
Abstract
Background and Objective
The energetic cost of cycling (CE) is a major contributor to cycling performance but whether CE can be improved by exercise intervention remains uncertain. Here, we sought to systematically review and determine the effect of exercise training on CE in healthy humans.
Methods
MEDLINE, Scopus, and Web of Science were searched since their inceptions up until December 2014 for articles assessing the effect of exercise training in healthy subjects on CE, as determined by cycling economy or efficiency. Meta-analyses were performed to determine the standardized mean difference (SMD) in CE between post- and pre-training measurements. Subgroup and meta-regression analyses were used to evaluate potential moderating/confounding factors.
Results
Fifty-one studies were included after systematic review, comprising a total of 531 healthy subjects (mean age = 20–66 years). Exercise interventions primarily consisted of endurance and/or strength training ranging from 4 to 34 weeks of duration. After data pooling, the meta-analysis revealed that CE was improved with strength training alone or along with endurance training (n = 16, SMD = −0.50, P < 0.0001) but not with endurance training alone (n = 33, SMD = −0.18, P = 0.08). In further subgroup analyses, endurance training alone was effective in improving CE in previously untrained (n = 20, SMD = −0.21, P = 0.04) but not in trained (n = 6, SMD = 0.09, P = 0.75) subjects. The SMD in CE was associated with the duration of training (n = 51, B = −0.03, P = 0.0002).
Conclusion
The current meta-analysis provides evidence that CE is improved by exercise training, particularly when strength training or untrained subjects are included.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
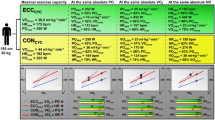
The energetic cost of cycling may be improved by exercise training in healthy humans. |
Exercise programs including strength training improve the energetic cost of cycling in previously trained or untrained subjects. |
Endurance training is only effective at improving the energetic cost of cycling in previously untrained subjects. |
1 Introduction
Humans exhibit a gain in oxygen uptake (VO2) of 14–25 mL·min−1·W−1 during submaximal cycle ergometer exercise [1–18], which roughly corresponds to 12–21 % mechanical efficiency as determined by the ratio of external work to total energy expenditure [19]. In the context of any activity limited by the capacity to expend energy, such as exercise performance, a high exercise economy and efficiency, as represented by low VO2and caloric cost during submaximal exercise, respectively, is of paramount importance [20–23]. Hence, there is a particular interest to identify potential determinants of and strategies to reduce the energetic cost of exercise (EE) [24–26].
Whole-body EE is determined by the combination of efficiencies along the chain of energy transformation and relates to biochemical, physiological, anatomical, and biomechanical factors [27, 28]. Given the relatively fixed body position during cycling, biomechanical aspects are seemingly a less relevant component of the energetic cost of cycling (CE) than running (RE), which might explain, in part, the lower between-individual variability in CE vs. RE [20, 26]. In contrast to other major determinants of exercise performance (e.g., maximal oxygen consumption, lactate threshold), relatively little is known regarding the trainability of EE [29]. It seems reasonable to expect changes in EE following interventions inducing widespread adaptations such as exercise training; indeed, a range of exercise interventions are suggested to improve RE [30]. However, it remains unclear whether CE is improved with exercise training [20, 31, 32], despite related research spans over 4 decades [1–18, 22, 33–48]. Presumably, the small sample size as well as distinct training characteristics, study population, and methodology of individual studies may have compounded the impact of exercise training on CE [1–18, 22, 33–48]. In this regard, a meta-analytical approach may contribute to clarify the effect of exercise training on CE, but to our knowledge, this has not yet been performed.
Therefore, the purpose of this study was to perform a systematic review and meta-analysis on the effect of exercise training on CE in healthy subjects as well as to identify potential moderating/confounding factors.
2 Methods
The review was conducted according to the Meta-analysis Of Observational Studies in Epidemiology (MOOSE) Group guidelines [49].
2.1 Data Sources and Searches
Our systematic search included the databases MEDLINE, Scopus, and Web of Science, from inception until December 2014. We used combinations of the subject headings ‘healthy’, ‘training’, ‘exercise’, ‘efficiency’, and ‘economy’; the search strategy for MEDLINE is shown in Fig. S1. We also performed hand searching in reviews identified through the systematic search, articles included in the meta-analysis, related citations in MEDLINE, personal bibliography, and Google.
2.2 Article Selection
To be included in the analysis, an original research article had to assess CE before and after an exercise training intervention in healthy subjects. Studies were excluded if they complied with the above criteria but involved other interventions deemed likely to influence CE. Likewise, studies were excluded if they assessed CE only at exercise intensities above the LT, to limit the potential confounding influence of anaerobic energy systems on the effect of exercise training on CE. In addition, if VO2 values during the CE test were divided by weight, the latter had to be not significantly altered by the training intervention. In the event of multiple publications pertaining to the same research, the first published or more comprehensive report was included. Inclusion of articles in our analysis was not limited by publication status or language.
2.3 Data Extraction and Quality Assessment
The following variables were summarized in a pre-formatted spreadsheet: authors, year of publication, characteristics of study participants (n, age, sex, height, weight, body fat, lean mass, body mass index, ventilation, heart rate, stroke volume, cardiac output, arteriovenous oxygen difference, lactate, blood pressure, vascular peripheral resistance, blood volume, red cell volume, Hb concentration, hematocrit, fiber-type distribution, mitochondrial content, muscle capillarization, maximal oxygen consumption, respiratory exchange ratio, maximal power with incremental exercise, maximal voluntary contraction, ratio of perceived exertion, fitness status, nutritional status, health status), exercise training features (type, modality, intensity, session length, frequency, duration), and characteristics of the CE assessment (workload, length, cadence, units of measurement). In the case of concurrent reports of CE at different workloads, the CE assessment at the lowest workload, after 5 min of warm-up, was used in the meta-analysis [6, 11, 14, 18, 22, 41, 43]. In the case of concurrent VO2 (l·min−1) and other units of measurement of CE, the former was used in the meta-analysis given its prevailing report, to attenuate the methodological variability between studies [1, 4, 44]. A systematic appraisal of quality for observational research (SAQOR) [50], previously applied in meta-analysis of observational studies evaluating the effect of exercise training [51], was performed to determine study quality. The SAQOR was adapted to assess (1) the study sample, (2) quality of CE assessment, (3) confounding variables, and (4) data. Overall, the SAQOR was scored out of 15, quality deemed better with a greater score (0–5 low, 6–10 moderate, 11–15 high).
2.4 Data Synthesis and Analysis
The meta-analysis and related analyses were performed using Review Manager software (RevMan 5.3, Cochrane Collaboration, Oxford, UK) and Comprehensive Meta-analysis software (version 2, Biostat, Englewood, NJ, USA). The primary outcome was the standardized mean difference (SMD) between post- and pre-training measurements in CE. The SMD summary statistic allowed us to standardize values obtained using different methods into a uniform scale to complete the meta-analysis [52]. Each SMD was weighted by the inverse variance and they were pooled with a random-effects model [52, 53]. According to Cohen’s conventional criteria [54], SMD of 0.2, 0.5, and 0.8 represents small, medium, and large effect sizes, respectively.
Heterogeneity among studies, defined as the variation in the intervention effects that are not compatible with chance alone, was assessed using the chi-squared test for heterogeneity and I 2 statistics. Potential moderating/confounding factors influencing the SMD in CE were evaluated by subgroup analysis comparing studies grouped by dichotomous variables. In addition, meta-regression analyses were performed to evaluate the associations between the SMD in CE and quantitative variables. In all meta-regression models, studies were weighted by the inverse variance of the dependent variable. Potential moderating/confounding factors were entered as independent variables in regressions models with the SMD in CE as the dependent variable. A negative association represents an increased positive effect of training on CE correlated with higher values of the associated variable, and vice versa. Publication and/or other biases were evaluated by the Begg and Mazumdar’s rank correlation test, Egger’s regression test, and visual inspection of funnel plot symmetry [52, 55]. A P value of less than 0.05 was considered statistically significant.
3 Results
3.1 Study Selection and Characteristics
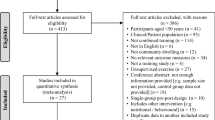
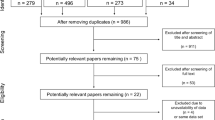
The process of article selection is illustrated in the flow diagram (Fig. 1), which resulted in the inclusion of 35 articles. Twelve of these articles comprised separate study groups [1, 2, 7, 11, 14–16, 34, 35, 38, 39, 48], each of which was evaluated as an individual study in the meta-analysis. Table 1 illustrates the main characteristics of the included 51 studies, comprising a total of 531 healthy (mostly male) subjects with a mean age ranging from 20 to 66 years. Twenty-six studies involved previously untrained subjects, 17 studies comprised trained subjects, while 8 studies did not report fitness status. Among the latter, none reported high VO2max levels according to age- and sex-adjusted guidelines [56]. The majority of the training interventions consisted of endurance- and/or strength-structured training programsof variable intensity performed by means of cycle ergometry, treadmill/running, and/or resistance exercise, ranging from 0.71 to 17 h per week and from 4 to 34 weeks of duration (Table 2). The quality of the studies was moderate. The mean score was 7.4 ± 2.1 out of a possible 15 points (Table S1). As for the evaluation of potential biases, the funnel plot (Fig. S2), Begg and Mazumdar’s rank correlation test (P = 0.62), and Egger’s regression test (P = 0.81) suggested the absence of publication and/or other biases for the SMD in CE in the studies included in the meta-analysis.

Flow diagram of the process of article selection. CE cycling energetic cost
3.2 Effect of Exercise Training on Cycling Economy (CE)
CE was determined in all studies during cycle ergometer exercise of low, moderate, or moderate-to-high intensity (Table 1). CE was predominantly expressed as VO2 (l·min−1) at a given submaximal workload (i.e., ‘gross’ CE). After data pooling, the meta-analysis revealed an improved CE after training (SMD = −0.28, 95 % confidence interval = −0.44, −0.13; P = 0.0004) (Fig. 2). Heterogeneity was detected between studies (I 2 = 36 %, P = 0.007). In subgroup analyses (Table 3), there was no effect of training on CE in studies including only female subjects (n = 4) or previously trained subjects (n = 17) (P = 0.10 and P = 0.19, respectively). Likewise, studies applying only endurance training (n = 33), assessing CE with free/unknown cadence (i.e., pedaling rate) (n = 16), or through multiple workloads (n = 11) did not result in improved CE after training (P = 0.08, P = 0.10, and P = 0.25, respectively). In previously trained subjects, CE was improved only in studies applying strength training (n = 11), while in previously untrained subjects, both endurance (n = 20) and strength training alone or along with endurance training (n = 5) resulted in improved CE. Nonetheless, none of the aforementioned subgroup analyses, except for the comparison between types of training in all subjects, revealed a significant difference between subgroups (P Difference > 0.05).

Forest plots of the standardized mean difference (SMD) between post- and pre-training measurements in CE. Squares the SMD for each study. Diamonds represents the pooled SMD across studies. CI confidence interval, CE cycling energetic cost, df degrees of freedom, IV inverse variance, SD standard deviation
3.3 Meta-Regression Analyses
Table 4 presents the associations between the SMD in CE and potential moderating/confounding factors. Considering all studies included in the meta-analysis, the SMD in CE was (1) positively associated with ∆body fat (B = 0.31, 95 % CI [0.11, 0.50]) and cadence (B = 0.04, [0.02, 0.06]) in the CE test, and (2) negatively associated with total hours (B = −0.00, 95 % CI [−0.01, −0.00]) and duration (B = −0.03, [−0.05, −0.01]) of training and pre training VO2 (B = −0.53, [−0.95, −0.11]) in the CE test. These and further associations were observed when potential moderating/confounding factors of the SMD in CE were assessed separately according to the training status of study participants or the type of training intervention implemented (see details in Table 4).
4 Discussion
In this systematic review and meta-analysis, we pooled and analyzed data from 51 studies assessing the effect of exercise training interventions on CE in a total of 531 healthy humans across a wide range of ages. The key observations of this analysis are: (1) strength training alone or along with endurance training improves CE and shows (2) a superior effect compared with endurance training alone; in turn, (3) endurance training alone is only effective at improving CE in previously untrained subjects.
Among the major contributors to endurance cycling performance, CE is considered the slowest responsive factor, if at all, to training [20, 57]. Nonetheless, given that even minor improvements in CE may yield substantial increases in performance [58], interventions/training regimes that may enhance CE are of great interest [29]. Herein, the meta-analytical evidence demonstrates that exercise programs including strength training improves CE to a moderate degree in previously trained and untrained healthy subjects (Fig. 2; Table 3). This agrees with the established improvement in RE following strength training [24]. Provided a negligible influence of biomechanics on CE, it seems unlikely that the effect of strength training on CE are related to biomechanical factors. Putative mechanisms by which strength training may enhance CE fundamentally comprise improved neuromuscular coordination [59, 60] and increased force per motor unit leading to reduced muscle activation at a given workload [61]. Importantly, none of the studies included in this meta-analysis reported the inclusion of strength-trained subjects (Table 1), in whom strength adaptations and possibly CE improvements might be of lesser magnitude [62]. Moreover, there might be quantitatively and qualitatively distinct adaptations and thereby CE modification in accordance with different modalities of strength training [63]; however, limited data availability precluded us to separately analyze the impact of strength training modalities in the present work. Regardless, the low variability of the effect of strength training alone or along with endurance training on CE is noteworthy (I 2 = 13 %, P = 0.31) (Fig. 2), suggesting similar CE responsiveness to exercise interventions including strength training.
On the basis of cross-sectional studies, endurance training is believed to have no influence on CE [57, 64, 65]. Yet, case reports in elite athletes have shown marked improvements in CE with years of endurance training [66, 67]. The present study reveals a small effect of endurance training (lasting 1–4 months) on CE in previously untrained, but not trained, subjects (Table 3). This suggests that (1) the nature and/or extent of typical short-term adaptations to endurance training such as increased oxygen delivery [68], muscle capillarization and mitochondrial content [69], among others, have little impact on CE and (2) longer endurance training interventions may be required to improve CE in physically fit humans. With respect to the latter, it has been hypothesized that the enhancement of CE with long-term endurance training is attributed to large increases in the percentage of type I muscle fibers [67], although related experimental evidence in humans is lacking. Additionally, changes in blood flow distribution following years of endurance training might influence CE [70]. In this regard, endurance athletes exhibit increased oxygen extraction, lower limb blood flow, and similar vascular conductanceper submaximal workloadcompared with untrained peers [70–72], conceivably due, in part, to a more efficient limb blood flow distribution towards exercising skeletal muscle [70]. This may contribute to lower myocardial work and improve CE, albeit onlyto a minor degree, in endurance athletes. Otherwise, long-term metabolic adaptations to endurance training [73–75] do not seem to affect the VO2/ATP production ratio component of CE because mithocondrial efficiency is similar over a wide range of fitness conditions [21, 25, 74]. In turn, the endurance training-induced improvement in ‘metabolic stability’ (i.e., reduced changes in the concentrations of muscle metabolites such as ADP, AMP, inosine monophosphate, creatine, inorganic phosphate, and H+ for a given ATP turnover) may be crucial to limit muscle fatigue, VO2 slow component, and CE impairment occurring at heavy and severe exercise intensities, particularly through a decrease in the ATP use/power output ratio [21–23].
The observation that CE was enhanced with the duration of the exercise intervention might challenge the independent status of the above findings. Yet, in the included studies no difference was detected for the weighted average duration of training according to type of training (P = 0.12) and fitness status (P = 0.18). It should be noted that there was no association between the SMD in CE and the duration of the intervention in studies including trained subjects, whereas a linear association was found in studies including untrained subjects (Table 4). This may denote the presence of a duration threshold for the impact of training on CE in previously trained subjects. In addition, several anthropometrical and methodological characteristics were associated with the effect of training on CE when considering all studies (Table 4). For instance, the higher the submaximal VO2 during baseline CE assessment, the greater the favorable effect of training was on CE. This could suggest an increased susceptibility for CE improvement in subjects with low CE at baseline. Likewise, the decrease in body fat percentage with training was directly related to the improvement in CE. Whilst speculative, a lower body fat percentage, if accompanied by reduced leg mass, may reduce CE through a decreased cost of leg movement. Furthermore, we detected an enhanced positive effect of training on CE with lower pedaling rates during the CE assessment. This adds to previous meta-analytical findings showing a worsened CE with higher cadence in un- to highly trained subjects [32], which also may imply that potential changes in CE may have been overlooked if determined with higher vs. lower cadences. Ultimately, given the nature and limited bivariate design of the heterogeneity analyses here applied, all associations should be considered exploratory and not as proof of causality [76].
There are additional limitations in this systematic review and meta-analysis worth addressing.
First, the majority of the included studies (44 out of 51) used VO2 during submaximal cycling at a given workload, i.e., economy, as a measure of CE (Table 1), thus the latter could have been modulated by training-induced adaptations in substrate metabolism (e.g., increased fat use and higherVO2/ATP production ratio). Nonetheless, there was no correlation between the SMD in CE and training-related changes in respiratory exchange ratio during the CE assessment (19 studies). This suggests that potential adaptations in substrate use did not affect the results of this meta-analysis, as indeed was also supported by the similar SMD in CE between studies that expressed CE in economy vs. efficiency units (P = 0.50). Second, studies assessing CE only at exercise intensities reasonably above the LT were excluded. This could have underestimated the effect of exercise training on CE because greater attenuation of the VO2/W slope above vs. below the LT after training has been reported [22, 41, 43]. Third, few studies comprised female individuals, which hinders any conclusion on the effect of sex on CE. Finally, the methodological quality of the included studies was determined as moderate, although there was no evidence of publication bias (Fig. S2).
5 Conclusions
The current meta-analysis demonstrates that exercise training may improve CE in healthy subjects. Such improvement is observed with exercise programs including, albeit not restricted to, strength training in previously trained subjects. In untrained subjects, CE is also enhanced by endurance training. These data therefore buttress the addition of strength training to any exercise program aiming to enhance CE and thereby endurance performance. Further research is needed to establish the most effective exercise strategy to improve CE in athletic populations.
References
Wang E, Naess MS, Hoff J, Albert TL, Quan P, Richardson RS, et al. Exercise-training-induced changes in metabolic capacity with age: the role of central cardiovascular plasticity. Age. 2014;36(2):665–76.
Shepherd SO, Cocks M, Tipton KD, Ranasinghe AM, Barker TA, Burniston JG, et al. Sprint interval and traditional endurance training increase net intramuscular triglyceride breakdown and expression of perilipin 2 and 5. J Physiol. 2013;591(Pt 3):657–75.
Zoladz JA, Szkutnik Z, Majerczak J, Grandys M, Duda K, Grassi B. Isometric strength training lowers the O2 cost of cycling during moderate-intensity exercise. Eur J Appl Physiol. 2012;112(12):4151–61.
Porcelli S, Marzorati M, Pugliese L, Adamo S, Gondin J, Bottinelli R, et al. Lack of functional effects of neuromuscular electrical stimulation on skeletal muscle oxidative metabolism in healthy humans. J Appl Physiol (1985). 2012;113(7):1101–9.
Ichinose T, Nomura S, Someya Y, Akimoto S, Tachiyashiki K, Imaizumi K. Effect of endurance training supplemented with green tea extract on substrate metabolism during exercise in humans. Scand J Med Sci Sports. 2011;21(4):598–605.
Majerczak J, Karasinski J, Zoladz JA. Training induced decrease in oxygen cost of cycling is accompanied by down-regulation of SERCA expression in human vastus lateralis muscle. J Physiol Pharmacol. 2008;59(3):589–602.
Van Zant RS, Bouillon LE. Strength cycle training: effects on muscular strength and aerobic conditioning. J Strength Cond Res. 2007;21(1):178–82.
Hansen EA, Raastad T, Hallen J. Strength training reduces freely chosen pedal rate during submaximal cycling. Eur J Appl Physiol. 2007;101(4):419–26.
Jacobs KA, Krauss RM, Fattor JA, Horning MA, Friedlander AL, Bauer TA, et al. Endurance training has little effect on active muscle free fatty acid, lipoprotein cholesterol, or triglyceride net balances. Am J Physiol Endocrinol Metab. 2006;291(3):E656–65.
Dressendorfer RH, Petersen SR, Lovshin SEM, Hannon JL, Lee SF, Bell GJ. Performance enhancement with maintenance of resting immune status after intensified cycle training. Clin J Sport Med. 2002;12(5):301–7.
Proctor DN, Miller JD, Dietz NM, Minson CT, Joyner MJ. Reduced submaximal leg blood flow after high-intensity aerobic training. J Appl Physiol (1985). 2001;91(6):2619–27.
Costes F, Prieur F, Feasson L, Geyssant A, Barthelemy JC, Denis C. Influence of training on NIRS muscle oxygen saturation during submaximal exercise. Med Sci Sports Exerc. 2001;33(9):1484–9.
Bergman BC, Butterfield GE, Wolfel EE, Casazza GA, Lopaschuk GD, Brooks GA. Evaluation of exercise and training on muscle lipid metabolism. Am J Physiol. 1999;276(1 Pt 1):E106–17.
Beere PA, Russell SD, Morey MC, Kitzman DW, Higginbotham MB. Aerobic exercise training can reverse age-related peripheral circulatory changes in healthy older men. Circulation. 1999;100(10):1085–94.
Gissane C, Corrigan DL, White JA. Gross efficiency responses to exercise conditioning in adult males of various ages. J Sports Sci. 1991;9(4):383–91.
Gardner AW, Poehlman ET, Corrigan DL. Effect of endurance training on gross energy expenditure during exercise. Hum Biol. 1989;61(4):559–69.
Hagberg JM, Hickson RC, Ehsani AA, Holloszy JO. Faster adjustment to and recovery from submaximal exercise in the trained state. J Appl Physiol Respir Environ Exerc Physiol. 1980;48(2):218–24.
Ekblom B, Astrand PO, Saltin B, Stenberg J, Wallstrom B. Effect of training on circulatory response to exercise. J Appl Physiol. 1968;24(4):518–28.
Coyle EF, Sidossis LS, Horowitz JF, Beltz JD. Cycling efficiency is related to the percentage of type I muscle fibers. Med Sci Sports Exerc. 1992;24(7):782–8.
Joyner MJ, Coyle EF. Endurance exercise performance: the physiology of champions. J Physiol. 2008;586(1):35–44.
Grassi B, Rossiter HB, Zoladz JA. Skeletal muscle fatigue and decreased efficiency: two sides of the same coin? Exerc Sport Sci Rev. 2015;43(2):75–83.
Majerczak J, Korostynski M, Nieckarz Z, Szkutnik Z, Duda K, Zoladz JA. Endurance training decreases the non-linearity in the oxygen uptake-power output relationship in humans. Exp Physiol. 2012;97(3):386–99.
Jones AM, Grassi B, Christensen PM, Krustrup P, Bangsbo J, Poole DC. Slow component of VO2 kinetics: mechanistic bases and practical applications. Med Sci Sports Exerc. 2011;43(11):2046–62.
Beattie K, Kenny IC, Lyons M, Carson BP. The effect of strength training on performance in endurance athletes. Sports Med. 2014;44(6):845–65.
Mogensen M, Bagger M, Pedersen PK, Fernstrom M, Sahlin K. Cycling efficiency in humans is related to low UCP3 content and to type I fibres but not to mitochondrial efficiency. J Physiol. 2006;571(Pt 3):669–81.
Moore IS, Jones AM, Dixon SJ. Mechanisms for improved running economy in beginner runners. Med Sci Sports Exerc. 2012;44(9):1756–63.
Williams KR, Cavanagh PR. Relationship between distance running mechanics, running economy, and performance. J Appl Physiol (1985). 1987;63(3):1236–45.
Williams KR. The relationship between mechanical and physiological energy estimates. Med Sci Sports Exerc. 1985;17(3):317–25.
Lundby C, Robach P. Performance enhancement: what are the physiological limits? J Physiol. 2015;30(4):282–92.
Barnes KR, Kilding AE. Strategies to improve running economy. Sports Med. 2015;45(1):37–56.
Hopker J, Passfield L, Coleman D, Jobson S, Edwards L, Carter H. The effects of training on gross efficiency in cycling: a review. Int J Sports Med. 2009;30(12):845–50.
Ettema G, Loras HW. Efficiency in cycling: a review. Eur J Appl Physiol. 2009;106(1):1–14.
Ronnestad BR, Hansen EA, Raastad T. Strength training affects tendon cross-sectional area and freely chosen cadence differently in noncyclists and well-trained cyclists. J Strength Cond Res. 2012;26(1):158–66.
Dhamrait SS, Williams AG, Day SH, Skipworth J, Payne JR, World M, et al. Variation in the uncoupling protein 2 and 3 genes and human performance. J Appl Physiol. 2012;112(7):1122–7.
Aagaard P, Andersen JL, Bennekou M, Larsson B, Olesen JL, Crameri R, et al. Effects of resistance training on endurance capacity and muscle fiber composition in young top-level cyclists. Scand J Med Sci Sports. 2011;21(6):e298–307.
Sunde A, Storen O, Bjerkaas M, Larsen MH, Hoff J, Helgerud J. Maximal strength training improves cycling economy in competitive cyclists. J Strength Cond Res. 2010;24(8):2157–65.
Lecoultre V, Boss A, Tappy L, Borrani F, Tran C, Schneiter P, et al. Training in hypoxia fails to further enhance endurance performance and lactate clearance in well-trained men and impairs glucose metabolism during prolonged exercise. Exp Physiol. 2010;95(2):315–30.
Paton CD, Hopkins WG, Cook C. Effects of low- vs. high-cadence interval training on cycling performance. J Strength Cond Res. 2009;23(6):1758–63.
Burgomaster KA, Howarth KR, Phillips SM, Rakobowchuk M, Macdonald MJ, McGee SL, et al. Similar metabolic adaptations during exercise after low volume sprint interval and traditional endurance training in humans. J Physiol. 2008;586(1):151–60.
Roels B, Millet GP, Marcoux CJ, Coste O, Bentley DJ, Candau RB. Effects of hypoxic interval training on cycling performance. Med Sci Sports Exerc. 2005;37(1):138–46.
Prieur F, Benoit H, Busso T, Castells J, Denis C. Effect of endurance training on the VO2-work rate relationship in normoxia and hypoxia. Med Sci Sports Exerc. 2005;37(4):664–9.
Paton CD, Hopkins WG. Combining explosive and high-resistance training improves performance in competitive cyclists. J Strength Cond Res. 2005;19(4):826–30.
Loveless DJ, Weber CL, Haseler LJ, Schneider DA. Maximal leg-strength training improves cycling economy in previously untrained men. Med Sci Sports Exerc. 2005;37(7):1231–6.
Hintzy F, Mourot L, Perrey S, Tordi N. Effect of endurance training on different mechanical efficiency indices during submaximal cycling in subjects unaccustomed to cycling. Can J Appl Physiol. 2005;30(5):520–8.
Carter SL, Rennie C, Tarnopolsky MA. Substrate utilization during endurance exercise in men and women after endurance training. Am J Physiol Endocrinol Metab. 2001;280(6):E898–907.
Friedlander AL, Casazza GA, Horning MA, Huie MJ, Piacentini MF, Trimmer JK, et al. Training-induced alterations of carbohydrate metabolism in women: women respond differently from men. J Appl Physiol (1985). 1998;85(3):1175–86.
Friedlander AL, Casazza GA, Horning MA, Huie MJ, Brooks GA. Training-induced alterations of glucose flux in men. J Appl Physiol (1985). 1997;82(4):1360–9.
Clausen JP, Klausen K, Rasmussen B, Trap-Jensen J. Central and peripheral circulatory changes after training of the arms or legs. Am J Physiol. 1973;225(3):675–82.
Stroup DF, Berlin JA, Morton SC, Olkin I, Williamson GD, Rennie D, et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA. 2000;283(15):2008–12.
Ross LE, Grigoriadis S, Mamisashvili L, Koren G, Steiner M, Dennis CL, et al. Quality assessment of observational studies in psychiatry: an example from perinatal psychiatric research. Int J Methods Psychiatr Res. 2011;20(4):224–34.
Montero D, Diaz-Cañestro C, Lundby C. Endurance training and VO2max: role of maximal cardiac output and oxygen extraction. Med Sci Sports Exerc. 2015 (Epub ahead of print).
Higgins JPT, Green S, (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from http://www.cochrane-handbook.org. Accessed 15 Dec 2014.
DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986;7(3):177–88.
Cohen J. Statistical power analysis for the behavioral sciences. 2nd ed. In: Hillsdale N, editor. Hillsdale: Lawrence Erlbaum Associates Publishers; 1988.
Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315(7109):629–34.
ACSM. ACSM’s guidelines for exercise testing and prescription. Hagerstown: Lippincott Raven; 2009.
Moseley L, Achten J, Martin JC, Jeukendrup AE. No differences in cycling efficiency between world-class and recreational cyclists. Int J Sports Med. 2004;25(5):374–9.
Olds T, Norton K, Craig N, Olive S, Lowe E. The limits of the possible: models of power supply and demand in cycling. Aust J Sci Med Sport. 1995;27(2):29–33.
Paavolainen L, Hakkinen K, Hamalainen I, Nummela A, Rusko H. Explosive-strength training improves 5-km running time by improving running economy and muscle power. J Appl Physiol (1985). 1999;86(5):1527–33.
Sale DG. Neural adaptation to resistance training. Med Sci Sports Exerc. 1988;20(5 Suppl):S135–45.
Moritani T, deVries HA. Neural factors versus hypertrophy in the time course of muscle strength gain. Am J Phys Med. 1979;58(3):115–30.
Kraemer WJ, Adams K, Cafarelli E, Dudley GA, Dooly C, Feigenbaum MS, et al. American College of Sports Medicine position stand. Progression models in resistance training for healthy adults. Med Sci Sports Exerc. 2002;34(2):364–80.
Vissing K, Brink M, Lonbro S, Sorensen H, Overgaard K, Danborg K, et al. Muscle adaptations to plyometric vs. resistance training in untrained young men. J Strength Cond Res. 2008;22(6):1799–810.
Marsh AP, Martin PE, Foley KO. Effect of cadence, cycling experience, and aerobic power on delta efficiency during cycling. Med Sci Sports Exerc. 2000;32(9):1630–4.
Nickleberry BL Jr, Brooks GA. No effect of cycling experience on leg cycle ergometer efficiency. Med Sci Sports Exerc. 1996;28(11):1396–401.
Jones AM. The physiology of the world record holder for the women’s marathon. Int J Sports Sci Coaching. 2006;1:101–16.
Coyle EF. Improved muscular efficiency displayed as Tour de France champion matures. J Appl Physiol (1985). 2005;98(6):2191–6.
Bonne TC, Doucende G, Fluck D, Jacobs RA, Nordsborg NB, Robach P, et al. Phlebotomy eliminates the maximal cardiac output response to six weeks of exercise training. Am J Physiol Regul Integr Comp Physiol. 2014;306(10):R752–60.
Hoppeler H, Howald H, Conley K, Lindstedt SL, Claassen H, Vock P, et al. Endurance training in humans: aerobic capacity and structure of skeletal muscle. J Appl Physiol (1985). 1985;59(2):320–7.
Kalliokoski KK, Oikonen V, Takala TO, Sipila H, Knuuti J, Nuutila P. Enhanced oxygen extraction and reduced flow heterogeneity in exercising muscle in endurance-trained men. Am J Physiol Endocrinol Metab. 2001;280(6):E1015–21.
Carrick-Ranson G, Hastings JL, Bhella PS, Fujimoto N, Shibata S, Palmer MD, et al. The effect of lifelong exercise dose on cardiovascular function during exercise. J Appl Physiol (1985). 2014;116(7):736–45.
Fleg JL, Schulman SP, O’Connor FC, Gerstenblith G, Becker LC, Fortney S, et al. Cardiovascular responses to exhaustive upright cycle exercise in highly trained older men. J Appl Physiol (1985). 1994;77(3):1500–6.
Coffey VG, Hawley JA. The molecular bases of training adaptation. Sports Med. 2007;37(9):737–63.
Jacobs RA, Lundby C. Mitochondria express enhanced quality as well as quantity in association with aerobic fitness across recreationally active individuals up to elite athletes. J Appl Physiol (1985). 2013;114(3):344–50.
Jacobs RA, Fluck D, Bonne TC, Burgi S, Christensen PM, Toigo M, et al. Improvements in exercise performance with high-intensity interval training coincide with an increase in skeletal muscle mitochondrial content and function. J Appl Physiol (1985). 2013;115(6):785–93.
Baker WL, White CM, Cappelleri JC, Kluger J, Coleman CI. Understanding heterogeneity in meta-analysis: the role of meta-regression. Int J Clin Pract. 2009;63(10):1426–34.
Acknowledgments
No sources of funding were used to assist in the preparation of this review.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
David Montero and Carsten Lundby declare that they have no conflict of interest.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Montero, D., Lundby, C. The Effect of Exercise Training on the Energetic Cost of Cycling. Sports Med 45, 1603–1618 (2015). https://doi.org/10.1007/s40279-015-0380-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40279-015-0380-1