
Abstract
Resistance training is essential for health and performance and confers many benefits such as increasing skeletal muscle mass, increasing strength and power output, and improving metabolic health. Resistance training is a major component of the physical activity guidelines, yet research in female populations is limited. Recent increases in the promotion of, and the participation by, females in sport and exercise, highlight the need for an increase in understanding of evidence-based best practice exercise prescription for females. The aim of this review is to provide an overview of the current research regarding resistance training performance and skeletal muscle adaptation in females, with a focus on the hormonal variables that may influence resistance training outcomes. Findings suggest that the menstrual cycle phase may impact strength, but not skeletal muscle protein metabolism. In comparison, oral contraception use in females may reduce skeletal muscle protein synthesis, but not strength outcomes, when compared to non-users. Future research should investigate the role of resistance training in the maintenance of skeletal muscle protein metabolism during pregnancy, menopause and in athletes experiencing relative energy deficiency in sport. The review concludes with recommendations for researchers to assist them in the inclusion of female participants in resistance training research specifically, with commentary on the most appropriate methods of controlling for, or understanding the implications of, hormonal fluctuations. For practitioners, the current evidence suggests possible resistance training practices that could optimise performance outcomes in females, although further research is warranted.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Females performing resistance training achieve similar relative strength and hypertrophy gains compared to males and may be able to optimise performance or muscle adaptation by emphasising training frequency during the follicular phase of the menstrual cycle, or with combined strength/power training throughout the cycle. |
The oral contraceptive pill, but not the menstrual cycle, may negatively influence skeletal muscle protein turnover in response to resistance training. Further evidence is needed to determine the influence of endogenous and exogenous estrogen, and other key hormones, on resistance training outcomes in young females. |
Researchers are encouraged to include female cohorts in resistance training research, and a number of strategies could be employed to ensure they investigate a homogenous cohort or control for potentially confounding variables. |
1 Introduction
The increasing development of and investment in women’s professional sporting leagues represents an important platform for promoting physical activity and exercise in the female population [1, 2]. However, research that informs practitioners of best-practice methods for maximising exercise performance and training adaptation in females is limited. In the top-ranked ‘sport science’ category journals, 39% of study participants are female, but only 4–13% of participant groups in original research are made up of females only [3]. This suggests that a large proportion of the exercise prescription information for females is based on research conducted in males. Hence, there is a need to better understand the exercise and training outcomes for physically active females and female athlete populations [3, 4]. Understanding the outcomes of exercise for females is critical for exercise professionals and coaches to appropriately prescribe training. The ability to implement exercise training interventions that are specifically designed to optimise females’ performance and health will transform the sport and health sector with an evidence-based approach for females aspiring to reach fitness and health goals.
Resistance training is a critical component of an athlete’s training programme to improve skeletal muscle strength and power, reduce the likelihood of injury and rehabilitate any injuries [5]. Further, the idea that ‘resistance training is medicine’ is now well established [6], with recent high-impact reviews highlighting the benefits of resistance training for increasing skeletal muscle mass [7] and reversing skeletal muscle loss [8], reducing body fat [9], improving cardiovascular [10], metabolic [11] and mental [12] health, and promoting physical function and strength [13]. The maintenance of skeletal muscle mass preserves or improves the health and functional capacity of skeletal muscle. Skeletal muscle cells are made up of ~ 80% proteins [14, 15] and skeletal muscle mass is regulated by the balance between the rate of protein synthesis and the rate of protein degradation in the muscle [15]. Resistance exercise stimulates contraction- and hormone-induced signalling pathways that upregulate skeletal muscle protein synthesis in the cell [7]. Acute increases in muscle protein synthesis after resistance exercise translate to the adaptive hypertrophic response to long-term resistance training [16]. Therefore, skeletal muscle protein metabolism underpins the benefits of resistance training in improving short- and long-term health and performance.
The relationship between resistance training and skeletal muscle adaptation has received substantially less attention in females than in males. This relative lack of research in females is mostly owing to researchers’ reluctance to account for the additional variability in dependent variables that is created by factors that are unique to females, such as the menstrual cycle, pregnancy, breastfeeding, hormonal contraceptives, or menopause [4]. However, it is the complexity of the female biological and physiological systems that makes research in this population so important. Researchers need to understand the interplay between these systems and decide how best to account for their interaction in their study designs so they can accurately forecast training implications for the wider female exercise community [4]. Therefore, the aim of this review is to outline key considerations for resistance training research conducted with females. The review first presents a brief overview of the performance outcomes and skeletal muscle adaptations that result from resistance training in females. Thereafter, the unique variables that may influence resistance training outcomes in females are discussed. Finally, a summary of the practical implications for researchers conducting resistance training studies with female cohorts, and for practitioners training female clients or athletes, is presented.
2 Sex Differences in Resistance Training Performance and Skeletal Muscle Adaptation
As in many aspects of sport performance, sex differences exist in muscle strength and adaptation to resistance training. Males demonstrate up to 157% greater relative upper and 60% greater relative lower body strength, respectively, than females in resistance exercise tests such as one repetition maximum (1 RM) testing [17]. Females also demonstrate 73% greater relative lower body strength compared to their upper body strength, yet this difference in relative muscle group strength is not observed in males [17]. In contrast, females demonstrate approximately twofold lower muscle fatigability [18]. Studies that have tested relative strength at 20–70% of maximum voluntary contraction report 46–87% greater fatigue resistance in females in comparison to males [19]. However, the advantage females hold over males in fatigability may dissipate at intensities beyond 80% 1 RM [19]. Additionally, females training at the same relative workload (i.e. an equal volume at a given percent of 1 RM) as males need less recovery time for force return both immediately post-exercise and over 24 h [18, 20, 21]. These differences may be explained by sex-specific lean body mass distribution, or by the greater proportion of type I muscle fibres in females that are more resistant to fatigue than type IIa and IIx muscle fibres [22].
While various sex differences exist in skeletal muscle strength and structure, several established resistance training methods for increasing muscle strength and hypertrophy are equally valid for both males and females. In trained males and females, multiple-set training is superior to single-set training [23, 24] and exercise sequence dictates the volume load output for each exercise performed in a training session [25, 26]. It follows that the relative performance adaptation (e.g. relative increased maximal strength output) to long-term resistance training is similar between males and females performing the same resistance training protocols. With up to 20 weeks of the same resistance training protocol, relative percentage strength increases from baseline are similar in males and females [27,28,29], and sometimes up to 10% greater in females [30, 31]. Nevertheless, while males and females may respond similarly to resistance training protocols for developing strength, albeit females at a lower absolute load, there may be optimal training approaches to maximise performance adaptations in females [32, 33].
Understanding how females can most effectively make improvements in strength is not only relevant to health and performance, but also to certain occupational circumstances whereby a minimum standard must be met, e.g. strength requirements for military personnel. Females performing combined strength and power training may make greater relative improvements compared with their male counterparts as judged in multi-joint exercises such as the 1-RM squat, 1-RM bench press, and 1-RM high pull, when compared with six months of combined strength and hypertrophy training [32]. Low-volume high-intensity training, typical of strength or power but not hypertrophy training, may therefore be most suitable for strength adaptations in female participants [32]. Certainly, there may be an upper threshold for the volume of resistance training (i.e. sets per muscle group) performed by trained females to achieve optimal muscle hypertrophy and strength gains [33]. Some authors have proposed that females may have a greater capacity for neural adaptations over hypertrophic adaptations [34,35,36], which could explain these findings. While neural adaptations are beyond the scope of this review, it is important to consider that strength develops through a combination of neural, structural and hypertrophic adaptations [36].
Muscle protein synthesis is a primary component of the skeletal muscle anabolic response following resistance exercise [16]. Muscle protein synthesis increases similarly in females and males in the immediate 1- to 5-h post-resistance training and remains elevated, compared with resting levels, up to 26 h post-training with feeding [37]. In their study, West et al. [37] disregarded the female menstrual cycle in their protocol because of previous findings that skeletal muscle protein metabolism is not influenced by the menstrual cycle phase (discussed in Sect. 3.1) [38]. Their findings are perhaps unsurprising, given that males and females express similar basal protein synthesis and protein degradation rates in skeletal muscle, when normalised to lean mass [39]. This lack of difference in skeletal muscle protein synthesis rates [37] is in line with the frequent observation that relative increases in muscle cross-sectional area with long-term resistance training are similar in males and females [31, 40]. This suggests that sex differences in lean muscle mass and absolute strength and hypertrophy across the lifespan [28, 41, 42] may be driven by other mechanisms, including mechanical (e.g. sarcomerogenesis) or metabolic stress (e.g. elevated hormone release) [43]. Based on the known sex differences in circulating hormone levels, the following section examines the role that anabolic and catabolic hormones may play in females’ responses to resistance training.
3 Hormonal Factors Influencing the Resistance Training Response and Adaptation in Females
The hormonal environment, both basal and exercise induced, is one of several key mechanisms for resistance training adaptation. A bout of resistance exercise triggers the secretion of specific hormones, which engage with their receptors on or within the target cell [44]. These ligand-receptor interactions initiate a cascade of events, leading to specific physiological outcomes such as an increase in muscle protein synthesis [44]. The following sections discuss how hormones, both endogenous and exogenous (e.g. hormonal contraceptives), may affect skeletal muscle protein metabolism and adaptation to training.
3.1 Endogenous Sex Hormones and the Menstrual Cycle in Young Females
Estrogens and androgens are groups of endogenous sex hormones that are produced by both males and females [44]. Testosterone is the most abundant androgen hormone [45]. By binding the androgen receptor at the surface of the muscle fibre, testosterone increases intracellular calcium release and activates the pathways that promote muscle protein synthesis [46] while inhibiting the pathways that promote muscle protein degradation [47]. Testosterone also stimulates growth hormone (GH) secretion [45]. The level of testosterone found in females is about 10% of that in males [45, 48]. In males, resistance exercise triggers the release of testosterone [45, 49]. The resulting elevated anabolic environment may promote skeletal muscle hypertrophy [50], potentially by enhancing androgen receptor content [51], a key factor driving relative increases in skeletal muscle hypertrophy in males [52]. In females, the exercise-induced testosterone response is limited, with most studies finding no testosterone response post-resistance exercise [49, 53,54,55]. Androgen receptor protein content in females is however upregulated at a faster rate than in males following an acute bout of resistance exercise [48]. This upregulation is not sufficient to counteract females’ low baseline level of testosterone, nor does testosterone fluctuate across the menstrual cycle [56]. Consequently, females have little opportunity to capitalise on the anabolic effects of testosterone and, in addition to the intrinsic (e.g mechanical loading) and extrinsic (e.g. protein ingestion) factors, must rely on other sex and non-sex hormones to increase skeletal muscle protein synthesis.
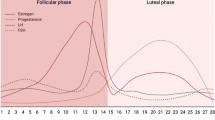
Estrogen and progesterone are two primary sex hormones that fluctuate with, and regulate, the menstrual cycle. Approximately 50% of both active and elite female athletes perceive that their menstrual cycle affects their exercise training and performance [57]. The menstrual cycle is part of the human reproductive process and is made up of two phases: the follicular phase, which is characterised by the onset of menses, and the luteal phase, which is characterised by the onset of ovulation (Fig. 1) [58]. From the early- to mid-follicular phase, estrogen and progesterone levels are low, with a spike in estrogen occurring during the late-follicular phase, meaning that the ratio of estrogen to progesterone is at its largest [58, 59]. Following ovulation, both progesterone and estrogen levels are high before decreasing again prior to menses (Fig. 1) [58, 59].

Hormonal fluctuation with a eumenorrheic menstrual cycle (based on a 28-day cycle with ovulation occurring at day 14). EF early follicular, EL early luteal, LF late follicular, LL late luteal, MF mid-follicular, ML mid-luteal
The possible implications of the surge in estrogen during the late-follicular phase on resistance training performance are evident from findings that maximal force is increased from the follicular phase to ovulation and declines in the early to mid-luteal phase [60,61,62]. The area under the curve of estradiol (the most abundant estrogen) increases for 65–95 min following an acute bout of resistance exercise, but substantially more so in the luteal phase compared with the follicular phase [63, 64]. Estradiol then remains up to 21% higher than resting levels at 24 h post-resistance exercise [65]. Long-term resistance training studies support a possible causal relationship between the heightened estrogen-progesterone ratio and performance, with greater muscle diameters and strength observed with up to 4 months of resistance training performed frequently in the follicular phase (e.g. five times per week in the follicular phase and two times per week in the luteal phase) compared with training performed frequently in the luteal phase or consistently (e.g. three times per week) throughout the cycle [66,67,68]. Interestingly, each of these training studies used a lower body hypertrophy protocol of 8–12 repetitions at ~ 80% 1 RM, with appropriate overload progressively implemented. In contrast, one study found no effect of menstrual cycle-based training frequency on strength or hypertrophy using an upper body protocol [69]. Importantly, while Wikstrom-Frisen et al. [66] included a control group who trained with constant frequency throughout the menstrual cycle, each of the studies discussed had a number of limitations in their design or implementation, indicating that the results should be taken with caution. Further research is needed to understand how menstrual cycle-based periodisation for hypertrophy training could be a feasible approach for females performing resistance training.
Several authors have suggested that estrogens may influence skeletal muscle hypertrophy [42, 70, 71]. When bound to its receptors, estrogen upregulates intracellular signalling pathways that stimulate skeletal muscle protein synthesis, such as the Akt/mechanistic target of rapamycin pathway (mTOR) [72]. Circulating estrogen enhances myoblast proliferation in vitro [73] and muscle size in rodents in vivo [74]. Estrogen may also play a key role in muscle repair and regeneration through the activation and proliferation of satellite cells [75, 76]. The administration of estrogen might reduce protein catabolism in males [77] and post-menopausal females [78]. Hormone replacement therapy using an estrogen-only [79] or combined estrogen-progesterone [80, 81] supplement in post-menopausal females has demonstrated increases in muscle mass and/or strength, possibly owing to an increase in estradiol by up to 50% with supplementation [80, 81]. Multiple comprehensive reviews detail the impact of estrogen on the skeletal muscle of early- and post-menopausal females [42, 70, 71], which may be relevant in understanding the role of estrogen in young females. However, it is also important to consider that the reduction in muscle strength in the early-mid luteal phase (i.e. post-ovulation) coincides with reduced maximal motor unit discharge rates, which may be influenced by the drop in estrogen and increase in progesterone in this phase [82]. Certainly, the effects of estrogen on skeletal muscle are promising, yet there remains a need to determine how young females (i.e. of menstruating age) performing resistance training can exploit naturally occurring surges in endogenous estrogen to maximise skeletal muscle strength and hypertrophy.
Progesterone may also play a role in skeletal muscle metabolism. Progesterone increases immediately following resistance exercise in the mid-luteal phase, but not in the early-follicular phase, and remains elevated up to 30 min post-resistance exercise [64]. Smith et al. [83] found that progesterone administration increases skeletal muscle protein synthesis rate, albeit in post-menopausal sedentary females. In contrast, some authors propose a catabolic effect of progesterone [84,85,86]. Landau and Poulos [86] reported that a large dose of progesterone (equivalent to that excreted in the first trimester of pregnancy) is associated with reduced serum amino acid levels, indicating an increase in protein degradation. To date, only one study of young females has tested protein myofibrillar rates following a resistance exercise session performed in the follicular and luteal phases of the menstrual cycle, with no difference found between phases [38]. Importantly, Miller et al. [38] conducted testing in the early-follicular phase and the early- to mid-luteal phase, when the ratio of estrogen to progesterone secretion is small. It has been suggested that the individual effects of endogenous progesterone and estrogen may counteract each other when produced at a similar rate [42]. The estrogen-progesterone ratio is largest (i.e. the difference between estrogen and progesterone secretion is large) during the late-follicular phase [58, 59]. Importantly, emphasising training frequency during the follicular phase coincides with greater strength and hypertrophy improvements over time [66,67,68]. Therefore, resistance exercise in the late-follicular phase of the menstrual cycle could potentially promote greater skeletal muscle protein synthesis than in other phases. Previous authors have highlighted that research is needed to compare muscle protein synthesis rates between the early and late follicular phases to understand the effect of estrogen independent of progesterone [42]. However, until research in this space is available, we have recommended (Sect. 5) for researchers to avoid exercise testing in the late-follicular phase because of potential changes in strength or muscle protein synthesis rates. These recommendations also warrant further research.
3.2 Endogenous Non-Sex Hormones in Young Females
Growth hormone (GH), insulin-like growth factor 1 (IGF-1) and cortisol are non-sex hormones that play an important role in resistance training-induced skeletal muscle protein metabolism [37, 87]. Growth hormone regulates carbohydrate, lipid and protein metabolism in a number of tissues, with a key role in promoting the release of IGF-1 from the liver [88]. In turn, IGF-1 directly upregulates skeletal muscle protein synthesis by activating the PI3k/Akt/mTOR pathway [88]. Resistance exercise stimulates large bursts of GH in males and females [89]. However, there is mixed evidence to support a correlation between the acute resistance exercise-induced GH response with the magnitude of muscle hypertrophy in males [54, 89,90,91]. Interestingly, the area under the curve for GH-levels post-resistance exercise is greater in females than in males [37]. Further, the GH response in females is greater with high-volume short-rest resistance exercise compared with a low-volume high-rest prescription [54, 89, 92]. While basal GH and IGF-1 remain stable across the menstrual cycle [93], there is evidence that resistance training-induced GH secretion is greater during the mid-luteal phase than the early follicular phase [63, 64]. Despite a greater acute increase in circulating GH after resistance exercise in the mid-luteal phase compared with the early follicular phase, emphasising training frequency during the luteal phase does not result in greater increases in hypertrophy or strength over time [66]. Authors have suggested that this increased GH production during the luteal phase may arise from greater circulating estradiol because estrogen plays a role in GH axis neuro-regulation in both rodents and humans [94]. Growth hormone secretion also increases following hormone (estrogen) replacement therapy in post-menopausal females [95]. Further research is needed to determine if the peak of estrogen during the late-follicular phase may stimulate greater resistance exercise-induced GH, which could promote greater training adaptations during this phase.
In contrast to the anabolic hormones discussed so far, cortisol is a catabolic hormone that, among other roles, is upregulated in response to psychological and physiological stress [96]. Stress induced at the whole-body level and the skeletal-muscle level with resistance training can elicit an increase in cortisol [54]. In turn, supraphysiological levels of cortisol increase skeletal muscle protein degradation, as well as markers of protein degradation, in both human and rodent muscle cells [97, 98]. Further, findings demonstrate that cortisol decreases muscle protein synthesis in humans [99] and that a mix of catabolic hormones including cortisol increases muscle protein breakdown in humans [100]. The secretion of cortisol in response to resistance exercise is similar between males and females [37]. While it is unclear whether cortisol secretion remains consistent across the menstrual cycle [56, 101] or increases in the luteal/ovulatory phase [102], rodent models suggest that cortisol is downregulated by testosterone [103] and stimulated by estrogen [104]. Given that females secrete little, if any, testosterone in response to resistance exercise, these rodent models may explain why only males show a cortisol adaptation to long-term training [27] with a reduction in baseline serum levels that may aid their hypertrophic adaptation. Further research is needed to determine if an increase in cortisol with estrogen during the luteal phase [102] might counteract the beneficial GH profile during this phase [63, 64] and explain females’ greater adaptation to resistance training performed in the follicular phase [66,67,68].
3.3 Hormonal Contraceptive Use
Another consideration for researchers and practitioners is hormonal contraceptive use. Many females use hormonal contraception to regulate their menstrual cycle or prevent pregnancy [105]. Hormonal contraceptives include the contraceptive pill, implant rod, contraceptive patch, progestogen injection, vaginal ring and the hormonal intrauterine device (IUD). While the most common methods for contraception vary regionally, use of oral contraceptive (OC) pills is more prevalent than other methods in Australia whereas the IUD is more commonly used in European countries compared with other countries [106]. Studies conducted in the USA and Norway indicate that hormonal contraceptive use is particularly common amongst athletes, with up to 57% of female athletes using OC [107, 108] and 9% using an IUD [107]. The hormonal IUD (a progestogen-only device) has been shown to reduce muscle mass after 12 months [109]; however, confounding variables such as age and physical activity were not considered in the analyses. No other evidence exists regarding the effect of the IUD or implant rod on skeletal muscle strength, hypertrophy or protein metabolism with resistance training. In contrast, the combined OC pill, the most common form of OC, is more widely researched. The combined OC pill contains a synthetic estrogen (ethinylestradiol) and one of six synthetic progestogens [110]. The combined OC pill is also split into four generations dependent on their type of progesterone [111]. The OC pill reduces endogenous estrogen, progestogen and testosterone [110, 112] to low but consistent levels. Therefore, the level of circulating sex steroids is dependent on the dose of synthetic hormones delivered in each OC pill. The dose of synthetic hormone differs between monophasic, biphasic and triphasic OC, as well as the brand of pill [110]; a US study of female participants using OC pills found 67% used a monophasic pill and 88 different brands of OC pills were reportedly used [111]. As such, there may be a large variation in hormonal fluctuations between individuals taking the OC pill that could impact skeletal muscle strength, hypertrophy and protein metabolism.
Despite, or perhaps because of, potential hormonal variation, no differences in maximal strength have been found between resistance-trained females with or without OC during acute performance tests [113] or following up to 4 months of resistance training [66, 114]. Maximal strength is also unaffected by differences in monophasic OC androgenicity (i.e. the dose of synthetic progestogen), tested at various stages of the menstrual cycle [115]. Further, maximal strength does not differ during each phase of the OC cycle itself (including five brands of combined monophasic OC) [113, 115]. Interestingly, OC use increases sex hormone-binding globulin (more so in third- and fourth-generation OC pills), which has a high affinity for testosterone, binding it and making it inactive [112]. Further, OC administration may also increase GH levels but decrease IGF in second- and fourth-generation OC pills [116, 117]. A down-regulation of anabolic hormones could possibly play a role in changes in skeletal muscle protein balance with ingestion of OC pills. In support of this theory, the myofibrillar protein fractional synthesis rate was lower in female third-generation, but not second-generation, OC users compared with non-OC users following prolonged submaximal resistance exercise [118]. In this study, Hansen et al. [118] tested second- and third-generation OC users during days 18–21 of the pill cycle and non-OC users during days 3–6 of menstruation, therefore exposing all participants to low endogenous estradiol and progesterone, and highlighting the influence of high exogenous hormone levels on skeletal muscle protein synthesis. Interestingly, the authors suggest that the inhibiting effect of third-generation OC pills on myofibrillar protein synthesis may be due to the greater progesterone level compared with second-generation OC pills [118, 119]. However, this hypothesis and how it relates to muscle hypertrophy needs further research.
Collectively, the studies discussed have used a myriad of OC formulations, and it is therefore difficult to interpret the true impact of OC use on resistance training and skeletal muscle outcomes. Further, muscle protein metabolism in males is influenced by training status [120], therefore investigating the interaction between training status and OC is warranted. Research comparing the type, composition or generation of OC is needed to reliably understand the outcomes for female OC users performing resistance training.
4 Future Directions
Whilst the research investigating the interaction between resistance training and skeletal muscle protein metabolism in females is sparse, the different stages of the lifespan have hardly been considered. While the heavy resistance training typically performed by elite or recreational athletes is contraindicated during pregnancy, athletes who are pregnant or postnatal need specific exercise guidelines [121]. Estrogen and progesterone production markedly increase during pregnancy, and then rapidly decline in the immediate post-partum period [122]. Interestingly, acute maximal strength does not change in untrained females between trimesters, nor between in vitro fertilisation phases [123]. As low- to moderate-intensity resistance training is indicated during pregnancy and postpartum periods, further research is needed to understand the implications of hormonal changes on resistance exercise outcomes and skeletal muscle protein metabolism during these stages of life.
In contrast to pregnancy and the postnatal period, menopause is characterised by a reduction in estrogen by up to 67% and an accelerated loss of skeletal muscle mass by up to 1% per year after the onset of menopause [71, 124]. Acute muscle strength is lost during and after menopause; however, resistance training can attenuate this loss in strength and muscle mass [80, 124]. Notably, post-menopausal females have a faster post-absorptive muscle protein synthesis rate than pre-menopausal females over a 5-h period [83], although this response is reduced with feeding [125]. The upregulation of catabolic gene expression in post-menopausal females (without hormone replacement therapy) [83] may explain the loss of muscle mass despite upregulated basal muscle protein synthesis. However, this hypothesis, as well as the role of resistance training in contributing to protein synthesis rates in post-menopausal females, requires further research. Understanding the outcomes associated with hormone replacement therapy in this population will also contribute to increasing our knowledge of the role of hormones in the maintenance of skeletal muscle mass in females in general.
Relative energy deficiency in sport (RED-S) is another potential concern for female athletes. RED-S is characterised by, but not limited to, impaired metabolic rate, muscle protein synthesis, menstrual function, bone health and immunity caused by relative energy deficiency [126]. Emerging literature suggests that the physiological impairments associated with RED-S may negatively impact muscle strength [126]. One study demonstrated that females with menstrual disturbances (i.e. low estradiol and progesterone) have an attenuated GH response to an acute bout of resistance exercise [64]. Further research is needed to understand the implications that an impaired anabolic hormone response may have on muscle protein synthesis. RED-S can develop from a reduction in energy intake, an increase in training load (intensity and/or volume), or a combination of both factors [126]. Athletes experiencing RED-S may therefore benefit from menstrual cycle-based periodised resistance training, given findings showing that when resistance training volume (frequency) is increased for 2 weeks during either the follicular or luteal phase, sex or other hormones such as cortisol and GH are not impaired [127]. Certainly, further research is needed to identify training methods that maximise performance and reduce negative exercise-related health problems in female athletes.
5 Implications for Research on Resistance Training in Females
Including female participants in resistance training research is essential to establish the associated health and performance outcomes for the female population. Additionally, there are some occupational settings, such as military positions or emergency services, where the physical strength requirements for males and females are equal [128], thus understanding the training outcomes for both sexes is critical. The following sections provide practical suggestions for researchers wanting to include females in research investigating the effect of resistance training. These suggestions may also be useful for researchers including female participants in other exercise physiology domains.
-
It should first be determined whether the anticipated primary outcome is likely to be sex dependent and/or menstrual cycle dependent. Examples from this review show that some adaptations to strength training are influenced by the menstrual cycle, such as strength output [66, 67]. Other findings imply no change in muscle protein synthesis with menstrual cycle phase [38] but given that this was measured at only two time points, and not around ovulation, these findings should be taken with caution. When in doubt or if a pilot study cannot be performed, it is safe to assume that the primary outcome may be sex dependent and/or menstrual cycle dependent. While some sex differences are apparent (e.g. absolute strength, fatigability), researchers should remain confident that female and male participants who perform the same resistance training protocol are likely to have a similar relative acute muscle protein synthesis response to training along with similar relative hypertrophy and strength adaptation. For sex comparisons, it is therefore recommended that researchers present strength, hypertrophy and skeletal muscle protein metabolism data in relative values (i.e. the change from baseline) rather than absolute values.
-
As best practice for both male and female cohorts, in a range of research domains, it is also important to consider and implement eligibility criteria specifying participants’ training status and stage of growth across the lifespan (i.e. pubescent, young, pregnant, pre-menopausal, post-menopausal) to ensure a homogenous sample.
-
The menstrual cycle typically ranges from 25 to 34 days [58]. Regardless of the duration of the intervention, researchers should collect a menstrual diary for at least two complete cycles prior to testing. This way, researchers can appropriately schedule laboratory visits or, when possible, moderate findings for hormonal variations across the cycle. Similarly, the menstrual diary should be completed for at least one cycle during and post-intervention, which will allow research teams to confirm the timing of particular testing sessions, relative to the menstrual cycle, and therefore contextualise unexpected individual findings. When possible, menstrual records should be supplemented by venous blood collection, urinary collection, or basal body temperature monitoring at key time points across the menstrual cycle and pre/post-intervention. For example, ovulation is expected to occur at or shortly following the nadir of basal body temperature, which is then followed by a steep rise in basal body temperature [129]. Measuring body temperature at waking each morning can be used to track this pattern.
-
Importantly, the type of analyses required to moderate for hormone levels would only be possible in large studies with enough female participants with outcomes measured at different stages of the cycle, which greatly exceeds the typical cohort size used in laboratory-based exercise physiology research.
-
While a homogenous sample is preferable, when testing both eumenorrheic and OC-using females, endogenous estrogen and progesterone levels in the early follicular phase are low for both groups and can therefore be considered alike when testing in this phase of the menstrual cycle [130]. Previous authors [110, 130] have recommended that inclusion criteria for OC users should be limited to a single brand, type and generation of OC to reduce hormonal variation. However, this approach is considered difficult to practically implement given the wide range of OC brands used by females. Therefore, it is recommended that for OC and other contraceptive methods, that researchers control for a single type of contraception (e.g. monophasic OC or hormonal IUD) and set limits about the acceptable dosage of synthetic progesterone and/or estradiol, which will in turn limit the number of brands included. While not the perfect approach, this may be a practical strategy to account for exogenous and endogenous hormone production between participants.
-
For ‘acute interventions’, with a duration less than one phase (i.e. 4 days):
-
The ideal approach is a cross-over design where each participant acts as her own control and all interventions are tested during the same phase of the cycle.
-
When a cross-over design is not possible, all women should be tested in the same stage of their menstrual cycle.
-
When neither option is available, it is recommended that participants are tested during the early follicular and mid-late luteal phase when the ratio between estrogen and progesterone is small (see Sect. 3.1 for background detail).
-
-
For non-acute interventions, with a duration less than one complete cycle:
-
If feasible, we recommend using a cross-over design where each participant acts as their own control and to follow the recommendations above.
-
When not possible to use a cross-over design, the start of the intervention should occur in the same phase for each participant. The ovulation phase should be avoided to rule out the potential impact of excessive differences in the oestrogen/progesterone ratio.
-
-
For long-term interventions, with a duration of more than one complete cycle:
-
Intervention testing, as well as pre- and post-intervention testing, should start in the same phase for each participant. The ovulation phase should be avoided to rule out the potential impact of excessive differences in the estrogen/progesterone ratio.
-
6 Practical Implications for Resistance Training in Females
While females and males performing the same resistance training protocols may have similar skeletal muscle protein synthesis responses [37] and performance adaptations [27,28,29], the differences in hormonal responses to resistance exercise suggest that there may be ways to optimise the training adaptations for females performing resistance training. The following points provide a summary of the current evidence for practitioners prescribing resistance training for female populations.
-
Females may acquire strength more efficiently with low-volume high-intensity training (i.e. combined strength and power training) as opposed to high-volume moderate-intensity training (i.e. combined strength and hypertrophy training) [32]. However, high-volume moderate-intensity training elicits a greater GH response than low-volume high-intensity training in females, which may be more beneficial for obtaining hypertrophy goals [89]. While the nuances of the response may differ, these recommendations are the same as for males.
-
Females may also achieve greater strength and hypertrophy gains by training with high frequency in the follicular phase of their menstrual cycle (e.g. five times per week in the follicular phase and two times per week in the luteal phase), compared to training with a high frequency in the luteal phase or with constant frequency throughout the entire menstrual cycle (e.g. three times per week) [66, 67]. This 2-week high-frequency training approach may be more feasible to implement for recreationally active females or individual sport athletes rather than team sport athletes whose menstrual cycles are unlikely to be synchronised with their team mates.
-
Use of OC has been shown to have no impact on skeletal muscle strength [113] and no published data exist regarding the interaction between OC and muscle hypertrophy. Further research is needed to determine the impact of specific types and brands of OC on skeletal muscle adaptations. Importantly, the use of OC may have other performance-related benefits including the reduction of premenstrual symptoms that could negatively impact performance [105].
-
Ultimately, it is important that females are provided with individualised and periodised resistance training programmes that consider their menstrual cycle and hormonal contraceptives, as well as amenorrhea, pregnancy or menopause, for optimal results wherever practical. The demand for female-specific programming is evident, with mobile applications that are supported by national sporting bodies already developed to provide females with personalised training recommendations tailored to their own menstrual cycle. Coaches and athletes are advised to consider periodising training using menstrual cycle data (i.e. from mobile applications) or by autoregulation, whereby athletes progressively overload resistance exercises based on how they feel on a daily or weekly basis [131].
7 Conclusions
This review has highlighted important differences in the resistance training performance, adaptation and skeletal muscle protein response to training between males and females, and amongst different female populations (Table 1). The findings have highlighted where researchers need to be vigilant to limit confounding physiological variables between and within female participants. However, the authors also caution against only testing female participants when endogenous or exogenous hormone levels are low and/or similar. Rather, it is important for future research to also investigate female participants across a range of time points (in the menstrual cycle, across stages of life), to understand the impact of hormonal variation on resistance exercise performance and skeletal muscle adaptation. The current landscape that encourages women’s participation in recreational and elite exercise programmes demands an equal input from researchers into female exercise, health and performance. The authors advocate for researchers to invest in rigorous research that advances the current exercise prescription and training outcomes for females performing resistance training.
References
European Commission. Gender equality in sport: proposal for strategic actions 2014–2020. https://ec.europa.eu/sport/news/2014/gender_equality_sport_en. Accessed 28 May 2019.
International Working Group on Women and Sport, WomenSport International. Women, gender equality and sport. New York (NY), 2007. http://www.un.org/womenwatch/daw/public/Women%20and%20Sport.pdf. Accessed 28 May 2019.
Costello JT, Bieuzen F, Bleakley CM. Where are all the female participants in sports and exercise medicine research? Eur J Sport Sci. 2014;14(8):847–51. https://doi.org/10.1080/17461391.2014.911354.
Bruinvels G, Burden RJ, McGregor AJ, Ackerman KE, Dooley M, Richards T, et al. Sport, exercise and the menstrual cycle: where is the research? Br J Sports Med. 2017;51(6):487–8.
Suchomel TJ, Nimphius S, Stone MH. The importance of muscular strength in athletic performance. Sports Med. 2016;46(10):1419–49. https://doi.org/10.1007/s40279-016-0486-0.
Westcott WL. Resistance training is medicine: effects of strength training on health. Curr Sports Med Rep. 2012;11(4):209–16. https://doi.org/10.1249/JSR.0b013e31825dabb8.
Marcotte GR, West DWD, Baar K. The molecular basis for load-induced skeletal muscle hypertrophy. Calcif Tissue Int. 2015;96(3):196–210. https://doi.org/10.1007/s00223-014-9925-9.
Phillips SM. Nutritional supplements in support of resistance exercise to counter age-related sarcopenia. Adv Nutr. 2015;6(4):452–60. https://doi.org/10.3945/an.115.008367.
Clark JE, Goon DT. The role of resistance training for treatment of obesity related health issues and for changing health status of the individual who is overfat or obese: a review. J Sports Med Phys Fit. 2015;55(3):205–22.
Cornelissen VA, Fagard RH, Coeckelberghs E, Vanhees L. Impact of resistance training on blood pressure and other cardiovascular risk factors: a meta-analysis of randomized, controlled trials. Hypertension. 2011;58(5):950–8. https://doi.org/10.1161/hypertensionaha.111.177071.
Strasser B, Pesta D. Resistance training for diabetes prevention and therapy: experimental findings and molecular mechanisms. Biomed Res Int. 2013;2013:805217. https://doi.org/10.1155/2013/805217.
O’Connor PJ, Herring MP, Caravalho A. Mental health benefits of strength training in adults. Am J Lifestyle Med. 2010;4(5):377–96. https://doi.org/10.1177/1559827610368771.
Kraemer WJ, Ratamess NA, French DN. Resistance training for health and performance. Curr Sports Med Rep. 2002;1(3):165–71.
Vandenburgh HH, Sheff MF, Zacks SI. Chemical composition of isolated rat skeletal sarcolemma. J Membr Biol. 1974;17(1):1–12.
Millward DJ, Garlick PJ, Nnanyelugo DO, Waterlow JC. The relative importance of muscle protein synthesis and breakdown in the regulation of muscle mass. Biochem J. 1976;156(1):185–8.
Damas F, Phillips S, Vechin FC, Ugrinowitsch C. A review of resistance training-induced changes in skeletal muscle protein synthesis and their contribution to hypertrophy. Sports Med. 2015;45(6):801–7. https://doi.org/10.1007/s40279-015-0320-0.
Monteiro ER, Brown AF, Bigio L, Palma A, dos Santos LG, Cavanaugh MT, et al. Male relative muscle strength exceeds females for bench press and back squat. J Exerc Physiol Online. 2016;19(5):79–85.
Martinez-Aranda LM, Fernandez-Gonzalo R. Effects of inertial setting on power, force, work, and eccentric overload during flywheel resistance exercise in women and men. J Strength Cond Res. 2017;31(6):687–97. https://doi.org/10.1519/JSC.0000000000001635.
Hicks AL, Kent-Braun J, Ditor DS. Sex differences in human skeletal muscle fatigue. Exerc Sport Sci Rev. 2001;29(3):109–12.
Fulco CS, Rock PB, Muza SR, Lammi E, Cymerman A, Butterfield G, et al. Slower fatigue and faster recovery of the adductor pollicis muscle in women matched for strength with men. Acta Physiol Scand. 1999;167(3):233–9. https://doi.org/10.1046/j.1365-201x.1999.00613.x.
Judge LW, Burke JR. The effect of recovery time on strength performance following a high-intensity bench press workout in males and females. Int J Sports Physiol Perform. 2010;5(2):184–96.
Hunter SK. Sex differences in human fatigability: mechanisms and insight to physiological responses. Acta Physiol (Oxf). 2014;210(4):768–89. https://doi.org/10.1111/apha.12234.
Wolfe BL, LeMura LM, Cole PJ. Quantitative analysis of single- vs. multiple-set programs in resistance training. J Strength Cond Res. 2004;18(1):35–47.
Schlumberger A, Stec J, Schmidtbleicher D. Single- vs. multiple-set strength training in women. J Strength Cond Res. 2001;15(3):284–9.
Simao R, Farinatti Pde T, Polito MD, Maior AS, Fleck SJ. Influence of exercise order on the number of repetitions performed and perceived exertion during resistance exercises. J Strength Cond Res. 2005;19(1):152–6.
Simao R, Farinatti TP, Polito MD, Viveiros L, Fleck SJ. Influence of exercise order on the number of repetitions performed and perceived exertion during resistance exercise in women. J Strength Cond Res. 2007;21(1):23–8. https://doi.org/10.1519/r-18765.1.
Staron RS, Karapondo DL, Kraemer WJ, Fry AC, Gordon SE, Falkel JE, et al. Skeletal muscle adaptations during early phase of heavy-resistance training in men and women. J Appl Physiol. 1994;76(3):1247–55. https://doi.org/10.1152/jappl.1994.76.3.1247.
Gentil P, Steele J, Pereira MC, Castanheira RP, Paoli A, Bottaro M. Comparison of upper body strength gains between men and women after 10 weeks of resistance training. Peer J. 2016;4:e1627. https://doi.org/10.7717/peerj.1627.
Abe T, DeHoyos DV, Pollock ML, Garzarella L. Time course for strength and muscle thickness changes following upper and lower body resistance training in men and women. Eur J Appl Physiol. 2000;81(3):174–80. https://doi.org/10.1007/s004210050027.
Kell RT. The influence of periodized resistance training on strength changes in men and women. J Strength Cond Res. 2011;25(3):735–44. https://doi.org/10.1519/JSC.0b013e3181c69f22.
O’Hagan F, Sale D, MacDougall J, Garner S. Response to resistance training in young women and men. Int J Sports Med. 1995;16(05):314–21.
Kraemer WJ, Mazzetti SA, Nindl BC, Gotshalk LA, Volek JS, Bush JA, et al. Effect of resistance training on women’s strength/power and occupational performances. Med Sci Sports Exerc. 2001;33(6):1011–25.
Barbalho M, Coswig VS, Steele J, Fisher JP, Paoli A, Gentil P. Evidence for an upper threshold for resistance training volume in trained women. Med Sci Sports Exerc. 2019;51(3):515–22. https://doi.org/10.1249/mss.0000000000001818.
Häkkinen K, Pakarinen A, Kallinen M. Neuromuscular adaptations and serum hormones in women during short-term intensive strength training. Eur J Appl Physiol Occup Physiol. 1992;64(2):106–11.
Ivey FM, Tracy BL, Lemmer JT, NessAiver M, Metter EJ, Fozard JL, et al. Effects of strength training and detraining on muscle quality: age and gender comparisons. J Gerontol A Biol Sci Med Sci. 2000;B55(3):152–7 (discussion B8–9).
Folland J, Williams A. The adaptations to strength training: morphological and neurological contributions to increased strength. Sports Med. 2007;37(2):145–68.
West DWD, Burd NA, Churchward-Venne TA, Camera DM, Mitchell CJ, Baker SK, et al. Sex-based comparisons of myofibrillar protein synthesis after resistance exercise in the fed state. J Appl Physiol. 2012;112(11):1805–13. https://doi.org/10.1152/japplphysiol.00170.2012.
Miller BF, Hansen M, Olesen JL, Flyvbjerg A, Schwarz P, Babraj JA, et al. No effect of menstrual cycle on myofibrillar and connective tissue protein synthesis in contracting skeletal muscle. Am J Physiol Endocrinol Metab. 2006;290(1):E163–8. https://doi.org/10.1152/ajpendo.00300.2005.
Fujita S, Rasmussen BB, Bell JA, Cadenas JG, Volpi E. Basal muscle intracellular amino acid kinetics in women and men. Am J Physiol Endocrinol Metab. 2007;292(1):E77–83. https://doi.org/10.1152/ajpendo.00173.2006.
Roth SM, Ivey FM, Martel GF, Lemmer JT, Hurlbut DE, Siegel EL, et al. Muscle size responses to strength training in young and older men and women. J Am Geriatr Soc. 2001;49(11):1428–33.
Lowe DA, Baltgalvis KA, Greising SM. Mechanisms behind estrogens’ beneficial effect on muscle strength in females. Exerc Sport Sci Rev. 2010;38(2):61–7. https://doi.org/10.1097/JES.0b013e3181d496bc.
Hansen M. Female hormones: do they influence muscle and tendon protein metabolism? Proc Nutr Soc. 2017;77(1):32–41. https://doi.org/10.1017/S0029665117001951.
Schoenfeld BJ. Potential mechanisms for a role of metabolic stress in hypertrophic adaptations to resistance training. Sports Med. 2013;43(3):179–94. https://doi.org/10.1007/s40279-013-0017-1.
Kraemer WJ, Ratamess NA. Hormonal responses and adaptations to resistance exercise and training. Sports Med. 2005;35(4):339–61.
Vingren JL, Kraemer WJ, Ratamess NA, Anderson JM, Volek JS, Maresh CM. Testosterone physiology in resistance exercise and training. Sports Med. 2010;40(12):1037–53. https://doi.org/10.2165/11536910-000000000-00000.
Urban RJ, Bodenburg YH, Gilkison C, Foxworth J, Coggan AR, Wolfe RR, et al. Testosterone administration to elderly men increases skeletal muscle strength and protein synthesis. Am J Physiol. 1995;269(5 Pt 1):E820–6. https://doi.org/10.1152/ajpendo.1995.269.5.E820.
Zhao W, Pan J, Zhao Z, Wu Y, Bauman WA, Cardozo CP. Testosterone protects against dexamethasone-induced muscle atrophy, protein degradation and mafbx upregulation. J Steroid Biochem Mol Biol. 2008;110(1–2):125–9. https://doi.org/10.1016/j.jsbmb.2008.03.024.
Vingren JL, Kraemer WJ, Hatfield DL, Volek JS, Ratamess NA, Anderson JM, et al. Effect of resistance exercise on muscle steroid receptor protein content in strength-trained men and women. Steroids. 2009;74(13):1033–9. https://doi.org/10.1016/j.steroids.2009.08.002.
Hakkinen K, Pakarinen A. Acute hormonal responses to heavy resistance exercise in men and women at different ages. Int J Sports Med. 1995;16(8):507–13. https://doi.org/10.1055/s-2007-973045.
Rønnestad BR, Nygaard H, Raastad T. Physiological elevation of endogenous hormones results in superior strength training adaptation. Eur J Appl Physiol. 2011;111(9):2249–59. https://doi.org/10.1007/s00421-011-1860-0.
Spiering BA, Kraemer WJ, Vingren JL, Ratamess NA, Anderson JM, Armstrong LE, et al. Elevated endogenous testosterone concentrations potentiate muscle androgen receptor responses to resistance exercise. J Steroid Biochem Mol Biol. 2009;114(3):195–9. https://doi.org/10.1016/j.jsbmb.2009.02.005.
Morton RW, Sato K, Gallaugher MPB, Oikawa SY, McNicholas PD, Fujita S, et al. Muscle androgen receptor content but not systemic hormones is associated with resistance training-induced skeletal muscle hypertrophy in healthy, young men. Front Physiol. 2018;9:1373. https://doi.org/10.3389/fphys.2018.01373.
Linnamo V, Pakarinen A, Komi PV, Kraemer WJ, Hakkinen K. Acute hormonal responses to submaximal and maximal heavy resistance and explosive exercises in men and women. J Strength Cond Res. 2005;19(3):566–71. https://doi.org/10.1519/r-15404.1.
Kraemer WJ, Fleck SJ, Dziados JE, Harman EA, Marchitelli LJ, Gordon SE, et al. Changes in hormonal concentrations after different heavy-resistance exercise protocols in women. J Appl Physiol. 1993;75(2):594–604. https://doi.org/10.1152/jappl.1993.75.2.594.
Bosco C, Colli R, Bonomi R, von Duvillard SP, Viru A. Monitoring strength training: neuromuscular and hormonal profile. Med Sci Sports Exerc. 2000;32(1):202–8.
Liening SH, Stanton SJ, Saini EK, Schultheiss OC. Salivary testosterone, cortisol, and progesterone: two-week stability, interhormone correlations, and effects of time of day, menstrual cycle, and oral contraceptive use on steroid hormone levels. Physiol Behav. 2010;99(1):8–16.
Bruinvels G, Burden R, Brown N, Richards T, Pedlar C. The prevalence and impact of heavy menstrual bleeding (menorrhagia) in elite and non-elite athletes. PLoS One. 2016;11(2):e0149881. https://doi.org/10.1371/journal.pone.0149881.
Mihm M, Gangooly S, Muttukrishna S. The normal menstrual cycle in women. Anim Reprod Sci. 2011;124(3):229–36. https://doi.org/10.1016/j.anireprosci.2010.08.030.
Janse de Jonge XA. Effects of the menstrual cycle on exercise performance. Sports Med. 2003;33(11):833–51.
Bambaeichi E, Reilly T, Cable NT, Giacomoni M. The isolated and combined effects of menstrual cycle phase and time-of-day on muscle strength of eumenorrheic females. Chronobiol Int. 2004;21(4–5):645–60. https://doi.org/10.1081/CBI-120039206.
Sarwar R, Niclos BB, Rutherford O. Changes in muscle strength, relaxation rate and fatiguability during the human menstrual cycle. J Physiol. 1996;493(1):267–72.
Phillips S, Sanderson A, Birch K, Bruce S, Woledge R. Changes in maximal voluntary force of human adductor pollicis muscle during the menstrual cycle. J Physiol. 1996;496(2):551–7.
Kraemer RR, Heleniak RJ, Tryniecki JL, Kraemer GR, Okazaki NJ, Castracane VD. Follicular and luteal phase hormonal responses to low-volume resistive exercise. Med Sci Sports Exerc. 1995;27(6):809–17.
Nakamura Y, Aizawa K, Imai T, Kono I, Mesaki N. Hormonal responses to resistance exercise during different menstrual cycle states. Med Sci Sports Exerc. 2011;43(6):967–73. https://doi.org/10.1249/MSS.0b013e3182019774.
Wolf MR, Fragala MS, Volek JS, Denegar CR, Anderson JM, Comstock BA, et al. Sex differences in creatine kinase after acute heavy resistance exercise on circulating granulocyte estradiol receptors. Eur J Appl Physiol. 2012;112(9):3335–40.
Wikstrom-Frisen L, Boraxbekk CJ, Henriksson-Larsen K. Effects on power, strength and lean body mass of menstrual/oral contraceptive cycle based resistance training. J Sports Med Phys Fit. 2017;57(1–2):43–52. https://doi.org/10.23736/s0022-4707.16.05848-5.
Sung E, Han A, Hinrichs T, Vorgerd M, Manchado C, Platen P. Effects of follicular versus luteal phase-based strength training in young women. SpringerPlus. 2014;3(1):668. https://doi.org/10.1186/2193-1801-3-668.
Reis E, Frick U, Schmidtbleicher D. Frequency variations of strength training sessions triggered by the phases of the menstrual cycle. Int J Sports Med. 1995;16(8):545–50. https://doi.org/10.1055/s-2007-973052.
Sakamaki-Sunaga M, Min S, Kamemoto K, Okamoto T. Effects of menstrual phase-dependent resistance training frequency on muscular hypertrophy and strength. J Strength Cond Res. 2016;30(6):1727–34. https://doi.org/10.1519/jsc.0000000000001250.
Enns DL, Tiidus PM. The influence of estrogen on skeletal muscle. Sports Med. 2010;40(1):41–58. https://doi.org/10.2165/11319760-000000000-00000.
Brown M. Estrogen effects on skeletal muscle. In: Spangenburg EE, editor. Integrative biology of women’s health. New York: Springer; 2013. p. 35–51.
Galluzzo P, Rastelli C, Bulzomi P, Acconcia F, Pallottini V, Marino M. 17beta-Estradiol regulates the first steps of skeletal muscle cell differentiation via er-alpha-mediated signals. Am J Physiol Cell Physiol. 2009;297(5):C1249–62. https://doi.org/10.1152/ajpcell.00188.2009.
Kahlert S, Grohe C, Karas RH, Lobbert K, Neyses L, Vetter H. Effects of estrogen on skeletal myoblast growth. Biochem Biophys Res Commun. 1997;232(2):373–8. https://doi.org/10.1006/bbrc.1997.6223.
Sciote JJ, Horton MJ, Zyman Y, Pascoe G. Differential effects of diminished oestrogen and androgen levels on development of skeletal muscle fibres in hypogonadal mice. Acta Physiol Scand. 2001;172(3):179–87. https://doi.org/10.1046/j.1365-201x.2001.00854.x.
Kitajima Y, Ono Y. Estrogens maintain skeletal muscle and satellite cell functions. J Endocrinol. 2016;229(3):267–75. https://doi.org/10.1530/joe-15-0476.
Enns DL, Tiidus PM. Estrogen influences satellite cell activation and proliferation following downhill running in rats. J Appl Physiol (1985). 2008;104(2):347–53. https://doi.org/10.1152/japplphysiol.00128.2007.
Hamadeh MJ, Devries MC, Tarnopolsky MA. Estrogen supplementation reduces whole body leucine and carbohydrate oxidation and increases lipid oxidation in men during endurance exercise. J Clin Endocrinol Metab. 2005;90(6):3592–9. https://doi.org/10.1210/jc.2004-1743.
Pöllänen E, Ronkainen PH, Suominen H, Takala T, Koskinen S, Puolakka J, et al. Muscular transcriptome in postmenopausal women with or without hormone replacement. Rejuvenation Res. 2007;10(4):485–500.
Taaffe DR, Newman AB, Haggerty CL, Colbert LH, de Rekeneire N, Visser M, et al. Estrogen replacement, muscle composition, and physical function: the Health ABC Study. Med Sci Sports Exerc. 2005;37(10):1741–7.
Sipila S, Taaffe DR, Cheng S, Puolakka J, Toivanen J, Suominen H. Effects of hormone replacement therapy and high-impact physical exercise on skeletal muscle in post-menopausal women: a randomized placebo-controlled study. Clin Sci (Lond). 2001;101(2):147–57.
Skelton DA, Phillips SK, Bruce SA, Naylor CH, Woledge RC. Hormone replacement therapy increases isometric muscle strength of adductor pollicis in post-menopausal women. Clin Sci (Lond). 1999;96(4):357–64.
Hackney A. Sex hormones, exercise and women: scientific and clinical aspects. Cham: Springer International Publishing; 2017.
Smith GI, Yoshino J, Reeds DN, Bradley D, Burrows RE, Heisey HD, et al. Testosterone and progesterone, but not estradiol, stimulate muscle protein synthesis in postmenopausal women. J Clin Endocrinol Metab. 2014;99(1):256–65. https://doi.org/10.1210/jc.2013-2835.
Kriengsinyos W, Wykes LJ, Goonewardene LA, Ball RO, Pencharz PB. Phase of menstrual cycle affects lysine requirement in healthy women. Am J Physiol Endocrinol Metab. 2004;287(3):E489–96. https://doi.org/10.1152/ajpendo.00262.2003.
Oosthuyse T, Bosch AN. The effect of the menstrual cycle on exercise metabolism. Sports Med. 2010;40(3):207–27. https://doi.org/10.2165/11317090-000000000-00000.
Landau RL, Poulos JT. The metabolic influence of progestins. Adv Metab Disord. 1971;5:119–47. https://doi.org/10.1016/B978-0-12-027305-8.50024-2.
Schoenfeld BJ. The mechanisms of muscle hypertrophy and their application to resistance training. J Strength Cond Res. 2010;24(10):2857–72.
Velloso CP. Regulation of muscle mass by growth hormone and IGF-I. Br J Pharmacol. 2008;154(3):557–68. https://doi.org/10.1038/bjp.2008.153.
Kraemer WJ, Gordon S, Fleck S, Marchitelli L, Mello R, Dziados J, et al. Endogenous anabolic hormonal and growth factor responses to heavy resistance exercise in males and females. Int J Sports Med. 1991;12(2):228–35.
Fink J, Kikuchi N, Nakazato K. Effects of rest intervals and training loads on metabolic stress and muscle hypertrophy. Clin Physiol Funct Imaging. 2018;38(2):261–8. https://doi.org/10.1111/cpf.12409.
McCall GE, Byrnes WC, Fleck SJ, Dickinson A, Kraemer WJ. Acute and chronic hormonal responses to resistance training designed to promote muscle hypertrophy. Can J Appl Physiol. 1999;24(1):96–107.
Mulligan SE, Fleck SJ, Gordon SE, Koziris LP, Triplett-McBride NT, Kraemer WJ. Influence of resistance exercise volume on serum growth hormone and cortisol concentrations in women. J Strength Cond Res. 1996;10(4):256–62.
Jaffe CA, Ocampo-Lim B, Guo W, Krueger K, Sugahara I, Demott-Friberg R, et al. Growth hormone secretory dynamics over the menstrual cycle. Endocr J. 2000;47(5):549–56.
Giustina A, Veldhuis JD. Pathophysiology of the neuroregulation of growth hormone secretion in experimental animals and the human. Endocr Rev. 1998;19(6):717–97. https://doi.org/10.1210/edrv.19.6.0353.
Kanaley JA, Giannopoulou I, Collier S, Ploutz-Snyder R, Carhart R Jr. Hormone-replacement therapy use, but not race, impacts the resting and exercise-induced GH response in postmenopausal women. Eur J Endocrinol. 2005;153(4):527–33. https://doi.org/10.1530/eje.1.02006.
Hellhammer DH, Wüst S, Kudielka BM. Salivary cortisol as a biomarker in stress research. Psychoneuroendocrinology. 2009;34(2):163–71.
Biedasek K, Andres J, Mai K, Adams S, Spuler S, Fielitz J, et al. Skeletal muscle 11beta-hsd1 controls glucocorticoid-induced proteolysis and expression of e3 ubiquitin ligases atrogin-1 and murf-1. PLoS One. 2011;6(1):e16674. https://doi.org/10.1371/journal.pone.0016674.
Auclair D, Garrel DR, Chaouki Zerouala A, Ferland LH. Activation of the ubiquitin pathway in rat skeletal muscle by catabolic doses of glucocorticoids. Am J Physiol. 1997;272(3 Pt 1):C1007–16. https://doi.org/10.1152/ajpcell.1997.272.3.C1007.
Paddon-Jones D, Sheffield-Moore M, Creson DL, Sanford AP, Wolf SE, Wolfe RR, et al. Hypercortisolemia alters muscle protein anabolism following ingestion of essential amino acids. Am J Physiol Endocrinol Metab. 2003;284(5):E946–53. https://doi.org/10.1152/ajpendo.00397.2002.
Gore DC, Jahoor F, Wolfe RR, Herndon DN. Acute response of human muscle protein to catabolic hormones. Ann Surg. 1993;218(5):679–84.
Gröschl M, Rauh M, Schmid P, Dörr H-G. Relationship between salivary progesterone, 17-hydroxyprogesterone, and cortisol levels throughout the normal menstrual cycle of healthy postmenarcheal girls. Fertil Steril. 2001;76(3):615–7. https://doi.org/10.1016/s0015-0282(01)01960-4.
Wolfram M, Bellingrath S, Kudielka BM. The cortisol awakening response (CAR) across the female menstrual cycle. Psychoneuroendocrinology. 2011;36(6):905–12.
Viau V, Meaney MJ. The inhibitory effect of testosterone on hypothalamic–pituitary–adrenal responses to stress is mediated by the medial preoptic area. J Neurosci. 1996;16(5):1866–76.
Viau V, Meaney MJ. Variations in the hypothalamic–pituitary–adrenal response to stress during the estrous cycle in the rat. Endocrinology. 1991;129(5):2503–11. https://doi.org/10.1210/endo-129-5-2503.
Bennell K, White S, Crossley K. The oral contraceptive pill: a revolution for sports women? Br J Sports Med. 1999;33(4):231–8.
United Nations, Department of Economic and Social Affairs, Population Division. Trends in contraceptive use worldwide 2015. New York (NY), 2015. http://www.un.org/en/development/desa/population/publications/pdf/family/trendsContraceptiveUse2015Report.pdf. Accessed 26 Apr 2018.
Verrilli LE, Landry M, Blanchard H. Contraceptive choices and menstrual patterns in high level female athletes. Fertil Steril. 2017;108(3):e122. https://doi.org/10.1016/j.fertnstert.2017.07.374.
Torstveit MK, Sundgot-Borgen J. Participation in leanness sports but not training volume is associated with menstrual dysfunction: a national survey of 1276 elite athletes and controls. Br J Sports Med. 2005;39(3):141–7. https://doi.org/10.1136/bjsm.2003.011338.
Dal’Ava N, Bahamondes L, Bahamondes MV, de Oliveira Santos A, Monteiro I. Body weight and composition in users of levonorgestrel-releasing intrauterine system. Contraception. 2012;86(4):350–3. https://doi.org/10.1016/j.contraception.2012.01.017.
Burrows M, Peters CE. The influence of oral contraceptives on athletic performance in female athletes. Sports Med. 2007;37(7):557–74.
Hall KS, Trussell J. Types of combined oral contraceptives used by U.S. women. Contraception. 2012;86(6):659–65. https://doi.org/10.1016/j.contraception.2012.05.017.
Zimmerman Y, Eijkemans MJC, Coelingh Bennink HJT, Blankenstein MA, Fauser B. The effect of combined oral contraception on testosterone levels in healthy women: a systematic review and meta-analysis. Hum Reprod Update. 2014;20(1):76–105. https://doi.org/10.1093/humupd/dmt038.
Elliott K, Cable N, Reilly T. Does oral contraceptive use affect maximum force production in women? Br J Sports Med. 2005;39(1):15–9. https://doi.org/10.1136/bjsm.2003.009886.
Nichols AW, Hetzler RK, Villanueva RJ, Stickley CD, Kimura IF. Effects of combination oral contraceptives on strength development in women athletes. J Strength Cond Res. 2008;22(5):1625–32. https://doi.org/10.1519/JSC.0b013e31817ae1f3.
Peters C, Burrows M. Androgenicity of the progestin in oral contraceptives does not affect maximal leg strength. Contraception. 2006;74(6):487–91. https://doi.org/10.1016/j.contraception.2006.08.005.
Balogh A, Kauf E, Vollanth R, Graser G, Klinger G, Oettel M. Effects of two oral contraceptives on plasma levels of insulin-like growth factor I (IGF-I) and growth hormone (HGH). Contraception. 2000;62(5):259–69.
Kraemer WJ, Nindl BC, Volek JS, Marx JO, Gotshalk LA, Bush JA, et al. Influence of oral contraceptive use on growth hormone in vivo bioactivity following resistance exercise: responses of molecular mass variants. Growth Horm IGF Res. 2008;18(3):238–44.
Hansen M, Langberg H, Holm L, Miller B, Petersen S, Doessing S, et al. Effect of administration of oral contraceptives on the synthesis and breakdown of myofibrillar proteins in young women. Scand J Med Sci Sports. 2011;21(1):62–72.
Chidi-Ogbolu N, Baar K. Effect of estrogen on musculoskeletal performance and injury risk. Front Physiol. 2019;9:1834. https://doi.org/10.3389/fphys.2018.01834.
Phillips SM, Parise G, Roy BD, Tipton KD, Wolfe RR, Tarnopolsky MA. Resistance-training-induced adaptations in skeletal muscle protein turnover in the fed state. Can J Physiol Pharmacol. 2002;80(11):1045–53.
Bo K, Artal R, Barakat R, Brown W, Davies GA, Dooley M, et al. Exercise and pregnancy in recreational and elite athletes: 2016 evidence summary from the IOC expert group meeting, Lausanne. Part 1. Exercise in women planning pregnancy and those who are pregnant. Br J Sports Med. 2016;50(10):571–89. https://doi.org/10.1136/bjsports-2016-096218.
Kumar P, Magon N. Hormones in pregnancy. Niger Med J. 2012;53(4):179–83.
Elliott Kirsty J, Cable Nigel T, Reilly T, Sefton V, Kingsland C, Diver M. Effects of supra-physiological changes in human ovarian hormone levels on maximum force production of the first dorsal interosseus muscle. Exp Physiol. 2005;90(2):215–23. https://doi.org/10.1113/expphysiol.2004.028258.
Sipila S. Body composition and muscle performance during menopause and hormone replacement therapy. J Endocrinol Investig. 2003;26(9):893–901. https://doi.org/10.1007/bf03345241.
Smith GI, Reeds DN, Hall AM, Chambers KT, Finck BN, Mittendorfer B. Sexually dimorphic effect of aging on skeletal muscle protein synthesis. Biol Sex Differ. 2012;3(1):11.
Mountjoy M, Sundgot-Borgen JK, Burke LM, Ackerman KE, Blauwet C, Constantini N, et al. IOC consensus statement on relative energy deficiency in sport (RED-S): 2018 update. Br J Sports Med. 2018;52(11):687–97. https://doi.org/10.1136/bjsports-2018-099193.
Wikstrom-Frisen L, Boraxbekk CJ, Henriksson-Larsen K. Increasing training load without risking the female athlete triad: menstrual cycle based periodized training may be an answer? J Sports Med Phys Fit. 2017;57(11):1519–25. https://doi.org/10.23736/s0022-4707.16.06444-6.
Nindl BC. Physical training strategies for military women’s performance optimization in combat-centric occupations. J Strength Cond Res. 2015;29(Suppl. 11):S101–6. https://doi.org/10.1519/jsc.0000000000001089.
Ecochard R, Boehringer H, Rabilloud M, Marret H. Chronological aspects of ultrasonic, hormonal, and other indirect indices of ovulation. BJOG. 2001;108(8):822–9.
Elliott-Sale KJ, Smith S, Bacon J, Clayton D, McPhilimey M, Goutianos G, et al. Examining the role of oral contraceptive users as an experimental and/or control group in athletic performance studies. Contraception. 2013;88(3):408–12. https://doi.org/10.1016/j.contraception.2012.11.023.
Mann JB, Thyfault JP, Ivey PA, Sayers SP. The effect of autoregulatory progressive resistance exercise vs. linear periodization on strength improvement in college athletes. J Strength Cond Res. 2010;24(7):1718–23. https://doi.org/10.1519/jsc.0b013e3181def4a6.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
No sources of funding were used to assist in the preparation of this article.
Conflict of interest
Olivia E. Knowles, Brad Aisbett, Luana C. Main, Eric J. Drinkwater, Liliana Orellana and Séverine Lamon have no conflicts of interest that are directly relevant to the content of this review.
Rights and permissions
About this article

Cite this article
Knowles, O.E., Aisbett, B., Main, L.C. et al. Resistance Training and Skeletal Muscle Protein Metabolism in Eumenorrheic Females: Implications for Researchers and Practitioners. Sports Med 49, 1637–1650 (2019). https://doi.org/10.1007/s40279-019-01132-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40279-019-01132-7