocial behavior, which may, in turn, discourage future prosocial behavior. Finally, using a modified Trust Game in the role of trustee, Shao and colleagues [35•] found reduced activity of the cognitive control network during proself behavior in patients with MDD compared to non-clinical controls. In sum, adults with MDD show reduced activation of the reward network during prosocial behavior, which may indicate blunted rewarding properties of prosocial behavior, and weaker activation of cognitive control network during proself behavior, suggesting a failure to inhibit selfish behavior.
Adolescent Prosocial Behavior and Depression
Studies to date have not assessed the link between depressive symptoms and prosocial behavior in adolescents with non-clinical levels of depression using behavioral economic paradigms (Table 2). However, adolescent prosociality has been studied extensively with self-report measures; studies that examine the relation between self-reported prosocial behavior and depressive symptoms generally report a negative correlation. Indeed, longitudinal studies show that depressive symptoms negatively predict prosocial behavior in adolescents [2,3,4,5]. Importantly, there is also some evidence that more prosocial behavior leads to fewer depressive symptoms in healthy youth [3]. Thus, it is plausible that behavioral economic paradigms would find a similar negative association in healthy adolescents. Indeed, the only functional magnetic resonance imaging (fMRI) study to have measured the association between prosociality and depression during adolescence found that more robust activation of the ventral striatum during prosocial behavior directed at family (using a variant of the Dictator Game) predicted fewer depressive symptoms 1 year later (gender differences were not reported) [43•]. Notably, the association between depressive symptoms and prosocial behavior was not reported [43•]. These findings stand in contrast with our proposed model; however, the discordant findings between non-clinical adult studies using experimental and self-report measures [6, 27,28,29] may indicate that individuals’ actual prosocial behavior does not align with self-reported behavior. Thus, it is possible that non-clinical adolescents display a positive association between prosocial behavior measured experimentally and depressive symptoms. However, more research using behavioral economic paradigms during the adolescent period is needed to confirm any association between depressive symptoms and prosocial behavior.
A limited number of studies have examined differences in prosocial behavior between youth with MDD and healthy controls using behavioral economic paradigms (Table 2). McClure and colleagues [44] show that MDD and anxiety patients respond more cooperatively than healthy controls following partner cooperation (but not defection) on the Prisoner’s Dilemma. A study by Harlé and colleagues corroborates this finding by showing that individuals with MDD accept more unfair offers on the Ultimatum Game despite reporting a more negative reaction to unfair offers, compared to healthy controls. Accepting unfair offers is typically considered a rational choice; however, the choice to accept an unfair offer benefits the proposer and can still be considered a prosocial choice. Indeed, in patients with MDD, this pattern of responding can reflect a fear of being socially rejected by a proposer after refusing the proposer’s unfair offer [22]. Thus, in contrast to the adult literature, these studies tentatively suggest that youth with MDD behave more prosocially than their healthy counterparts; however, this effect may be partially attributed to anxiety. To our knowledge, there are no studies measuring differences in prosocial behavior via self-report between adolescents diagnosed with MDD and healthy or non-clinical controls. Overall, these findings support our theoretical model, such that potential fear of rejection and heightened social-evaluative concern during a depressive episode fuel other-oriented prosocial motivations and subsequent prosocial behavior, perpetuating the cycle of depressive symptoms (Fig. 1).
Summary
Adults with MDD display less prosocial behavior than healthy controls, potentially via anhedonia and blunted reward system activation, as well as weaker recruitment of the cognitive control network, leading to poor inhibition of proself behavior. Similarly, an accumulating literature has begun to indicate a negative association between self-reported depressive symptoms and prosocial behavior, such that more depressive symptoms predict less prosocial behavior and more prosocial behavior predicts less depressive symptoms in adolescence (although neither effect has been confirmed experimentally). The latter mechanism is supported by an fMRI study reporting that stronger ventral striatal brain response during prosocial behavior, albeit not prosocial behavior per se, predicts fewer depressive symptoms in non-clinical adolescents [43•]. By contrast, recent work suggests that clinically significant depressive illness in adolescents may associate with more prosocial behaviors than in healthy controls [44, 45]. The shift from negative to positive associations between prosocial behavior and depressive symptoms following MDD onset may reflect a disease state-dependent shift in mechanism or strategy supporting prosocial behavior. However, as proposed by our theoretical model (Fig. 1), the influence of gender, oxytocin, and testosterone on prosocial behavior and depressive symptoms must be considered in order to determine the direction of the effect (positive or negative) of prosocial behavior on depressive symptoms (or vice versa).
Gender
Gender differences in prosocial behavior using behavioral economic paradigms only emerge under certain conditions [46•]. Framing the experimental context with social and emotional conditions tends to increase prosocial behavior in women. For instance, reducing social distance (i.e., playing with a friend versus stranger) increases prosocial behavior in women, but not men [47]. In contrast, framing prosocial behavior to be consistent with self-interests by introducing a delay in decision making that promotes reflection [48, 49] or by explicitly stating how prosocial behavior benefits the individual [50] can make men, but not women, behave less prosocially [46•]. Importantly, gender differences are absent in adulthood if social interactions are conducted with a stranger or a computer program [51•, 52], suggesting that prosocial behavior is generally the same for men and women under baseline conditions, but begins to differ when context and motivation for social behavior is manipulated.
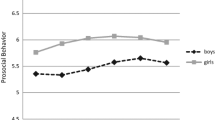
Although many studies using self-report measures, observation, and teacher/peer ratings indicate that adolescent girls are more prosocial than boys [53], studies using behavioral economic paradigms report mixed findings. Critically, the majority of adolescent studies have not examined gender differences directly [54, 55•, 56,57,58,59,60,61]. A study using the Prisoner’s Dilemma reports that adolescent girls are more cooperative than boys [62•]. Using the Trust Game, another study shows that adolescent boys display more trust behavior (trustor) than girls, but no gender differences in reciprocity (trustee) are found [63•]. Notably, in this study, more girls identify as “prosocials” than “proselfs,” and prosocial individuals are more likely to be trusting and trustworthy [63•], indicating that adolescent boys may be trusting because they are actually less risk averse. Other studies in healthy adolescents have reported no gender difference in prosocial behavior using a Public Goods Game [64•] and a Trust Game in the role of trustee [65]. Similar to adulthood, this discrepancy in findings might be explained by differential sensitivity to experimental cues by girls compared to boys; however, this remains to be empirically tested in adolescents.
Oxytocin and Testosterone
Oxytocin and testosterone are implicated in prosocial behavior and depression [66•]. Oxytocin is a neuropeptide produced in the hypothalamus and released by the posterior pituitary to facilitate social behavior. In addition, oxytocin is positively associated with depression [66•]. Neural oxytocin binding sites are re-distributed from the postnatal period through adulthood, with one shift in distribution occurring after the onset of puberty, representing a refinement of the social brain [15], which may indicate that oxytocin plays a larger role in prosocial behavior and depression following puberty. In contrast, testosterone is a steroid that is primarily produced in the testes and adrenal glands. Testosterone has many behavioral effects, including increasing aggression and (broadly) decreasing prosocial behavior. During puberty, testosterone increases dramatically, especially in boys, which could help explain gender differences in prosocial behavior.
The great majority of studies report that oxytocin is positively associated with prosocial behavior, but this effect varies based on individual factors and task conditions. For instance, oxytocin tends to increase prosocial behavior directed at individuals belonging to an in-group [67,68,69,70,71,72]; in some cases, oxytocin is negatively related to prosocial behavior directed to individuals of an out-group [73] or in response to betrayal [74]. Importantly, some studies report no associations between prosocial behavior and oxytocin [75,76,77], indicating that this relationship is complex and requires further study. Indeed, some of this complexity may be accounted for by gender differences. Studies reporting that oxytocin increases or is positively associated with prosocial behavior also show that this effect is particularly robust for female children [78] and adults [79,80,81], compared to males. However, not all studies report gender differences in the effect of oxytocin on prosocial behavior [75, 76]. In general, however, oxytocin signals the presence of a socially relevant stimulus that requires attention and ultimately promotes social affiliation [66•]. The association between oxytocin and prosocial behavior has not been measured during adolescence, although one study shows that adolescent males with higher salivary oxytocin levels report fewer conduct problems [82], which can be cautiously interpreted as more prosocial behavior. Finally, one study reported elevated oxytocin levels in adolescents with treatment-resistant MDD, compared to non-treatment resistant and healthy control adolescents [83•]. However, the association between prosocial behavior and oxytocin in pubertal patients with MDD remains to be studied.
In contrast to oxytocin, testosterone is generally associated with less prosocial behavior and fewer depressive symptoms [66•]. Recent studies using behavioral economic paradigms indicate that higher testosterone is typically associated with less prosocial behavior in males [84,85,86,87,88]—although not always [89, 90]. However, if the prosocial behavior is directed at someone belonging to the participant’s in-group (e.g., a friend), higher testosterone is associated with more cooperative behavior in males [84, 91, 92]. In women, the link between testosterone and prosocial behavior is mixed, with studies reporting a negative association [93], in one case following mild stress [87] and a positive association [93, 94], in one case only when reciprocating generosity [93]. Although the association between testosterone in prosocial behavior per se has not been studied across adolescence, there is a positive relationship between testosterone and antisocial behavior that intensifies across adolescence in males, but not females, which may be informed by social experiences and higher fetal exposure to testosterone [95]. A negative association between testosterone and depression has been reported [96]; however, to our knowledge, the association between testosterone and prosocial behavior in relation to depression has not been studied previously.
In sum, oxytocin is generally positively associated with prosocial behavior and depressive symptoms; however, gender differences in the effect of oxytocin on prosocial behavior in MDD have yet to be determined. Testosterone appears to increase proself behavior when there is a potential social challenge or threat (i.e., members of an out-group), but it may increase prosocial behavior in the absence of threat or when status or reputation maybe well served by prosocial actions. Therefore, the combination of high oxytocin and low testosterone may lead to more depressive symptoms and prosocial behavior, particularly if that behavior is directed at a member of an in-group, such as a friend. The combination of (1) gender-specific effects of oxytocin on prosociality favoring more prosocial behavior in females compared to males and (2) the inverse association between prosociality and testosterone favoring less prosocial behavior in males, who have higher levels of testosterone than females, may facilitate more altruistic prosocial behavior in adolescent girls compared to boys, which increases personal burden and risk for depressive symptoms.
Conclusions
The literature presented here support a developmental dissociation between prosociality and depression, such that adults with MDD demonstrate less prosocial behavior and adolescents with MDD demonstrate more prosocial behavior, compared to healthy and non-clinical controls. Furthermore, these associations may be different in non-clinical populations. In non-clinical adults, there is no relation between depressive symptoms and prosocial behavior, which stands in contrast with studies measuring prosocial behavior via self-report that indicate a negative association. In non-clinical adolescents, a negative association between depressive symptoms and prosocial behavior has been reported by studies using self-report measures of prosocial behavior, but this association has not been studied using behavioral economic paradigms.
The lack of studies using behavioral economic paradigms to study prosocial behavior in non-clinical adolescent samples makes it difficult to conclusively determine whether clinical status of an individual affects the associations between prosocial behavior and depressive symptoms. However, if we assume that behavioral economic paradigms will replicate the effects obtained with self-report measures of prosocial behavior then it may the case that prior to MDD diagnosis, adolescents benefit from the protective effects of prosocial behavior; however, after diagnosis, they may seek relief from their negative emotional state or avoid social rejection by engaging in more prosocial behavior. An alternative interpretation is that social-evaluative concern and other-oriented motivations inform altruistic prosocial behavior and play a larger role in shaping risk for depression in non-clinical adolescents that continues after MDD diagnosis. It may that for a subset of individuals, such as adolescent girls, a positive association between depression and prosocial behavior (measured experimentally) exists due to the cost associated with heightened social-evaluative concern. Once in a state of MDD, social-evaluative concern is reinforced and perpetuates more altruistic prosocial behavior (Fig. 1). Future research considering prosocial motivations driving behavior will be needed to distinguish between these possibilities.
Consideration of factors that interact with depression and have biological underpinnings, such as gender, brain activation, oxytocin, and testosterone, will be crucial to achieve full comprehension of the relationship between prosocial behavior and depression. A focus on reward, cognitive control, and social cognition brain networks, and the interactions between oxytocin and testosterone across development would be most fruitful. Studies that directly assess adolescent gender differences (in contrast to statistically controlling for gender) in neural activity during prosocial behavior are needed. Manipulating behavioral economic task conditions can assist with isolating context-related differences between male and female prosocial behavior. For instance, comparing prosocial behavior that is directed at individuals with varying degrees of closeness (i.e., strangers versus friends) may lead to gender differences and may also elucidate the effects of oxytocin and testosterone on prosocial behavior, as these hormones are both sensitive to the in-group versus out-group distinction. Moreover, manipulating social desirability (e.g., popularity) of prosocial targets may differentiate between self- versus other-oriented prosocial motivations, such that other-oriented individuals (e.g., girls) might behave prosocially towards all targets, even at a personal cost, whereas more self-oriented individuals (e.g., boys) would restrict prosocial behavior towards the most desirable peer in order to gain favor or some other personal benefit. Most importantly, longitudinal assessments of the effects of prosocial behavior, specifically altruistic prosocial development, on depressive symptoms are needed. By elucidating this relationship, we stand to uncover behavioral risk factors and markers of MDD that will be much more amenable for use in prevention and intervention efforts.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance
Katz SJ, Conway CC, Hammen CL, Brennan PA, Najman JM. Childhood social withdrawal, interpersonal impairment, and young adult depression: a mediational model. J Abnorm Child Psychol. 2011;39(8):1227–38. doi:10.1007/s10802-011-9537-z.
Flynn E, Ehrenreich SE, Beron KJ, Underwood MK. Prosocial behavior: long-term trajectories and psychosocial outcomes. Soc Dev. 2015;24(3):462–82. doi:10.1111/sode.12100.
Davis AN, Carlo G, Schwartz SJ, Unger JB, Zamboanga BL, Lorenzo-Blanco EI, et al. The longitudinal associations between discrimination, depressive symptoms, and prosocial behaviors in U.S. Latino/a recent immigrant adolescents. J Youth Adolesc. 2016;45(3):457–70. doi:10.1007/s10964-015-0394-x.
Haroz EE, Murray LK, Bolton P, Betancourt T. Adolescent resilience in northern Uganda: the role of social support and prosocial behavior in reducing mental health problems. J Res Adolesc. 2013;23:138–48. doi:10.1111/j.1532-7795.2012.00802.x.
Padilla-Walker LM, Carlo G, Nielson MG. Does helping keep teens protected? Longitudinal bidirectional relations between prosocial behavior and problem behavior. Child Dev. 2015;86(6):1759–72. doi:10.1111/cdev.12411.
Musick MA, Wilson J. Volunteering and depression: the role of psychological and social resources in different age groups. Soc Sci Med. 2003;56(2):259–69. doi:10.1016/S0277-9536(02)00025-4.
Carlson M, Charlin V, Miller N. Positive mood and helping behavior: a test of six hypotheses. J Pers Soc Psychol. 1988;55(2):211–29.
Steger MF, Kashdan TB. Stability and specificity of meaning in life and life satisfaction over one year. J Happiness Stud. 2007;8:161–79. doi:10.1007/s10902-006-9011-8.
Simpson B, Willer R. Altruism and indirect reciprocity: the interaction of person and situation in prosocial behavior. Soc Psychol Quart. 2008;71(1):37–52.
• Lanaj K, Johnson RE, Wang M. When lending a hand depletes the will: the daily costs and benefits of helping. J Appl Psychol. 2016;101(8):1097–110. doi:10.1037/apl0000118. The costs and benefits of helping were determined using a daily diary across three work weeks of adults. This study found that responding to help requests leads to depletion of regulatory resources (i.e., internal energy consumed when regulating attention, managing emotions, etc). Notably, individuals that are more prosocially motivated are depleted to a larger extent and do not replenish to the same degree by the perceived prosocial impact of helping. The potential burden of prosocial behavior on well-being is highlighted by this study, suggesting that there is a personal cost that accompanies the benefits of prosocial behavior
Keenan K, Hipwell AE. Preadolescent clues to understanding depression in girls. Clin Child Fam Psychol Rev. 2005;8(2):89–105. doi:10.1007/s10567-005-4750-3.
Steinberg L. Cognitive and affective development in adolescence. Trends Cogn Sci. 2005;9(2):69–74. doi:10.1016/j.tics.2004.12.005.
Eisenberg N, Cumberland A, Guthrie IK, Murphy BC, Shepard SA. Age changes in prosocial responding and moral reasoning in adolescence and early adulthood. J Res Adolesc. 2005;15(3):235–60. doi:10.1111/j.1532-7795.2005.00095.x.
Nolen-Hoeksema S, Girgus JS. The emergence of gender differences in depression during adolescence. Psychol Bull. 1994;115(3):424–43. doi:10.1037/0033-2909.115.3.424.
Sannino S, Chini B, Grinevich V. Lifespan oxytocin signaling: maturation, flexibility, and stability in newborn, adolescent, and aged brain. Dev Neurobiol. 2017;77(2):158–68. doi:10.1002/dneu.22450.
Steinberg L. A social neuroscience perspective on adolescent risk-taking. Developmental review : DR. 2008;28(1):78–106. doi:10.1016/j.dr.2007.08.002.
Blakemore SJ, Burnett S, Dahl RE. The role of puberty in the developing adolescent brain. Hum Brain Mapp. 2010;31(6):926–33. doi:10.1002/hbm.21052.
Rudolph KD, Conley CS. The socioemotional costs and benefits of social-evaluative concerns: do girls care too much? J Pers. 2005;73(1):115–38. doi:10.1111/j.1467-6494.2004.00306.x.
Smith RL, Rose AJ. The "cost of caring" in youths’ friendships: considering associations among social perspective taking, co-rumination, and empathetic distress. Dev Psychol. 2011;47(6):1792–803. doi:10.1037/a0025309.
Carlo G, Randall BA. The development of a measure of prosocial behaviors for late adolescents. Journal of Youth and Adolescence. 2002;31(1):31–44. doi:10.1023/A:1014033032440.
• Eberly-Lewis MB, Coetzee TM. Dimensionality in adolescent prosocial tendencies: individual differences in serving others versus serving the self. Personal Individ Differ. 2015;82:1–6. doi:10.1016/j.paid.2015.02.032. This study explores whether adolescent prosocial tendencies can be distinguished by serving others (i.e., empathy) versus serving the self (i.e., egoistic). The study found that concern about disapproval, empathic concern and perspective taking are positively associated with emotional, dire and opportunistic prosocial tendencies, while concern about approval is positively correlated with dire, compliant and public prosocial tendencies. Narcissism and impulsivity are positively correlated with public prosocial tendencies. Boys are more likely to endorse public prosocial tendencies. This study exemplifies the multidimensionality of prosocial behavior and the motivations that support it
Kupferberg A, Bicks L, Hasler G. Social functioning in major depressive disorder. Neurosci Biobehav Rev. 2016;69:313–32. doi:10.1016/j.neubiorev.2016.07.002.
Sanathara VA, Gardner CO, Prescott CA, Kendler KS. Interpersonal dependence and major depression: aetiological inter-relationship and gender differences. Psychol Med. 2003;33(5):927–31. doi:10.1017/S0033291703007542.
Camerer CF. Neuroeconomics: opening the gray box. Neuron. 2008;60(3):416–9. doi:10.1016/j.neuron.2008.10.027.
• Declerck CH, Boone C, Emonds G. When do people cooperate? The neuroeconomics of prosocial decision making. Brain Cogn. 2013;81(1):95–117. doi:10.1016/j.bandc.2012.09.009. This is a review about the neuroeconomics of prosocial behavior that covers theory of social decision making, including economic (i.e., extrinsic) and social (e.g., trust) incentives and the neural systems engaged in costly prosocial behavior. Literature supporting the interpretation that (1) the reward network generates motivation to cooperate (or not), (2) the cognitive control network processes extrinsic incentives to inform prosocial motivation, and (3) the social cognition network processes social and threat signals that affect prosocial motivation is discussed. The function of these networks during altruistic punishment is also discussed
• Wang Y, Yang LQ, Li S, Zhou Y. Game theory paradigm: a new tool for investigating social dysfunction in major depressive disorders. Frontiers in psychiatry / Frontiers Research Foundation. 2015;6:128. doi:10.3389/fpsyt.2015.00128. The utility of behavioral economic theory as a tool for investigating dysfunction of prosocial behavior in major depressive disorders (MDD) is reviewed by first summarizing the most commonly used paradigms and by detailing studies that have utilized them in MDD populations. A substantial section of the review also discusses factors that modulate behavior in these economic paradigms, including social status, emotion, stake size and others. Limitations and biological bases of social dysfunction in MDD are also discussed
Sorgi KM, van’t Wout M. The influence of cooperation and defection on social decision making in depression: a study of the iterated Prisoner’s Dilemma Game. Psychiatry Res. 2016;246:512–9. doi:10.1016/j.psychres.2016.10.025.
Brendan Clark C, Thorne CB, Hardy S, Cropsey KL. Cooperation and depressive symptoms. J Affect Disord. 2013;150(3):1184–7. doi:10.1016/j.jad.2013.05.011.
Surbey MK. Adaptive significance of low levels of self-deception and cooperation in depression. Evol Hum Behav. 2011;32:29–40. doi:10.1016/j.evolhumbehav.2010.08.009.
Pulcu E, Thomas EJ, Trotter PD, McFarquhar M, Juhasz G, Sahakian BJ, et al. Social-economical decision making in current and remitted major depression. Psychol Med. 2015;45(6):1301–13. doi:10.1017/S0033291714002414.
Zhang HJ, Sun D, Lee TM. Impaired social decision making in patients with major depressive disorder. Brain and behavior. 2012;2(4):415–23. doi:10.1002/brb3.62.
Radke S, Schafer IC, Muller BW, de Bruijn ER. Do different fairness contexts and facial emotions motivate ‘irrational’ social decision-making in major depression? An exploratory patient study. Psychiatry Res. 2013;210(2):438–43. doi:10.1016/j.psychres.2013.07.017.
• Gradin VB, Perez A, Macfarlane JA, Cavin I, Waiter G, Tone EB, et al. Neural correlates of social exchanges during the Prisoner’s Dilemma game in depression. Psychol Med. 2016;46(6):1289–300. doi:10.1017/S0033291715002834. Behavior and brain activation of depressed and healthy adults was compared during the Prisoner’s Dilemma. Although behavior in the task did not differ by group, depressed adults reported more negative feelings during the game and showed less activation of the dorsolateral prefrontal cortex (DLPFC) during imbalanced events (i.e., defection by the participant or partner). Activation of DLPFC was negatively correlated with feelings of guilt. This study highlights the importance of the cognitive control network in response to proself behavior (i.e., participant defects, but partner cooperates) and receipt of proself behavior (i.e., partner defects, but participant cooperates)
• Gradin VB, Perez A, JA MF, Cavin I, Waiter G, Engelmann J, et al. Abnormal brain responses to social fairness in depression: an fMRI study using the Ultimatum Game. Psychol Med. 2015;45(6):1241–51. doi:10.1017/S0033291714002347. Behavior and brain activation during the Ultimatum Game (responder) is compared between healthy adults and adults diagnosed with major depressive disorder (MDD). Although groups do not differ based on behavior, adults with MDD report less happiness in response to fair offers. Moreover, increasing fairness of offers results in weaker nucleus accumbens and dorsal caudate activation in adults with MDD. The lack of nucleus accumbens activation is correlated with anhedonia. This study adds to the evidence that the reward network is involved in prosocial behavior during MDD and that affective blunting, by way of reduced reward network activation, may negatively impact prosocial behavior
• Shao R, Zhang HJ, Lee TM. The neural basis of social risky decision making in females with major depressive disorder. Neuropsychologia. 2015;67:100–10. doi:10.1016/j.neuropsychologia.2014.12.009. Reciprocity in low- and high-risk conditions is measured using the Trust Game during functional magnetic resonance imaging and compared in women with MDD and women with no clinical dignosis. Women with MDD exhibit more prosocial behavior under low risk than non-clinical controls, but no differences are observed under high-risk conditions. However, depressive symptoms are not correlated with prosocial behavior in either condition. Patients also demonstrate weaker activation of dorsolateral prefrontal cortex during low-risk proself trials. This study illustrates that the cognitive control network is implicated in prosocial behavior
Caceda R, Moskovciak T, Prendes-Alvarez S, Wojas J, Engel A, Wilker SH, et al. Gender-specific effects of depression and suicidal ideation in prosocial behaviors. PLoS One. 2014;9(9):e108733. doi:10.1371/journal.pone.0108733.
Destoop M, Schrijvers D, De Grave C, Sabbe B, De Bruijn ER. Better to give than to take? Interactive social decision-making in severe major depressive disorder. J Affect Disord. 2012;137(1–3):98–105. doi:10.1016/j.jad.2011.12.010.
Scheele D, Mihov Y, Schwederski O, Maier W, Hurlemann R. A negative emotional and economic judgment bias in major depression. Eur Arch Psychiatry Clin Neurosci. 2013;263(8):675–83. doi:10.1007/s00406-013-0392-5.
Wang Y, Zhou Y, Li S, Wang P, Wu GW, Liu ZN. Impaired social decision making in patients with major depressive disorder. BMC psychiatry. 2014;14:18. doi:10.1186/1471-244X-14-18.
Allen NB, Badcock PB. The social risk hypothesis of depressed mood: evolutionary, psychosocial, and neurobiological perspectives. Psychol Bull. 2003;129(6):887–913. doi:10.1037/0033-2909.129.6.887.
Crone EA, Elzinga BM. Changing brains: how longitudinal functional magnetic resonance imaging studies can inform us about cognitive and social-affective growth trajectories. Wiley Interdiscip Rev Cogn Sci. 2015;6(1):53–63. doi:10.1002/wcs.1327.
Knoch D, Pascual-Leone A, Meyer K, Treyer V, Fehr E. Diminishing reciprocal fairness by disrupting the right prefrontal cortex. Science. 2006;314(5800):829–32. doi:10.1126/science.1129156.
• Telzer EH, Fuligni AJ, Lieberman MD, Galvan A. Neural sensitivity to eudaimonic and hedonic rewards differentially predict adolescent depressive symptoms over time. Proc Natl Acad Sci U S A. 2014;111(18):6600–5. doi:10.1073/pnas.1323014111. This study shows that activation in ventral striatum during an allocation game (variant of Dictator Game) predicts fewer depressive symptoms one year later in adolescents. In contrast, ventral striatum activation during a task that measures hedonic reward positively predicts depressive symptoms. Although behavior on the prosocial task does not predict depressive symptoms (not measured), this study demonstrates that brain activity in a brain region important for processing prosocial behavior (i.e., reward network) predicts depressive symptoms
McClure EB, Parrish JM, Nelson EE, Easter J, Thorne JF, Rilling JK, et al. Responses to conflict and cooperation in adolescents with anxiety and mood disorders. J Abnorm Child Psychol. 2007;35(4):567–77. doi:10.1007/s10802-007-9113-8.
Harle KM, Allen JJ, Sanfey AG. The impact of depression on social economic decision making. J Abnorm Psychol. 2010;119(2):440–6. doi:10.1037/a0018612.
• Espinosa MP, Kovarik J. Prosocial behavior and gender. Front Behav Neurosci. 2015;9:88. doi:10.3389/fnbeh.2015.00088. This study re-analyzes previously published papers to uncover how various treatment effects of behavioral economic paradigms affect prosocial behavior in men and women. They find that social framing tends to increase prosocial behavior in women, but not men. In contrast, encouraging reflection decreases prosociality in males, but not females. This study shows that prosocial behavior is malleable for both men and women, but in distinct ways and highlights the importance of experimental design when comparing performance across studies
Branas-Garza P, Cobo-Reyes R, Espinosa MP, Jimenez N, Kovarik J, Ponti G. Altruism and social integration. Game Econ Behav. 2010;69(2):249–57. doi:10.1016/j.geb.2009.10.014.
Branas-Garza P, Kovarik J, Neyse L. Second-to-fourth digit ratio has a non-monotonic impact on altruism. PLoS One. 2013;8(4). ARTN):e60419. doi:10.1371/journal.pone.0060419.
Grimm V, Mengel F. Let me sleep on it: delay reduces rejection rates in ultimatum games. Econ Lett. 2011;111(2):113–5. doi:10.1016/j.econlet.2011.01.025.
Willer R, Wimer C, Owens LA. What drives the gender gap in charitable giving? Lower empathy leads men to give less to poverty relief. Soc Sci Res. 2015;52:83–98. doi:10.1016/j.ssresearch.2014.12.014.
• Matsumoto Y, Yamagishi T, Li Y, Kiyonari T. Prosocial behavior increases with age across five economic games. PLoS One. 2016;11(7):e0158671. doi:10.1371/journal.pone.0158671. The association between age and prosocial behavior in adults (20 – 59 years old) is measured using the Prisoner’s Dilemma, a Dictator Game, a Public Goods Game and a Trust Game (trustee). Prosocial behavior increases with age and is mediated by (1) a decline in the belief that manipulating people is a wise strategy and (2) an increase in satisfaction with unilateral exploitation (in Prisoner’s Dilemma) with age. Participants play under baseline conditions (e.g., play against strangers, no social manipulations), which may explain the lack of gender differences reported (see Espinosa & Kovarik, 2015)
Balliet D, Li NP, Macfarlan SJ, Van Vugt M. Sex differences in cooperation: a meta-analytic review of social dilemmas. Psychol Bull. 2011;137(6):881–909. doi:10.1037/a0025354.
Rose AJ, Rudolph KD. A review of sex differences in peer relationship processes: potential trade-offs for the emotional and behavioral development of girls and boys. Psychol Bull. 2006;132(1):98–131. doi:10.1037/0033-2909.132.1.98.
Guroglu B, van den Bos W, Crone EA. Sharing and giving across adolescence: an experimental study examining the development of prosocial behavior. Front Psychol. 2014;5:291. doi:10.3389/fpsyg.2014.00291.
• Van Hoorn J, Van Dijk E, Guroglu B, Crone EA. Neural correlates of prosocial peer influence on public goods game donations during adolescence. Soc Cogn Affect Neurosci. 2016;11(6):923–33. doi:10.1093/scan/nsw013. Adolescents across a wide age range (9–18 years) participated in a Trust Game with partners of varying social closeness: friends, antagonists, neutral classmates and anonymous peers. Whereas 9- and 12-year-olds do not behave differently across partner types, older adolescents show more prosocial behavior toward friends. The age-related increases in prosocial behavior toward friends is mediated by perspective-taking skills. This study indicates the relevance of the target when engaging in prosocial behavior and the importance of measuring perspective-taking ability when examining developmental changes in prosociality
Steinmann E, Schmalor A, Prehn-Kristensen A, Wolff S, Galka A, Mohring J, et al. Developmental changes of neuronal networks associated with strategic social decision-making. Neuropsychologia. 2014;56:37–46. doi:10.1016/j.neuropsychologia.2013.12.025.
Overgaauw S, Guroglu B, Rieffe C, Crone EA. Behavior and neural correlates of empathy in adolescents. Dev Neurosci. 2014;36(3–4):210–9. doi:10.1159/000363318.
Will GJ, Crone EA, van Lier PA, Guroglu B. Longitudinal links between childhood peer acceptance and the neural correlates of sharing. Dev Sci. 2016; doi:10.1111/desc.12489.
van den Bos W, van Dijk E, Westenberg M, Rombouts SA, Crone EA. Changing brains, changing perspectives: the neurocognitive development of reciprocity. Psychol Sci. 2011;22(1):60–70. doi:10.1177/0956797610391102.
Fett AK, Gromann PM, Giampietro V, Shergill SS, Krabbendam L. Default distrust? An fMRI investigation of the neural development of trust and cooperation. Soc Cogn Affect Neurosci. 2012;9(4):395–402. doi:10.1093/scan/nss144.
Moor BG, Guroglu B, Op de Macks ZA, Rombouts SA, Van der Molen MW, Crone EA. Social exclusion and punishment of excluders: neural correlates and developmental trajectories. NeuroImage. 2012;59(1):708–17. doi:10.1016/j.neuroimage.2011.07.028.
• Molina JA, Gimenez-Nadal JI, Cuesta JA, Gracia-Lazaro C, Moreno Y, Sanchez A. Gender differences in cooperation: experimental evidence on high school students. PLoS One. 2013;8(12):e83700. doi:10.1371/journal.pone.0083700. Male and female adolescent prosocial behavior is compared using the Prisoner’s Dilemma. Participants were instructed that they would be playing against neighboring students that comprised a social network. This study ( n = 1,200) finds that male adolescents engage in less cooperation than females, supporting previous research showing that females are more prosocial than males, particularly when their behavior is socially framed
• Derks J, Lee NC, Krabbendam L. Adolescent trust and trustworthiness: role of gender and social value orientation. J Adolesc. 2014;37(8):1379–86. doi:10.1016/j.adolescence.2014.09.014. Gender differences in prosocial behavior are measured in adolescents ( n = 206) using the Trust Game (trustor and trustee). Youth are instructed that they would play against adolescents from another school over the internet. They found that boys are more trusting (trustor) than girls, but no gender differences in trustworthiness (trustee) are observed. Girls are more likely to rate themselves as “prosocials” than “proselfs” (i.e., social value orientation) and prosocials are more trusting and trustworthy than proselfs. Social value orientation and gender predict trusting behavior independently, but only social value orientation significantly predicts trustworthiness. The gender difference in trusting behavior also supports the notion that males are less risk averse than females
• Keil J, Michel A, Sticca F, Leipold K, Klein AM, Sierau S, et al. The Pizzagame: a virtual public goods game to assess cooperative behavior in children and adolescents. Behav Res Methods. 2016; doi:10.3758/s13428-016-0799-9. An age-appropriate version of Public Goods Game is used to measure prosocial behavior in 191 youth between the ages of 9 and 16 years old. Participants are instructed they would play the game with two same-aged, same-sex co-players. Youth demonstrate more cooperation as the cooperativeness of their co-players increases; however, age and gender do not influnece prosocial behavior in any condition (cooperative, selfish and divergent co-players). The task was developed to be “as gender-neutral as possible,” which may explain the lack of sex differences
Sutter M, Kocher MG. Trust and trustworthiness across different age groups. Game Econ Behav. 2007;59(2):364–82. doi:10.1016/j.geb.2006.07.006.
• Crespi BJ. Oxytocin, testosterone, and human social cognition. Biol Rev Camb Philos Soc. 2016;91(2):390–408. doi:10.1111/brv.12175. This review covers the physiology, neurobiology, psychology and evolutionary biology of oxytocin before describing the opposing functions of testosterone. The functions of oxytocin and testosterone are integrated into a model for studying psychotic and affective disorders framed around the concept of mentalizing, such that (1) higher testosterone and lower oxytocin predict hypo-mentalizing, which is characteristic of disorders like autism and (2) lower testosterone and higher oxytocin predict hyper-mentalizing, which is characteristic of psychotic and affective disorders. This review highlights the relavance of oxytocin and testosterone in affective disorders like MDD and provides a means through which these hormones may connect to prosocial behavior—mentalizing or perspective taking
De Dreu CK. Oxytocin modulates the link between adult attachment and cooperation through reduced betrayal aversion. Psychoneuroendocrinology. 2012;37(7):871–80. doi:10.1016/j.psyneuen.2011.10.003.
De Dreu CK, Greer LL, Handgraaf MJ, Shalvi S, Van Kleef GA, Baas M, et al. The neuropeptide oxytocin regulates parochial altruism in intergroup conflict among humans. Science. 2010;328(5984):1408–11. doi:10.1126/science.1189047.
Daughters K, Manstead AS, Ten Velden FS, De Dreu CK. Oxytocin modulates third-party sanctioning of selfish and generous behavior within and between groups. Psychoneuroendocrinology. 2016;77:18–24. doi:10.1016/j.psyneuen.2016.11.039.
Declerck CH, Boone C, Kiyonari T. Oxytocin and cooperation under conditions of uncertainty: the modulating role of incentives and social information. Horm Behav. 2010;57(3):368–74. doi:10.1016/j.yhbeh.2010.01.006.
Declerck CH, Boone C, Kiyonari T. The effect of oxytocin on cooperation in a prisoner’s dilemma depends on the social context and a person’s social value orientation. Soc Cogn Affect Neurosci. 2014;9(6):802–9. doi:10.1093/scan/nst040.
Radke S, de Bruijn ER. The other side of the coin: oxytocin decreases the adherence to fairness norms. Front Hum Neurosci. 2012;6:193. doi:10.3389/fnhum.2012.00193.
Zheng H, Kendrick KM, Yu R. Fear or greed? Oxytocin regulates inter-individual conflict by enhancing fear in men. Horm Behav. 2016;85:12–8. doi:10.1016/j.yhbeh.2016.07.003.
Yao S, Zhao W, Cheng R, Geng Y, Luo L, Kendrick KM. Oxytocin makes females, but not males, less forgiving following betrayal of trust. Int J Neuropsychopharmacol. 2014;17(11):1785–92. doi:10.1017/S146114571400090X.
Feng C, Hackett PD, DeMarco AC, Chen X, Stair S, Haroon E, et al. Oxytocin and vasopressin effects on the neural response to social cooperation are modulated by sex in humans. Brain Imaging Behav. 2015;9(4):754–64. doi:10.1007/s11682-014-9333-9.
Feng C, Lori A, Waldman ID, Binder EB, Haroon E, Rilling JK. A common oxytocin receptor gene (OXTR) polymorphism modulates intranasal oxytocin effects on the neural response to social cooperation in humans. Genes Brain Behav. 2015;14(7):516–25. doi:10.1111/gbb.12234.
Christensen JC, Shiyanov PA, Estepp JR, Schlager JJ. Lack of association between human plasma oxytocin and interpersonal trust in a Prisoner’s Dilemma paradigm. PLoS One. 2014;9(12):e116172. doi:10.1371/journal.pone.0116172.
Fujii T, Schug J, Nishina K, Takahashi T, Okada H, Takagishi H. Relationship between salivary oxytocin levels and generosity in preschoolers. Sci Rep. 2016;6:38662. doi:10.1038/srep38662.
Barraza JA, Zak PJ. Empathy toward strangers triggers oxytocin release and subsequent generosity. Ann N Y Acad Sci. 2009;1167:182–9. doi:10.1111/j.1749-6632.2009.04504.x.
Rilling JK, Demarco AC, Hackett PD, Chen X, Gautam P, Stair S, et al. Sex differences in the neural and behavioral response to intranasal oxytocin and vasopressin during human social interaction. Psychoneuroendocrinology. 2014;39:237–48. doi:10.1016/j.psyneuen.2013.09.022.
Christ CC, Carlo G, Stoltenberg SF. Oxytocin receptor (OXTR) single nucleotide polymorphisms indirectly predict prosocial behavior through perspective taking and empathic concern. J Pers. 2016;84(2):204–13. doi:10.1111/jopy.12152.
Levy T, Bloch Y, Bar-Maisels M, Gat-Yablonski G, Djalovski A, Borodkin K, et al. Salivary oxytocin in adolescents with conduct problems and callous-unemotional traits. Eur Child Adoles Psy. 2015;24(12):1543–51. doi:10.1007/s00787-015-0765-6.
• Sasaki T, Hashimoto K, Oda Y, Ishima T, Yakita M, Kurata T, et al. Increased serum levels of oxytocin in ‘Treatment Resistant Depression in Adolescents (TRDIA)’ group. PLoS One. 2016;11(8):e0160767. doi:10.1371/journal.pone.0160767. This study examines the association between serum oxytocin and a diagnosis of treatment-resistant depression in adolescence. Oxytocin levels are higher in treatment-resistant depression compared to non-treatment resistant depression and healthy controls. However, depressive symptoms are not significantly correlated with oxytocin levels. This study supports the the finding that higher oxytocin levels are present in individuals with major depressive disorder, but extends it to an adolescent population
Burnham TC. High-testosterone men reject low ultimatum game offers. Proc Biol Sci. 2007;274(1623):2327–30. doi:10.1098/rspb.2007.0546.
Zak PJ, Kurzban R, Ahmadi S, Swerdloff RS, Park J, Efremidze L, et al. Testosterone administration decreases generosity in the ultimatum game. PLoS One. 2009;4(12):e8330. doi:10.1371/journal.pone.0008330.
Mehta PH, Beer J. Neural mechanisms of the testosterone-aggression relation: the role of orbitofrontal cortex. J Cogn Neurosci. 2010;22(10):2357–68. doi:10.1162/jocn.2009.21389.
Prasad S, Narayanan J, Lim VK, Koh GC, Koh DS, Mehta PH. Preliminary evidence that acute stress moderates basal testosterone’s association with retaliatory behavior. Horm Behav. 2016; doi:10.1016/j.yhbeh.2016.10.020.
Dreher JC, Dunne S, Pazderska A, Frodl T, Nolan JJ, O’Doherty JP. Testosterone causes both prosocial and antisocial status-enhancing behaviors in human males. Proc Natl Acad Sci U S A. 2016;113(41):11633–8. doi:10.1073/pnas.1608085113.
Huoviala P, Rantala MJ. A putative human pheromone, androstadienone, increases cooperation between men. PLoS One. 2013;8(5):e62499. doi:10.1371/journal.pone.0062499.
Cueva C, Roberts RE, Spencer TJ, Rani N, Tempest M, Tobler PN, et al. Testosterone administration does not affect men’s rejections of low ultimatum game offers or aggressive mood. Horm Behav. 2017;87:1–7. doi:10.1016/j.yhbeh.2016.09.012.
Reimers L, Diekhof EK. Testosterone is associated with cooperation during intergroup competition by enhancing parochial altruism. Front Neurosci. 2015;9:183. doi:10.3389/fnins.2015.00183.
Diekhof EK, Wittmer S, Reimers L. Does competition really bring out the worst? Testosterone, social distance and inter-male competition shape parochial altruism in human males. PLoS One. 2014;9(7):e98977. doi:10.1371/journal.pone.0098977.
Boksem MA, Mehta PH, Van den Bergh B, van Son V, Trautmann ST, Roelofs K, et al. Testosterone inhibits trust but promotes reciprocity. Psychol Sci. 2013;24(11):2306–14. doi:10.1177/0956797613495063.
Eisenegger C, Naef M. Combining behavioral endocrinology and experimental economics: testosterone and social decision making. Journal of Visualized Experiments: JoVE. 2011;49 doi:10.3791/2065.
Yildirim BO, Derksen JJL. A review on the relationship between testosterone and life-course persistent antisocial behavior. Psychiatry Res. 2012;200(2–3):984–1010. doi:10.1016/j.psychres.2012.07.044.
Amanatkar HR, Chibnall JT, Seo BW, Manepalli JN, Grossberg GT. Impact of exogenous testosterone on mood: a systematic review and meta-analysis of randomized placebo-controlled trials. Ann Clin Psychiatry. 2014;26(1):19–32.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Dr. Gabriela Alarcón and Dr. Erika E. Forbes declare that they have no conflicts of interest.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
This article is part of the Topical Collection on Child and Developmental Psychiatry
Rights and permissions
About this article

Cite this article
Alarcón, G., Forbes, E.E. Prosocial Behavior and Depression: a Case for Developmental Gender Differences. Curr Behav Neurosci Rep 4, 117–127 (2017). https://doi.org/10.1007/s40473-017-0113-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40473-017-0113-x