
Abstract
Injuries have a detrimental impact on team and individual athletic performance. Deficits in maximal strength, rate of force development (RFD), and reactive strength are commonly reported following several musculoskeletal injuries. This article first examines the available literature to identify common deficits in fundamental physical qualities following injury, specifically strength, rate of force development and reactive strength. Secondly, evidence-based strategies to target a resolution of these residual deficits will be discussed to reduce the risk of future injury. Examples to enhance practical application and training programmes have also been provided to show how these can be addressed.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Residual deficits in maximal strength, rate of force development and reactive strength are documented following musculoskeletal injury. |
Targeting these residual deficits following injury can reduce the risk of future injury as a means of tertiary prevention. |
Rehabilitation should prepare athletic populations to tolerate loads and velocities across the full spectrum of the force–velocity curve and this is essential for returning injured athletes to high performance levels. |
1 Introduction
Injuries have a detrimental impact on team and individual athletic performance, with increased player availability improving the chances of success [1]. The available data suggest an interaction between injury, performance, physical outputs, and success at both team and individual levels [2,3,4]. It seems logical that all staff involved should strive to work together in an interdisciplinary fashion to prevent injuries and to improve performance. Furthermore, several studies have reported that a previous injury may increase the risk for subsequent injuries [5,6,7,8,9,10]. This raises the question of whether persistent deficits have been fully assessed and targeted before athletes return to play (RTP), and if a greater emphasis should be placed on a return to performance strategy as a means of tertiary prevention [11].
Following the occurrence of injury or pain onset, deficits in strength [12,13,14,15,16], strength ratios [17], rate of force development [18,19,20,21,22,23], reactive strength [24,25,26], leg stiffness [27,28,29,30,31], and peak power [32,33,34], have all been shown in athletic populations. Equally, these same attributes are widely considered important physical performance determinants in high-performance sport [35, 36]. In spite of this, rehabilitation programmes often adopted in research and clinical practice are mainly focused on restoring strength [37,38,39,40], which by definition, consists of high forces at low velocities. However, this alone may not fully prepare the musculoskeletal system to accept and produce moderate to high loads at rapid velocities, which underpin most sporting actions. Furthermore, maximal strength and ballistic power training (which is typically advocated for the latter) induce different physiological adaptations. There is, however, a strong interplay and overlap in both performance and physiological determinants between maximal strength development and ballistic power training. Maximal strength serves as the foundation for the expression of high power outputs, making the adoption of training with heavy loads advantageous, not only for relatively weaker athletes, but also for improving physiological features necessary for high-velocity actions [41, 42]. Strength training with heavy loads (i.e. ≥ 80% one repetition maximum (1RM)) increases neural drive, intermuscular coordination, myofibrillar cross-sectional area (CSA) of Type II fibres, lean muscle mass, and pennation angle [43, 44]. Ballistic power training is more specific in increasing maximal power output, rate of force development (RFD), movement velocity, jump height and sprint performance via lowered motor unit recruitment thresholds, improved motor unit firing frequency, and synchronisation, as well as enhanced intermuscular coordination [43, 45]. These positive physiological and performance changes are relevant from both a rehabilitative as well as performance perspective and should lead towards a unified vision that encompasses robustness and resilience for enhanced performance and reduced risk of re-/subsequent injury.
This article will examine the available literature pertaining to strength and power development to provide a theoretical framework, from which, clear strategies are developed to indicate how these principles and training modes can be incorporated into rehabilitation, optimising the return to play and return to performance process. The aim of this article is to give clinicians guidance with clear practical applications to assist with resolving persistent deficits that may be present in athletic populations following injury. This information is important as it will enhance sports performance and reduce the risk of recurrence and subsequent injury.
2 Maximal Strength
The development of muscular strength can be broadly divided into morphological and neural factors [46]. The maximal force generated by a single muscle fibre is directly proportional to its cross-sectional area (CSA) [47, 48] which is determined by the number of sarcomeres in parallel, an important parameter of its force generating capacity. Greater pennation angles are more common in hypertrophied than in normal muscles. Maximal force is also influenced by the muscle fibres composition [44, 46, 49, 50]. Specifically, type II fibres (IIa/IIx) have a greater capacity to generate power per unit CSA, than the relatively smaller type I fibres. Architectural features such as longer fascicle length allow more force production through an optimal length–tension relationship [46]. The number of sarcomeres in series influences a muscle’s contractility and the rate at which it can shorten. In regards to neural factors, the size principle dictates that motor unit (MU) recruitment is related to motor unit type and that MUs are recruited in a sequenced manner based on their size (smallest to largest) [51]. Thus, the availability of high-threshold MUs and/or lower threshold of MU recruitment is advantageous for higher force production. Furthermore, a higher rate of neural impulses (firing frequency) and the concurrent activation of multiple motor units (motor unit synchronisation) enhance the magnitude of force generated during a contraction. These, together with an effective inter-muscular coordination (i.e. appropriate magnitude and timing of activation of agonist, synergist and antagonist muscles) permit maximal force production [44, 46, 49, 50, 52].
2.1 The Importance of Maximal Strength
In sport, the ability to generate maximal force is limited by the time constraints of specific tasks; thus, rate of force development (RFD) and power are a critical part of optimising physical performance. Maximal strength can be defined as the upper limit of the neuromuscular system to produce force [53], with increases in this capacity correlated with RFD and power [45, 54,55,56]. Current literature suggests that athletes who can back squat 2 × body mass are able to best capitalise on these associations [55], as well as changes in endocrine concentrations (namely testosterone) in response to training [57]. Furthermore, current evidence suggests that until athletes can squat at least 1.6 × body mass, maximal strength training should be the dominant training modality [43]. Specifically, Cormie et al. [43] examined the effect of a 10-week (3/week) training intervention of either strength training or ballistic-power training on jumping and sprinting performances, force–velocity profile, muscle architecture, and neural drive in a cohort of 24 male subjects who were proficient in the back squat. They found that despite both groups displaying similar improvements in performance, relatively weak men (back squat < 1.6 × BM) benefited more from strength training due to its potential long-term improvement. This occurred as a result of increased neural activation and muscle thickness, which are adaptations specific to this type of training stimulus. This is in line with the recent research performed by Comfort et al. [58] who showed that prior identification of athletic physical characteristics (here using the dynamic strength index calculation) may improve the prediction of significant changes in response to a specific type of training. In particular, they emphasised the importance of increasing force production via strength training in weaker athletes. This is reinforced by James et al. [59], who revealed that the magnitude of improvement in peak velocity in response to ballistic training was significantly influenced by baseline strength levels in the first 5 weeks of training. Overall, the available evidence suggests that achieving and maintaining a high level of strength is of utmost importance in the athletic population for positive adaptations.
Indeed, developing maximal strength has been shown to have significant benefits on musculotendinous stiffness [60], neuromuscular inhibition [44, 61], and connective tissue strength [62,63,64,65], culminating in decreases in the relative force (% of maximum) applied during the loading phase of running at ground contact [66,67,68]. Collectively, this reduces metabolic demand for the same force output, creating a motor unit reserve available for additional work [67]. Normative data to ensure when a patient or an athlete is “strong enough” are available for isometric bilateral adductor strength tests [5, 13], although strength ratios between muscle groups of the same limb [17, 69] or threshold for inter-limb asymmetries are more commonly reported [12, 70,71,72,73,74,75]. These values may be used to examine single joint strength and guide training programmes, and to determine readiness to return to play following injuries; however, global measures of maximal strength are also warranted which display heightened transfer to athletic performance.
In addition to the physiological and performance advantages of developing maximal strength, it is not surprising that injury risk may be reduced by the adoption of this training modality. Lauersen et al. [76] indicated that a variety of strength training modalities can reduce sports injuries by one third, and overuse injuries by almost half. Furthermore, strength training programmes appears superior to neuromuscular training and multicomponent programmes in injury reduction [76]. More recently, Malone et al. [77] have shown that over two consecutive seasons, athletes who are stronger, faster, and have better repeated sprint ability (RSA) times have a lower injury risk than their weaker counterparts. Thus, increasing strength is a key component of any tertiary prevention approach and should be targeted within injury rehabilitation to reduce the risk of re-injury [11]. However, while research and clinical practice promote increases in strength, this has been largely investigated in several injury types in isolation, often with much lighter loads and subsequently higher repetition ranges. For example, loading schemes of < 80% 1RM are often reported in research articles with a rep-set configuration of “15 × 3” or “10 × 3” without a clear indication of the load employed [78, 79], or using relatively low loads, thus not targeting higher threshold motor units to maximise strength adaptations [80,81,82,83]. Instead, the clarity in details of exercise prescription is fundamental to define the physical as well as athletic adaptations targeted.
2.2 Strength Deficits Following Injury
Increased inhibitory inputs may reduce the extent to which muscles are voluntarily activated [84]. It is widely acknowledged that in the acute phase after an injury, local phenomena occurring in peripheral tissues such as swelling, inflammation and joint laxity, may change the discharge of sensory receptors, which causes neuromuscular inhibition. This is often referred to as arthrogenic muscle inhibition after distension or damage to structures of a joint [85]. Neuromuscular inhibition can persist even in the absence of effusion or pain [86], leading to persistent strength deficits that impair normal physical function, return to full performance, and increase the risk of re-injury and subsequent injury [87]. Mechanisms for this inhibition include complex neural adaptations from spinal reflex (affecting the group I non-reciprocal (Ib) inhibitory pathway, the flexion reflex and the gamma loop) and corticomotor excitability pathways [86, 88,89,90]. Neuromuscular inhibition would, therefore, explain persistent neuromuscular alterations (e.g. shift in joint torque–angle relationship, atrophy, reduction in in-series sarcomeres) and limit positive muscle adaptations to training despite the return to play [91,92,93,94].
Knee extensor and flexor strength is significantly reduced after anterior cruciate ligament reconstruction (ACLR) [16], even up to 10 years post-surgery [95]. These measures have been used to guide rehabilitation status [32] and reported as a significant predictor of re-injury [70]. Similarly, several studies have indicated that lower levels of eccentric knee flexor strength increased the risk of hamstrings re-injury [12]. This may be due to the directional specificity of the hamstring complex or this persistent maladaptive feature not being completely resolved in previously injured players. In fact, Brughelli et al. [96] showed that Australian Rules Football players with previous hamstring injuries had significant deficits in horizontal but not vertical force during running at submaximal velocities. Similarly, Lord et al. [97] demonstrated that horizontal force production decreases at a greater rate in previously injured than uninjured hamstrings during an RSA test in football players. Charlton et al. [98] found isometric knee flexion strength deficits in semi-professional Australian Rules Football players with a past history of hamstring injury for up to three seasons following injury. Other studies investigating common lower limb injuries revealed discrepancies in the association between strength values and risk of injury [32, 99] as well as inconsistent patterns of strength and performance change in symptomatic and asymptomatic subjects [100]. In addition, research has shown that muscle strength is impaired bilaterally and below normative data in runners with Achilles tendinopathy [101].
2.3 Using Maximal Strength Training to Target Deficits
The available data suggest that higher strength levels help to reduce the risk of sports injuries [12, 76, 102]. From a rehabilitation perspective, patients should be gradually progressed to heavier loads in a periodized manner, with high-intensity resistance training being a valid and effective therapeutic tool across age and gender in the treatment of the most common musculoskeletal injuries [103, 104]. From a neurobiological perspective, it may also reverse alterations in intra-cortical inhibitory networks in individuals with persistent musculoskeletal pain [88, 89, 100].
Current evidence indicates that prescription of maximal strength training should involve a load (or intensity) of 80–100% of the participant’s one-repetition maximum (1-RM), utilising approximately 1–6 repetitions, across 3–5 sets, with rest periods of 3–5 min and a frequency of 2–3 times per week [105]. Hence, for clinicians whose specific aim at a particular phase is to improve maximal force, they should be progressively working toward this volume load prescription. Evidence-based recommendations for an effective stimulus for tendon adaptation suggest high intensity loading (85–90% iMVC) applied in five sets of four repetitions with a contraction and relaxation duration of 3 s each and an inter-set rest of 2 min [106]. However, in the initial stages when they are unable to tolerate heavy loads, lower intensities may be employed in multiple high volume sets until momentary failure, to recruit the highest threshold motor units and to increase CSA [107, 108]. Alternatively, blood flow restriction training can be used to provide an effective stimulus during rehabilitation for patients who are load compromised [109]. Cross-education (i.e. heavy resistance training of the unaffected limb) can be also a viable option to reduce corticospinal inhibition [110], to increase contralateral limb strength [111] and to induce hypoalgesia [112]. A potential progression based on the rehabilitation phase and the patient’s irritability post-ACLR might be: (1) bodyweight single leg squat performed at high volume sets focusing on technique mastery and cross-education (2) single leg squat with light load and high volume sets until failure (with/without blood flow restriction) (3) split squat with progressive loading in a traditional periodization scheme until reaching the recommended prescription for maximal strength and (4) split squat performed accordingly with maximal strength recommendations, with potential adaptations highlighted in Table 1.
2.4 Using Isometric Strength Training to Target Deficits
From a rehabilitation perspective, isometric contractions may be employed during specific phases where dynamic contractions may be contraindicated. Although dependent on the persistent musculoskeletal condition analysed, isometric contractions are capable of inducing hypoalgesia for chronic hand, knee, and shoulder injuries [113], also during in-season [114, 115]. The hypoalgesic effect is, however, variable and not always consistent [116, 117]. This may depend on the population analysed, the tissues properties, the physical activity level, and the pain modulation profile of the subjects assessed [118,119,120,121,122].
During isometric contractions, the muscle-tendon unit remains at a constant length. Isometric muscle actions have been widely used due to their tightly controlled application of force at specific joint angles, their ability to develop greater force than concentric contractions, and their high reliability in assessing and tracking force production [123]. Isometric training at long muscle lengths and at high volumes is more effective for inducing muscle hypertrophy than at short muscle lengths [124,125,126], potentially due to greater blood flow occlusion, rates of oxygen consumption, and metabolite build-up [127]. Although it may not be an effective strategy for directly improving sports performance, isometric training shows the largest improvements at the trained angles [123]. This has connotations for athletes who are rehabilitating following injury. For example, in subjects who had previously sustained an ACL rupture, between-limbs deficits in quadriceps torque were evident at angles of less than 40 degrees knee flexion, as opposed to peak torque (which does not consider the angle at which the peak value occurs) [128, 129]. This may reveal the potential utility of implementing positional isometrics in a rehabilitation programme for ACL-deficient patients. Similarly, isometric quadriceps muscle actions, using the leg extension machine at 80% of the MVIC, and holding for 45 s for 5 sets, with 1 min between sets, may be employed for subjects with patellar tendinopathy when isotonic contractions are not tolerated or during in-season [114, 115, 130].
3 Rate of Force and Torque Development
3.1 The Importance of Rate of Force Development
Rate of Force Development (RFD) is defined as the ability of the neuromuscular system to produce a high rate of rise in muscle force per unit of time during the initial phase following contraction onset [45]; torque refers to a force that causes rotation. Contractile RFD is a parameter used for measuring “explosive” strength capabilities. It is determined from the slope of the force time curve (generally between 0 and 250 ms), and calculated as ∆Force/∆Time. Several factors can impact RFD, particularly the early phase (< 100 ms relative to contraction onset), which is more influenced by intrinsic muscle properties and neural drive; while the late phase (> 100 ms relative to contraction onset) is more respondent to maximal muscle strength [45, 131]. Considering that force application during skills such as sprinting, jumping, throwing, and kicking lasts approximately 30–200 ms [56], RFD is a critical performance characteristic central to success in most power-based sporting events, as well as endurance running performance [132].
3.2 RFD Deficits Following Injury
In addition to the short time frames available to execute sporting tasks, it has been demonstrated that non-contact ACL tears occur in a timeframe of less than 50 ms; while the quadriceps, for example, requires more than 300 ms to reach peak torque during isometric testing [22]. Angelozzi et al. [19] found significant deficits in RFD at 6 months post-ACLR in professional soccer players who had completed a typical standardised rehabilitation programme and achieved nearly full recovery in the International Knee Documentation Committee (IKDC), Tegner activity scale, KT1000 and MVIC, which are objective measures commonly used to guide return to sports decision-making. Similarly, Kline et al. [22] demonstrated reduced quadriceps RFD in subjects at 6 months post-ACLR with patellar tendon autograft.
Deficits in RFD have also been shown in other common pathologies. For example, Nunes et al. [18] found reduced RFD in hip abduction and extension in a cohort of physically active females with patellofemoral pain. In addition, Wang et al. [20] demonstrated lower values in early RFD in the triceps surae muscle in elite athletes with unilateral chronic Achilles tendinopathy, while Opar et al. [23] showed lower rate of torque development in previously injured hamstrings. Cumulatively, the available evidence indicates that restoration of the ability to apply high forces in short time frames is crucial from both a rehabilitative and performance perspective.
3.3 Using Training to Target RFD Deficits
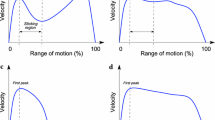
The available evidence indicates that training at high velocities or with the intention to move loads quickly is highly effective in eliciting marked gains in rapid force production capacity [131, 133,134,135]. This includes medicine ball throws, plyometrics [136], Olympic weightlifting and their derivatives [55, 137] (see Table 2 for further examples). The prescription of these can be best appreciated by defining the mechanical parameters that underpin power. Mechanically, power is the work performed per unit of time, or force multiplied by velocity. The inverse relationship between force and velocity can be illustrated by the force–velocity (FV) curve (Fig. 1), which identifies that maximum strength is exerted under high loads, and maximum speed is produced under low loads [56]. Subsequently, the goal of strength and conditioning programming is to improve force capability under the full spectrum of loads and thus velocities. For example, emerging evidence shows how different force–velocity profiles exist within individuals, thus suggesting that improving maximal strength may be most beneficial for some athletes, while others may benefit most from improving force at high velocity [137, 138]. This has been shown recently by Jimenez-Reyes et al. [138] who tailored the training programme based on the Force–Velocity profile during jumping. An individualised training programme specifically based on the difference between the actual and optimal Force–Velocity profiles of each individual (F–V imbalance) was more effective in improving jumping performance than traditional resistance training common to all subjects (velocity-deficit, force-deficit, and well-balanced increased by 12.7 ± 5.7% ES = 0.93 ± 0.09, 14.2 ± 7.3% ES = 1.00 ± 0.17, and 7.2 ± 4.5% ES = 0.70 ± 0.36, respectively). Furthermore, despite being just a case report, Mendiguchia et al. found that the capability to produce horizontal force at low speed (FH0) was altered both before and after return to sport from a hamstring injury in two professional athletes; thus, changing the slope of the F–V relationship [139]. The data collectively show that athletes need a well-rounded approach that prepares them to tolerate high and low loads as well as high and low velocities, not only from a performance perspective, but also to empower resilience to different stress stimuli and to increase musculoskeletal robustness.

Concentric portion of the force–velocity curve
4 Reactive Strength
4.1 The importance of Reactive Strength
Eccentric actions are those in which the musculotendinous unit actively lengthens throughout the muscle action. Eccentric training has received considerable attention due to its potentially more favourable adaptations compared to concentric, isometric, and traditional isotonic (eccentric/concentric) training [140, 141]. These include superior benefits for isometric and concentric strength, preferential recruitment of type II muscle fibres, power, RFD and stiffness, muscle architecture, and increased muscle activation, as well as improved performance in sporting actions [44, 142, 143]. Forceful eccentric contractions may have a superior impact in reducing intra-cortical inhibition and in increasing intra-cortical facilitation [110, 144]. These improvements can occur where there are high eccentric stretch loads, such as landing and change of direction mechanics, and fast stretch-shortening cycle (SSC) demands, because an athlete’s reactive strength ability is underpinned by relative maximal eccentric strength [145]; this again reinforces the need of substantial high levels of strength values before developing SSC capabilities [59]. The reactive strength index (RSI) has been widely employed to quantify plyometric or SSC performance, that is the ability to change quickly from an eccentric to concentric muscle action [146]. The factors that underpin an efficient SSC are related to the storage and the reutilization of elastic energy. These are the result of a number of mechanisms including utilisation of intrinsic muscle-tendon stiffness, involuntary reflex muscle activity, antagonistic co-contraction, and the SSC pre-stretch [147]. The latter, referred also as pre-activation during the eccentric phase, may allow for a greater number of motor units to be recruited during the concentric contraction through neural potentiation, thus indicating the important role of eccentric force production in SSC capabilities [146, 148].
The RSI can be used to assess leg stiffness. This can be described as the resistance to the deformation of the lower limb in response to an applied force. Therefore, a certain amount of lower extremity stiffness is required for effective storage and re-utilisation of elastic energy in SSC activities [132]. Lower extremity stiffness is considered to be a key attribute in the enhancement of running, jumping and hopping activities [149, 150]. Indeed, numerous studies reported that lower extremity stiffness increases with running velocity and this is concomitant with increased vertical ground reaction forces (GRFs), increased ground contact frequency, and shorter ground contact times [148, 151]. SSC activities have been divided into fast SSC (< 250 ms) and slow SSC (> 250 ms) accordingly with the ground contact time.
4.2 Reactive Strength Deficits Following Injury
Emerging evidence shows the importance of incorporating drop jumps in the evaluation of RSI as criteria for return to play. King et al. [26] revealed that the single leg drop jump identified greater performance deficits between the ACL reconstructed limb and the non-operated limb compared to the single leg hop for distance, suggesting insufficient rehabilitation status at 9 months post-surgery. Incomplete restoration of reactive strength and stiffness capabilities may also be present in the periods following a range of other injuries. Gore et al. [27] found that hip abductor stiffness was impaired in a cohort of subjects with athletic groin pain compared to controls and that this difference was no longer significant after the rehabilitation period. In the presence of Achilles Tendinopathy, several studies have shown that the tendon mechanical properties [152, 153], modulations of the SSC, leg stiffness, and RFD are altered [20, 28, 29]. This is in contrast with the normal function of the tendon complex, whose key role is to store, recoil and release energy while maintaining optimal efficiency in power production [154].
4.3 Using Training to Target Reactive Strength Deficits
Attainment of an adequate strength level is fundamental to the development of reactive strength as discussed previously. In addition, plyometric training can enhance early and late RFD as well as optimising leg stiffness and the modulation of the SSC [55, 155]. Plyometric training exploits the rapid cyclical muscle action of the SSC whereby the muscle undergoes a lengthening movement (“eccentric muscle action”), followed by a transitional period prior to the shortening movement (“concentric contraction”) and can be used to improve eccentric force generation capacity. Flanagan et al. [146] suggested a 4-step progression focusing on the eccentric jumping action while landing (phase 1); rebound spring-like actions with short ground contact times (phase 2); hurdle jumps with an emphasis on short ground contact while increasing intensity of the eccentric stimulus (phase 3); and finally depth jumps to maximise jump height while maintaining minimal ground contact times (phase 4) (Table 3). Furthermore, progressive training intensities might be an effective prescription to achieve improvements in change of direction ability [149, 156].
Alternative strategies for athletes who have attained the requisite level of strength include accentuated eccentric loading (AEL) to increase eccentric strength via supra-maximal loading [140, 145]. Examples include adopting weight releasers or dumbbells dropped in the bottom position to overload the eccentric portion of the movement, enhancing the subsequent concentric action. Following ACLR, patients who have undergone a suitable period of rehabilitation and reached normative strength values across different ranges of motion and velocities, may benefit from AEL to further increase quadriceps eccentric strength [157], together with progressive intensities of plyometric training. However, AEL by definition is not commonly employed in rehabilitation strategies, although sports medicine professionals are now widely applying eccentric loads for the prevention and rehabilitation of hamstring injuries. The Nordic hamstring exercise has been shown to significantly reduce the risk of hamstring injuries [158,159,160]. Furthermore, even a low training volume can stimulate increases in fascicle length and improvements in eccentric knee flexor strength [40]. Similarly, the Copenhagen adduction exercise is commonly prescribed due to its superior ability to increase eccentric hip adduction strength [82] and the eccentric triceps surae exercise has been shown to increase not only maximal strength, tendon stiffness, Young’s modulus and tendon CSA [60, 106, 161], but also ankle dorsiflexion [162] and the SSC behaviour.
Practically, AEL can be applied by completing the concentric portion of the movement with both limbs at high loading schemes and using only the involved limb for the eccentric portion, thus resulting in load above 100% of 1RM. Similarly, the athlete may also be assisted during the concentric portion of the exercise while the eccentric portion is completed independently. Alternatively, the use of heavy chains allows increases of load during both the early concentric phase of the lift as well as early eccentric phase of the descent, due to the favourable muscle leverage and the additional chain links [163].
4.4 Return to Play Tests and the Need to Test Multiple Physical Capacities
A recent review on the topic of ACL rehabilitation summarised that there is a high rate of return to sport overall (81–82%) but a lower rate for competitive sports (44–55%). These data appear to be dictated by fear of re-injury as well as functional capabilities of the reconstructed knee; the latter tended to be deemed optimal when both Limb Symmetry Index and hop tests reach at least 90% of the contralateral limb [16]. However, Ardern et al. [164] found that, despite obtaining what was considered normal strength values, the rate of return to sport was low. This suggests that evaluating maximal strength at low velocities only, as per current most common criteria to return athletes to unrestricted sports activities, is not sufficient. Indeed, a recent review [165] analysed the discharge criteria for RTS following primary ACLR in studies published from 2001 to 2011, revealing that 85% of studies used time based measures as RTS criterion. Strength criteria were reported in 41% of studies, whereas physical performance-based criteria in only 20% of studies. This may indicate a potential gap in the implementation of performance strategies and tests in rehabilitation settings. Return to play criteria should, therefore, also consider multiple physical capacities and assessments of maximal strength, reactive strength, RFD and power capabilities along the whole F–V curve and in multiple planes, in addition to vertical jumps, change of directions, acceleration, deceleration and speed actions as dictated by each individual’s sports demands through the completion of a comprehensive needs analysis.
4.5 Programme Design
When attempting to maximise power output, provided that a high overall level of strength has been reached, a periodized mixed methods approach, in which a variety of loads and exercise types are used is suggested. This is because it allows a more complete development of the force–velocity relationship (Fig. 1). The use of low-load, high-velocity movements (such as unloaded jump squats) may have a greater influence on the high-velocity area of the force–velocity curve; while heavier loads (e.g. used in the back squat) improve to a greater degree the high-force portion [50]. Training modalities may, therefore, include weightlifting exercises and/or derivatives, unilateral and/or bilateral training with a range of loads, and plyometric or ballistic exercises in an appropriately periodized manner [55, 131, 166]. Optimal levels of maximal strength are the foundation for the development of efficient SSC properties, as well as for ballistic sport-specific movements. Furthermore, volume and intensity will be manipulated to maximise physical capabilities throughout their rehabilitation as dictated by their ability to load safely in the context of their injury and also as the athlete transitions towards a return to sports performance [167, 168]. Examples of potential rehabilitation programmes are outlined in Tables 4 and 5.
4.6 Conclusion
This article has examined persistent deficits in fundamental physical qualities, such as strength, rate of force development and reactive strength following injury. Training strategies to target these deficits have also been discussed to increase an athlete’s readiness to return to sport. The concepts expressed in this article may help clinicians to reduce the gap between rehabilitation and sports performance, while providing a means of tertiary prevention following injury. Rehabilitation should aim to optimise physical performance, not only return athletes to participation. To achieve this, a strong cooperation among health professionals, coaches and strength and conditioning specialists is essential. Furthermore, implementation of the best available evidence of strength and conditioning and exercise physiology is required to maximise training adaptation.
References
Drew MK, Raysmith BP, Charlton PC. Injuries impair the chance of successful performance by sportspeople: a systematic review. Br J Sports Med. 2017;51(16):1209–14.
Hagglund M, et al. Injuries affect team performance negatively in professional football: an 11-year follow-up of the UEFA Champions League injury study. Br J Sports Med. 2013;47(12):738–42.
Williams S, et al. Time loss injuries compromise team success in Elite Rugby Union: a 7-year prospective study. Br J Sports Med. 2016;50(11):651.
Windt J, et al. Does player unavailability affect football teams’ match physical outputs? A two-season study of the UEFA champions league. J Sci Med Sport. 2018;21(5):525–32.
Esteve E, et al. Preseason adductor squeeze strength in 303 Spanish Male Soccer Athletes: a cross-sectional study. Orthop J Sports Med. 2018;6(1):2325967117747275.
Hägglund M, Waldén M, Ekstrand J. Risk factors for lower extremity muscle injury in professional soccer: the UEFA injury study. Am J Sports Med. 2012;41(2):327–35.
Arnason A, et al. Risk factors for injuries in football. Am J Sports Med. 2004;32(1 Suppl):5s–16s.
Hagglund M, Walden M, Ekstrand J. Previous injury as a risk factor for injury in elite football: a prospective study over two consecutive seasons. Br J Sports Med. 2006;40(9):767–72.
Fulton J, et al. Injury risk is altered by previous injury: a systematic review of the literature and presentation of causative neuromuscular factors. Int J Sports Phys Ther. 2014;9(5):583–95.
Toohey LA, et al. Is subsequent lower limb injury associated with previous injury? A systematic review and meta-analysis. Br J Sports Med. 2017;51(23):1670–8.
Jacobsson J, Timpka T. Classification of prevention in sports medicine and epidemiology. Sports Med. 2015;45(11):1483–7.
Bourne MN, et al. An evidence-based framework for strengthening exercises to prevent hamstring injury. Sports Med. 2017.
Delahunt E, Fitzpatrick H, Blake C. Pre-season adductor squeeze test and HAGOS function sport and recreation subscale scores predict groin injury in Gaelic football players. Phys Ther Sport. 2017;23:1–6.
O’Neill S, Watson PJ, Barry S. A Delphi study of risk factors for Achilles tendinopathy-opinions of world tendon experts. Int J Sports Phys Ther. 2016;11(5):684–97.
Neal BS, Lack SD. Risk factors for patellofemoral pain: a systematic review and meta-analysis. Br J Sports Med. 2019;53:270–81.
Anderson MJ, et al. A systematic summary of systematic reviews on the topic of the anterior cruciate ligament. Orthop J Sports Med. 2016;4(3):2325967116634074.
Thorborg K, et al. Eccentric and isometric hip adduction strength in male soccer players with and without adductor-related groin pain: an assessor-blinded comparison. Orthop J Sports Med. 2014;2(2):2325967114521778.
Nunes GS, Barton CJ, Serrao FV. Hip rate of force development and strength are impaired in females with patellofemoral pain without signs of altered gluteus medius and maximus morphology. J Sci Med Sport. 2017.
Angelozzi M, et al. Rate of force development as an adjunctive outcome measure for return-to-sport decisions after anterior cruciate ligament reconstruction. J Orthop Sports Phys Ther. 2012;42(9):772–80.
Wang HK, et al. Evoked spinal reflexes and force development in elite athletes with middle-portion Achilles tendinopathy. J Orthop Sports Phys Ther. 2011;41(10):785–94.
Cobian DG, et al. Knee extensor rate of torque development before and after arthroscopic partial meniscectomy, with analysis of neuromuscular mechanisms. J Orthop Sports Phys Ther. 2017;47(12):945–56.
Kline PW, et al. Impaired quadriceps rate of torque development and knee mechanics after anterior cruciate ligament reconstruction with patellar tendon autograft. Am J Sports Med. 2015;43(10):2553–8.
Opar DA, et al. Rate of torque and electromyographic development during anticipated eccentric contraction is lower in previously strained hamstrings. Am J Sports Med. 2013;41(1):116–25.
Doherty C, et al. Coordination and symmetry patterns during the drop vertical jump, 6-months after first-time lateral ankle sprain. J Orthop Res. 2015;33(10):1537–44.
Doherty C, et al. Recovery from a first-time lateral ankle sprain and the predictors of chronic ankle instability: a prospective cohort analysis. Am J Sports Med. 2016;44(4):995–1003.
King E. et al. Whole-body biomechanical differences between limbs exist 9 months after ACL reconstruction across jump/landing tasks. Scand J Med Sci Sports. 2018.
Gore SJ, Franklyn-Miller A. Is stiffness related to athletic groin pain? Scand J Med Sci Sports. 2018;28(6):1681–90.
Debenham JR, et al. Achilles tendinopathy alters stretch shortening cycle behaviour during a sub-maximal hopping task. J Sci Med Sport. 2016;19(1):69–73.
Maquirriain J. Leg stiffness changes in athletes with Achilles tendinopathy. Int J Sports Med. 2012;33(7):567–71.
Pruyn EC, et al. Relationship between leg stiffness and lower body injuries in professional Australian football. J Sports Sci. 2012;30(1):71–8.
Lorimer AV, Hume PA. Stiffness as a risk factor for achilles tendon injury in running athletes. Sports Med. 2016;46(12):1921–38.
O’Malley E, et al. Countermovement jump and isokinetic dynamometry as measures of rehabilitation status after anterior cruciate ligament reconstruction. J Athletes Train. 2018;53(7):687–95.
Pratt KA, Sigward SM. Detection of knee power deficits following ACL reconstruction using wearable sensors. J Orthop Sports Phys Ther. 2018;48:1–24.
Lee DW, et al. Single-leg vertical jump test as a functional test after anterior cruciate ligament reconstruction. Knee. 2018;25(6):1016–26.
Morin JB, Samozino P. Interpreting power-force-velocity profiles for individualized and specific training. Int J Sports Physiol Perform. 2016;11(2):267–72.
Lorenz DS, Reiman MP. Performance enhancement in the terminal phases of rehabilitation. Sports Health. 2011;3(5):470–80.
Macdonald B et al. The single-leg Roman chair hold is more effective than the Nordic hamstring curl in improving hamstring strength-endurance in Gaelic footballers with previous hamstring injury. J Strength Cond Res. 2018.
Beyer R, et al. Heavy slow resistance versus eccentric training as treatment for achilles tendinopathy: a randomized controlled trial. Am J Sports Med. 2015;43(7):1704–11.
Lack S, et al. Proximal muscle rehabilitation is effective for patellofemoral pain: a systematic review with meta-analysis. Br J Sports Med. 2015;49(21):1365–76.
Presland JD, et al. The effect of Nordic hamstring exercise training volume on biceps femoris long head architectural adaptation. Scand J Med Sci Sports. 2018;28(7):1775–83.
Newton RU, Kraemer WJ. Developing explosive muscular power: implications for a mixed methods training strategy. Strength Cond J. 1994;16(5):20–31.
Kawamori N, Haff GG. The optimal training load for the development of muscular power. J Strength Cond Res. 2004;18(3):675–84.
Cormie P, McGuigan MR, Newton RU. Adaptations in athletic performance after ballistic power versus strength training. Med Sci Sports Exerc. 2010;42(8):1582–98.
Suchomel TJ, et al. The importance of muscular strength: training considerations. Sports Med. 2018;48:765.
Rodríguez-Rosell D, et al. Physiological and methodological aspects of rate of force development assessment in human skeletal muscle. Clin Physiol Funct Imaging. 2018;38(5):743–62.
Cormie P, McGuigan MR, Newton RU. Developing maximal neuromuscular power: part 1—biological basis of maximal power production. Sports Med. 2011;41(1):17–38.
Hornsby WG, et al. What is the impact of muscle hypertrophy on strength and sport performance? Strength Cond J. 2018;40(6):99–111.
Taber CB, et al. Exercise-induced myofibrillar hypertrophy is a contributory cause of gains in muscle strength. Sports Med. 2019;49(7):993–7.
Hughes DC, Ellefsen S, Baar K. Adaptations to endurance and strength training. Cold Spring Harb Perspect Med. 2017;8(6).
Haff GG, Stone MH. Methods of developing power with special reference to football players. Strength Cond J. 2015;37(6):2–16.
Henneman E, Somjen G, Carpenter DO. Excitability and inhibitability of motoneurons of different sizes. J Neurophysiol. 1965;28(3):599–620.
Clark BC, et al. The power of the mind: the cortex as a critical determinant of muscle strength/weakness. J Neurophysiol. 2014;112(12):3219–26.
Stone MH, et al. The importance of isometric maximum strength and peak rate-of-force development in sprint cycling. J Strength Cond Res. 2004;18(4):878–84.
Aagaard P, et al. Increased rate of force development and neural drive of human skeletal muscle following resistance training. J Appl Physiol (1985). 2002;93(4):1318–26.
Haff GG, Nimphius S. Training principles for power. Strength Cond Res. 2012;34(6):2–12.
Taber C, et al. Roles of maximal strength and rate of force development in maximizing muscular power. Strength Cond Res. 2016;38(1):71–8.
Crewther BT, et al. Baseline strength can influence the ability of salivary free testosterone to predict squat and sprinting performance. J Strength Cond Res. 2012;26(1):261–8.
Comfort P, Thomas C. Changes in dynamic strength index in response to strength training. Sports. 2018;6:176.
James LP, et al. The impact of strength level on adaptations to combined weightlifting, plyometric, and ballistic training. Scand J Med Sci Sports. 2018;28(5):1494–505.
Bohm S, Mersmann F, Arampatzis A. Human tendon adaptation in response to mechanical loading: a systematic review and meta-analysis of exercise intervention studies on healthy adults. Sports Med Open. 2015;1(1):7.
Kidgell DJ, et al. Corticospinal responses following strength training: a systematic review and meta-analysis. Eur J Neurosci. 2017;46(11):2648–61.
Watson SL, et al. High-intensity resistance and impact training improves bone mineral density and physical function in postmenopausal women with osteopenia and osteoporosis: the LIFTMOR randomized controlled trial. J Bone Miner Res. 2018;33(2):211–20.
Magnusson SP, Kjaer M. The impact of loading, unloading, ageing and injury on the human tendon. J Physiol. 2019;597(5):1283–98.
Goodman CA, Hornberger TA, Robling AG. Bone and skeletal muscle: key players in mechanotransduction and potential overlapping mechanisms. Bone. 2015;80:24–36.
Grzelak P, et al. Hypertrophied cruciate ligament in high performance weightlifters observed in magnetic resonance imaging. Int Orthop. 2012;36(8):1715–9.
Ploutz L, et al. Effect of resistance training on muscle use during exercise. J Appl Physiol. 1994;76:1675–81.
Stone M, Stone M, Sands W. Principles and practice or resistance training. New York: Human Kinetics; 2007.
Ploutz LL, et al. Effect of resistance training on muscle use during exercise. J Appl Physiol (1985). 1994;76(4):1675–81.
Baroni BM et al. Hamstring-to-quadriceps torque ratios of professional male soccer players: a systematic review. J Strength Cond Res. 2018.
Grindem H, et al. Simple decision rules can reduce reinjury risk by 84% after ACL reconstruction: the Delaware–Oslo ACL cohort study. Br J Sports Med. 2016;50(13):804–8.
Bourne MN, et al. Eccentric knee flexor strength and risk of hamstring injuries in Rugby Union: a prospective study. Am J Sports Med. 2015;43(11):2663–70.
Kyritsis P, et al. Likelihood of ACL graft rupture: not meeting six clinical discharge criteria before return to sport is associated with a four times greater risk of rupture. Br J Sports Med. 2016;50(15):946–51.
Adams D, et al. Current concepts for anterior cruciate ligament reconstruction: a criterion-based rehabilitation progression. J Orthop Sports Phys Ther. 2012;42(7):601–14.
Ardern CL, et al. 2016 Consensus statement on return to sport from the First World Congress in Sports Physical Therapy, Bern. Br J Sports Med. 2016;50(14):853.
Grindem H, et al. How does a combined preoperative and postoperative rehabilitation programme influence the outcome of ACL reconstruction 2 years after surgery? A comparison between patients in the Delaware–Oslo ACL Cohort and the Norwegian National Knee Ligament Registry. Br J Sports Med. 2015;49(6):385–9.
Lauersen JB, Bertelsen DM, Andersen LB. The effectiveness of exercise interventions to prevent sports injuries: a systematic review and meta-analysis of randomised controlled trials. Br J Sports Med. 2014;48(11):871.
Malone S, et al. Can the workload-injury relationship be moderated by improved strength, speed and repeated-sprint qualities? J Sci Med Sport. 2019;22(1):29–34.
Holden S, Barton CJ. ‘What should I prescribe?’: time to improve reporting of resistance training programmes to ensure accurate translation and implementation. Br J Sports Med. 2018;53:264–5.
Holden S, et al. How can we implement exercise therapy for patellofemoral pain if we don’t know what was prescribed? A systematic review. Br J Sports Med. 2018;52(6):385.
Murphy M, et al. Rate of improvement of pain and function in mid-portion achilles tendinopathy with loading protocols: a systematic review and longitudinal meta-analysis. Sports Med. 2018;48(8):1875–91.
Malliaras P, et al. Achilles and patellar tendinopathy loading programmes: a systematic review comparing clinical outcomes and identifying potential mechanisms for effectiveness. Sports Med. 2013;43(4):267–86.
Ishoi L, et al. Large eccentric strength increase using the Copenhagen Adduction exercise in football: a randomized controlled trial. Scand J Med Sci Sports. 2016;26(11):1334–42.
Yousefzadeh A, et al. The effect of therapeutic exercise on long-standing adductor-related groin pain in athletes: modified Holmich protocol. Rehabil Res Pract. 2018;2018:10.
Sonnery-Cottet B, Saithna A. Arthrogenic muscle inhibition after ACL reconstruction: a scoping review of the efficacy of interventions. Br J Sports Med. 2019;53(5):289–98.
Hopkins JT, Ingersoll CD. Arthrogenic muscle inhibition: a limiting factor in joint rehabilitation. J Sport Rehabil. 2000;9(2):135–59.
Rice DA, McNair PJ. Quadriceps arthrogenic muscle inhibition: neural mechanisms and treatment perspectives. Semin Arthritis Rheum. 2010;40(3):250–66.
Pietrosimone BG, et al. Neural excitability alterations after anterior cruciate ligament reconstruction. J Athl Train. 2015;50(6):665–74.
Roy JS, et al. Beyond the joint: the role of central nervous system reorganizations in chronic musculoskeletal disorders. J Orthop Sports Phys Ther. 2017;47(11):817–21.
Chang WJ, et al. Altered primary motor cortex structure, organization, and function in chronic pain: a systematic review and meta-analysis. J Pain. 2018;19(4):341–59.
Te M, et al. Primary motor cortex organization is altered in persistent patellofemoral pain. Pain Med. 2017;18(11):2224–34.
Fyfe JJ, et al. The role of neuromuscular inhibition in hamstring strain injury recurrence. J Electromyogr Kinesiol. 2013;23(3):523–30.
Brockett CL, Morgan DL, Proske U. Predicting hamstring strain injury in elite athletes. Med Sci Sports Exerc. 2004;36(3):379–87.
Roig M, et al. The effects of eccentric versus concentric resistance training on muscle strength and mass in healthy adults: a systematic review with meta-analysis. Br J Sports Med. 2009;43(8):556–68.
Silder A, et al. MR observations of long-term musculotendon remodeling following a hamstring strain injury. Skelet Radiol. 2008;37(12):1101–9.
Bourne MN, et al. Eccentric knee flexor weakness in elite female footballers 1–10 years following anterior cruciate ligament reconstruction. Phys Ther Sport. 2019;37:144–9.
Brughelli M, et al. Contralateral leg deficits in kinetic and kinematic variables during running in Australian rules football players with previous hamstring injuries. J Strength Cond Res. 2010;24(9):2539–44.
Lord C, et al. Greater loss of horizontal force after a repeated-sprint test in footballers with a previous hamstring injury. J Sci Med Sport. 2019;22(1):16–21.
Charlton PC, et al. Knee flexion not hip extension strength is persistently reduced following hamstring strain injury in Australian Football athletes: implications for Periodic Health Examinations. J Sci Med Sport. 2018;21(10):999–1003.
Rathleff MS, et al. Is hip strength a risk factor for patellofemoral pain? A systematic review and meta-analysis. Br J Sports Med. 2014;48(14):1088.
Rio E, et al. Tendon neuroplastic training: changing the way we think about tendon rehabilitation: a narrative review. Br J Sports Med. 2016;50(4):209–15.
O’Neill S, Barry S, Watson P. Plantarflexor strength and endurance deficits associated with mid-portion Achilles tendinopathy: the role of soleus. Phys Ther Sport. 2019;37:69–76.
Thorborg K. Why hamstring eccentrics are hamstring essentials. Br J Sports Med. 2012;46(7):463–5.
Kristensen J, Franklyn-Miller A. Resistance training in musculoskeletal rehabilitation: a systematic review. Br J Sports Med. 2012;46(10):719.
Booth J, et al. Exercise for chronic musculoskeletal pain: a biopsychosocial approach. Musculoskelet Care. 2017;15(4):413–21.
American College of Sports Medicine position stand. Progression models in resistance training for healthy adults. Med Sci Sports Exerc. 2009;41(3):687–708.
Mersmann F, Bohm S, Arampatzis A. Imbalances in the development of muscle and tendon as risk factor for tendinopathies in youth athletes: a review of current evidence and concepts of prevention. Front Physiol. 2017;8:987.
Schoenfeld BJ, et al. Strength and hypertrophy adaptations between low- vs high-load resistance training: a systematic review and meta-analysis. J Strength Cond Res. 2017;31(12):3508–23.
Schoenfeld BJ, Grgic J, Krieger J. How many times per week should a muscle be trained to maximize muscle hypertrophy? A systematic review and meta-analysis of studies examining the effects of resistance training frequency. J Sports Sci. 2018;37:1–10.
Hughes L, et al. Blood flow restriction training in clinical musculoskeletal rehabilitation: a systematic review and meta-analysis. Br J Sports Med. 2017;51(13):1003.
Kidgell DJ, et al. Increased cross-education of muscle strength and reduced corticospinal inhibition following eccentric strength training. Neuroscience. 2015;300:566–75.
Cirer-Sastre R, Beltrán-Garrido JV, Corbi F. Contralateral effects after unilateral strength training: a meta-analysis comparing training loads. J Sports Sci Med. 2017;16(2):180–6.
Vaegter HB. Exercising non-painful muscles can induce hypoalgesia in individuals with chronic pain. Scand J Pain. 2017;15:60–1.
Naugle KM, Fillingim RB, Riley I. A meta-analytic review of the hypoalgesic effects of exercise. J Pain. 2012;13(12):1139–50.
Rio E, et al. Isometric contractions are more analgesic than isotonic contractions for patellar tendon pain: an in-season randomized clinical trial. Clin J Sport Med. 2017;27(3):253–9.
Rio E et al. isometric exercise to reduce pain in patellar tendinopathy in-season; is it effective “on the road?”. Clin J Sport Med. 2017.
O’Neill S, et al. Acute sensory and motor response to 45-s heavy isometric holds for the plantar flexors in patients with Achilles tendinopathy. Knee Surg Sports Traumatol Arthrosc. 2018;27(9):2765–73.
Riel H, Vicenzino B. The effect of isometric exercise on pain in individuals with plantar fasciopathy: a randomized crossover trial. Scand J Med Sci Sports. 2018;28(12):2643–50.
Lemley KJ, Hunter SK, Bement MK. Conditioned pain modulation predicts exercise-induced hypoalgesia in healthy adults. Med Sci Sports Exerc. 2015;47(1):176–84.
Naugle KM, et al. Physical activity behavior predicts endogenous pain modulation in older adults. Pain. 2017;158(3):383–90.
Naugle KM, et al. Isometric exercise as a test of pain modulation: effects of experimental pain test, psychological variables, and sex. Pain Med. 2014;15(4):692–701.
Sluka KA, Frey-Law L, Hoeger Bement M. Exercise-induced pain and analgesia? Underlying mechanisms and clinical translation. Pain. 2018;159(Suppl 1):S91–7.
Coombes BK, Tucker K. Achilles and patellar tendinopathy display opposite changes in elastic properties: a shear wave elastography study. Scand J Med Sci Sports. 2018;28(3):1201–8.
Oranchuk DJ, et al. Isometric training and long-term adaptations; effects of muscle length, intensity and intent: a systematic review. Scand J Med Sci Sports. 2019;29(4):484–503.
Alegre LM, et al. Effects of isometric training on the knee extensor moment-angle relationship and vastus lateralis muscle architecture. Eur J Appl Physiol. 2014;114(11):2437–46.
Kubo K, et al. Effects of isometric training at different knee angles on the muscle-tendon complex in vivo. Scand J Med Sci Sports. 2006;16(3):159–67.
Noorkoiv M, Nosaka K, Blazevich AJ. Neuromuscular adaptations associated with knee joint angle-specific force change. Med Sci Sports Exerc. 2014;46(8):1525–37.
de Ruiter CJ, et al. Knee angle-dependent oxygen consumption during isometric contractions of the knee extensors determined with near-infrared spectroscopy. J Appl Physiol (1985). 2005;99(2):579–86.
Huang H, et al. Isokinetic angle-specific moments and ratios characterizing hamstring and quadriceps strength in anterior cruciate ligament deficient knees. Sci Rep. 2017;7(1):7269.
Eitzen I, et al. Anterior cruciate ligament-deficient potential copers and noncopers reveal different isokinetic quadriceps strength profiles in the early stage after injury. Am J Sports Med. 2010;38(3):586–93.
Rio E, et al. Isometric exercise induces analgesia and reduces inhibition in patellar tendinopathy. Br J Sports Med. 2015;49(19):1277–83.
Maffiuletti NA, et al. Rate of force development: physiological and methodological considerations. Eur J Appl Physiol. 2016;116(6):1091–116.
Brazier J, et al. Lower extremity stiffness: considerations for testing, performance enhancement, and injury risk. J Strength Cond Res. 2019;33(4):1156–66.
Andersen LL, et al. Early and late rate of force development: differential adaptive responses to resistance training? Scand J Med Sci Sports. 2010;20(1):e162–9.
Tillin NA, Pain MT, Folland JP. Short-term training for explosive strength causes neural and mechanical adaptations. Exp Physiol. 2012;97(5):630–41.
Balshaw TG, et al. Training-specific functional, neural, and hypertrophic adaptations to explosive- vs. sustained-contraction strength training. J Appl Physiol (1985). 2016;120(11):1364–73.
Butler RJ, Crowell HP 3rd, Davis IM. Lower extremity stiffness: implications for performance and injury. Clin Biomech (Bristol, Avon). 2003;18(6):511–7.
Suchomel TJ, Comfort P, Lake JP. Enhancing the force–velocity profile of athletes using weightlifting derivatives. Strength Cond J. 2017;39(1):10–20.
Jiménez-Reyes P, et al. Effectiveness of an individualized training based on force–velocity profiling during jumping. Front Physiol. 2016;7:677.
Mendiguchia J, et al. Field monitoring of sprinting power-force-velocity profile before, during and after hamstring injury: two case reports. J Sports Sci. 2016;34(6):535–41.
Aagaard P. Spinal and supraspinal control of motor function during maximal eccentric muscle contraction: Effects of resistance training. J Sport Health Sci. 2018;7(3):282–93.
Nishikawa K. Eccentric contraction: unraveling mechanisms of force enhancement and energy conservation. J Exp Biol. 2016;219(2):189.
Wagle JP, et al. Accentuated eccentric loading for training and performance: a review. Sports Med. 2017;47(12):2473–95.
Harden M, et al. An evaluation of supramaximally loaded eccentric leg press exercise. J Strength Cond Res. 2018;32(10):2708–14.
Tallent J, et al. Enhanced corticospinal excitability and volitional drive in response to shortening and lengthening strength training and changes following detraining. Front Physiol. 2017;8:57.
Beattie K, et al. The relationship between maximal strength and reactive strength. Int J Sports Physiol Perform. 2017;12(4):548–53.
Flanagan EP, Comyns TM. The use of contact time and the reactive strength index to optimize fast stretch-shortening cycle training. Strength Cond J. 2008;30(5):32–8.
Pedley JS, et al. Drop jump: a technical model for scientific application. Strength Cond J. 2017;39(5):36–44.
McBride JM, McCaulley GO, Cormie P. Influence of preactivity and eccentric muscle activity on concentric performance during vertical jumping. J Strength Cond Res. 2008;22(3):750–7.
Asadi A, et al. The effects of plyometric training on change-of-direction ability: a meta-analysis. Int J Sports Physiol Perform. 2016;11(5):563–73.
Lum D, et al. Effects of intermittent sprint and plyometric training on endurance running performance. J Sport Health Sci. 2019;8(5):471–7.
Butler RJ, Crowell I, Davis IM. Lower extremity stiffness: implications for performance and injury. Clin Biomech. 2003;18(6):511–7.
Child S, et al. Mechanical properties of the achilles tendon aponeurosis are altered in athletes with achilles tendinopathy. Am J Sports Med. 2010;38(9):1885–93.
Obst SJ, et al. Are the mechanical or material properties of the achilles and patellar tendons altered in tendinopathy? A systematic review with meta-analysis. Sports Med. 2018;48(9):2179–98.
Turner AN, Jeffreys I. The stretch-shortening cycle: proposed mechanisms and methods for enhancement. Strength Cond J. 2010;32(4):87–99.
Maloney SJ, et al. Unilateral stiffness interventions augment vertical stiffness and change of direction speed. J Strength Cond Res. 2019;33(2):372–9.
Maloney SJ, et al. Do stiffness and asymmetries predict change of direction performance? J Sports Sci. 2017;35(6):547–56.
Lepley LK, Palmieri-Smith R. Effect of eccentric strengthening after anterior cruciate ligament reconstruction on quadriceps strength. J Sport Rehabil. 2013;22(2):150–6.
van der Horst N, et al. The preventive effect of the nordic hamstring exercise on hamstring injuries in amateur soccer players: a randomized controlled trial. Am J Sports Med. 2015;43(6):1316–23.
Arnason A, et al. Prevention of hamstring strains in elite soccer: an intervention study. Scand J Med Sci Sports. 2008;18(1):40–8.
Petersen J, et al. Preventive effect of eccentric training on acute hamstring injuries in men’s soccer: a cluster-randomized controlled trial. Am J Sports Med. 2011;39(11):2296–303.
Geremia JM, et al. Effects of high loading by eccentric triceps surae training on Achilles tendon properties in humans. Eur J Appl Physiol. 2018;118(8):1725–36.
Aune AAG, et al. Acute and chronic effects of foam rolling vs eccentric exercise on ROM and force output of the plantar flexors. J Sports Sci. 2018;37:1–8.
Ghigiarelli JJ, et al. The effects of a 7-week heavy elastic band and weight chain program on upper-body strength and upper-body power in a sample of division 1-AA football players. J Strength Cond Res. 2009;23(3):756–64.
Ardern CL, et al. Return to sport following anterior cruciate ligament reconstruction surgery: a systematic review and meta-analysis of the state of play. Br J Sports Med. 2011;45(7):596–606.
Burgi CR, et al. Which criteria are used to clear patients to return to sport after primary ACL reconstruction? A scoping review. Br J Sports Med. 2019;53(18):1154–61.
Comfort P, McMahon JJ, Suchomel TJ. Optimizing squat technique—revisited. Strength Cond J. 9000. (Publish Ahead of Print).
Kiely J. Periodization theory: confronting an inconvenient truth. Sports Med. 2018;48(4):753–64.
Cunanan AJ, et al. The general adaptation syndrome: a foundation for the concept of periodization. Sports Med. 2018;48(4):787–97.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Luca Maestroni, Paul Read, Chris Bishop and Anthony Turner declare that they have no conflict of interest.
Funding
No financial support was received for the preparation of this manuscript
Rights and permissions
About this article

Cite this article
Maestroni, L., Read, P., Bishop, C. et al. Strength and Power Training in Rehabilitation: Underpinning Principles and Practical Strategies to Return Athletes to High Performance. Sports Med 50, 239–252 (2020). https://doi.org/10.1007/s40279-019-01195-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40279-019-01195-6