
Abstract
Aim
This was to determine dental caries determinants in the study participants.
Methodology
This was a secondary data study extracted from primary data through a school-based study that recruited students from primary and secondary schools in a suburban population in Nigeria. The variables included age, gender, socio-economic status, oral hygiene status, type of parenting, birth rank, family size and presence of dental caries. The diagnosis of dental caries was based on the World Health Oral Health Survey recommendations while oral hygiene was determined using simplified-oral hygiene index (OHI-S). Data was analysed using STATA version 13, statistical significance was set at P < 0.05.
Results
The prevalence of dental caries for the study population was 12.2%, DMFT and dmft were 0.16 and 0.06 respectively. Children within age groups 11–13 and 14–16 years had reduced chances of having dental caries (P = 0.01; P = 0.01); children with fair oral hygiene and poor oral hygiene had increased odds of having dental caries (P ≤ 0.001; P ≤ 0.001), last child of the family also had increased odds of having dental caries while children from large family size had reduced odds of having dental caries. This study also showed that first permanent molars and second primary molars were mostly affected by dental caries but there was no significant difference between distribution of the maxillary or mandibular jaw or between right and left quadrants.
Conclusion
Age, oral hygiene, birth rank and family size were the significant determinants of dental caries in the study population and the teeth mostly affected were first permanent molars and second primary molars.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Dental caries is a complex chronic oral disease and the most prevalent chronic disease of childhood (Mignogma and Fedele 2006). It refers to the localised destruction of susceptible dental hard tissues by acidic by-products from the bacterial fermentation of dietary carbohydrate (Pau et al. 2008).
In spite of a range of oral diseases affecting the world’s population, dental caries continues to be the most prevalent oral disease in children and adolescents worldwide, leading to pain, poor nutrition, time out of school and interference with quality of life (Petersen 2003; Egri and Gunay 2004; Blumenshine et al. 2008).
Dental caries is a multifactorial disease that has a complex interaction of cultural, social, behavioural, nutritional and biological risk factors that are associated with its initiation and progression (Ismail et al. 1997). Other factors include poor oral hygiene (Parisotto et al. 2010; Arora et al. 2011) low maternal education (Congiu et al. 2014; Baggio et al. 2015). A child’s family structure is an important social factor that has a significant effect on the oral health of children, playing a critical role on how the physical and emotional support needed to cope with a disease, its treatment, and its financial burden are provided (Mayo et al. 2000). Reports from a study among Brazilian children showed that dental caries is more common in children from single-parent families and those with parents of low educational level, especially of illiterate mothers (Maciel et al. 2001).
In Nigeria, a significant number (9%) of children live without biological parents (National Population Commission 2009) and many children living with guardians do not receive the much-needed attention as do children living with their biological parents (Chipungu and Bent-Goodley 2004). Folayan et al. (2010) that dmft/DMFT was higher in subjects who were only-children and last children in the family but the study failed to establish any increased risk for caries as the birth rank increases or decreases. Family size, birth rank, age difference between the subject and next oldest sibling and parent’s age at birth of the subject were significantly associated with the dental caries experience of the study participant (Wellappuli and Amarasena 2012). In addition, another Nigerian study (Folayan et al. 2017) reported that the number of siblings and the birth rank increased the chances of having caries and use of fluoridated toothpaste respectively, among their study participants. Vaneeobbergen et al. (2001) reported that gender, age, oral hygiene habits, use of fluorides, dietary habits, geographical factors and parental modelling were considered to be predictors for dental caries.
Poor oral hygeine and age have beeen established as determining factors for dental caries. In fact studies have shown that dmft/DMFT decreased with increasing age (Jablonski-Momeni et al. 2014) and that there is an association between the risk of developing dental caries and poor oral hygiene habits and consuming sugary foods and drinks (Vaneeobbergen et al. 2001; Mwakayoka et al. 2017). Hence this study aimed at assessing the determinants of dental caries among children and adolescents so that the findings could be used in the prevention of dental caries. Specifically, this study explored the impact of oral hygiene on dental caries and association of socio-demographic factors (age, gender, socio-economic status, birth rank, family size and type of parenting) on dental caries prevalence among the study participants.
Methodology
Study population
The data used for this study was secondary data extracted from primary data which was collected through a school-based study that recruited students from primary and secondary schools in a suburban population in Nigeria. This was a cross-sectional study that recruited primary and secondary school students aged 8–16 years, residing in Ile-Ife Nigeria. One of the objectives of the main study was to determine the co-morbidity associated with molar-incisor hypomineralisation. Details of the primary study have been reported by Oyedele et al. (2015).
Sample selection
The study participants were recruited through a multi-stage sampling technique involving both public and private schools, primary and secondary schools in order to ensure adequate representation of all the socio-economic strata. The details of this sampling technique have been previously reported by Oyedele et al. (2015).
Sample size calculation
The sample size for this study was arrived at using the formula proposed by Araoye (2003) for epidemiological study. Previous studies in the study environment showed caries prevalence of 13.9–17.4% (Kubota et al. 1990; Adekoya-Sofowora et al. 2006; Oziegbe and Esan 2013). Using an average of 15.7%, the minimum sample size for the population was 203 children. However, the data available for analysis of this study was based upon 2017 samples.
Methods of data collection
Self-administered questionnaires were used for the participants in the secondary schools, while interviewer-administered questionnaires were used for those in the primary schools. The questionnaires captured the age as at last birthday, gender, socio-economic status, type of parenting, birth rank and the number of children in the family.
The socio-economic status was determined using a multiple scoring index that utilizes the mother’s level of education and the father’s profession (Bernard 1957). This scoring index had been previously used for studies in this environment (Olusanya et al. 1985; Folayan et al. 2003). Each child’s socio-economic status was classified as Class I (upper class), Class II (upper middle class), Class III (middle class), Class IV (lower middle class) and Class V (lower class). Study participants were also asked about their birth position, the number of children in the family and the form of parenting, whether by both parents, single parent or other forms of parenting.
Oral hygiene examination
The oral hygiene of the study participants was determined using the simplified-oral hygiene index (OHI-S) described by Greene and Vermillion (1964). The calculus index simplified (CI-S) and debris index simplified (DI-S) values may range from 0 to 3, the OHI-S value that is the sum of CI-S and DI-S ranged from 0 to 6. Oral hygiene index score of 0–1.2 meant good oral hygiene; 1.3–3.0 meant fair oral hygiene and 3.0–6.0 meant poor oral hygiene.
Dental caries examination
The diagnosis of dental caries was based on the World Health Oral Health Survey recommendations (WHO 2005). Each tooth was examined for dental caries using a plain mouth mirror under natural light while the child was seated on a chair. Caries status was assessed using the Decayed Missing and Filled (DMFT) index for permanent teeth and decayed missing teeth (dmft) for the primary teeth. Decayed (D/d) teeth were defined as any tooth whose crown had an unmistakable cavitation on the pits or fissures, or on a tooth surface or a filled crown with decay, when it has one or more permanent restorations that are decayed. The F/f was defined as a filled crown with no decay, when it had one or more permanent restorations, and there is no caries anywhere on the crown. The M/m was defined as a missing tooth due to caries; when a tooth has been extracted due to caries. To arrive at a DMFT/dmft score for each participant, three values must be determined: the number of teeth with carious lesions, the number of extracted teeth due to caries, and the number of teeth with fillings or crowns. The numbers of teeth are then summed together to give the DMFT score for the permanent dentition and dmft score for the primary teeth.
Intra-examiner reliability
Before the commencement of the study one of the authors (TAO) went through a series of calibration exercises for dental caries detection. Calibration for dental caries was completed using a pictorial chart of teeth with carious lesions of different patterns. This was then followed by the examination and diagnosis of carious lesion, in live patients at different intervals. The data was then subjected to unweight kappa scores analysis, to determine intra-examiner reliability, which was 0.91.
Data analysis
The socio-economic status of the children was grouped into 3 during data entry. Classes1 and II were classified as high socio-economic status, class III remained the middle socio-economic status and classes IV and V were classified as low socio-economic status. The age of the participants was also grouped into three, 8–10, 11–13, and 14–16 years age groups. This age grouping was used in the previous study (Oyedele et al. 2015).
Birth rank was grouped into first born, last born and other birth ranks. The number of children in the family was grouped into 0–1, 2–4 and more than 4. Association between age, gender, socio-economic status, birth rank, number of children and type of parenting was determined using Chi square analysis. The determinants of dental caries were assessed using logistics regression. The reference groups in the model were females, children from the low socio-economic status, other birth ranks, more than one child and living with both parents. Statistical analysis was conducted with the use of STATA version 12.0. Statistical significance was established at P values equal to or less than 0.05.
Ethical clearance
Ethical clearance for the primary study was obtained from Obafemi Awolowo University Teaching Hospitals Complex, Ile-Ife Health Research Ethics Committee (ERC/2011/06/03).
Results
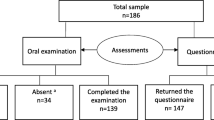
Data available for 2,107 children and for this secondary data analysis. There were 53.4% females and while 46.6% males that participated in this study. Two hundred and fifty-eight of the study population had dental caries in one or more teeth giving a prevalence of 12.2%. The DMFT of the population was 0.16 and dmft was 0.06.
Table 1 shows the association between dental caries, oral hygiene and socio-demographic variables. The age distribution of participants with dental caries shows that age group 8–10 years had higher caries prevalence (16.4%) compared with age groups 11–13 years (11.0%) and 14–16 years (11.1%), the association between dental caries and age distribution was found to be statistically significant (χ2 = 9.8, P = 0.01). In terms of gender distribution there was no significant difference in the prevalence distribution between males and females (12.1 vs 12.4%; χ2 = 0.03, P = 0.87).
In addition, Table 1 showed the socio-economic status of the study participants, there was slight higher prevalence of dental caries among children from high socio-economic group compare to middle and low socio-economic group. The association between dental caries and socio-economic status was however not statistically significant (χ2 = 2.19, P = 0.34).
Table 1 also showed the relationship between dental caries and oral hygiene, children with fair oral hygiene and poor oral hygiene had high prevalence of dental caries (14.5, 15.7% respectively) compare with children with good oral hygiene (9.0%). The association between oral hygiene and dental caries was statistically significant (χ2 = 16.66, P = ≤ 0.001). There was no statistically significant association between dental caries and type of parenting (χ2 = 1.23, P = 0.54), and dental caries and birth rank (χ2 = 2.24, P = 0.33). However, children who were the only child of the family had higher caries prevalence (23.7%) compared with children from a family size of 2–4 children (12.8%) or greater than four children (10.6%). The association between the number of children in the family and dental caries was statistically significant (χ2 = 6.73, P = 0.04).
Table 2 shows determinants of dental caries among the study participants. Age, oral hygiene, birth rank and number of children in the family were the significant determinants of dental caries in the study population. Children from age group 11–13 years (AOR 0.61; P = 0.01) and age group 14–6 years (AOR 0.62; P = 0.01) were less likely to have dental caries when compared to children from age group 8–10 years.
Also children with fair oral hygiene (AOR 1.73; P ≤ 0.001) and poor oral hygiene (AOR 2.13; P ≤ 0.001) were more likely to have dental caries when compared with children with good oral hygiene. Children that were the last child of the family were also more likely to have dental caries (AOR 1.50; P = 0.03) compared to the first child and other birth ranks and children from a family with 2–4 children (AOR 0.36; P = 0.01) and greater than four children (AOR 0.30; P = 0.00) were less likely to develop dental caries compared to a family with an only-child.
Table 3 shows the distribution of teeth affected by dental caries in the study participants. First permanent molars were the teeth mostly affected by dental caries in this study population (72.6%) followed by second permanent molars (21.9%) and the least affected teeth were canine and third permanent molars (0.7%). For the carious primary teeth in this study population, second primary molars were mostly affected by dental caries (64.0%) and the least were the canines (1.6%).
Table 4 shows jaw distributions of teeth affected by dental caries. Dental caries was found more in the mandibular jaw (70.8%) compared to the maxillary jaw (29.2%) and the left quadrants recorded higher percentage of dental caries (54.5%) compared with right quadrants (45.5%). The association between jaw distribution and dental caries was statistically non-significant (χ2 = 0.33, P = 0.57).
Discussion
The main objective of the present study was to identify the determinants of dental caries among the children aged 8–16 years living in a suburban population. We specifically looked at the effect of age, gender, oral hygiene, socio-economic status, birth rank, type of parenting and number of children on dental caries. This study showed that age, oral hygiene, birth rank, and number of children in the family were significant determinants of dental caries.
The study also showed that teeth mostly affected by dental caries were first permanent molar for permanent teeth and second primary molar in primary dentition. There was no significant difference in the jaw or quadrant affected by dental caries in this study population.
The prevalence of dental caries recorded in this present study was 12.2%, this prevalence was close to those reported by Denloye et al. (2005), higher to that reported by Oziegbe and Esan (2013) among 7–12 and 13–16 years, and that reported by Kolawole et al. (2016) in the same study environment.
The findings of this study are similar to previous studies. For instance, we found that the chance of having dental caries was reduced by about 60% in older age groups (11–13, 14–16 years) when compared to younger age groups (8–10 years) in the study participants. This was similar to the study by Oziegbe and Esan (2013) that reported higher prevalence in children 4–6 years as compared to children aged 7–12 and 13–16 years. It is however at variance with the study from the same environment by Kolawole et al. (2016) who showed that as age increases, caries risk increases. The higher prevalence of dental caries in the younger age group may not be unconnected to higher consumption of refined sugar. Folayan et al. (2010) suggested in their study that, even though many had postulated that caries experience was related to the length of time the tooth had stayed in the mouth being reason for some reporting higher caries experience in older age groups, there was the possibility that children who were predisposed to dental caries had lesions occurring at an early age. This may also explain the higher prevalence seen in younger age groups in this present study.
The results of this study also showed the significant role of oral hygiene in the aetiology of dental caries. This study showed that dental caries prevalence was higher in children with fair oral hygiene and poor oral hygiene as compared to children with good oral hygiene. Poor state of oral cleanliness resulting in fair or poor oral hygiene has been shown to lead to accumulation of bacterial plaque that harbour bacteria and their toxins which play an important role in development of dental caries (Bhayat et al. 2013).
This study also showed that children who were the last born in the family had a higher experience of dental caries. A previous study (Folayan et al. 2010) in this environment had reported that being a last-born was associated with higher caries experience but that study failed to establish any statistically significant association.
This present study was however able to establish a significant association between dental caries and birth rank. This may be attributed to the fact that last-born children in many families are usually given special preferences, as most of the older siblings tend to pamper the child by buying lots of refined sugar-containing snacks for them.
The present study also found significant association between the size of the family and dental caries; children from larger families had a lower chance of developing dental caries. This was however not in agreement with a previous study by Sujlana and Pannu (2015) who reported a higher dmft with a larger family size. Also, the study by Folayan et al. (2017) showed that children from larger families had higher caries experience that was attributed to a likely reduction in family expenses, which may necessitate purchase of non-fluoridated toothpaste. We found no explanation for our finding of higher caries experience for single children compared to those from larger families. However, we suggest that parents of only-children may indulge them in high sugar-containing diets and frequent refined carbohydrates between meals. In addition, children from larger family size may have little access to refined sugars, due to limited family income to cater for a large number and this may be a reflection of the socio-economic status of the parents.
This study also looked at the pattern of dental caries among the study participants, teeth most affected by dental caries were first permanent molars while second primary molars were the teeth most affected in the primary dentition. This was in agreement with the study by Bajomo et al. (2004) which also reported first permanent molars being affected. In addition it was observed that mandibular teeth were more affected than the maxillary teeth and more teeth were affected on the left side of the jaw compared to the right side of the jaw, this was similar to the finding by Manal and Yasser (2006).
One of the strengths of this study was the availability of large data that made the analysis to be robust however, the study failed to look into the association between parental level of education and dental caries. In addition, analysis of the effect of each of the components of the OHI-S would have added new information.
Conclusions
This study showed that fair oral hygiene, poor oral hygiene, age, birth rank and number of children in the family were significant determinants of dental caries in the study participants. It also showed that first permanent molars and second primary molars were the teeth most affected by dental caries in the study group. The findings of this study has added to general understanding of some of the determinants of dental caries and this will help to focus on these determinants in order to further prevent dental caries.
References
Adekoya-Sofowora CA, Nasir WO, Oginni AO, Taiwo M. Dental caries in 12-year-old suburban Nigerian school children. Afr Health Sci. 2006;6:145–50.
Araoye MO. Research methodology with statistics for health and social science. Ilorin: Nathadex Publisher; 2003. pp. 115–9.
Arora A, Schwarz E, Blinkhorn AS. Risk factors for early childhood caries in disadvantaged populations. J Investig Clin Dent. 2011;2:223–8.
Baggio S, Abarca M, Bodenmann P, Gehri M, Madrid C. Early childhood caries in Switzerland: a marker of social inequalitie BMC Oral Health. 2015;15:82.
Bajomo AS, Rudolph MJ, Ogunbodede EO. Dental caries in Six, 12 and 15 year-old venda children in South Africa. East Afr Med J 2004; 81.
Bernard B. Indices of social classification. In: Merton RK, editor. Social stratification: a comparative analysis of structure and process. 2nd ed. San Diego: Harcourt Brace; 1957. pp. 78–185.
Bhayat A, Ahmad MS, Hifnawy T, et al. correlating dental caries with oral bacteria and the buffering capacity of saliva in children in Madinah, Saudi Arabia. J IntSocPrev Community Dent. 2013;3(1):38–43.
Blumenshine SL, Vann WF Jr, Gizlice Z, Lee JY. Children’s school performance: impact of general and oral health. J Public Health Dent. 2008;68:82–7.
Chipungu SS, Bent-Goodley TB. Meeting the challenges of contemporary foster care. Future Child. 2004;14:74–93.
Congiu G, Campus G, Sale S, et al. Are distinctive risk indicators associated with different stages of caries in children? A cross-sectional studyJ. Public Health Dent. 2014;74:147 – 52.
Denloye O, Ajayi D, Bankole O. A study of dental caries prevalence in 12–14 year old school children in Ibadan, Nigeria. Pediatr Dent J. 2005;15:147–51.
Egri M, Gunay O. Association between some educational indicators and dental caries experience of 12-year-old children in developing countries: an ecological approach. Commun Dent Health. 2004;21:227–9.
Folayan MO, Idehen EE, Ufomata D. The effect of sociodemographic factors on dental anxiety in children seen in a suburban Nigerian hospital. Int J Paediatr Dent. 2003;13:20–6.
Folayan MO, Owotade F, Oziegbe EO, Fadeyibi R. Effect of birth rank on the caries experience of children from a suburban population in Nigeria. J Dent Oral Hyg. 2010;2:27–30.
Folayan MO, Kolawole KA, Oziegbe EO, et al. Association between family structure and oral health of children with mixed dentition in suburban Nigeria. J Indian Soc Pedod Prev Dent. 2017;35:134–42.
Greene JC, Vermillion JR. The simplified oral hygiene index. J Am Dent Assoc. 1964;68:7–13.
Ismail AI, Tanzer JM, Digle JL. Current trends of sugar comsumption in developing societies. Commun Dent Oral Epidmiol. 1997;25:438–43.
Jablonski-Momeni A, Winter J, Petrakakis P, Schmidt-Scheafer S. Caries prevalence (ICDAS) in 12year-olds from low caries prevalence areas and association with independent variables. Int J Paediatgr Dent. 2014;24:90–7.
Kolawole KA, Folayan MO, Agbaje HO, et al. digit sucking habit and association with dental caries and oral hygiene status of children aged 6 months to 12 years resident in semi-urban Nigeria. PLoS One. 2016;11(2):e0148322. https://doi.org/10.1371/journal.pone.0148322.
Kubota K, Yonemitsu M, Hollist NO,et al. Five-year follow-up caries study among Nigerian children. Commun Dent Oral Epidemiol. 1990;18:197–9.
Maciel SM, Marcenes W, Sheiham A. The relationship between sweetness preference, level of salivary mutans streptococci and caries experience in Brazilian pre-school children. Int J Paediatr Dent. 2001;11:123–30.
Manal IA, Yasser AR. Prevalence of dental caries, severity and pattern in age 6 to7-year-old children in a selected community in Saudi Arabia. J Contemp Dent Pract. 2006; 7.
Mayo NE, Wood-Dauphinee S, Côté R, et al. There’s no place like home: an evaluation of early supported discharge for stroke. Stroke. 2000;31:1016–23.
Mignogna M, Fedele S. The neglected global burden of chronic oral diseases. J Dent Res. 2006;85:390–1.
Mwakayoka H, Masalu JR, Namakuka Kikwilu E. Dental caries and associated factors in children aged 2–4 years old in Mbeya City. Tanzan J Dent. 2017;18:104–11.
National Population Commission [Nigeria]. Nigeria Demographic and Health Survey 2008. Calverton, Maryland: National Population Commission and ORC Macro; 2009.
Olusanya O, Okpere O, Ezimokhai M. The importance of social class in voluntary fertility control in developing country. West Afr J Med. 1985;4:205–12.
Oyedele TA, Folayan MO, Adekoya-Sofowora CA, Oziegbe EO. Co-morbidities associated with molar-incisor hypomineralisation in 8 to 16 year old pupils in Ile-Ife, Nigeria. BMC Oral Health. 2015. https://doi.org/10.1186/s12903-015-0017-7.
Ozeigbe EO, Esan TA. Prevalence and clinical consequences of untreated dental caries using PUFA index in suburban Nigerian school children. Eur Arch Paediatr Dent. 2013;14:227–31.
Parisotto TM, Steiner-Oliveira C, Silva CM, Rodrigues LK, Nobre-dos-Santos M. Early childhood caries and mutans streptococci: a systematic review. Oral Health Prev Dent. 2010;8:59–70.
Pau A, Khan SS, Baba MG, Croucher R. Dental pain and care-seeking in 11–14-year-old adolescents in a low-income country. Eur J Oral Sci. 2008;116:451–7.
Petersen PE, The World Oral Health Report. Continuous improvement of oral health in the 21st century—the approach of the WHO Global Oral Health Program. Commun Dent Oral Epidemiol. 2003;31:3–23.
Sujlana A, Pannu PK. Family related factors associated with caries prevalence in the primary dentition of five-year-old children. J Indian Soc Pedod Prev Dent. 2015;33:83–7.
Vanobbergen J, Martens L, Lesaffre E, Bogaerts K, Declerck D. Assessing risk indicators for dental caries in the primary dentition. Community Dent Oral Epidemiol. 2001;29:424–34.
Wellappuli N, Amarasena N. Influence of family structure on dental caries experience of preschool children in Sri Lanka. Caries Res. 2012;46(3):208–12.
World Health Organization. Oral health survey-basic method. 4th ed. Geneva: WHO; 2005.
Acknowledgements
The authors acknowledge the parents and pupils that participated in the study.
Funding
There was no external funding for this research; solely funded by authors.
Author information
Authors and Affiliations
Contributions
TAO conceived the idea and collected the data. FD, AYI, NCL AND LAM participated in the study design. TAO, FD, AYI, NCL AND LAM took part in data analysis and drafting of the final manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that there were no competing interests.
Rights and permissions
About this article

Cite this article
Oyedele, T.A., Fadeju, A.D., Adeyemo, Y.I. et al. Impact of oral hygiene and socio-demographic factors on dental caries in a suburban population in Nigeria. Eur Arch Paediatr Dent 19, 155–161 (2018). https://doi.org/10.1007/s40368-018-0342-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40368-018-0342-z