
Abstract
Background
Increases in maximal oxygen uptake (VO2max) are strongly associated with improved cardiovascular health.
Objective
The aim was to perform a systematic review and meta-analysis to determine whether VO2max responses to endurance training (ET), the most effective intervention to improve VO2max, are influenced by sex.
Methods
We conducted a systematic search of MEDLINE and Web of Science since their inceptions until February 2019 for articles assessing the VO2max response to a given sex-matched dose of ET in healthy age-matched men and women. Meta-analyses were performed to determine the mean difference between VO2max responses in men versus women. Subgroup and meta-regression analyses were used to assess potential moderating factors.
Results
After systematic review, eight studies met the inclusion criteria. All studies implemented common modalities of ET in healthy untrained individuals, comprising a total of 175 men and women (90 ♂, 85 ♀). ET duration and intensity were sex-matched in all studies. After data pooling, ET induced substantially larger increases in absolute VO2max in men compared with women (mean difference = + 191 ml·min−1, 95% CI 99, 283; P < 0.001). A greater effect of ET on relative VO2max was also observed in men versus women (mean difference = + 1.95 ml·min−1·kg−1, 95% CI 0.76, 3.15; P = 0.001). No heterogeneity was detected among studies (I2 = 0%, P ≥ 0.59); the meta-analytical results were robust to potential moderating factors.
Conclusion
Pooled evidence demonstrates greater improvements in VO2max in healthy men compared with women in response to a given dose of ET, suggesting the presence of sexual dimorphism in the trainability of aerobic capacity.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Aerobic capacity, determined by maximal oxygen uptake (VO2max), is improved to a greater extent in men compared with women in response to a given dose of endurance training. |
The consistency of this finding against potential confounding factors suggests the presence of a sexual dimorphism regarding VO2max trainability. |
1 Introduction
Maximal oxygen uptake (VO2max), a hallmark of aerobic capacity, lies within 30–85 ml·min−1·kg−1 in healthy adults, encompassing a spectrum of aerobic capacities from untrained to elite endurance athletes [1,2,3]. Importantly, the higher is the VO2max, the greater the likelihood to be free of cardiovascular disease (CVD), the main cause of mortality worldwide [4, 5]. Every gain in VO2max counts; indeed, one metabolic equivalent increase in VO2max (+ 3.5 ml·min−1·kg−1) is independently associated with ≥ 13% reduction in cardiovascular events and all-cause mortality [6]. The mortality benefit of high VO2max seems to be slightly enhanced in women compared with men, possibly due to sex-specific adaptations underlying VO2max improvement [4, 5]. Efforts to enhance VO2max are commendable from functional and clinical standpoints in men and women.
The most effective intervention to improve VO2max in humans is endurance training (ET), with typical increases ranging from 1 to 3 metabolic equivalents after 6 weeks or longer ET programs [2, 3, 7]. Analogous to the dose-response of pharmacological interventions, VO2max responses to ET (thus termed VO2max trainability) primarily depend on the total training dose, a function of exercise intensity, frequency and duration [7,8,9]. As a matter of fact, the extreme VO2max levels reported in endurance athletes are underpinned by massive doses of ET sustained over several years [1, 10]. This observation is common to both male and female endurance athletes, albeit women frequently present with ~ 10 ml·min−1·kg−1 less VO2max compared with men of similar training status [1, 10]. Key determinants of VO2max improvement such as cardiac adaptations are also attenuated in women versus men in response to the same ET dose [11]. On the other hand, skeletal muscle adaptations may be augmented in women relative to men matched by VO2max and running performance [12]. Taken together, it has been suggested that women must be subjected to a higher ET dose than men to achieve a given VO2max [12], a notion entailing a new variant of sex dimorphism with potential prognostic implications. Yet, very few studies have been specifically designed to elucidate sex differences in training responsiveness [11, 13]. Likewise, the identification of ET interventions separately reporting men and women VO2max responses to the same training dose requires a systematic search of small sample size studies with seemingly conflicting results [11, 13,14,15,16,17,18,19]. Therefore, the primary purpose of this analysis was to systematically review and meta-analyze the effect of sex-matched doses of ET on VO2max in healthy men and women, as well as to determine the influence of potential moderating factors.
2 Methods
The review is reported according to the Meta-analysis Of Observational Studies in Epidemiology (MOOSE) Group guidelines [20].
2.1 Data Sources and Searches
The systematic search included MEDLINE and Web of Science, since their inceptions until February 2019. We used combinations of the subject headings ‘female’, ‘male’, ‘women’, ‘men’, ‘training’, ‘effect’, ‘adaptation’, ‘VO2max’ and ‘VO2peak’; the search strategy for MEDLINE is shown in Electronic Supplementary Material, Figure S1. We also performed hand searching in reference citations of identified reviews, personal article collections, articles included in meta-analysis and related citations in MEDLINE and Google Scholar.
2.2 Article Selection
To be included in the analysis, an original research article had to meet the following criteria: (1) ET intervention including healthy age-matched men and women, (2) definite sex-matched training dose, and (3) VO2max reported prior to and after training. Studies following the above criteria but including additional interventions deemed likely to influence VO2max were excluded. In the event of multiple publications pertaining to the same research, the most comprehensive report was included. Inclusion of articles was not limited by publication status or language.
2.3 Data Extraction and Quality Assessment
The following variables were summarized in a pre-formatted spreadsheet: authors, year of publication, characteristics of study participants (n, age, sex, height, body surface area, body mass index, weight, body fat percentage, heart rate, blood pressure, hematological profile, and health/fitness status), characteristics of the assessment of VO2max (pre-testing conditions, test protocol, and criteria of VO2max) and ET features (type, modality, frequency, intensity, session length, duration, and training dose). Given the observational design of the included studies, their methodological quality was assessed by a systematic appraisal of quality for observational research (SAQOR) [21] previously applied in meta-analyses evaluating VO2max responses to exercise training [2, 3]. The SAQOR was adjusted to assess (1) the study sample, (2) quality of VO2max assessment, (3) confounding variables and (4) data. Overall, the SAQOR was scored out of 14, quality deemed better with a greater score. Data extraction and quality assessment were performed independently and in duplicate by two investigators (D. M.) and (C. D).
2.4 Data Synthesis and Analysis
The meta-analysis was performed using Review Manager software (RevMan 5.3, Cochrane Collaboration, UK) and Comprehensive Meta-analysis software (CMA 2.0, Biostat, Englewood, USA). The primary outcomes were the mean difference between the effect of training on absolute VO2max (ml·min−1) or relative VO2max (ml·min−1·kg−1) in men versus women. If the variability of change (i.e., standard deviation of change (SDc)) for a given outcome was not reported, the formula SDc = √ [(SDpre)2 + (SDpost)2 − (2 × corrpre,post × SDpre × SDpost)] was applied [22]. SDpre, SDpost and corrpre,post represent the standard deviation of the pre-training value, the standard deviation of the post-training value, and the correlation coefficient between pre- and post-training values, respectively. The corrpre,post was conservatively set at 0.5. Each mean difference was weighted by the inverse variance and they were pooled with a random-effects model [23].
Heterogeneity among studies was assessed using the Chi-squared test for heterogeneity and I2 statistics. Potential moderating factors influencing the mean difference in VO2max were evaluated by subgroup analysis comparing studies grouped by qualitative variables related to the training program and methodology of exercise testing (e.g., use of continuous intensity versus interval training, assessment of VO2max with cycle ergometer versus treadmill). In addition, meta-regression analyses were performed to determine the association between the mean difference in VO2max and sex-related differences in potential moderating quantitative variables (age, height, weight, body surface area, body composition, maximal heart rate, training characteristics, baseline VO2max, year of publication, and methodological quality score). In all meta-regression models, studies were weighted by the inverse variance of the dependent variable. Potential moderating factors were entered as independent variables in regression models with the mean difference in VO2max as the dependent variable. Publication and/or other biases were evaluated by the Begg and Mazumdar’s rank correlation test and Egger’s regression test [24]. A P value < 0.05 was considered statistically significant.
3 Results
3.1 Study Selection and Characteristics
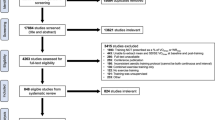
The flow diagram of the process of article selection is illustrated in Fig. 1, which resulted in the inclusion of 8 studies. Table 1 shows main characteristics of the included studies, comprising a total of 175 healthy individuals (90 ♂, 85 ♀). The mean age and weight ranged from 22 to 64 years and 59–82 kg, respectively. All the studies included untrained individuals, i.e., not engaged in regular exercise training and presenting with sedentary normal VO2max levels. VO2max was determined in all studies prior to and after ET with established incremental (cycle ergometer or treadmill) exercise protocols. The percentage change in VO2max from pre- to post-training ranged from 5.0 to 27.5% in men and from 2.9 to 26.3% in women. With respect to ET characteristics (Table 2), cycling was a modality of endurance exercise in all studies, while 3 studies additionally comprised running, walking and/or swimming [11, 13, 17]. Average session length, frequency and duration of the training program ranged from 0.4 to 3 h, 3–6 sessions per week and 7–52 weeks. The overall training dose, defined by exercise intensity and total training time, was matched between men and women in all studies (Electronic Supplementary Material, Table S1).

Flow diagram of the process of article selection
The methodological quality of the studies was moderate-to-high (Electronic Supplementary Material, Table S2). The average score was 8.4 ± 1.8 out of a possible 14 points. With respect to the evaluation of potential biases for the mean difference in VO2max, the Begg and Mazumdar’s rank correlation test (P = 0.71) and Egger’s regression test (P = 0.48) did not suggest the presence of publication bias and/or other biases in the studies included in the meta-analysis.
3.2 Effect of Endurance Training on VO2max in Men Versus Women
ET induced significant increases in absolute (ml·min−1) and relative (ml·min−1·kg−1) VO2max in all studies. After data pooling, ET induced a larger increase in absolute VO2max in men compared with women (n = 175, mean difference = 191 ml·min−1, 95% CI 99, 283 ml·min−1; P < 0.001) (Fig. 2). No heterogeneity was detected among studies (I2 = 0%, P = 0.69). Likewise, the meta-analysis revealed a greater effect of ET on relative VO2max in men versus women (n = 175, mean difference = 1.95 ml·min−1·kg−1, 95% CI 0.76, 3.15 ml·min−1·kg−1; P = 0.001) (Fig. 3), with null heterogeneity among studies (I2 = 0%, P = 0.59). Furthermore, subgroup and meta-regression analyses did not detect any significant influence of potential qualitative and quantitative moderating factors (main characteristics of study subjects, ET features, and study methodology) on the mean difference in VO2max, either in absolute or relative terms.

Forest plot of the mean difference between the training effect on absolute VO2max (ml·min−1) in men versus women. Squares represent the mean difference for each study. Diamonds represents the pooled mean difference across studies. CI confidence interval, df degrees of freedom, IV inverse variance, SD standard deviation

Forest plot of the mean difference between the training effect on relative VO2max (ml·min−1·kg−1) in men versus women. Squares represent the mean difference for each study. Diamonds represents the pooled mean difference across studies. CI confidence interval, df degrees of freedom, IV inverse variance, SD standard deviation
4 Discussion
In this systematic review and meta-analysis, we pooled and analyzed data from eight studies assessing the effects of sex-matched ET doses on VO2max in a total of 175 healthy men and women. The main finding of this meta-analysis is that ET elicits greater increases in VO2max in men compared with women, an outcome that was remarkably robust across potential moderating variables including baseline subject characteristics, ET features and exercise testing methodology.
The present meta-analysis of longitudinal studies indicates that for a given dose of ET, the VO2max response differs between men and women. In response to ET, men exhibit almost + 200 ml·min−1 and + 2 ml·min−1·kg−1 in VO2max, i.e., more than a half metabolic equivalent increase, compared with women, a gain associated with ~ 7–9% reductions in cardiovascular events and all-cause mortality [6]. Moreover, no significant heterogeneity was detected among studies. In line with our results, lower VO2max in women relative to men of comparable training status has been reported in cross-sectional studies [12, 25, 26]. Likewise, sedentary women generally present lower VO2max than men [27]. These differences could be explained by multiple factors, possibly assorted into two main categories: ‘constitutional’ and ‘environmental’. Conforming to the first category, sex differences in VO2max could primarily lie in sex-specific genetic traits. In contrast, distinct levels of physical activity/ET, possibly not discernible in cross-sectional studies, belong to the second class. The consistent results of this meta-analysis imply that ‘constitutional’, i.e., genetic factor(s) might underlie the sex-specific VO2max trainability. We may thus suggest the presence of inherent differences between men and women in VO2max responsiveness to ET, i.e., sex dimorphism of VO2max trainability [28]. Whilst speculative, from an evolutionary perspective DNA variant facilitating adaptations in VO2max could have been particularly selected in men [29]. Yet, the underpinning genetic basis of VO2max trainability remains unresolved and candidate genes (e.g., ACE) thought to explain high levels of VO2max have not been confirmed in population studies [30, 31]. Notwithstanding, the potential implications of the current findings in terms of sex-specific strategies to improve cardiovascular fitness and prevent CVD [4, 5, 30] will have to be addressed by future investigations.
The question arises as to which adaptations to ET could explain sex differences in VO2max trainability. Previous experimental studies have demonstrated the fundamental role of increases in blood volume and hemoglobin mass for ET-induced improvements in VO2max [7, 16, 32]. Blood volume expansion, comprising ~ 10% increments in plasma and red blood cell volume, is observed following approximately 4–6 weeks of ET in healthy previously untrained individuals [7, 16, 32,33,34]. As a result, cardiac preload, stroke volume and cardiac output are enhanced, collectively leading to increased capacity to deliver oxygen, the main determinant of VO2max in healthy humans [30, 32]. In fact, VO2max improvements are reverted to pre-training levels when hematological adaptations are abolished by means of phlebotomy [32, 35]. Yet, whether blood volume adaptations dictate cardiac function and aerobic capacity in women remains uncertain. The vast majority of previous experimental studies underpinning our current understanding of VO2max determinants mainly comprise young men. Provided that blood volume–cardiac interactions are not altered by sex, reduced VO2max trainability in women could be partly explained by blunted hematological adaptations [36]. In this respect, cross-sectional studies in elite female endurance athletes (Olympic medalists) clearly show high blood volumes (5–6 l), albeit far lower than those of male athlete counterparts with similar anthropometric measures [1]. Otherwise, observational evidence from longitudinal studies is scarce and inconclusive with respect to sex differences in blood volume adaptations to ET [11, 16]. Exiguous, but more consistent results have been reported regarding cardiac structural and functional variables that may facilitate increases in stroke volume and cardiac output. Of note, cardiac adaptations seem to be enhanced with ET interventions comprising high-intensity ET and/or exercise modalities involving greater central hemodynamic loads [37,38,39,40,41,42]. A 1-year long-distance running program sex-matched by training stimuli, including high-intensity exercise, induced a less prominent increase in left ventricular (LV) mass and Frank–Starling curves in women versus men [11]. Similarly, in prepubertal children, 3 months of ET resulted in attenuated increases in LV internal chamber size in girls compared with boys, a cardiac adaptation linearly related to the effect of ET on stroke volume, cardiac output and VO2max [43]. These adaptations are coherent with cross-sectional analyses in endurance athletes [44] and population studies, in that adult sedentary women commonly present with lower LV mass and volume for a given LV filling pressure compared with body size-matched men [45, 46]. The women’s heart may thus be stiffer and less amenable to eccentric remodeling than in men [47], thus limiting central adaptations underlying VO2max trainability.
In addition to central determinants of VO2max, peripheral variables along the O2 transport and utilization chain can be hypothesized to play a role in VO2max trainability. With this regard, adaptations in systemic and skeletal muscle blood flow distribution, mitochondrial content and function might facilitate O2 extraction. Yet, the fact that O2 extraction is near peak levels at VO2max in untrained (male) individuals limits the potential contribution of peripheral adaptations to enhanced VO2max responses to ET in men relative to women [48, 49]. On the other hand, sex differences in specific peripheral adaptations such as skeletal muscle vasodilation leading to decreased systemic vascular resistance might contribute to central adaptations (augmented stroke volume) and VO2max improvement [43]. Collectively considered, further research is needed to establish the mechanisms that explain the blunted VO2max trainability in women.
4.1 Limitations and Strengths
We selected studies assessing ET interventions in healthy individuals to limit the influence of disease-related confounding factors. Further research will elucidate whether the present findings can be extrapolated to clinical populations. Second, a relatively few number of studies were included and the majority of them involved different intensities and doses of cycle ergometry ET; thus, our conclusions should be taken with caution and be primarily limited to this type of endurance exercise. Third, there might be sex differences in the lag time between ET and VO2max responses. Yet, a reduced VO2max trainability in women versus men was observed independently of the duration of ET, including in long-term studies, in that a plateau in VO2max was plausibly achieved [11, 13, 17]. Fourth, the included studies did not report comprehensive information about lifestyle factors, which could differ between untrained men and women. Future studies and meta-analyses might take lifestyle factors into account to provide far-reaching insights. Finally, the mean methodological quality of the included studies was determined as moderate-to-high and no publication bias and/or other biases were detected.
5 Conclusions
The current meta-analysis provides evidence that VO2max, a hallmark of aerobic capacity, is further improved in men compared with women healthy individuals in response to a given ET dose. The consistency of this finding against potential confounding factors suggests the presence of a sexual dimorphism regarding the main physiological adaptations determining VO2max improvement with ET. The specific mechanisms underlying sex-specific VO2max trainability are speculative at present and will have to be characterized in future experimental studies.
Data Availability Statement
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
References
Lundby C, Robach P. Performance enhancement: what are the physiological limits? Physiology (Bethesda). 2015;30(4):282–92.
Montero D, Diaz-Canestro C. Endurance training and maximal oxygen consumption with ageing: role of maximal cardiac output and oxygen extraction. Eur J Prev Cardiol. 2016;23(7):733–43.
Montero D, Diaz-Canestro C, Lundby C. Endurance training and VO2max: role of maximal cardiac output and oxygen extraction. Med Sci Sports Exerc. 2015;47(10):2024–33.
Lee DC, Artero EG, Sui X, Blair SN. Mortality trends in the general population: the importance of cardiorespiratory fitness. J Psychopharmacol. 2010;24(4 Suppl):27–35.
Mandsager K, Harb S, Cremer P, Phelan D, Nissen SE, Jaber W. Association of cardiorespiratory fitness with long-term mortality among adults undergoing exercise treadmill testing. JAMA Netw Open. 2018;1(6):e183605.
Kodama S, Saito K, Tanaka S, Maki M, Yachi Y, Asumi M, et al. Cardiorespiratory fitness as a quantitative predictor of all-cause mortality and cardiovascular events in healthy men and women: a meta-analysis. JAMA. 2009;301(19):2024–35.
Montero D, Lundby C. Refuting the myth of non-response to exercise training: ‘non-responders’ do respond to higher dose of training. J Physiol. 2017;595(11):3377–87.
Ross R, de Lannoy L, Stotz PJ. Separate effects of intensity and amount of exercise on interindividual cardiorespiratory fitness response. Mayo Clin Proc. 2015;90(11):1506–14.
Sisson SB, Katzmarzyk PT, Earnest CP, Bouchard C, Blair SN, Church TS. Volume of exercise and fitness nonresponse in sedentary, postmenopausal women. Med Sci Sports Exerc. 2009;41(3):539–45.
Rusko HK. Development of aerobic power in relation to age and training in cross-country skiers. Med Sci Sports Exerc. 1992;24(9):1040–7.
Howden EJ, Perhonen M, Peshock RM, Zhang R, Arbab-Zadeh A, Adams-Huet B, et al. Females have a blunted cardiovascular response to 1 year of intensive supervised endurance training. J Appl Physiol (Bethesda, Md: 1985). 2015;119(1):37–46.
Montero D, Madsen K, Meinild-Lundby AK, Edin F, Lundby C. Sexual dimorphism of substrate utilization: differences in skeletal muscle mitochondrial volume density and function. Exp Physiol. 2018;103(6):851–9.
Kohrt WM, Malley MT, Coggan AR, Spina RJ, Ogawa T, Ehsani AA, et al. Effects of gender, age, and fitness level on response of VO2max to training in 60–71 year olds. J Appl Physiol (Bethesda, Md: 1985). 1991;71(5):2004–11.
Carter SL, Rennie C, Tarnopolsky MA. Substrate utilization during endurance exercise in men and women after endurance training. Am J Physiol Endocrinol Metab. 2001;280(6):E898–907.
McKenzie S, Phillips SM, Carter SL, Lowther S, Gibala MJ, Tarnopolsky MA. Endurance exercise training attenuates leucine oxidation and BCOAD activation during exercise in humans. Am J Physiol Endocrinol Metab. 2000;278(4):E580–7.
Montero D, Breenfeldt-Andersen A, Oberholzer L, Haider T, Goetze JP, Meinild-Lundby AK, et al. Erythropoiesis with endurance training: dynamics and mechanisms. Am J Physiol Regul Integr Comp Physiol. 2017;312(6):R894–902.
Seip RL, Moulin P, Cocke T, Tall A, Kohrt WM, Mankowitz K, et al. Exercise training decreases plasma cholesteryl ester transfer protein. Arterioscler Thromb J Vasc Biol. 1993;13(9):1359–67.
Tarnopolsky MA, Rennie CD, Robertshaw HA, Fedak-Tarnopolsky SN, Devries MC, Hamadeh MJ. Influence of endurance exercise training and sex on intramyocellular lipid and mitochondrial ultrastructure, substrate use, and mitochondrial enzyme activity. Am J Physiol Regul Integr Comp Physiol. 2007;292(3):R1271–8.
Weber CL, Schneider DA. Increases in maximal accumulated oxygen deficit after high-intensity interval training are not gender dependent. Journal of Appl Physiol (Bethesda, Md: 1985). 2002;92(5):1795–801.
Stroup DF, Berlin JA, Morton SC, Olkin I, Williamson GD, Rennie D, et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA. 2000;283(15):2008–12.
Ross LE, Grigoriadis S, Mamisashvili L, Koren G, Steiner M, Dennis CL, et al. Quality assessment of observational studies in psychiatry: an example from perinatal psychiatric research. Int J Methods Psychiatr Res. 2011;20(4):224–34.
Higgins JPT, Green S, (editors). Cochrane handbook for systematic reviews of interventions version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. http://www.cochrane-handbook.org. Accessed Mar 2019.
DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986;7(3):177–88.
Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315(7109):629–34.
Roepstorff C, Steffensen CH, Madsen M, Stallknecht B, Kanstrup IL, Richter EA, et al. Gender differences in substrate utilization during submaximal exercise in endurance-trained subjects. Am J Physiol Endocrinol Metab. 2002;282(2):E435–47.
Roepstorff C, Thiele M, Hillig T, Pilegaard H, Richter EA, Wojtaszewski JF, et al. Higher skeletal muscle alpha2AMPK activation and lower energy charge and fat oxidation in men than in women during submaximal exercise. J Physiol. 2006;574(Pt 1):125–38.
Carrick-Ranson G, Hastings JL, Bhella PS, Shibata S, Fujimoto N, Palmer D, et al. The effect of age-related differences in body size and composition on cardiovascular determinants of VO2max. J Gerontol A Biol Sci Med Sci. 2013;68(5):608–16.
Glucksmann A. Sexual dimorphism in mammals. Biol Rev Camb Philos Soc. 1974;49(4):423–75.
Lindenfors P, Revell LJ, Nunn CL. Sexual dimorphism in primate aerobic capacity: a phylogenetic test. J Evol Biol. 2010;23(6):1183–94.
Lundby C, Montero D, Joyner M. Biology of VO2max: looking under the physiology lamp. Acta Physiol (Oxf). 2017;220(2):218–28.
Rankinen T, Wolfarth B, Simoneau JA, Maier-Lenz D, Rauramaa R, Rivera MA, et al. No association between the angiotensin-converting enzyme ID polymorphism and elite endurance athlete status. J Appl Physiol (Bethesda, Md: 1985). 2000;88(5):1571–5.
Montero D, Cathomen A, Jacobs RA, Fluck D, de Leur J, Keiser S, et al. Haematological rather than skeletal muscle adaptations contribute to the increase in peak oxygen uptake induced by moderate endurance training. J Physiol. 2015;593(20):4677–88.
Montero D, Lundby C. Regulation of red blood cell volume with exercise training. Compr Physiol. 2018;9(1):149–64.
Sawka MN, Convertino VA, Eichner ER, Schnieder SM, Young AJ. Blood volume: importance and adaptations to exercise training, environmental stresses, and trauma/sickness. Med Sci Sports Exerc. 2000;32(2):332–48.
Bonne TC, Doucende G, Fluck D, Jacobs RA, Nordsborg NB, Robach P, et al. Phlebotomy eliminates the maximal cardiac output response to six weeks of exercise training. Am J Physiol Regul Integr Comp Physiol. 2014;306(10):R752–60.
Falz R, Fikenzer S, Hoppe S, Busse M. Normal values of hemoglobin mass and blood volume in young, active women and men. Int J Sports Med. 2019;40(4):236–44.
Baekkerud FH, Solberg F, Leinan IM, Wisloff U, Karlsen T, Rognmo O. Comparison of three popular exercise modalities on VO2max in overweight and obese. Med Sci Sports Exerc. 2016;48(3):491–8.
Cornelis J, Beckers P, Taeymans J, Vrints C, Vissers D. Comparing exercise training modalities in heart failure: a systematic review and meta-analysis. Int J Cardiol. 2016;15(221):867–76.
Daussin FN, Ponsot E, Dufour SP, Lonsdorfer-Wolf E, Doutreleau S, Geny B, et al. Improvement of VO2max by cardiac output and oxygen extraction adaptation during intermittent versus continuous endurance training. Eur J Appl Physiol. 2007;101(3):377–83.
Ray CA, Cureton KJ, Ouzts HG. Postural specificity of cardiovascular adaptations to exercise training. J Appl Physiol (Bethesda, Md: 1985). 1990;69(6):2202–8.
Weston M, Taylor KL, Batterham AM, Hopkins WG. Effects of low-volume high-intensity interval training (HIT) on fitness in adults: a meta-analysis of controlled and non-controlled trials. Sports Med. 2014;44(7):1005–17.
Wisloff U, Stoylen A, Loennechen JP, Bruvold M, Rognmo O, Haram PM, et al. Superior cardiovascular effect of aerobic interval training versus moderate continuous training in heart failure patients: a randomized study. Circulation. 2007;115(24):3086–94.
Obert P, Mandigouts S, Nottin S, Vinet A, N’Guyen LD, Lecoq AM. Cardiovascular responses to endurance training in children: effect of gender. Eur J Clin Investig. 2003;33(3):199–208.
Whyte GP, George K, Sharma S, Firoozi S, Stephens N, Senior R, et al. The upper limit of physiological cardiac hypertrophy in elite male and female athletes: the British experience. Eur J Appl Physiol. 2004;92(4–5):592–7.
de Simone G, Devereux RB, Daniels SR, Meyer RA. Gender differences in left ventricular growth. Hypertension. 1995;26(6 Pt 1):979–83.
Mendes LA, Davidoff R, Cupples LA, Ryan TJ, Jacobs AK. Congestive heart failure in patients with coronary artery disease: the gender paradox. Am Heart J. 1997;134(2 Pt 1):207–12.
Regitz-Zagrosek V, Kararigas G. Mechanistic pathways of sex differences in cardiovascular disease. Physiol Rev. 2017;97(1):1–37.
Lundby C, Sander M, van Hall G, Saltin B, Calbet JA. Maximal exercise and muscle oxygen extraction in acclimatizing lowlanders and high altitude natives. J Physiol. 2006;573(Pt 2):535–47.
Rud B, Foss O, Krustrup P, Secher NH, Hallen J. One-legged endurance training: leg blood flow and oxygen extraction during cycling exercise. Acta Physiol (Oxf). 2012;205(1):177–85.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
David Montero is funded by the Discovery Grant from the Natural Sciences and Engineering Research Council of Canada (NSERC) (Grant no. RGPIN-2019-04833). Candela Diaz-Canestro is the recipient of the Early Postdoc Mobility Grant from the Swiss National Foundation (SNF). No specific sources of funding were used to assist in the preparation of this article.
Conflict of interest
David Montero and Candela Diaz-Canestro declare that they have no conflicts of interest relevant to the content of this review.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Diaz-Canestro, C., Montero, D. Sex Dimorphism of VO2max Trainability: A Systematic Review and Meta-analysis. Sports Med 49, 1949–1956 (2019). https://doi.org/10.1007/s40279-019-01180-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40279-019-01180-z