
Abstract
Background
Resistance training (RT) has been investigated as a potential intervention strategy for improving muscle function, but the effects on lower-extremity muscle power in middle-aged and older adults have not been systematically reviewed.
Objective
The aim of this meta-analysis is to provide a quantitative estimate of the effect of RT on lower-extremity muscle power in middle-aged and older adults and to examine independent moderators of this relationship.
Methods
Randomized controlled trials that examined the effects of RT on either leg press (LP) or knee extension (KE) muscle power in adults aged ≥50 years were included. Data were aggregated with meta-analytic techniques, and multi-level modeling was used to adjust for nesting effects. A total of 52 effects from 12 randomized controlled trials were analyzed with a random-effects model to estimate the effect of RT on lower-extremity muscle power. A multiple-regression analysis was conducted to examine independent moderators of the mean effect.
Results
The adjusted aggregated results from all studies indicate that RT has a small-to-moderate effect on lower-extremity muscle power (Hedges’ d = 0.34, 95 % confidence interval [CI] 0.25–0.43), which translated to 54.90 watts (95 % CI 40.37–69.43). Meta-regression analyses indicated that high-velocity RT was superior to traditional RT (Δ = 0.62 vs. 0.20, respectively) for increasing lower-extremity muscle power. In addition, training volume significantly moderated the effect of RT on muscle power.
Conclusion
The findings from this meta-analysis indicate that RT is an efficacious intervention strategy for improving LP and KE muscle power in adults aged ≥50 years. Training mode and volume independently moderate the effect of RT on lower-extremity muscle power, and should be considered when prescribing RT exercise for middle-aged and older adults.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Resistance training is recommended as an exercise strategy for improving muscle power during aging, but no review has quantified the effect of resistance training on lower-extremity muscle power in adults aged ≥50 years. |
The results of this meta-analysis indicate that resistance training has a small-to-moderate effect on leg press and knee extensor power in adults aged ≥50 years, and suggest that mode of training and training volume are independent moderators of this effect. |
Additional randomized controlled trials are needed to determine the optimal exercise intervention for increasing lower-extremity muscle power in older adults. |
1 Introduction
The population of adults aged 45–64 and ≥65 years living in the USA increased by 24 and 21 %, respectively, from 2002 to 2012 [1]. The unprecedented growth in the number of middle-aged and older adults is noteworthy, as the likelihood of physical function limitations increases with age. Data from the National Health Interview Survey indicated a significant increase in difficulty with mobility-related physical functions (stooping, bending or kneeling, standing 2 h, walking a ¼ mile, climbing ten steps) among adults aged 50–64 years (“young–old”) from 1997 to 2007 [2]. However, the prevalence of one or more physical limitations increases with age, from 17 % of adults aged 50–59 years to 43 % among adults aged ≥80 years [3]. Because the onset of physical limitations manifests between the ages 40–55 years for 50 % of adults [4], early intervention with evidence-based exercise strategies may have a critical role in preventing physical disability during later adulthood.
Recently, the International Working Group on Sarcopenia established a consensus definition of sarcopenia as the age-associated reduction in skeletal muscle size and function [5]. Similarly, the European Working Group on Sarcopenia in Older People suggested an algorithm for the operational diagnosis of sarcopenia in older adults using age- and sex-specific cut-points for decrements in muscle mass, strength, and physical performance [6]. Importantly, while skeletal muscle size and function decline with advancing age [7], the rate of decline in muscle power is more precipitous than the decrease in either muscle mass or strength [8, 9], with recent longitudinal evidence indicating an annual loss of power at 6 % over 3 years among adults aged 70–85 years [10]. This is particularly concerning because muscle power, defined as the product of muscle force and contraction velocity [11], is a contributor to physical function in both middle-aged (45–64 years) and older adults (≥65 years) [12–22]. Lower-extremity muscle power has been associated with several indices of physical function, such as self-reported functional status [12], chair rise time and stair climb performance [13], and walking speed [16]. In a previous review, Reid and Fielding [23] delineated the importance of muscle power in the context of the disablement process [24], indicating that muscle pathologies (loss of motor units and muscle fiber atrophy) can ultimately manifest as physical disability for an older adult (difficulty crossing the street due to reduced gait speed). Because declines in skeletal muscle mass, strength, and power become evident at ~35 years of age [5], intervention strategies that can effectively improve muscle power during middle and later adulthood are urgently required.
Accordingly, resistance training (RT) has been suggested as a safe and effective intervention strategy for preventing the loss of muscle power in adults [23, 25], and position statements by the American College of Sports Medicine (ACSM) [26–28] recommend it for all adults. Traditionally, progressive RT is defined as the gradual increase in stress placed upon the body during RT exercise [29]. Two recent meta-analyses have reported that RT exercise interventions can significantly improve skeletal muscle mass and strength in adults aged ≥50 years [30, 31]. However, while multiple intervention trials [32–38] have demonstrated that RT is an efficacious exercise strategy for eliciting gains in muscle power in cohorts of older adults, to our knowledge, no reviews have synthesized a quantitative estimate of the effects of RT on lower-extremity muscle power in randomized controlled trials (RCTs) of adults aged ≥50 years.
Moreover, due to the relation between muscle power and physical function [12, 14, 16, 21], there has been increasing interest in identifying the optimal mode of RT for increasing skeletal muscle power [23, 39]. Because the physiological adaptations in response to a training intervention are specific to the RT stimulus, referred to as the specificity of training [29], it has been suggested that RT programs for older adults should be designed to increase muscle power [39]. Congruent with this notion, some research [37], but not all [33], suggests that high-velocity RT (e.g., power training), which is characterized by an individual performing the concentric phase of each repetition as rapidly as possible [23, 39], may be a more effective training stimulus for improving skeletal muscle power than traditional slow-speed RT. However, whether the mode of RT (high-velocity vs. traditional slow-speed RT) moderates the effect of training on muscle power in adults aged ≥50 years has not been well-characterized.
Thus, the purpose of this meta-analysis was to estimate the effect size of RT on two widely reported measures of lower-extremity muscle power, leg press (LP) and knee extension (KE), in RCTs of adults aged ≥50 years, and to examine independent moderators of the effect, including age, sex, baseline muscle power, and critical acute intervention variables (mode of RT, training frequency, intensity of training, and training volume). We hypothesized that RT interventions would significantly increase lower-extremity muscle power relative to control groups. We also hypothesized that mode of RT (high-velocity RT vs. traditional RT) and other acute intervention variables, specifically training intensity, would be associated with the mean effect of RT on lower-extremity muscle power.
2 Methods
The present meta-analysis is reported in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analyses) statement [40].
2.1 Literature Search
RCTs published by 1 November 2014 were identified via a systematic literature search on Google Scholar with all of the terms ‘older adults’ and ‘randomized controlled trial’, the exact phrase ‘muscle power’, and with at least one of the terms ‘resistance training’ and ‘strength training’. Our search was limited to studies of adults aged ≥50 years as this age demarcation is congruent with previous review articles that have described the effects of RT on physical function [41], skeletal muscle quality [42], mass [31] and strength [30] in older adults. We also manually reviewed reference lists from retrieved articles to identify additional studies.
2.2 Inclusion and Exclusion Criteria
Eligible studies met the following inclusion criteria: (1) peer-reviewed publication, (2) available in English, (3) participants were randomly assigned to an RT group or a control group, (4) participants were aged ≥50 years, and (5) an index of lower-extremity muscle power (LP or KE; watts) was reported. Studies were excluded from the analysis for the following reasons: (1) not available in English, (2) did not report LP or KE indices of muscle power, (3) included adults aged <50 years, (4) recruited participants from a clinical population (e.g., institutionalized residents), (5) included RT as part of a multicomponent intervention (e.g., exercise + pharmacologic treatment), (6) compared RT with an active treatment condition (e.g., high-velocity RT vs. traditional RT), and (7) not enough information was provided for data extraction.
In order to operationalize RT and control conditions, we defined RT according to the ACSM position stand, which identifies muscle-strengthening activities such as a progressive-weight training program, weight bearing calisthenics, and similar resistance exercises that use the body’s major muscle groups [27]. Moreover, the ACSM position stand indicates that several different types of RT equipment can be used to improve muscular fitness, and these include free weights, machines (stacked weights or pneumatic resistance), and resistance bands [26], and all of these modalities were considered during the literature search. The control condition was defined as a group that was instructed not to deviate from their habitual physical activity level, or any sham exercise group that had no theoretical or empirical relationship with lower-extremity muscle power (e.g., balance and flexibility).
2.3 Data Extraction
Two of the authors independently extracted mean and/or peak LP or KE muscle power (watts), standard deviations, and sample sizes from eligible studies. A majority of the included studies provided data in a table or in the text; however, means and standard deviations had to be estimated in several instances. One study reported baseline and post-intervention LP and KE values as mean ± standard errors (SEs), which were converted to standard deviations [33]. In another study, the means were calculated from within-group percentage changes reported in LP and KE muscle power [43]. In a third study, mean changes in muscle power for the experimental and control groups were estimated from a figure [44]. The intraclass correlation coefficient, which provides an indication of inter-rater reliability and the original agreement between the authors, was calculated as 0.96, and all discrepancies were resolved.
2.4 Effect Size Calculation
Hedges’ g effect sizes were calculated by subtracting the mean change in the control group from the mean change in the experimental group and dividing the difference by the pooled standard deviation of the baseline scores [45]. A separate effect size was calculated for each LP and KE outcome, and muscle power index (e.g., LP or KE) was examined as a primary moderator in our meta-regression analysis. To correct for sampling error, effects were converted to Hedges’ d [45]. Effects were coded so that positive values represented an improvement in muscle power.
2.5 Aggregation of Effects
Effects were weighted using the inverse variance method and aggregated using a random-effects model [46]. The random-effects model was used due to variability in experimental factors (e.g., training intensity, mode of RT, etc.) across RCTs included in our review. Macro MeanES [46] was executed within SPSS version 22.0 (SPSS IBM, New York, NY, USA) and used to estimate the mean effect and examine the influence of potential moderators. Heterogeneity and consistency were inspected with the Q and I 2 statistics [47, 48]. Presence of publication bias was determined by evaluation of forest and funnel plots and calculation of Egger’s test for publication bias [49]. We calculated the number of effects needed to overturn the result (N+) [50].
In most studies, multiple outcome measures or repeated measurements across time yielded nested effects within studies (median of four effects per study), which might systematically differ from each other. Hence, a multi-level model with robust maximum likelihood estimation was used to adjust for between-study variance and correlated effects within studies [51] according to standard procedures [52, 53] using Mplus 7.11 (Muthén & Muthén, Los Angeles, CA, USA) [51]. Parameters and their errors were estimated with clustering on study using the Huber-White sandwich estimator to calculate SEs that are robust to heteroscedasticity and correlated effects [54–56].
2.6 Moderator Analysis
We selected moderators a priori that are theoretically or empirically associated with lower-extremity muscle power in older adults (Table 1). The eight primary moderators were the age of the participants, the percentage of the sample that was female, baseline level of LP or KE muscle power, index of muscle power assessed (LP or KE), and critical acute RT program variables identified in ACSM position stands [26–28]: mode of training (traditional RT vs. high-velocity or power RT), training frequency (day/week), intensity of training (percentage of one-repetition maximum [1-RM]) and training volume (product of sets × repetitions; categorized as low [<24], moderate [24], and high [>24]).
A meta-regression analysis using random-effects maximum likelihood estimation was performed with macro METAREG [46] within SPSS version 22.0 (SPSS IBM). Independence of significant univariate effects was examined with multiple regression and multi-level modeling. The effect of moderators in the multi-level nested model was tested by comparing the conditional model (which included the intercept and the moderator) with the unconditional intercept-only model using a likelihood ratio test and the adjusted Bayesian Information Criterion (BIC) [53].
3 Results
3.1 Preliminary and Descriptive Results
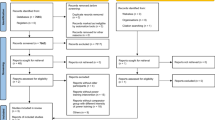
The search produced 1445 full-text articles; 1433 were excluded. Figure 1 provides a flowchart delineating study selection. A total of 52 effects (k) from 12 studies were included in the final exercise versus control effect size calculation [32–35, 38, 43, 44, 57–61]. Table 2 provides a description of study characteristics of RCTs included in the analysis. Table 3 provides a list of univariate analyses of moderators for the exercise versus control analysis.

Flow chart of study selection. KE knee extension, LP leg press, RT resistance training
3.2 Primary Results
The percent changes in lower-extremity muscle power (watts) for the experimental and control groups were +16.96 and –0.80 %, respectively. The unadjusted mean effect size Δ for RT compared with control was 0.34 (95 % confidence interval [CI] 0.21–0.47; z = 4.99; p < 0.00001). The effect was heterogeneous (Q = 92.4219, p = 0.0003; I 2 = 45.90, 95 % CI 36.19–54.14). The distribution of effects, which ranged from –0.97 to 1.31, was negatively skewed (–0.65, SE = 0.33) and leptokurtic (0.60, SE = 0.65). A total of 81 % (42 of 52) of the exercise-control effect sizes were greater than 0, favoring an improvement in LP or KE power following RT. The fail-safe number of effects was 612. Examination of the funnel (Fig. 2) and forest (Fig. 3) plots showed a lack of publication bias. Egger’s test for publication bias was not significant, t (1,50) = 0.41, p = 0.68. In the multi-level, intercept-only model (χ 2 (2) = 188.0, BIC = 189.7), the mean was 0.34 (95 % CI 0.25–0.43) with non-significant variance between effects (0.001, SE = 0.010, z = 0.102, p = 0.919).

Funnel plot of Hedges’ d effect sizes versus the study standard error

Forest plot of Hedges’ d effect sizes for resistance training compared with control (k = 52). Positive values favor resistance training and negative values favor control. Each row represents an individual effect that was extracted from a given study. The broken vertical line represents the mean effect size (Δ = 0.34). Data in parentheses are confidence intervals
3.3 Moderator Analysis
The unadjusted multiple-regression model was significant (p = 0.008; R 2 = 0.25). The mean effect was significantly moderated by the mode of training (β = –0.44, z = –3.44, p = 0.0006) and training volume (β = –0.25, z = –1.98, p = 0.047). The effect of RT on muscle power was larger for (1) high-velocity/power RT interventions (Δ = 0.62; 95 % CI 0.42–0.82) than for traditional RT programs (Δ = 0.20; 95 % CI 0.04–0.35) and (2) RT interventions with a moderate training volume (Δ = 0.41; 95 % CI 0.24–0.58) than for those with a low (Δ = 0.40, 95 % CI 0.10–0.70) or high (Δ = 0.18; 95 % CI –0.14 to 0.40) training volume.
In the multi-level model, mode of training (β = 0.197, SE = 0.036, z = 5.5, p < 0.001) and training volume (β = 0.221, SE = 0.093, z = 2.4, p = 0.017) improved model fit (χ 2 (4) = 157, BIC = 160) compared with the intercept-only model (Δχ 2 (2) = 6.2, p = 0.045). There was zero residual variance (p = 0.980), indicating that all of the variance between effects was explained by these two moderators (e.g., variance in the conditional model including mode and volume in the intercept-only model).
4 Discussion
The aggregated results of this investigation indicate that RT is an effective exercise intervention for improving lower-extremity muscle power in middle-aged and older adults compared with control groups (Δ = 0.34 or 54.90 watts), after adjustment for nesting effects. Our findings expand upon the current literature on RT and muscle power by synthesizing a quantitative estimate of the effect of RT on LP and KE power in adults aged ≥50 years, and identify independent moderators of the effect of RT on muscle power. As an accumulating body of evidence has demonstrated that lower-body muscle power is a salient determinant of physical function during later adulthood (≥50 years) [12, 14, 16, 20, 21, 23], the findings from the present analysis also have substantial clinical relevance due to the implications for potentially reducing the likelihood of physical disability.
Previous meta-analyses have indicated that RT is an effective exercise strategy for increasing muscle strength [30, 62, 63] and lean mass [31] in older adults, and these findings support the inclusion of muscle-strengthening activities in position stands by the ACSM [26–28]. However, to our knowledge, no meta-analysis has quantified the effect of RT on lower-extremity muscle power in RCTs of adults aged ≥50 years. Sarcopenia, which describes the age-related loss of both muscle size and function (strength and power) [5, 6], is a hallmark of the aging process. Thus, from a clinical standpoint, it is important to describe the efficacy of intervention strategies designed to improve muscle function, and particularly power, in middle-aged and older adults [23, 39, 64, 65]. Specifically, lower-extremity muscle power is of critical importance due to the paramount role of these muscle groups (gluteals, quadriceps, and hamstrings) in performing functional activities such as rising from a chair, stair ascent, and ambulation [42]. Our meta-regression analysis revealed that the index of muscle power assessed (e.g., LP or KE) did not significantly moderate the effect of RT, indicating that RT interventions are equally effective for improving both LP and KE power (Δ = 0.30 vs. 0.38, respectively). Thus, RT interventions can improve muscle power of the lower-body muscle groups that are most important for carrying out daily functional tasks during later adulthood.
Our regression analysis examined the impact of several moderators, including the most pertinent training intervention variables, on the effect of RT on lower-extremity muscle power in middle-aged and older adults. As expected, in support of our hypothesis, we found that mode of training (high-velocity/power RT vs. traditional RT) significantly moderated the effect of RT on muscle power, indicating that high-velocity training was superior to traditional RT for improving muscle power (Δ = 0.62 vs. 0.20, respectively). This finding is in agreement with a previous review that reported power training was more effective than progressive RT for improving muscle power in older adults (standardized mean difference = 1.66, 95 % CI 0.08–3.24) [63]; however, this analysis did not compare modes of RT versus control groups in RCTs. High-velocity training interventions are characterized by performing the concentric muscle contraction as rapidly as possible, while the eccentric phase of each movement is performed in a slow and controlled manner [64]. Because muscle power is the product of contraction force and movement velocity, it is physiologically plausible that rapid concentric contractions would increase muscle power to a greater extent than traditional RT.
Relatedly, the optimal training intensity using isotonic contractions (e.g., constant external load) for improving muscle power in older adults is unclear. The most recent ACSM position stand indicates that an RT intensity of 20–50 % 1-RM should be performed to increase muscle power in healthy adults [27]. Conversely, others have suggested that older adults should perform RT with heavy loads (e.g., ≥60 % 1-RM) to increase muscle power [64]. Finally, in a previous ACSM position stand on progression models for RT, Kraemer et al. [28] suggested a combination of light-to-moderate RT (30–60 % of 1-RM) performed at an explosive velocity to improve speed of contraction, and heavy RT (85–100 % 1-RM) to improve muscle force, thereby targeting both components of muscle power. Because a consensus has not been established regarding the optimal training intensity for improving power, we investigated training intensity as a primary moderator in our regression analysis. However, the meta-regression revealed that training intensity did not significantly moderate the effect of RT on LP or KE power in the RCTs included in our review. This is in contrast to a previous meta-analysis that aggregated the effects of RT on muscle strength in adults aged ≥50 years, and found that an increase in training intensity subgroup (e.g., 70–79 % 1-RM vs. ≥80 % 1-RM) was associated with a 5.5 % increase in muscle strength [30]. However, the effect of training intensity on muscle power is less clear due to the force-velocity relationship in skeletal muscle. Classically, the concentric force-velocity relationship indicates that peak muscle power is developed at 60–70 % of maximal force and 30–40 % of maximal velocity [66]. While this suggests there is an optimal training intensity (e.g., percentage of 1-RM) for improving muscle power, literature that has compared different RT intensities in the middle-aged and/or older adult cohorts is sparse. Notably, de Vos et al. [38] investigated the effects of RT intensity on muscle power in older adults and observed similar percentage improvements in muscle power following 8–12 weeks of explosive RT at 20, 50, and 80 % of 1-RM. More recently, Reid et al. [36] found that 16 weeks of high-velocity RT at low (40 % 1-RM) and high (70 % 1-RM) external resistances elicited similar percentage improvements in LP power (34 vs. 42 %, respectively) in community-dwelling older adults. Thus, as suggested in the above ACSM position stand on RT, it is probable that different training intensities (e.g., light vs. heavy) manipulate different components of power. Specifically, greater training intensities may improve absolute muscle force, while lower RT intensities may elicit gains in power by increasing fiber contraction velocity. Future research is needed to determine the optimal training intensity for improving muscle power in both middle-aged and older adults, and to elucidate the mechanisms through which different RT intensities operate to improve muscle power.
In a previous review, Steib et al. [63] found that power training was more effective than progressive RT for improving muscle power of adults aged ≥65 years in a comparison of four intervention trials. However, that analysis did not compare RT with a control group or specifically examine lower-extremity muscle power as the primary outcome. In addition, that study was limited by insufficient data regarding salient intervention variables (intensity, volume, frequency, duration), thus precluding a meta-regression analysis of independent moderators. The current investigation expands upon that study by indicating that both mode of RT and training volume (product of sets × repetitions) are independent moderators of the effect of RT on LP and KE muscle power in middle-aged and older adults. Specifically, our regression model indicated that training volume was inversely associated with the mean effect of RT on muscle power, suggesting that lower training volumes were associated with greater improvements. To date, specific guidelines have not been published regarding the optimal RT volume for improving muscle power in ostensibly healthy middle-aged and older adults. However, it is possible that lower volumes of higher RT intensities may confer greater benefits for muscle power than other training regimens. Additional research is needed to better characterize the impact of manipulating RT volume (repetitions and sets) on lower-extremity muscle power in middle-aged and older adults. Furthermore, determining the relative importance of RT volume and intensity will be critical for developing RT guidelines for muscle power in these cohorts.
In our meta-regression model, age and sex did not influence the effect of RT on lower-body muscle power. Congruent with the results of our analysis, Peterson et al. [30] found that age was not associated with the mean effect of RT on LP or KE strength in men and women aged ≥50 years. Taken together, these findings suggest that middle-aged and older adults have the capacity to improve lower-extremity muscle power with RT. In addition, percentage of female participants in each effect did not significantly influence the mean effect of RT on muscle power. Although cross-sectional studies have demonstrated older women have lower absolute and relative muscle power compared with older men [9, 16, 67], our analysis suggests that RT interventions are equally effective for improving lower-extremity muscle power across sexes.
In addition, the RCTs included in this meta-analysis involved community-dwelling middle-aged and older adults, and the observed effect of RT on lower-extremity muscle power may not be generalizable to other populations of adults, such as those with severe chronic disease or mobility limitations. Reid et al. [44] recently demonstrated that a cohort of 57 community-dwelling older adults with mobility limitations (a Short Physical Performance Battery score of 7.7 ± 1.4) significantly increased lower-extremity muscle power following 12 weeks of either high-velocity RT or traditional RT relative to a control group. However, additional research is needed to determine the optimal training regimen for men and women with mobility limitations, as these individuals represent a subgroup of the middle-aged and older adult cohorts that is particularly susceptible to future physical disability.
This meta-analysis also underscores the need for standard reporting of salient methodological characteristics of RCTs investigating the effects of RT interventions in middle-aged and older adults. Descriptive characteristics of the sample, such as age, body mass index, percentage of men and women, and presence of comorbid medical conditions, is necessary for improving generalizability of findings. In addition, it is strongly recommended that intervention trials report critical acute program variables, including training intensity, volume, frequency, and duration. To advance our understanding of the optimal RT intervention for maximizing lower-extremity muscle power in middle-aged and older adults, standard reporting of exercise training protocols used in well-designed RCTs is paramount for quantifying the effect of RT in future meta-analyses.
Finally, limitations to the present review should be acknowledged. First, we did not use a standardized procedure, such as the Jadad scale [68], to assess the methodological quality of the RCTs included in our meta-analysis. However, assessing the quality of RCTs is limited in meta-analyses of clinical exercise trials where it is not feasible to blind participants to treatment group. In addition, although the age range (≥50 years) of participants in our review was similar to that in other meta-analyses [30, 31], our analysis only included one study where the mean age was <60 years [57], as RCTs that have investigated the impact of RT on lower-extremity muscle power in the “young–old” (50–64 years) are lacking. However, we examined age as a continuous variable in our meta-regression analysis, and it did not significantly moderate the effect of RT on lower-extremity muscle power. It is also important to note that while high-velocity or power RT is generally characterized by participants performing the concentric phase of each repetition as rapidly as possible and the eccentric portion in a slow and controlled manner (2–3 s), there is no universal definition for power RT in older adults, and the RCTs included in this analysis may have operationalized this training modality differently. Finally, due to the eligibility criteria used for determining inclusion in this analysis, it is important to generalize our results cautiously. For example, we reported the mean effect of RT on LP and KE muscle power; however, it is not possible to infer the effect of RT from our analysis on other outcomes of muscle power (e.g., leg curl or ankle flexor power). Moreover, participants involved in these RCTs were ostensibly healthy, and extrapolating the effect of RT on lower-extremity muscle power to other populations of older adults, including those with mobility limitations, should be done carefully.
5 Conclusion
This meta-analysis provides a quantitative estimate of the effect of RT interventions on lower-extremity muscle power in middle-aged and older adults and identifies independent moderators that influence the effect of RT. The available evidence indicates that RT has a small-to-moderate effect (Hedges’ d = 0.34; 54.90 watts) on muscle power compared with a control group. In addition, our moderator analysis indicates that power training is more effective than traditional RT for improving muscle power, and that training volume is a critical acute intervention variable that influences the magnitude of change in LP and KE muscle power. Since the prevalence of physical limitations increases 2.5-fold from ages 50–59 to ≥80 years [3], implementing RT interventions through public health initiatives may reduce the risk of future functional decline and physical disability among community-dwelling middle-aged and older adults.
References
Administration on Aging. A profile of older Americans: 2013. Washington, DC: US Department of Health and Human Services; 2013.
Martin LG, Freedman VA, Schoeni RF, et al. Trends in disability and related chronic conditions among people ages fifty to sixty-four. Health Aff (Millwood). 2010;29:725–31.
Holmes J, Powell-Griner E, Lethbridge-Cejku M, et al. Aging differently: physical limitations among adults aged 50 years and over: United States, 2001–2007. NCHS Data Brief. 2009:1–8.
National Center for Health Statistics. Health, United States, 1996–97 and Injury chartbook. Hyattsville: US Department of Health and Human Services; 1997.
Fielding RA, Vellas B, Evans WJ, et al. Sarcopenia: an undiagnosed condition in older adults. Current consensus definition: prevalence, etiology, and consequences. International working group on sarcopenia. J Am Med Dir Assoc. 2011;12:249–56.
Cruz-Jentoft AJ, Baeyens JP, Bauer JM, et al. Sarcopenia: European consensus on definition and diagnosis: report of the European Working Group on Sarcopenia in Older People. Age Ageing. 2010;39:412–23.
Barbat-Artigas S, Rolland Y, Zamboni M, et al. How to assess functional status: a new muscle quality index. J Nutr Health Aging. 2012;16:67–77.
Metter EJ, Conwit R, Tobin J, et al. Age-associated loss of power and strength in the upper extremities in women and men. J Gerontol A Biol Sci Med Sci. 1997;52:B267–76.
Skelton DA, Greig CA, Davies JM, et al. Strength, power and related functional ability of healthy people aged 65–89 years. Age Ageing. 1994;23:371–7.
Clark DJ, Pojednic RM, Reid KF, et al. Longitudinal decline of neuromuscular activation and power in healthy older adults. J Gerontol A Biol Sci Med Sci. 2013;68:1419–25.
Knuttgen HG, Kraemer WJ. Terminology and measurement in exercise performance. J Strength Cond Res. 1987;1:1–10.
Foldvari M, Clark M, Laviolette LC, et al. Association of muscle power with functional status in community-dwelling elderly women. J Gerontol A Biol Sci Med Sci. 2000;55:M192–9.
Suzuki T, Bean JF, Fielding RA. Muscle power of the ankle flexors predicts functional performance in community-dwelling older women. J Am Geriatr Soc. 2001;49:1161–7.
Bean JF, Kiely DK, Herman S, et al. The relationship between leg power and physical performance in mobility-limited older people. J Am Geriatr Soc. 2002;50:461–7.
Cuoco A, Callahan DM, Sayers S, et al. Impact of muscle power and force on gait speed in disabled older men and women. J Gerontol A Biol Sci Med Sci. 2004;59:1200–6.
Rantanen T, Avela J. Leg extension power and walking speed in very old people living independently. J Gerontol A Biol Sci Med Sci. 1997;52:M225–31.
Bean JF, Leveille SG, Kiely DK, et al. A comparison of leg power and leg strength within the InCHIANTI study: which influences mobility more? J Gerontol A Biol Sci Med Sci. 2003;58:728–33.
Kuo HK, Leveille SG, Yen CJ, et al. Exploring how peak leg power and usual gait speed are linked to late-life disability: data from the National Health and Nutrition Examination Survey (NHANES), 1999–2002. Am J Phys Med Rehabil. 2006;85:650–8.
Skelton DA, Kennedy J, Rutherford OM. Explosive power and asymmetry in leg muscle function in frequent fallers and non-fallers aged over 65. Age Ageing. 2002;31:119–25.
Bassey EJ, Fiatarone MA, O’Neill EF, et al. Leg extensor power and functional performance in very old men and women. Clin Sci (Lond). 1992;82:321–7.
Ward-Ritacco CL, Adrian AL, Johnson MA, et al. Adiposity, physical activity, and muscle quality are independently related to physical function performance in middle-aged postmenopausal women. Menopause. 2014;21:1114–21.
Straight CR, Brady AO, Evans EM. Muscle quality and relative adiposity are the strongest predictors of lower-extremity physical function in older women. Maturitas. 2015;80:95–9.
Reid KF, Fielding RA. Skeletal muscle power: a critical determinant of physical functioning in older adults. Exerc Sport Sci Rev. 2012;40:4–12.
Verbrugge LM, Jette AM. The disablement process. Soc Sci Med. 1994;38:1–14.
Evans WJ, Campbell WW. Sarcopenia and age-related changes in body composition and functional capacity. J Nutr. 1993;123:465–8.
Nelson ME, Rejeski WJ, Blair SN, et al. Physical activity and public health in older adults: recommendation from the American College of Sports Medicine and the American Heart Association. Circulation. 2007;116:1094–105.
Garber CE, Blissmer B, Deschenes MR, et al. American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: guidance for prescribing exercise. Med Sci Sports Exerc. 2011;43:1334–59.
Kraemer WJ, Adams K, Cafarelli E, et al. American College of Sports Medicine position stand. Progression models in resistance training for healthy adults. Med Sci Sports Exerc. 2002;34:364–80.
American College of Sports Medicine. American College of Sports Medicine position stand. Progression models in resistance training for healthy adults. Med Sci Sports Exerc. 2009;41:687–708.
Peterson MD, Rhea MR, Sen A, et al. Resistance exercise for muscular strength in older adults: a meta-analysis. Ageing Res Rev. 2010;9:226–37.
Peterson MD, Sen A, Gordon PM. Influence of resistance exercise on lean body mass in aging adults: a meta-analysis. Med Sci Sports Exerc. 2011;43:249–58.
Hruda KV, Hicks AL, McCartney N. Training for muscle power in older adults: effects on functional abilities. Can J Appl Physiol. 2003;28:178–89.
Henwood TR, Riek S, Taaffe DR. Strength versus muscle power-specific resistance training in community-dwelling older adults. J Gerontol A Biol Sci Med Sci. 2008;63:83–91.
Skelton DA, Young A, Greig CA, et al. Effects of resistance training on strength, power, and selected functional abilities of women aged 75 and older. J Am Geriatr Soc. 1995;43:1081–7.
Marsh AP, Miller ME, Rejeski WJ, et al. Lower extremity muscle function after strength or power training in older adults. J Aging Phys Act. 2009;17:416–43.
Reid KF, Martin KI, Doros G, et al. Comparative effects of light or heavy resistance power training for improving lower extremity power and physical performance in mobility-limited older adults. J Gerontol A Biol Sci Med Sci. 2014;70:374–80.
Fielding RA, LeBrasseur NK, Cuoco A, et al. High-velocity resistance training increases skeletal muscle peak power in older women. J Am Geriatr Soc. 2002;50:655–62.
de Vos NJ, Singh NA, Ross DA, et al. Optimal load for increasing muscle power during explosive resistance training in older adults. J Gerontol A Biol Sci Med Sci. 2005;60:638–47.
Evans WJ. Exercise strategies should be designed to increase muscle power. J Gerontol A Biol Sci Med Sci. 2000;55:M309–10.
Moher D, Liberati A, Tetzlaff J, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6:e1000097.
Delmonico MJ, Lofgren IE. Resistance training during weight loss in overweight and obese older adults: what are the benefits? Am J Lifestyle Med. 2010;4:309–13.
Straight CR, Brady AO, Evans EM. Muscle quality in older adults: what are the health implications? Am J Lifestyle Med. 2015;9:130–6.
Henwood TR, Taaffe DR. Improved physical performance in older adults undertaking a short-term programme of high-velocity resistance training. Gerontology. 2005;51:108–15.
Reid KF, Callahan DM, Carabello RJ, et al. Lower extremity power training in elderly subjects with mobility limitations: a randomized controlled trial. Aging Clin Exp Res. 2008;20:337–43.
Hedges L, Olkin I. Statistical methods for meta-analysis. New York: Academic Press; 1985.
Lipsey M, Wilson D. Practical meta-analysis. Thousand Oaks: Sage Publications; 2001.
Cochran WG. The combination of estimates from different experiments. Biometrics. 1954;10:101–29.
Higgins JP, Thompson SG, Deeks JJ, et al. Measuring inconstency in meta-analyses. BMJ. 2003;327:557–60.
Egger M, Smith GD, Schneider M, et al. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315:629–34.
Rosenberg MS. The file-drawer problem revisited: a general weighted method for calculating fail-safe numbers in meta-analysis. Evolution. 2005;59:464–8.
Muthén L, Muthén B. Mplus user’s guide. Los Angeles: Muthen & Muthen; 1998–2012.
Cheung M. A model for integrating fixed-, random-, and mixed-effects meta-analyses into structural equation modeling. Psychol Methods. 2008;13:182–202.
Hox J, editor. Multilevel analysis: techniques and applications. 2nd ed. New York; 2010.
Froot K. Consistent covariance matrix estimation with cross-sectional dependence and heteroskedasticity in financial data. J Financ Quant Anal. 1989;24:333–55.
White H. A heteroskedasticity-consistent covariance matrix estimator and a direct test for heteroskedasticity. Econometrica. 1980;48:817–38.
Williams R. A note on robust variance estimation for cluster-correlated data. Biometrics. 2000;56:645–6.
Holviala J, Kraemer WJ, Sillanpaa E, et al. Effects of strength, endurance and combined training on muscle strength, walking speed and dynamic balance in aging men. Eur J Appl Physiol. 2012;112:1335–47.
Liu-Ambrose T, Nagamatsu LS, Graf P, et al. Resistance training and executive functions: a 12-month randomized controlled trial. Arch Intern Med. 2010;170:170–8.
Lohne-Seiler H, Torstveit MK, Anderssen SA. Traditional versus functional strength training: effects on muscle strength and power in the elderly. J Aging Phys Act. 2013;21:51–70.
Ramsbottom R, Ambler A, Potter J, et al. The effect of 6 months training on leg power, balance, and functional mobility of independently living adults over 70 years old. J Aging Phys Act. 2004;12:497–510.
Sayers SP, Gibson K. A comparison of high-speed power training and traditional slow-speed resistance training in older men and women. J Strength Cond Res. 2010;24:3369–80.
Latham NK, Bennett DA, Stretton CM, et al. Systematic review of progressive resistance strength training in older adults. J Gerontol A Biol Sci Med Sci. 2004;59:48–61.
Steib S, Schoene D, Pfeifer K. Dose-response relationship of resistance training in older adults: a meta-analysis. Med Sci Sports Exerc. 2010;42:902–14.
Hazell T, Kenno K, Jakobi J. Functional benefit of power training for older adults. J Aging Phys Act. 2007;15:349–59.
Porter MM. Power training for older adults. Appl Physiol Nutr Metab. 2006;31:87–94.
McComas AJ. Skeletal muscle: form and function. Champaign: Human Kinetics; 1996.
Straight CR, Brady AO, Evans E. Sex-specific relationships of physical activity, body composition, and muscle quality with lower-extremity physical function in older men and women. Menopause. 2015;22:297–303.
Jadad AR, Moore RA, Carroll D, et al. Assessing the quality of reports of randomized clinical trials: is blinding necessary? Control Clin Trials. 1996;17:1–12.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
No sources of funding were used to assist in the preparation of this review.
Conflict of interest
Chad Straight, Jacob Lindheimer, Anne Brady, Rodney Dishman, and Ellen Evans declare that they have no conflicts of interest relevant to the content of this review.
Rights and permissions
About this article

Cite this article
Straight, C.R., Lindheimer, J.B., Brady, A.O. et al. Effects of Resistance Training on Lower-Extremity Muscle Power in Middle-Aged and Older Adults: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Sports Med 46, 353–364 (2016). https://doi.org/10.1007/s40279-015-0418-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40279-015-0418-4