
Abstract
Migraine is a disabling and recurrent neurological disorder characterized by headache attacks that are often accompanied by sensory and motor disturbances. The value and importance of reliable biomarkers in migraine have been long recognized and a diverse range of biomarkers from biological samples to electrophysiological patterns and brain imaging has been proposed. There is still no consensus on specific biomarker(s) for migraine. Ideally, not a single but a battery of biomarkers would provide a multidisciplinary way to understand and treat migraine better. Translational research has witnessed an escalating number of studies on microRNAs (miRNAs) during the last decade. Identification of the first miRNA occurred in 1993, and currently more than 2000 human miRNAs have been recognized. miRNAs are a group of endogenous small non-coding molecules that play a key role in post-transcriptional gene processes and hence are involved in health and disease. miRNAs have already been found to be involved in the onset and progression of several human disorders including chronic pain conditions; however, there have been far fewer studies in migraine and other headaches. Current evidence does suggest that miRNAs play a role in migraine and its relief and hence these molecules are proposed as potential migraine biomarkers. This review updates the current evidence for the role of miRNAs in migraine; including their potential as biomarkers, with a role in understanding of its pathogenesis, the population at risk, diagnosis, patient stratification, chronification risk factors, response to treatments, and miRNA-based therapeutic options. Limitations exist and further research is required to completely unwrap the potential of miRNAs in migraine research and practice.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
1 Introduction to Migraine
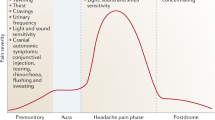
Migraine is one of the most common neurological disorders and has been listed among the top ten sources of disability [1]. Consequently, it causes a lowered quality of life and poses an economic burden to society due to direct treatment costs and indirect loss of employment and lowered work productivity [2]. Migraine occurs in pediatric, adult, and geriatric populations and demonstrates sex- and age-related phenotypes [3, 4]. Currently, the diagnosis of migraine is based on classification of headaches by the International Headache Society (3rd edition of the International Classification of Headache Disorders [ICHD-3]) [5], relying on clinical manifestations of associated symptoms including recurrent episodes of headache attacks lasting 4–72 h accompanied by sensory and motor disturbances [6]. Migraine appears with and without aura [7, 8]; at present, it is still controversial as to whether these are two distinct disorders or if they share a common initiating signaling pathway [9,10,11]. However, it is generally accepted that aura is a manifestation of cortical-spreading depression that occurs prior to migraine pain; it occurs in 20% of individuals [8, 12], mostly in the form of a visual aura [13]. Extensive investigation has revealed that the pathogenesis of migraine is complex [14], involves several regions of the nervous system, and is influenced by genetic factors [15, 16] and epigenetics [17,18,19]. Migraine is classified as episodic (EM; fewer than 15 migraine or headache days per month) or chronic (CM; during a 15-day period, 8 or more are migraine days) [20, 21]. Chronification of migraine has been explained partly by epigenetic mechanisms [18]. The hypothesis is that in migraine, frequent headache attacks may lower the threshold for subsequent attacks and synaptic plasticity occurs, resulting in a feed-forward loop, which may promote stable epigenetic changes and chronification [18]. Psychological stress and sex hormones are known to exert their effects in migraine, at least in part, through epigenetic mechanisms [17]. Hence, research is ongoing for disease modification in migraine by application of epigenetic approaches. Indeed, precision medicine has now been considered for migraine relief [17, 22], in which integration of genomic data, functional investigation, and data from biomarker-driven clinical trials can facilitate migraine molecular profiling to offer a multidisciplinary approach for treatment [22].
Therapeutic options for migraine, both abortive and prophylactic agents, are available [23], but are either only effective in a proportion of patients or carry off-target effects [24]. Recent studies have introduced new therapeutic agents for migraine that were developed following a ‘translational’ approach and ‘biomarker-based’ drug discovery process, in which calcitonin gene-related peptide (CGRP) was considered the initiative biomarker [25,26,27]. Both antagonists of CGRP receptor and antibodies against CGRP peptide and its receptor are being developed [26, 28], some of which have already been marketed [29, 30].
2 Biomarkers in Migraine
Recognition of the value and importance of reliable biomarkers in migraine is not a new concept and dates back to the 1990s [31]. The concept of biomarkers has been investigated for migraine diagnosis, providing insights into pathophysiology of migraine, response to treatment, and for drug development strategies. Over the years, several substances, e.g., neurotransmitters, neuropeptides, gliotransmitters, and hormones, have been proposed as potential biomarkers of migraine [32,33,34,35], including cytokines, homocysteine, serotonin, hypocretin-1, CGRP, and glutamate [36, 37]. Still, there are no commonly accepted, established, and validated biomarker(s) for migraine despite extensive interest and investigation, and perhaps this is partly due to the fact that many of these proposed substances are not solely specific to migraine [36]. Small study sample sizes, a diverse range of applied methodological approaches, lack of standard guidelines for sampling, assays and analysis, and non-uniform inclusion and exclusion criteria are also among potential contributors for the current inconclusive outcomes in the field of migraine biomarkers. A review from 2006 [38] presented several ‘types’ of biomarkers in migraine, including bio-fluid-based biomarkers, as well as their potentials, limitations, and practical applications [35, 38, 39]. According to the biomarker definition [40, 41], “a biomarker is a characteristic that is objectively measured and evaluated as an indicator of normal biologic processes, pathogenic processes, or pharmacological responses to a therapeutic intervention”. Hence, migraine biomarkers are characteristics that can be objectively measured to assist in migraine diagnosis, understanding pathogenesis, and responsiveness to treatments [36]. Besides potential migraine biomarkers that have been reported in biological samples (e.g., blood, urine, cerebrospinal fluid), there are also gene marker or gene products, x-ray, magnetic resonance or computed tomographic imaging findings, and patterns of electrocardiogram, electroencephalogram, or nerve conduction [35, 42]. Considering this broadness in the spectrum of migraine biomarkers, one can recognize considerable research potential in the understanding of migraine, in addition to the clinical potential for recognition of individuals at risk, improvement in diagnosis of migraine and to follow-up treatment response, disease phenotypes, or disease progression [31, 34]. One must consider important limitations of biomarkers in general, including concerns with validity, reliability, accuracy, and precision [43]. Similar to any other field, a combination of biomarkers might be more useful than a single marker to improve sensitivity and specificity [44]. Ethical and legal considerations and the associated expenses in the use of biomarkers [45] are also among the important factors to consider regarding use of biomarkers in the health sector [46].
Research is underway to identify novel, suitable, and effective biomarker candidates for migraine [34]. An ideal bio-based biomarker presents with high specificity, high sensitivity, early detection, and significant variation in levels during the different stages of a given disorder, with predictive potential, a long half-life, robustness, and translatable characteristics that can be assessed non-invasively in circulating bio-fluids [47]. Discovery of the non-coding RNA family has offered a promising set of biomarker candidates [48,49,50]. Non-coding RNAs can be divided in long non-coding RNAs (lncRNAs; > 200 nucleotides) and small non-coding RNAs (up to 22 nucleotides; microRNAs [miRNAs; miRs]) [51]. These classes are both reported to be involved in migraine [31, 52]; however, the high degree of stability of miRNAs [53] has identified them as attractive biomarkers and, so far, these have been most extensively studied [31]. miRNAs were identified for the first time in Caenorhabditis elegans [54] and are key regulators of gene expression at the post-transcriptional level [55], either by inhibition of translation or by leading to degradation of the messenger RNA (mRNA) target [45]. Advancement in technology has permitted isolation of these small molecules and the pattern of their alterations in body tissues or body fluids. For example, next-generation sequencing (NGS) is emerging as the preferred method for miRNA profiling; it offers high sensitivity, single-nucleotide resolution, and the possibility to profile a considerable number of samples in parallel [56]. Due to their cell-specific expression, miRNAs can provide mechanistic links to underlying pathological mechanisms of human diseases [57]. Altered levels of these stable circulating biomarkers in bio-fluids can also assist in clinical diagnosis, selecting appropriate treatment strategies, and monitoring treatment responses [58]. This review presents current evidence on potential use of miRNAs as migraine biomarkers for different purposes, from diagnosis to treatment.
2.1 MicroRNAs (miRNAs)
Post-transcription regulation of genes by miRNAs accounts for 30% of all protein-coding genes [59]. According to miRBase version 22, 1917 human precursors and 2656 mature miRNAs have been identified in humans [60]. A recent study has experimentally extrapolated 2300 true human mature miRNAs, of which 1115 are currently annotated in miRBase [61]. Downregulation of gene expression by miRNA at the post-transcriptional level is done either by degradation of specific mRNAs, mRNA when fully paired to the seed region binding site of the mRNA target, or by inhibition of translation through partial base-pairing to complementary sites [62, 63]. Conversely, miRNAs might upregulate translation by other mechanisms [64]. Hence, upregulation or downregulation of miRNAs can either provide disease protection or potentiate disease states, and circulating miRNAs can therefore be potential biomarkers of health and disease [47]. Consequently, they can be used for a diverse range of purposes, one of which is disease diagnosis [65,66,67]. A comprehensive overview on miRNA biogenesis, regulation, and cross-talk with other cellular pathways can be found in excellent recent reviews [55, 68].
During pathological conditions in patients, specific miRNAs are altered compared with healthy controls and this pattern change can be utilized as a molecular biomarker for disease diagnosis. In fact, along with a wide range of cancers, a significant correlation has been identified between specific miRNAs and certain other diseases, including epilepsy [69], Alzheimer’s disease [70], cardiovascular diseases [71], infectious diseases [72], diabetes mellitus [73], and in conditions where neuroinflammation is underlying mechanism of diseases [74]. Rationally, identification of miRNAs involved in diseases has potentiated research in targeting them. Due to their small size, relative ease of delivery, and sequence specificity in recognizing their targets, miRNAs are also considered promising therapeutic targets [75, 76].
2.1.1 miRNAs and Pain
miRNAs have also been explored in pain [77,78,79,80,81,82] and headache, including migraine [18, 31, 83,84,85,86], and findings from current data have also proposed great benefits for clinical diagnostic and therapeutic applications of miRNAs in pain and headache.
miRNAs in pain is a large area to cover and beyond the main scope of this review; therefore, it is only briefly discussed here with the purpose of providing some insights that can also be applied in migraine research and for inspirational purposes for further research. Readers are encouraged to see the excellent reviews that are available for updated comprehensive overviews on miRNA in pain [77, 78, 80, 81, 87,88,89,90,91,92], miRNA signatures in animal models of pain [93,94,95] (see Fig. 1) and a number of pain conditions in humans (see Table 1), miRNA modulation in analgesic research [95,96,97,98], and potential therapeutic targets [99, 100] (see Fig. 2).

Reused with permission, copyright © 2018 Dai et al. [95], https://doi.org/10.3389/fnmol.2018.00080, The Creative Commons Attribution License (CCBY)
The overlaps between dysregulated microRNAs (miRNAs; miRs). The circles include miRNAs that have been mainly implicated in nociceptive pain, neuropathic pain, bone cancer pain, microglia and morphine tolerance. Overlapping regions indicate miRNA intersections (in common) with the reported abnormal states. miRNAs are indicated in black, red, and yellow if dysregulated in one, two, and four states, respectively.

Reused with permission, copyright © 2018 Dai et al. [95], The Creative Commons Attribution License (CCBY), https://doi.org/10.3389/fnmol.2018.00080
MicroRNA (miRNA; miR) mimics and inhibitors administration in different rodent models of pain. Specific miRNAs that are altered in animal models of nociceptive pain (formalin, complete Freund’s adjuvant [CFA] or carrageenan injection), neuropathic pain (chronic constriction injury [CCI], partial sciatic nerve injury [SNL], spinal cord injury [SCI], spared nerve injury, or ventral root transection [VRT]), and cancer-related pain (bone cancer pain [BCP]) have been identified as potential therapeutic targets. Schematic indicates that viral vectors (lentivirus [LV], herpes simplex virus [HSV], or adeno-associated virus [AAV]), stabilized locked nucleic acid mimics, miRNA agomir or antagomir, and anti-miRNA oligonucleotides (AMO) are therapeutic strategies that have successfully reversed pain phenotypes.
miRNA expression profiles are altered in several pain-related disorders such as visceral pain [106], complex regional pain syndrome (CRPS) [82, 107], endometriosis [108], fibromyalgia [102], osteoarthritis [105], and rheumatoid arthritis [109]. Several basic studies have also examined alterations in miRNA expression in tissue samples collected from rodent models of inflammatory and neuropathic pain [81, 95]. It is therefore promising to consider circulating miRNAs (and potentially other non-coding RNAs) that can be associated with both nociceptive and neuropathic origins of pain syndromes [79]. Both neuronal and immune alterations in the peripheral and central nervous system have been found important in pathogenesis of pain [110]. Interestingly, miRNAs (and other non-coding RNAs) regulate both immune and neuronal processes [91]. miRNAs control functions of neurons, glia, and immune cells and regulate signals for cross-talk between neuronal and immune systems in pain signaling [91]. Therefore, miRNAs can act as master switches of pain modulation and, hence, identification of the pattern of miRNA expression, and its variations in different pain conditions [111] may provide benefit as biomarkers for nociception, pain, endogenous analgesia, and the analgesic response to therapeutics [91]. Indeed, it has been found that circulating miRNA levels are altered by pharmacological treatments, including analgesics, indicating a potential role for miRNA in mediating drug effects [96]. Drug modulation of miRNA may regulate downstream effectors responsible for therapeutic effects of a given drug, e.g., µ-opioid receptors [112]. miRNAs and miRNA polymorphisms can also modify a drug response [113]. miRNA-based therapeutics in pain may have superior advantages by targeting multiple pain-associated genes [91]. Moreover, modulating several miRNAs is useful in attenuating or preventing pain [81].
The potential therapeutic impact of miRNAs in pain is as yet largely unexplored. To date, therapeutic approaches have been mainly applied in rodent models. For example, miR-124 is upregulated after chronic constrictive nerve injury (CCI); intrathecal administration of miR-124 can prevent and treat persistent inflammatory and neuropathic pain [114]. Investigation is also ongoing on miRNAs that can be druggable molecular targets for pain [91]. Two of the more straightforward approaches for miRNA modulation are miRNA mimics and antagomirs [115]. Alternative methodologies are being used in the experimental setting, including miRNA sponges [116]. An important difficulty in developing neuronal miRNA therapeutics is delivery, since targeting the brain may involve crossing the blood–brain barrier [117, 118]. Another point to consider is off-target effects [91]. Nevertheless, therapeutic efficacy of certain approaches such as the use of LNA (locked nucleic acid) antagomirs has been demonstrated [119], and certain neuronal miRNA therapeutic approaches are now in preclinical development [120].
In addition to the potential for application of miRNA in diagnosis and treatment in pain conditions, assessing miRNA changes before and after treatment could provide insights into miRNA signatures and its alteration in good responders, placebo responders, and poor responders. For example, hsa-miR-124 expression in CD4 T cells in chronic low back pain has been shown to be predictive of treatment response [121]. Therefore, samples from both failed and successful clinical trials can provide meaningful insights and guidance for design of future clinical trials [96], assist ongoing trials, and clinical applications such as decision-making regarding choice or response to treatment [53]. miRNAs are also expected to have potential for personalized pain medicine as biomarkers for risk assessment, drug selection, and non-pharmacological strategies for pain relief [80].
2.1.2 miRNAs and Migraine
The literature demonstrates that miRNAs play a role in migraine [17, 31, 73]. This role is yet to be clarified, but altered miRNA levels in human bio-fluids can be used as a potential biomarker in differentiation of, for example, primary headache disorders such as cluster headache, tension-type headache, and migraine; phases of a headache disorder, such as migraine phases; types of a headache disorders, such as EM versus CM; or could even provide more insight into migraine with and without aura.
miRNA alterations that occurred during migraine attacks and pain-free periods were investigated by our group [86, 122]. Migraineurs and age- and sex-matched healthy controls were included from two cohorts and serum miRNA profiles of migraineurs during attacks, and pain-free periods in comparison with healthy controls were assessed by high-content serum miRNA arrays. Of the 372 assessed, 32 miRNAs were found differentially expressed and miR-34a-5p, miR-29c-5p, miR-382-5p, and miR-26b-3p were selected for further analysis. During migraine attacks, an acute upregulation in miR-34a-5p and miR-382-5p expression was evident. Interestingly, miR-382-5p, which exhibited an upregulation during an attack, also presented differentiation in pain-free periods in migraine patients compared with the healthy control group. This study [86] showed that miRNA aberrations occur in migraine attack, but also that some alterations remain sustained in pain-free periods. Opposite to our findings, another study published in 2014 [123] failed to demonstrate any differences in miRNA expression profiles of blood cells in migraine. This study recruited 20 migraine patients (EM and CM, with and without aura) together with five healthy controls. The patient group and controls were best matched for age, sex, and family history of migraine. To profile miRNA expression in this study, RNA was extracted from peripheral blood mononuclear cells (PBMCs) and the results did not show any differences in miRNA expression in these cells in migraine. The authors consequently proposed that cell sources for miRNA profiling might be an important factor as miRNAs are cell-specific. Therefore, the results might be different if, for example, the assay can be explored in brain tissue [123], most likely postmortem, as is done for Alzheimer’s disease [70]. Inconsistency in results between this study and ours might also be related to different issues. For example, it could stem from technical variations or limitations in comparability due to differences in patient groups. To improve comparability, patients must be cautiously selected, profiled, and grouped so that a direct comparison could be made between studies. This point highlights the value of having a standardized analytical protocol, storage time, and quantification method for future studies including multicenter comparisons [70]. Recently, a final report became available from the same group of researchers that received funding in 2015 for the so-called microMIG study from the Migraine Research Foundation (2015 Migraine Research Foundation research grantee: Patricia Pozo Rosich) [124]. This report does not specify differentially expressed miRNAs that were found in PBMCs of EM and CM patients compared with healthy controls. However, it does note “5 significant differentially expressed miRNAs between healthy controls and all migraineurs (CM+EM), 10 between controls and CM, and 8 between controls and EM” [124]. The researchers involved in this study note that they intend to continue their study in a local and a heterogeneous international cohort.
In line with the importance of careful consideration of patient groups and clinical characteristics, a pilot study has profiled miRNA in migraine without aura [84] with the aim of identifying differentially expressed circulating miRNAs in migraine without aura. Migraine patients without aura (15 females) and matched healthy controls were profiled for their circulating miRNA expression. Several miRNAs were selected and validated by quantitative real-time polymerase chain reaction (qRT-PCR), including miR-22, miR-26a, miR-26b, miR-27b, miR-29b, let-7b, miR-181a, miR-221, miR-30b, and miR-30e [84]. The results demonstrated four differentially expressed miRNAs when patients were compared with healthy matched controls. miR-27b was significantly upregulated, and miR-181a, let-7b, and miR-22 were significantly downregulated [84]. Downregulation of miR-22 and let-7b was also found in circulating blood monocytes. Based on their findings, the authors proposed that a specific circulating miRNA profile is associated with migraine without aura. Interestingly, similar miRNAs are known to also be involved in atherosclerosis and stroke conditions in humans. Hence, the authors suggested that miRNA alteration might be an explanation for a link between migraine without aura and cardiovascular risk that was still debated [84].
The link between vascular dysfunction and migraine also attracted the interest of another group of researchers [73]. It has been reported that migraine could potentiate cardiovascular risks in affected patients. Indeed, migraine patients have been found to have a two-fold higher risk of ischemic stroke, and the higher the frequency of attacks, the higher the risk. In this regard, women and those of a younger age are more at risk than other groups [73]. A group of investigators [85] looked into circulating endothelial-specific miRNAs in migraine patients. Their hypothesis was based on reports that vascular dysfunction in migraine was remarkable. Therefore, this study explored whether circulating levels of the miRNAs that are known to be associated with endothelial function are the ones that are also altered in migraine [85]. Thirty migraine patients without vascular risk factors and sex- and age-matched healthy controls were recruited. Expression levels of miR-155, miR-126, miR-21, and let-7 g—four miRNAs that regulate endothelial function—were assessed and compared with controls. In addition, miRNA levels were tested for an association with headache characteristics and co-morbidity with syncope. The study results reported that miR-155, miR-126, and let-7 g were elevated in migraine patients and that, interestingly, miR-155 and miR-126 were also associated with syncope frequency in the past year in migraine patients. In this study, patients both with and without aura were included, and analysis presented no significant difference in expression of miRNA levels in migraine patients with aura compared with those without aura [85]. Although most results showing an association with a higher risk of cardiovascular events concern migraine with aura, studies [125, 126] also suggest an increased risk in migraine without aura.
In the pathogenesis of migraine, the origin of pain is still being debated and there is evidence of both peripheral and central origins. The literature supports the idea that the initiation of headache in migraine may involve nociceptive signals that originate in pain-sensitive intra- and extra-cranial regions, and that signals travel through peripheral nociceptors to central trigeminovascular neurons [125,126,127,128,131]. In an attempt to identify one of the extracranial sources of migraine pain [132], a group of researchers compared the number of copies of gene transcripts (mRNA) that encode proteins known to play roles in inflammatory and immune responses [133]. In addition, they looked into the number of copies of molecules that regulate the expression of those genes (miRNA) in periosteum tissue from CM patients and healthy controls [133]. This study revealed that 36 of 524 mRNAs and 27 of 726 miRNAs were differentially expressed in periosteum samples in CM patients. The results demonstrated that 25 genes were upregulated, and they encode pro-inflammatory proteins. The downregulated genes (11) were those that are involved in the anti-inflammatory process. miRNA sequences were identified and of 27 post-transcripts, 11 had low transcript levels and these regulate expression of pro-inflammatory genes; high levels were reported for the 16 that regulate expression of anti-inflammatory genes. These findings support the importance of the molecular environment (in this case, periosteal pain fiber) and the point that expression of genes that promote inflammation could potentially be linked to migraine [132, 133].
Another group of researchers looked into miR-30a and whether it can possibly relieve migraine by degrading the calcitonin/alpha-CGRP gene (CALCA) [83]. These researchers obtained blood samples from migraine patients and healthy controls to investigate both the relationship between and underlying mechanism of miR-30a and migraine. Results from this study revealed that miR-30a expression in migraine patients were significantly lower than in healthy controls and the methylation level of miR-30a in the promoter region was remarkably increased. The opposite results were observed in the expression level of CALCA, which was significantly elevated in serum samples from migraine patients. Based on the finding that identified the target gene of miR-30a, by the TargetScan, showing that CALCA can bind to mir-30a, the authors proposed that miR-30a is involved in migraine pathogenesis and that elevation of miR-30a could potentially suppress the progression of migraine through the degradation of CALCA [83].
A recent review [31] has highlighted the role of miR-590-5p in migraine. The authors noticed that miR-590-5p was a commonality among the miRNAs that are dysregulated in a human migraine attack and those that are dysregulated in mouse models of different pain conditions. In a complete Freund’s adjuvant model in mice, this particular miRNA has been modulated by celecoxib, a cyclo-oxygenase-2-selective non-steroidal anti-inflammatory drug (NSAID), when it was used to provide evidence on the utility of circulating miRNAs as biomarkers of drug response [93]. Celecoxib could reverse downregulation of mmu-miR-211, mmu-miR-411, and mmu-miR-342-5p. Another study [134] reported that mmu-miR-342-5p suppressed Akt1 and consequently induced pro-inflammatory mediators nitric oxide synthase 2 (Nos2) and interleukin (IL)-6 via upregulation of mmu-miR-155. Celecoxib also upregulated the expression of mmu-miR-1904, mmu-miR-1969, mmu-miR-196a, mmu-miR-337-5p, and mmu-miR-590-5p [93]. Interestingly, miR-590-5p in human is dysregulated in CRPS [82], which is proposed to have a link with migraine. Therefore, perturbation of miRNAs can be identified in co-morbid disorders or could have the potential to evaluate the efficacy of drugs. Based on these data, the authors proposed that miR-590-5p could be an interesting candidate with a double meaning: while it can be a biomarker of general pain, including migraine, it can also serve as a marker to evaluate relevant drug efficacy [31]. Indeed, a role for miRNAs has long been proposed in relation to drug efficacy [135]; for example, the literature shows investigations in this field for Toll-like receptors (including TLR7) and TRPA1 [136, 137]. Besides an investigation in relation to drug efficacy, miRNAs have also been reviewed for their role in therapy resistance [138]. Currently, most of the pharmacogenomics knowledge regarding miRNAs is focused on their response to chemotherapeutics for cancers; however, it would be valuable to investigate pharmacogenomic sets of miRNA–gene–drug relationships for pain and migraine. For example, a pharmacogenomic set of miRNA–monoamine oxidase A (MAOA)–cytochrome P450 (CYP) 1A2–triptans would potentially be valuable for tailoring the choice of triptan for migraine [31]. Hypothetically, each abortive or prophylactic agent for migraine could influence the pattern of miRNAs and hence it might be possible to estimate efficacy or drug resistance in patients [31]. This concept can also be tested for non-drug interventions. For example, a group of researchers observed that 6 weeks of a biphasic ketogenic diet could influence circulating miRNAs linked to energy metabolism [139]. In this study, six females reported an improvement in their migraine, and the investigators analyzed miRNAs associated with pain-migraine as well. They found that has-miR-590–5p and hsa-miR-660–3p, which are involved in cytokine signaling, were strongly affected by the ketogenic diet. The authors concluded that the diet, potentially thought to modulate miRNAs, could contribute by counteracting neuroinflammation to improve migraine pain [139]. Neurogenic inflammation has been proposed in pathogenesis of migraine [138,139,140,143] and, recently, migraine with aura has been imaged in patients to show the association of neuroimmune activation and neuroinflammation in support of a link between cortical spreading depression and glial activation [142].
The occurrence of migraine headache in children, or pediatric migraine, ranges from 3% in younger children to approximately 20% in adolescents [144]. It is disabling and can be difficult to diagnose [145] and manage [146]. Hence, finding biomarkers in the pediatric population would potentially have high value. A recent study [147] has looked into miRNAs as biomarkers of migraine in children. In this study, expression of hsa-miR-34a-5p and hsa-miR-375 in the serum and saliva of participants with migraine without aura (some of whom were on pharmacological treatments) was assessed in comparison with a healthy matched control group. The qRT-PCR method was used to determine miRNAs. In order to identify genes as target of the identified hsa-miRNAs (i.e., hsa-miR-34a-5p and hsa-miR-375), in silico analysis was performed in this study. Levels of hsa-miRs in blood and saliva were comparable based on findings from the qRT-PCR. In untreated migraine patients without aura, hsa-miR-34a-5p and hsa-miR-375 were expressed at higher levels than controls using saliva samples. In treated patients, a significant decrease of hsa-miR-34a-5p and hsa-miR-375 was evident in saliva and blood when compared with samples from untreated patients. This study had been designed based on a rationale for selection of miRNAs and used has-miR-34a-5p, which had shown increased expression in adult patients with migraine [86]. Also, hsa-miR-375 has been reported to play a role in cancer and metabolic, immune, and inflammatory diseases [148]. The concept of non-invasive collection of bio-fluid samples from special populations such as children also led the researchers in this study to collect saliva samples. Their findings presented, for the first time, elevated expression of hsa-miR-34a-5p and hsa-miR-375 in both the serum and saliva of untreated children with migraine compared with controls and treated children [147]. Findings from the comparison between drug and no-drug groups in this study also indicated a possible role of hsa-miR-34a-5p and hsa-miR-375 as biomarkers for the prediction of therapeutic response, in line with previous reports that miRNAs could be relevant as indicators of drug response [135]. Medications in this study included short-term NSAIDs and long-term magnesium [147]. In addition, this study, for the first time, presented expression of miRNAs in saliva samples that could be considered as a potential peripheral milieu for an indirect readout of migraine pathogenesis. Although this pilot study had some limitations, namely limited sample size (specifically in the control group), as also has been acknowledged by the authors, it elegantly demonstrated that hsa-miR-34a-5p and hsa-miR-375 could be considered as biomarkers of disease and drug efficacy in children with migraine without aura and that saliva could be used to monitor these biomarkers [147].
Taken together, these studies (see Table 2) highlight that investigating miRNA patterns in migraine has definitely enhanced our understanding of the pathogenesis of migraine, but has also opened up the possibility of considering these cellular markers for the diagnosis, subclassification, origin determination, identification of co-morbid conditions, and monitoring of therapeutic treatments and dietary factors in migraine.
3 Conclusion and Future Perspectives
There is no doubt that discovery of miRNAs has revolutionized our understanding of health and disease. miRNAs are proving to be useful tools in a vast range of applications in the medical field. Advancement of technology over the years has permitted higher quality and validity in profiling miRNAs, with lower expenses and in a diverse range of biomaterials. Research in miRNAs is an active field, ranging from diagnosis to treatment of a number of human diseases, including chronic pain conditions and migraine. Researchers are providing useful evidence on the value of miRNA signatures, including prediction of the ‘at-risk’ population, diagnosis, patient stratification, and follow-up of responders to treatments. Future clinical trials can use these findings, e.g., when a study is being designed or for inclusion of patients in trials, or even when data obtained from trials is being analyzed. Biomarker-based clinical trials are emerging and biomarker-based drug discovery based on CGRP has already been successful in migraine [25, 149]. Identification of the important role of miRNAs in determining drug efficacy is a highly valuable step towards precision medicine and identification of adverse events, therapeutic off-targets, and drug resistance while potentiating effective therapeutic strategies. In addition, elucidating the mechanistic significance of miRNA alterations could be an indirect marker of drug adherence for certain treatments [96]. Non-pharmacological modulation of chronic pain and migraine might also benefit from miRNA investigation, such as vagal nerve stimulation, acupuncture, and biofeedback. For example, miRNA response to acupuncture in rats with hypertension has shown promising results [150]. Studying co-morbidities of migraine, e.g., cardiovascular diseases, would also be advanced using miRNAs [73].
miR-27b has been found to be overexpressed in female migraine patients without aura [84], and miR-34a-5p and miR-382-5p have been found to have high serum levels during migraine attacks [86]. miRNAs as potential targets for treatment of atherosclerosis, diabetes, and migraine—based on studies on the effects of specific antagomir in experimental models—have been reported by Tana et al. [73], including miR-92a, miR-208a, miR-21, and miR-103/107. However, information on the therapeutic role of miRNAs, drugability of miRNAs, and modulatory effects of current abortive and prophylactic agents on miRNAs in migraine has just started to appear and more studies are required to gain further knowledge in this field. A recent mini-review has elegantly listed clinical research studies of miRNAs as medical intervention drugs for a range of conditions, including wound healing, hepatitis, liver and other cancers, and heart failure [76]. Therefore, it is not unlikely to expect a future landscape of miRNAs not only as biomarkers but also as therapeutics in pain and headaches. It is expected that human trials in the future will expand the epigenetic targets to focus on [76].
miRNAs can be extracted from almost every body tissue and bio-fluid [151]. A Human miRNA Tissue Atlas (http://www.ccb.uni-saarland.de/tissueatlas) has been created [151] that contains miRNA profiles from lung, prostate, gastric tissue, whole blood, fractioned blood cell isolates, serum, plasma, urine, and saliva. The current version of this web-based repository hosts 982 full miRNomes, which are all measured using the same microarray technology [151]. This platform is not only valuable for studying miRNA biomarkers but also presents cell or tissue specificity for some of those biomarkers [151]. The studies available for migraine have so far utilized blood-based miRNAs including serum and plasma, periosteum, and saliva. Recent literature on the use of saliva for studying biomarkers of pain [152] and miRNAs in children with migraine [147] emphasizes that salivary biomarkers might be highly relevant in migraine. miRNAs have been shown to be expressed in saliva with high stability, and therefore might be ideal biomarker candidates [31]. In healthy humans, salivary miRNA profiles measured with high-throughput sequencing has shown high reproducibility. When miRNA content was assessed in 12 human body fluids, it was demonstrated that saliva, breast milk, and seminal fluid contain the highest content. Interestingly, some of the most abundantly expressed miRNAs in saliva are found to be involved in inflammation and in the response to neuronal injury. A recent study [153] has looked into salivary miRNAs for concussion; it investigated the ability of salivary miRNAs to predict the duration and character of concussion symptoms. If salivary miRNA represents an easily measured, physiologically relevant, and objective biomarker with clinical potential in pain [152] and migraine [147], future studies would greatly benefit from integrating it into research and clinical practice. Ideally, in-office or home-based collection of saliva using a simple technique may provide a point-of-care tool that can offer individualized treatment plans [154]. Certainly, additional studies validating these results in larger cohorts are needed [147, 154] to also explore confounding variables on salivary miRNA expression, patterns of salivary miRNA in longitudinal studies, and investigate salivary miRNA patterns considering age and sex.
We may still need to know more about the tissue-specific function of miRNAs [58] and mechanisms that regulate post-transcriptional miRNA production [155]. It should also be remembered that a set of biomarkers will provide a better multidisciplinary approach towards prevention or treatment. Application of miRNAs together with neuroimaging, electrophysiology, and clinical examination, along with comprehensive patient reports, may provide a powerful tool that accurately leads to diagnosis and correct choices in treatment strategies for patients.
The available data from miRNA profiling, miRNA drug discovery, and their current status in clinical trials, and the potential for utilization of these in research and clinical practice, are highly promising, and diagnostic and interventional approaches will also continue to evolve [76]. A wide range of molecular-based tests are already available; however, alternative technologies aimed at exploring genome complexity without PCR are anticipated to gain momentum in the coming years, as sequencing devices are expected to be less expensive in the future [156]. Furthermore, development of integrated silicon chips mounted with biomolecules is going to change the concept of the traditional wet lab to that of a lab-on-a-chip [156]. The overall prediction is that miRNA-based prevention and treatment of most human diseases will have broader applications in the near future, and migraine is not an exception to this.
References
Steiner TJ, Stovner LJ, Vos T, Jensen R, Katsarava Z. Migraine is first cause of disability in under 50 s: will health politicians now take notice? J Headache Pain. 2018;19:17. https://doi.org/10.1186/s10194-018-0846-2.
Lanteri-Minet M. Economic burden and costs of chronic migraine. Curr Pain Headache Rep. 2013;18(1):385. https://doi.org/10.1007/s11916-013-0385-0.
Straube A, Andreou AP. Primary headaches during lifespan. J Headache Pain. 2019;20:71. https://doi.org/10.1186/s10194-019-1025-9.
Vetvik KG, MacGregor EA. Sex differences in the epidemiology, clinical features, and CrossMark pathophysiology of migraine. Lancet Neurol. 2017;16(1):76–87. https://doi.org/10.1016/S1474-4422(16)30293-9.
Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders, 3rd edition. Cephalalgia. 2018;38(1):1–211.
Dodick DW. Migraine. Lancet. 2018;391(10127):1315–30. https://doi.org/10.1016/S0140-6736(18)30478-1.
Russo A, Silvestro M, Tessitore A, Tedeschi G. Recent insights in migraine with aura: a narrative review of advanced neuroimaging. Headache. 2019;59(4):637–49. https://doi.org/10.1111/head.13512.
Hadjikhani N, Vincent M. Neuroimaging clues of migraine aura. J Headache Pain. 2019;20:32. https://doi.org/10.1186/s10194-019-0983-2.
Manzoni GC, Torelli P. Migraine with and without aura: a single entity? Neurol Sci. 2008;29:S40–3. https://doi.org/10.1007/s10072-008-0884-7.
Russell MB, Ulrich V, Gervil M, Olesen J. Migraine without aura and migraine with aura are distinct disorders. A population-based twin survey. Headache. 2002;42(5):332–6. https://doi.org/10.1046/j.1526-4610.2002.02102.x.
Ligthart L, Boomsma DI, Martin NG, Stubbe JH, Nyholt DR. Migraine with aura and migraine without aura are not distinct entities: further evidence from a large Dutch population study. Twin Res Hum Genet. 2006;9(1):54–63. https://doi.org/10.1375/183242706776403019.
Viana M, Linde M, Sances G, Ghiotto N, Guaschino E, Allena M, et al. Migraine aura symptoms: duration, succession and temporal relationship to headache. Cephalalgia. 2016;36(5):413–21. https://doi.org/10.1177/0333102415593089.
Viana M, Tronvik EA, Do TP, Zecca C, Hougaard A. Clinical features of visual migraine aura: a systematic review. J Headache Pain. 2019;20:64. https://doi.org/10.1186/s10194-019-1008-x.
Charles A. The pathophysiology of migraine: implications for clinical management. Lancet Neurol. 2018;17(2):174–82. https://doi.org/10.1016/S1474-4422(17)30435-0.
Sutherland HG, Albury CL, Griffiths LR. Advances in genetics of migraine. J Headache Pain. 2019;20:72. https://doi.org/10.1186/s10194-019-1017-9.
Kondratieva N, Azimova J, Skorobogatykh K, Sergeev A, Naumova E, Kokaeva Z, et al. Biomarkers of migraine: part 1 - genetic markers. J Neurol Sci. 2016;369:63–76. https://doi.org/10.1016/j.jns.2016.08.008.
Gazerani P. Current evidence on the role of epigenetic mechanisms in migraine: the way forward to precision medicine. OBM Genet. 2018;2(4):040. https://doi.org/10.21926/obm.genet.1804040.
Eising E, Datson NA, van den Maagdenberg AMJM, Ferrari MD. Epigenetic mechanisms in migraine: a promising avenue? BMC Med. 2013;11:26. https://doi.org/10.1186/1741-7015-11-26.
Terlizzi R, Bacalini MG, Pirazzini C, Giannini G, Pierangeli G, Garagnani P, et al. Epigenetic DNA methylation changes in episodic and chronic migraine. Neurol Sci. 2018;39:S67–8. https://doi.org/10.1007/s10072-018-3348-8.
Lipton RB, Silberstein SD. Episodic and chronic migraine headache: breaking down barriers to optimal treatment and prevention. Headache. 2015;55 Suppl 2:103–22 (quiz 23–6). https://doi.org/10.1111/head.12505_2.
Katsarava Z, Buse DC, Manack AN, Lipton RB. Defining the differences between episodic migraine and chronic migraine. Curr Pain Headache Rep. 2012;16(1):86–92. https://doi.org/10.1007/s11916-011-0233-z.
Zhang LM, Dong Z, Yu SY. Migraine in the era of precision medicine. Ann Transl Med. 2016;4(6):105. https://doi.org/10.21037/atm.2016.03.13.
Antonaci F, Ghiotto N, Wu SZ, Pucci E, Costa A. Recent advances in migraine therapy. Springerplus. 2016;5:637. https://doi.org/10.1186/s40064-016-2211-8.
Gooriah R, Nimeri R, Ahmed F. Evidence-based treatments for adults with migraine. Pain Res Treat. 2015;2015:629382. https://doi.org/10.1155/2015/629382.
Scuteri D, Adornetto A, Rombola L, Naturale MD, Morrone LA, Bagetta G, et al. New trends in migraine pharmacology: targeting calcitonin gene-related peptide (CGRP) with monoclonal antibodies. Front Pharmacol. 2019;10:363. https://doi.org/10.3389/fphar.2019.00363.
Tringali G, Navarra P. Anti-CGRP and anti-CGRP receptor monoclonal antibodies as antimigraine agents. Potential differences in safety profile postulated on a pathophysiological basis. Peptides. 2019;116:16–21. https://doi.org/10.1016/j.peptides.2019.04.012.
Tepper SJ. History and review of anti-calcitonin gene-related peptide (CGRP) therapies: from translational research to treatment. Headache. 2018;58:238–75. https://doi.org/10.1111/head.13379.
Lipton RB, Croop R, Stock EG, Stock DA, Morris BA, Frost M, et al. Rimegepant, an oral calcitonin gene-related peptide receptor antagonist, for migraine. N Engl J Med. 2019;381(2):142–9. https://doi.org/10.1056/NEJMoa1811090.
Moreno-Ajona D, Chan C, Villar-Martinez MD, Goadsby PJ. Targeting CGRP and 5-HT1F receptors for the acute therapy of migraine: a literature review. Headache. 2019;59(Suppl 2):3–19. https://doi.org/10.1111/head.13582.
Negro A, Martelletti P. Gepants for the treatment of migraine. Expert Opin Investig Drugs. 2019;28(6):555–67. https://doi.org/10.1080/13543784.2019.1618830.
Gallelli L, Cione E, Caroleo MC, Carotenuto M, Lagana P, Siniscalchi A, et al. microRNAs to monitor pain-migraine and drug treatment. Microrna. 2017;6(3):152–6. https://doi.org/10.2174/2211536606666170913152821.
Borsook D, Becerra L, Hargreaves R. Biomarkers for chronic pain and analgesia. Part 1: the need, reality, challenges, and solutions. Discov Med. 2011;11(58):197–207.
Borsook D, Becerra L, Hargreaves R. Biomarkers for chronic pain and analgesia. Part 2: how, where, and what to look for using functional imaging. Discov Med. 2011;11(58):209–19.
Durham P, Papapetropoulos S. Biomarkers associated with migraine and their potential role in migraine management. Headache. 2013;53(8):1262–77. https://doi.org/10.1111/head.12174.
Loder E, Graham JR. From subjective to objective: biomarkers in migraine. Headache. 2006;46(7):1045. https://doi.org/10.1111/j.1526-4610.2006.00497.x.
Kowalska M, Prendecki M, Kozubski W, Lianeri M, Dorszewska J. Molecular factors in migraine. Oncotarget. 2016;7(31):50708–18. https://doi.org/10.18632/oncotarget.9367.
Kowalska M, Kapelusiak-Pielok M, Grzelak T, Wypasek E, Kozubski W, Dorszewska J. The new *G29A and G1222A of HCRTR1, 5-HTTLPR of SLC6A4 Polymorphisms and hypocretin-1, serotonin concentrations in migraine patients. Front Mol Neurosci. 2018;11:191. https://doi.org/10.3389/fnmol.2018.00191.
Loder E, Rizzoli P. Biomarkers in migraine: their promise, problems, and practical applications. Headache. 2006;46(7):1046–58. https://doi.org/10.1111/j.1526-4610.2006.00498.x.
Loder E, Harrington MG, Cutrer M, Sandor P, De Vries B. Selected confirmed, probable, and exploratory migraine biomarkers. Headache. 2006;46(7):1108–27. https://doi.org/10.1111/j.1526-4610.2006.00525.x.
Califf RM. Biomarker definitions and their applications. Exp Biol Med. 2018;243(3):213–21. https://doi.org/10.1177/1535370217750088.
Neuroscience biomarkers and biosignatures: converging technologies, emerging partnerships, workshop summary. The National Academies Collection: reports funded by National Institutes of Health. Washington, DC: The National Academies Press; 2008.
Belvís R, Pozo-Rosich P, Pascual J. New insights into diagnostic biomarkers of migraine: biological, genetic and radiological. Int J Neuro Disord Interv. 2015;1:105. https://doi.org/10.15344/ijndi/2015/105.
Drucker E, Krapfenbauer K. Pitfalls and limitations in translation from biomarker discovery to clinical utility in predictive and personalised medicine. EPMA J. 2013;4(1):7. https://doi.org/10.1186/1878-5085-4-7.
Mayeux R. Biomarkers: potential uses and limitations. NeuroRx. 2004;1(2):182–8. https://doi.org/10.1602/neurorx.1.2.182.
Casteleyn L, Dumez B, Van Damme K, Anwar WA. Ethics and data protection in human biomarker studies in environmental health. Int J Hyg Envir Heal. 2013;216(5):599–605. https://doi.org/10.1016/j.ijheh.2013.03.016.
Coppola L, Cianflone A, Grimaldi AM, Incoronato M, Bevilacqua P, Messina F, et al. Biobanking in health care: evolution and future directions. J Transl Med. 2019;17:172. https://doi.org/10.1186/s12967-019-1922-3.
Kuzhandai Velu V, Ramesh R, Srinivasan AR. Circulating MicroRNAs as biomarkers in health and disease. J Clin Diagn Res. 2012;6(10):1791–5. https://doi.org/10.7860/JCDR/2012/4901.2653.
Esteller M. Non-coding RNAs in human disease. Nat Rev Genet. 2011;12(12):861–74. https://doi.org/10.1038/nrg3074.
Backes C, Meese E, Keller A. Specific miRNA disease biomarkers in blood, serum and plasma: challenges and prospects. Mol Diagn Ther. 2016;20(6):509–18. https://doi.org/10.1007/s40291-016-0221-4.
Trzybulska D, Vergadi E, Tsatsanis C. miRNA and other non-coding RNAs as promising diagnostic markers. EJIFCC. 2018;29(3):221–6.
Wei JW, Huang K, Yang C, Kang CS. Non-coding RNAs as regulators in epigenetics. Oncol Rep. 2017;37(1):3–9. https://doi.org/10.3892/or.2016.5236.
Camara MS, Martin Bujanda M, Mendioroz Iriarte M. Epigenetic changes in headache. Neurologia Epub. 2017. https://doi.org/10.1016/j.nrl.2017.10.010.
Kreth S, Hubner M, Hinske LC. MicroRNAs as clinical biomarkers and therapeutic tools in perioperative medicine. Anesth Analg. 2018;126(2):670–81. https://doi.org/10.1213/Ane.0000000000002444.
Lim LP, Lau NC, Weinstein EG, Abdelhakim A, Yekta S, Rhoades MW, et al. The microRNAs of Caenorhabditis elegans. Gene Dev. 2003;17(8):991–1008. https://doi.org/10.1101/gad.1074403.
O’Brien J, Hayder H, Zayed Y, Peng C. Overview of MicroRNA biogenesis, mechanisms of actions, and circulation. Front Endocrinol. 2018;9:402. https://doi.org/10.3389/fendo.2018.00402.
Coenen-Stass AML, Magen I, Brooks T, Ben-Dov IZ, Greensmith L, Hornstein E, et al. Evaluation of methodologies for microRNA biomarker detection by next generation sequencing. RNA Biol. 2018;15(8):1133–45. https://doi.org/10.1080/15476286.2018.1514236.
Li Y, Kowdley KV. MicroRNAs in common human diseases. Genom Proteom Bioinform. 2012;10(5):246–53. https://doi.org/10.1016/j.gpb.2012.07.005.
Kandhro AH. MicroRNAs from diagnosis to therapy: future perspective. Transl Biomed. 2016. https://doi.org/10.2167/2172-0479.100089.
Lewis BP, Burge CB, Bartel DP. Conserved seed pairing, often flanked by adenosines, indicates that thousands of human genes are microRNA targets. Cell. 2005;120(1):15–20. https://doi.org/10.1016/j.cell.2004.12.035.
Kozomara A, Birgaoanu M, Griffiths-Jones S. miRBase: from microRNA sequences to function. Nucleic Acids Res. 2019;47(D1):D155–62. https://doi.org/10.1093/nar/gky1141.
Alles J, Fehlmann T, Fischer U, Backes C, Galata V, Minet M, et al. An estimate of the total number of true human miRNAs. Nucleic Acids Res. 2019;47(7):3353–64. https://doi.org/10.1093/nar/gkz097.
Bartel DP. MicroRNAs: target recognition and regulatory functions. Cell. 2009;136(2):215–33. https://doi.org/10.1016/j.cell.2009.01.002.
Bartel DP. MicroRNAs: genomics, biogenesis, mechanism, and function. Cell. 2004;116(2):281–97. https://doi.org/10.1016/S0092-8674(04)00045-5.
Ling H, Fabbri M, Calin GA. MicroRNAs and other non-coding RNAs as targets for anticancer drug development. Nat Rev Drug Discov. 2013;12(11):847–65. https://doi.org/10.1038/nrd4140.
Osman A. MicroRNAs in health and disease—basic science and clinical applications. Clin Lab. 2012;58(5–6):393–402.
Ardekani AM, Naeini MM. The role of microRNAs in human diseases. Avicenna J Med Biotechnol. 2010;2(4):161–79.
Tufekci KU, Oner MG, Meuwissen RL, Genc S. The role of microRNAs in human diseases. Methods Mol Biol. 2014;1107:33–50. https://doi.org/10.1007/978-1-62703-748-8_3.
Treiber T, Treiber N, Meister G. Author correction: regulation of microRNA biogenesis and its crosstalk with other cellular pathways. Nat Rev Mol Cell Biol. 2018;19(12):808. https://doi.org/10.1038/s41580-018-0070-6.
Ma YH. The challenge of microRNA as a biomarker of epilepsy. Curr Neuropharmacol. 2018;16(1):37–42. https://doi.org/10.2174/1570159x15666170703102410.
Swarbrick S, Wragg N, Ghosh S, Stolzing A. Systematic review of miRNA as biomarkers in Alzheimer’s disease. Mol Neurobiol. 2019;56(9):6156–67. https://doi.org/10.1007/s12035-019-1500-y.
Zhou SS, Jin JP, Wang JQ, Zhang ZG, Freedman JH, Zheng Y, et al. miRNAS in cardiovascular diseases: potential biomarkers, therapeutic targets and challenges. Acta Pharmacol Sin. 2018;39(7):1073–84. https://doi.org/10.1038/aps.2018.30.
Ojha R, Nandani R, Pandey RK, Mishra A, Prajapati VK. Emerging role of circulating microRNA in the diagnosis of human infectious diseases. J Cell Physiol. 2019;234(2):1030–43. https://doi.org/10.1002/jcp.27127.
Tana C, Giamberardino MA, Cipollone F. microRNA profiling in atherosclerosis, diabetes, and migraine. Ann Med. 2017;49(2):93–105. https://doi.org/10.1080/07853890.2016.1226515.
Slota JA, Booth SA. MicroRNAs in Neuroinflammation: implications in disease pathogenesis, biomarker discovery and therapeutic applications. Noncoding RNA. 2019;5(2):E35. https://doi.org/10.3390/ncrna5020035.
Gambari R, Fabbri E, Borgatti M, Lampronti I, Finotti A, Brognara E, et al. Targeting microRNAs involved in human diseases: a novel approach for modification of gene expression and drug development. Biochem Pharmacol. 2011;82(10):1416–29. https://doi.org/10.1016/j.bcp.2011.08.007.
Hanna J, Hossain GS, Kocerha J. The potential for microRNA therapeutics and clinical research. Front Genet. 2019;10:478. https://doi.org/10.3389/fgene.2019.00478.
Lopez-Gonzalez MJ, Landry M, Favereaux A. MicroRNA and chronic pain: from mechanisms to therapeutic potential. Pharmacol Ther. 2017;180:1–15. https://doi.org/10.1016/j.pharmthera.2017.06.001.
Andersen HH, Duroux M, Gazerani P. MicroRNAs as modulators and biomarkers of inflammatory and neuropathic pain conditions. Neurobiol Dis. 2014;71:159–68. https://doi.org/10.1016/j.nbd.2014.08.003.
Dayer CF, Luthi F, Le Carre J, Vuistiner P, Terrier P, Benaim C, et al. Differences in the miRNA signatures of chronic musculoskeletal pain patients from neuropathic or nociceptive origins. PLoS One. 2019;14(7):e0219311. https://doi.org/10.1371/journal.pone.0219311.
Ramanathan S, Ajit SK. MicroRNA-based biomarkers in pain. Adv Pharmacol. 2016;75:35–62. https://doi.org/10.1016/bs.apha.2015.12.001.
McDonald MK, Ajit SK. MicroRNA biology and pain. Prog Mol Biol Transl Sci. 2015;131:215–49. https://doi.org/10.1016/bs.pmbts.2014.11.015.
Orlova IA, Alexander GM, Qureshi RA, Sacan A, Graziano A, Barrett JE, et al. MicroRNA modulation in complex regional pain syndrome. J Transl Med. 2011;9:195. https://doi.org/10.1186/1479-5876-9-195.
Zhai Y, Zhu YY. MiR-30a relieves migraine by degrading CALCA. Eur Rev Med Pharmacol Sci. 2018;22(7):2022–8.
Tafuri E, Santovito D, de Nardis V, Marcantonio P, Paganelli C, Affaitati G, et al. MicroRNA profiling in migraine without aura: pilot study. Ann Med. 2015;47(6):468–73. https://doi.org/10.3109/07853890.2015.1071871.
Cheng CY, Chen SP, Liao YC, Fuh JL, Wang YF, Wang SJ. Elevated circulating endothelial-specific microRNAs in migraine patients: a pilot study. Cephalalgia. 2018;38(9):1585–91. https://doi.org/10.1177/0333102417742375.
Andersen HH, Duroux M, Gazerani P. Serum microRNA signatures in migraineurs during attacks and in pain-free periods. Mol Neurobiol. 2016;53(3):1494–500. https://doi.org/10.1007/s12035-015-9106-5.
Sakai A, Suzuki H. microRNA and pain. Adv Exp Med Biol. 2015;888:17–39. https://doi.org/10.1007/978-3-319-22671-2_3.
Sakai A, Suzuki H. Emerging roles of microRNAs in chronic pain. Neurochem Int. 2014;77:58–67. https://doi.org/10.1016/j.neuint.2014.05.010.
Odell DW. Epigenetics of pain mediators. Curr Opin Anesthesiol. 2018;31(4):402–6. https://doi.org/10.1097/Aco.0000000000000613.
Andersen HH, Gazerani P. MicroRNAs and pain. In: Ruberti F, editor. Mapping of nervous system diseases via MicroRNAs. Frontiers in neurotherapeutics series. Boca Raton: CRC; 2016. p. 181–202.
Kress M, Huttenhofer A, Landry M, Kuner R, Favereaux A, Greenberg D, et al. microRNAs in nociceptive circuits as predictors of future clinical applications. Front Mol Neurosci. 2013;6:33. https://doi.org/10.3389/fnmol.2013.00033.
Lutz BM, Bekker A, Tao YX. Noncoding RNAs new players in chronic pain. Anesthesiology. 2014;121(2):409–17. https://doi.org/10.1097/Aln.0000000000000265.
Qureshi RA, Tian Y, McDonald MK, Capasso KE, Douglas SR, Gao R, et al. Circulating microRNA signatures in rodent models of pain. Mol Neurobiol. 2016;53(5):3416–27. https://doi.org/10.1007/s12035-015-9281-4.
Guo JB, Zhu Y, Chen BL, Song G, Peng MS, Hu HY, et al. Network and pathway-based analysis of microRNA role in neuropathic pain in rat models. J Cell Mol Med. 2019;23(7):4534–44. https://doi.org/10.1111/jcmm.14357.
Dai Z, Chu HC, Ma JH, Yan Y, Zhang XY, Liang YX. The regulatory mechanisms and therapeutic potential of microRNAs: from chronic pain to morphine tolerance. Front Mol Neurosci. 2018;11:80. https://doi.org/10.3389/fnmol.2018.00080.
Ramanathan S, Shenoda BB, Ajit SK. Overview of microRNA modulation in analgesic research. Curr Protoc Pharmacol. 2017;79:9.25.1–9.25.10. https://doi.org/10.1002/cpph.29.
Toyama K, Kiyosawa N, Watanabe K, Ishizuka H. Identification of circulating miRNAs differentially regulated by opioid treatment. Int J Mol Sci. 2017;18(9):E1991. https://doi.org/10.3390/ijms18091991.
Kiyosawa N, Watanabe K, Toyama K, Ishizuka H. Circulating miRNA signature as a potential biomarker for the prediction of analgesic efficacy of hydromorphone. Int J Mol Sci. 2019;20(7):1665. https://doi.org/10.3390/ijms20071665.
Kynast KL, Russe OQ, Geisslinger G, Niederberger E. Novel findings in pain processing pathways: implications for miRNAs as future therapeutic targets. Expert Rev Neurother. 2013;13(5):515–25. https://doi.org/10.1586/Ern.13.34.
Niederberger E, Resch E, Parnham MJ, Geisslinger G. Drugging the pain epigenome. Nat Rev Neurol. 2017;13(7):434–47. https://doi.org/10.1038/nrneurol.2017.68.
Andersen HH, Duroux M, Gazerani P. MicroRNAs as modulators and biomarkers of inlammatory and neuropathic pain conditions. Neurobiol Dis. 2014;71:159–68. https://doi.org/10.1016/j.nbd.2014.08.003
Bjersing JL, Lundborg C, Bokarewa MI, Mannerkorpi K. Profile of cerebrospinal microRNAs in fibromyalgia. PLoS ONE. 2013;8(10):e78762. https://doi.org/10.1371/journal.pone.0078762.
Zhou Q, Souba WW, Croce CM, Verne GN. MicroRNA-29a regulates intestinal membrane permeability in patients with irritable bowel syndrome. Gut. 2010;59(6):775–84. https://doi.org/10.1136/gut.2009.181834.
Wang WT, Zhao YN, Han BW, Hong SJ, Chen YQ. Circulating microRNAs identified in a genome-wide serum microRNA expression analysis as noninvasive biomarkers for endometriosis. J Clin Endocrinol Metab. 2013;98(1):281–9. https://doi.org/10.1210/jc.2012-2415.
Beyer C, Zampetaki A, Lin NY, Kleyer A, Perricone C, Iagnocco A, et al. Signature of circulating microRNAs in osteoarthritis. Ann Rheum Dis. 2015;74(3):e18. https://doi.org/10.1136/annrheumdis-2013-204698.
Tao ZY, Xue Y, Li JF, Traub RJ, Cao DY. Do microRNAs modulate visceral pain? Biomed Res Int. 2018;2018:5406973. https://doi.org/10.1155/2018/5406973.
Birklein F, Ajit SK, Goebel A, Perez R, Sommer C. Complex regional pain syndrome—phenotypic characteristics and potential biomarkers. Nat Rev Neurol. 2018;14(5):272–84. https://doi.org/10.1038/nrneurol.2018.20.
Bjorkman S, Taylor HS. MicroRNAs in endometriosis: biological function and emerging biomarker candidatesdagger. Biol Reprod. 2019;100(5):1135–46. https://doi.org/10.1093/biolre/ioz014.
Filkova M, Jungel A, Gay RE, Gay S. MicroRNAs in rheumatoid arthritis: potential role in diagnosis and therapy. BioDrugs. 2012;26(3):131–41. https://doi.org/10.2165/11631480-000000000-00000.
Chavan SS, Pavlov VA, Tracey KJ. Mechanisms and therapeutic relevance of neuro-immune communication. Immunity. 2017;46(6):927–42. https://doi.org/10.1016/j.immuni.2017.06.008.
Ciszek BP, Khan AA, Dang H, Slade GD, Smith S, Bair E, et al. MicroRNA expression profiles differentiate chronic pain condition subtypes. Transl Res. 2015;166(6):706–20. https://doi.org/10.1016/j.trsl.2015.06.008.
Hwang CK, Wagley Y, Law PY, Wei LN, Loh HH. MicroRNAs in opioid pharmacology. J Neuroimmune Pharmacol. 2012;7(4):808–19. https://doi.org/10.1007/s11481-011-9323-2.
Li MP, Hu YD, Hu XL, Zhang YJ, Yang YL, Jiang C, et al. miRNAs and miRNA polymorphisms modify drug response. Int J Environ Res Public Health. 2016;13(11):E1096. https://doi.org/10.3390/ijerph13111096.
Willemen HLDM, Huo XJ, Mao-Ying QL, Zijlstra J, Heijnen CJ, Kavelaars A. MicroRNA-124 as a novel treatment for persistent hyperalgesia. J Neuroinflamm. 2012;9:143. https://doi.org/10.1186/1742-2094-9-143.
Baumann V, Winkler J. miRNA-based therapies: strategies and delivery platforms for oligonucleotide and non-oligonucleotide agents. Future Med Chem. 2014;6(17):1967–84. https://doi.org/10.4155/fmc.14.116.
Ebert MS, Neilson JR, Sharp PA. MicroRNA sponges: competitive inhibitors of small RNAs in mammalian cells. Nat Methods. 2007;4(9):721–6. https://doi.org/10.1038/nmeth1079.
Bors LA, Erdo F. Overcoming the blood-brain barrier. Challenges and tricks for CNS drug delivery. Sci Pharm. 2019;87(1):6. https://doi.org/10.3390/scipharm87010006.
Wen MM. Getting miRNA therapeutics into the target cells for neurodegenerative diseases: a mini-review. Front Mol Neurosci. 2016;9:129. https://doi.org/10.3389/fnmol.2016.00129.
Simion V, Nadim WD, Benedetti H, Pichon C, Morisset-Lopez S, Baril P. Pharmacomodulation of microRNA expression in neurocognitive diseases: obstacles and future opportunities. Curr Neuropharmacol. 2017;15(2):276–90. https://doi.org/10.2174/1570159x14666160630210422.
Christopher AF, Kaur RP, Kaur G, Kaur A, Gupta V, Bansal P. MicroRNA therapeutics: discovering novel targets and developing specific therapy. Perspect Clin Res. 2016;7(2):68–74. https://doi.org/10.4103/2229-3485.179431.
Luchting B, Heyn J, Hinske LC, Azad SC. Expression of miRNA-124a in CD4 cells reflects response to a multidisciplinary treatment program in patients with chronic low back pain. Spine (Phila Pa 1976). 2017;42(4):E226–E33. https://doi.org/10.1097/BRS.0000000000001763.
Andersen HH, Gazerani P, Duroux M. EHMTI-0122. Serum micrornas as potential biomarkers of migraine. J Headache Pain. 2014;15(Suppl 1):F1.
Vila-Pueyo M, Fernandez-Morales J, Torres-Ferrus M, Alvarez-Sabin J, Pozo-Rosich P. Lack of differences in microrna expression profiles of blood cells in migraine [abstract no. EHMTI-0361]. J Headache Pain. 2014;15:H3. https://doi.org/10.1186/1129-2377-15-S1-H3.
Migraine Research Foundation. Final report: microRNA Expression Profile in Migraine: the microMIG study. New York: Migraine Research Foundation; 2019. https://migraineresearchfoundation.org/researchers/patricia-pozo-rosich-md-phd/. Accessed 24 Sep 2019.
Tana C, Santilli F, Martelletti P, di Vincenzo A, Cipollone F, Davi G, et al. Correlation between migraine severity and cholesterol levels. Pain Pract. 2015;15(7):662–70. https://doi.org/10.1111/papr.12229.
Tana C, Tafuri E, Tana M, Martelletti P, Negro A, Affaitati G, et al. New insights into the cardiovascular risk of migraine and the role of white matter hyperintensities: is gold all that glitters? J Headache Pain. 2013;14:9. https://doi.org/10.1186/1129-2377-14-9.
Varma A, Jain S, Majid A, De Felice M. Central and peripheral processes in headache. Curr Opin Support Pa. 2018;12(2):142–7. https://doi.org/10.1097/Spc.0000000000000336.
Olesen J, Burstein R, Ashina M, Tfelt-Hansen P. Origin of pain in migraine: evidence for peripheral sensitisation. Lancet Neurol. 2009;8(7):679–90. https://doi.org/10.1016/S1474-4422(09)70090-0.
Panerai AE. Is migraine a disorder of the central nervous system? Neurol Sci. 2013;34(1):S33–5. https://doi.org/10.1007/s10072-013-1363-3.
Goadsby PJ, Holland PR, Martins-Oliveira M, Hoffmann J, Schankin C, Akerman S. Pathophysiology of migraine: a disorder of sensory processing. Physiol Rev. 2017;97(2):553–622. https://doi.org/10.1152/physrev.00034.2015.
Peng KP, May A. Migraine understood as a sensory threshold disease. Pain. 2019;160(7):1494–501. https://doi.org/10.1097/j.pain.0000000000001531.
Perry CJ, Blake P, Buettner C, Papavassiliou E, Schain AJ, Bhasin MK, et al. Upregulation of inflammatory gene transcripts in periosteum of chronic migraineurs: implications for extracranial origin of headache. Ann Neurol. 2016;79(6):1000–13. https://doi.org/10.1002/ana.24665.
Burstein R, Perry C, Blake P, Buettner C, Bhasin M. Abnormal expression of gene transcripts linked to inflammatory response in the periosteum of chronic migraine patients: implications to extracranial origin of headache [abstract no. EHMTI-0354]. J Headache Pain. 2014;15:K2. https://doi.org/10.1186/1129-2377-15-S1-K2.
Wei Y, Nazari-Jahantigh M, Chan L, Zhu M, Heyll K, Corbalan-Campos J, et al. The microRNA-342-5p fosters inflammatory macrophage activation through an Akt1- and microRNA-155-dependent pathway during atherosclerosis. Circulation. 2013;127(15):1609–19. https://doi.org/10.1161/CIRCULATIONAHA.112.000736.
Rukov JL, Vinther J, Shomron N. Pharmacogenomics genes show varying perceptibility to microRNA regulation. Pharmacogenet Genom. 2011;21(5):251–62. https://doi.org/10.1097/FPC.0b013e3283438865.
Fabbri M, Paone A, Calore F, Galli R, Croce CM. A new role for microRNAs, as ligands of Toll-like receptors. RNA Biol. 2013;10(2):169–74. https://doi.org/10.4161/rna.23144.
Park CK, Xu ZZ, Berta T, Han QJ, Chen G, Liu XJ, et al. Extracellular microRNAs activate nociceptor neurons to elicit pain via TLR7 and TRPA1. Neuron. 2014;82(1):47–54. https://doi.org/10.1016/j.neuron.2014.02.011.
Fatima F, Nawaz M. Vesiculated long non-coding RNAs: offshore packages deciphering trans-regulation between cells, cancer progression and resistance to therapies. Noncoding RNA. 2017;3(1). https://doi.org/10.3390/ncrna3010010.
Cannataro R, Perri M, Caroleo MC, Gallelli L, Sarro G, Cione E. Modulation of microRNAs linked to pain-migraine by ketogenic diet [abstract no. P14-007-19]. Curr Dev Nutr. 2019;3(Suppl 1):nzz052.P14-007-19. https://doi.org/10.1093/cdn/nzz052.P14-007-19.
Malhotra R. Understanding migraine: potential role of neurogenic inflammation. Ann Indian Acad Neurol. 2016;19(2):175–82. https://doi.org/10.4103/0972-2327.182302.
Ramachandran R. Neurogenic inflammation and its role in migraine. Semin Immunopathol. 2018;40(3):301–14. https://doi.org/10.1007/s00281-018-0676-y.
Albrecht DS, Mainero C, Ichijo E, Ward N, Granziera C, Zurcher NR, et al. Imaging of neuroinflammation in migraine with aura: a [(11)C]PBR28 PET/MRI study. Neurology. 2019;92(17):e2038–50. https://doi.org/10.1212/WNL.0000000000007371.
Spierings EL. Spreading depression, neurogenic inflammation, and the parallel theory of migraine pathogenesis. Headache. 2001;41(9):911–3.
Lewis DW. Pediatric migraine. Neurol Clin. 2009;27(2):481–501. https://doi.org/10.1016/j.ncl.2008.11.003.
Torriero R, Capuano A, Mariani R, Frusciante R, Tarantino S, Papetti L, et al. Diagnosis of primary headache in children younger than 6 years: a clinical challenge. Cephalalgia. 2017;37(10):947–54. https://doi.org/10.1177/0333102416660533.
Papetti L, Ursitti F, Moavero R, Ferilli MAN, Sforza G, Tarantino S, et al. prophylactic treatment of pediatric migraine: is there anything new in the last decade? Front Neurol. 2019;10:771. https://doi.org/10.3389/fneur.2019.00771.
Gallelli L, Cione E, Peltrone F, Siviglia S, Verano A, Chirchiglia D, et al. Hsa-miR-34a-5p and hsa-miR-375 as biomarkers for monitoring the effects of drug treatment for migraine pain in children and adolescents: a pilot study. J Clin Med. 2019;8(7):928. https://doi.org/10.3390/jcm8070928.
Chen XH, Li BX, Luo RC, Cai SN, Zhang C, Cao XL. Analysis of the function of microRNA-375 in humans using bioinformatics. Biomed Rep. 2017;6(5):561–6. https://doi.org/10.3892/br.2017.889.
Ferroni P, Barbanti P, Spila A, Fratangeli F, Aurilia C, Fofi L, et al. Circulating biomarkers in migraine. New opportunities for precision medicine. Curr Med Chem. Epub 2018 Jun 22. https://doi.org/10.2174/0929867325666180622122938.
Wang JY, Li H, Ma CM, Wang JL, Lai XS, Zhou SF. MicroRNA profiling response to acupuncture therapy in spontaneously hypertensive rats. Evid Based Compl Alternat Med. 2015;2015:204367. https://doi.org/10.1155/2015/204367.
Fehlmann T, Ludwig N, Backes C, Meese E, Keller A. Distribution of microRNA biomarker candidates in solid tissues and body fluids. RNA Biol. 2016;13(11):1084–8. https://doi.org/10.1080/15476286.2016.1234658.
Jasim H, Carlsson A, Hedenberg-Magnusson B, Ghafouri B, Ernberg M. Saliva as a medium to detect and measure biomarkers related to pain. Sci Rep. 2018;8:3220. https://doi.org/10.1038/s41598-018-21131-4.
Johnson JJ, Loeffert AC, Stokes J, Olympia RP, Bramley H, Hicks SD. Association of salivary microRNA changes with prolonged concussion symptoms. JAMA Pediatr. 2018;172(1):65–73. https://doi.org/10.1001/jamapediatrics.2017.3884.
Hicks SD. Saliva: a new tool for concussion diagnosis? NeurologyTimes. 2018. https://www.neurologytimes.com/tbi/saliva-new-tool-concussion-diagnosis. Accessed 20 Jul 2019.
Michlewski G, Caceres JF. Post-transcriptional control of miRNA biogenesis. RNA. 2019;25(1):1–16. https://doi.org/10.1261/rna.068692.118.
Dwivedi S, Purohit P, Misra R, Pareek P, Goel A, Khattri S, et al. Diseases and molecular diagnostics: a step closer to precision medicine. Indian J Clin Biochem. 2017;32(4):374–98. https://doi.org/10.1007/s12291-017-0688-8.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Parisa Gazerani is the head of research at EMProS bio, and the scientific consultant for BalancAir, both of which are companies that focus their interest on migraine.
Funding
The author has no funding to report in relation to this article.
Rights and permissions
About this article

Cite this article
Gazerani, P. Current Evidence on Potential Uses of MicroRNA Biomarkers for Migraine: From Diagnosis to Treatment. Mol Diagn Ther 23, 681–694 (2019). https://doi.org/10.1007/s40291-019-00428-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40291-019-00428-8