
Abstract
Background
Team ball sports such as soccer, basketball and volleyball have high participation levels worldwide. Musculoskeletal injuries are common in team ball sports and are associated with significant treatment costs, participation loss and long-term negative side effects. The results of recent randomized controlled trials provide support for the protective effect of injury-prevention exercise programmes (IPEPs) in team ball sports, but also highlight that achieving adequate compliance can be challenging. A key process in enhancing the ultimate impact of team ball sport IPEPs is identifying the specific implementation components that influence the adoption, execution and maintenance of these interventions. Despite this, no systematic review focussing on the specific implementation components of team ball sport IPEPs has been conducted.
Objectives
Our objective was to assess the reporting of specific implementation components in the published literature on team ball sport IPEPs using the Reach Efficacy Adoption Implementation Maintenance (RE-AIM) framework.
Methods
Six electronic databases were systematically searched from inception to December 2012 for papers reporting team ball sport IPEP trials. All eligible papers were independently evaluated by two raters before reaching consensus on the reporting of individual RE-AIM items, using the RE-AIM Model Dimension Items Checklist (RE-AIM MDIC).
Results
A total of 60 papers, reporting 52 unique intervention trials, met eligibility criteria. Before consensus, the level of agreement across all trials between reviewers using the RE-AIM MDIC ranged from 81 to 91 %. The RE-AIM MDIC dimension of ‘efficacy’ had the highest level of reporting, with the five individual items in this dimension reported in 19–100 % of eligible trials (mean 58 %). The RE-AIM MDIC dimension ‘maintenance-setting level’ had the lowest level of reporting, with none of the four individual items in this dimension reported. For other dimensions, the mean level of reporting and range across items were ‘reach’ 34 % (12–60 %); ‘adoption-setting level’ 1 % (0–2 %); ‘adoption-delivery agent level’ 7 % (4–10 %); ‘implementation’ 36 % (13–63 %) and ‘maintenance individual level’ 1 % (0–4 %).
Conclusion
Information on the specific implementation components of team ball sport IPEPs in published studies is scarce. In particular, major reporting gaps exist regarding the adoption and maintenance of these programmes. The RE-AIM MDIC can be successfully applied to reviewing literature in this context.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
1 Introduction
Team ball sports enjoy worldwide popularity. Soccer alone has over 265 million participants [1]. Injuries in team ball sports are common [2], and injury prevention in this context is important to minimise the associated treatment costs, participation loss and long-term negative side effects [3–5]. Injury-prevention exercise programmes (IPEPs) in team ball sports have shown considerable promise in preventing musculoskeletal injuries [6–8]. However, the full potential of these programmes will only be realised if they are adopted, correctly executed and sustained by their intended end users [9, 10]. There is a real need to identify which specific implementation components of team ball sport IPEPs are critical in achieving the desired injury-prevention outcomes [11–13], to guide their wider and more successful implementation.
Application of established models and frameworks from implementation science has the potential to enhance sports injury-prevention implementation efforts [9, 11, 14]. One such framework, the Reach Efficacy Adoption Implementation Maintenance (RE-AIM) framework, was developed to improve the translatability and impact of health interventions, and has been employed in over 70 published studies across a broad spectrum of health-related fields, including sports injury prevention [9, 14–16]. The framework incorporates five key dimensions [17]:
-
Reach The absolute number, proportion, and representativeness of individuals who are willing to participate in a given initiative, intervention or programme.
-
Efficacy/effectiveness The impact of an intervention on important health outcomes, including potential negative effects, quality of life and economic outcomes.
-
Adoption The absolute number, proportion and representativeness of settings and delivery agents who are willing to initiate a programme.
-
Implementation The degree to which an intervention is delivered as intended, and the time and cost of the intervention.
-
Maintenance The extent to which an intervention is sustained by the targeted individuals and settings over time.
To enhance the ultimate impact of team ball sport IPEPs, consideration of all RE-AIM dimensions is important. It should be noted that the above definition of ‘implementation’, as a specific RE-AIM dimension, differs from the broader definition of implementation in the field of implementation science. In the broad sense, implementation relates to any methods aimed at integrating research findings into practice and/or policy [18].
In the field of sports injury prevention, the RE-AIM framework has primarily been employed to facilitate the planning and evaluation of interventions [9]. However, in other health-related areas, the framework has also been successfully employed as a tool for reviewing published literature [19–21]. Recently, Kessler et al. [22] developed the RE-AIM Model Dimension Items Checklist (MDIC) and reported its application to reviewing project grant applications. This 31-item checklist covers the five RE-AIM dimensions of ‘reach’ (four items), ‘efficacy’ (five items), ‘adoption’ (eight items), ‘implementation’ (five items) and ‘maintenance’ (nine items). Reporting against each item of the MDIC can be coded as ‘yes’, ‘no’, ‘yes – inappropriate use’ or ‘not applicable’. We conducted a systematic review to assess the reporting of specific implementation components of team ball sport IPEP trials as outlined in the RE-AIM MDIC. The aim was to identify the extent to which key factors for ensuring successful implementation of team ball sport IPEPs in real-world settings are reported in published studies. This information is needed to guide future implementation efforts and highlight knowledge gaps requiring further research.
2 Methods
2.1 Search Strategy
The following details reproduce previously reported systematic review methods [23] that also relate to the specific aims of this current review. The following electronic databases were systematically searched from inception to December 2012 by one author (JO’B): PubMed, MEDLINE, CINAHL, Embase, Scopus and the Cochrane Controlled Trials Register. Search terms were combined into the following search strings, representing the key themes: (‘team sport’ OR ‘team sports’ OR soccer OR football OR rugby OR gridiron OR basketball OR netball OR hockey OR handball OR volleyball) AND (program* OR exercise* OR training) AND (injur*) AND (prevent*). Additional papers were sought by scanning the reference lists of retrieved articles and by contacting experts.
2.1.1 Study Eligibility Criteria
All identified records were pooled and duplicates removed. The titles and abstracts of all records were screened for eligibility by one author (JO’B) using the criteria shown in Table 1. The full-text versions of the remaining papers were retrieved before repeating eligibility screening.
2.2 Quality Appraisal Process
All eligible trial reports were first assessed by both authors against a purposely designed RE-AIM screening worksheet. Following consensus on the screening worksheet, all trial reports were assessed using the full RE-AIM MDIC. It was anticipated that this two-stage process would enhance agreement between reviewers.
2.2.1 RE-AIM Screening Worksheet
In order to successfully apply the RE-AIM MDIC to this specific study context, information on the intervention, intervention target and delivery agents is needed [24]. A detailed description of the reporting of these factors has been reported elsewhere [23]. Additionally, the terms ‘primary outcome’ and ‘setting’, as used in the RE-AIM MDIC, need to be applied to the specific study context. Two reviewers independently evaluated all eligible full-text papers using a purposely designed RE-AIM screening worksheet. One worksheet was used for each unique trial: in cases where more than one paper reported the same trial, they were considered together. The reporting of the intervention, primary outcome, intervention target, delivery agents and settings was coded as ‘yes’, ‘no’ or ‘unclear’. In cases coded as ‘yes’, reviewers also recorded their answers to the corresponding questions in the worksheet: ‘What is the intervention?’, ‘What is the outcome?’, ‘Who is the target?’, ‘Who are the delivery agents?’ and ‘What are the settings?’ Table 2 summarises the outcomes of this screening assessment.
Following independent reviewer assessment, consensus was then reached on all screening worksheet items before proceeding to application of the RE-AIM MDIC.
2.2.2 Appraisal with the RE-AIM Model Dimension Items Checklist (RE-AIM MDIC)
Following the screening process, the reporting of all eligible trials was independently assessed by the same two reviewers against the 31-item RE-AIM MDIC. Minor modifications were made to the wording in the MDIC to reflect the specific context of team ball sport (Electronic Supplementary Material [ESM] Table S1). For each individual trial, the results of the screening worksheet were used to guide the coding of the RE-AIM MDIC. For example, if the screening indicated that a trial did not involve any delivery agents, the MDIC items relating to delivery agents were coded as ‘not applicable’. To facilitate this process, a Microsoft Excel™ spreadsheet was formatted for each unique trial, containing both the screening worksheet and the full RE-AIM MDIC (ESM Table S1). Formulae were used to pre-fill certain RE-AIM MDIC items according to the results of the screening worksheet. The types of intervention, primary outcome, intervention target, delivery agents and settings, identified through the screening worksheet, were also automatically entered into the left-hand column of the RE-AIM MDIC, entitled ‘This component refers to’ through the use of formulae (ESM Table S1).
The eligible trial reports were ordered alphabetically by first author, and divided into five batches of approximately equal size, which were reviewed on consecutive days. After reviewing each batch, the reviewers met to discuss their findings. Discrepancies between the two reviewers were resolved through discussion and re-consideration of the RE-AIM MDIC items, before proceeding to the next batch of trial reports. This process was intended to develop consensus on application of the RE-AIM MDIC to this context, rather than to formally test inter-rater reliability. For each batch, the percentage level of agreement between reviewers prior to consensus was calculated as follows: (number of RE-AIM MDIC items with matching codes/total number of RE-AIM MDIC items) × 100.
The proportion of all eligible trials reporting each of the 31 individual RE-AIM MDIC items was calculated as: (number of trials coded as ‘yes’ for the item/total number of trials) × 100. The proportion of all eligible trials reporting each overall RE-AIM dimension was calculated by averaging the proportion of trials reporting each individual RE-AIM MDIC items within the dimension.
3 Results
3.1 Search Strategy
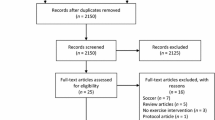
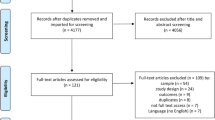
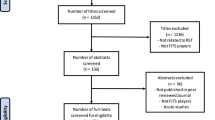
The initial systematic search retrieved a total of 60 eligible papers, covering 52 unique trials. Details of the search are provided in Fig. 1.

Results of the search strategy (PRISMA flowchart) used to identify team ball sport injury-prevention exercise programme trial reports. PRISMA Preferred Reporting Items for Systematic Reviews and Meta-Analyses
3.1.1 Description of Eligible Trials
As multiple papers reporting the same trial were considered together, the following results are presented in terms of the 52 trials. The most commonly investigated sports were soccer (26 trials, 50 % of the total), handball (five trials, 10 %), Australian Football (four trials, 8 %), basketball (four trials, 8 %) and American Football (four trials, 8 %). A total of 23 trials (44 %) included only male players, 17 (33 %) only females and ten (19 %) both sexes, while the sex of participants was not reported in two (4 %) of the trials. Although the eligible trials incorporated a variety of study designs, the majority were randomised controlled trials or cluster-randomised controlled trials, which primarily provide evidence on the efficacy of interventions [9].
3.2 Agreement between Reviewers on Coding the RE-AIM MDIC Prior to Consensus
The level of agreement between the reviewers for each of the five batches of reviewed trial reports, in chronological order, was 81, 90, 89, 90 and 91 %. In comparison, the level of agreement between the same two reviewers in a previous trial, without use of the screening worksheet, was 53 % [24].
3.3 Consensus Codes and Answers for the RE-AIM Screening Worksheet
The consensus codes for the five questions in the screening worksheet are listed in ESM Table S2. The types of reported intervention, intervention target and delivery agents, and the proportion of trials for which each type was reported, have been previously reported [24] and are also summarised in ESM Table S3. The types of reported primary outcome, and the proportion of trials for which each type of primary outcome was reported, are illustrated in Fig. 2, with fuller detail in ESM Table S3. A measure of injury incidence was reported as the primary outcome of interest in 48 (93 %) of the trials. In two (4 %) trials, the primary outcome of interest was related to the behaviour of the coaches delivering an injury-prevention intervention. Other reported primary outcomes of interest were the cross-sectional area of specific muscles [25], and changes in landing skills [26]. The targeting of settings was only reported in one trial, involving 181 female football clubs [27]. Although some studies [6, 28, 29] reported the involvement of settings during the recruitment of participants (e.g. contacting school principals to recruit high school team ball sport players), in these trials the research intervention was targeted at players, rather than those settings.

Percentage of 52 team ball sport injury-prevention exercise programme trials for which each type of primary outcome was reported
3.4 Level of Reporting of Individual RE-AIM MDIC Items
Figure 3 illustrates the proportion of the 52 trials in which each of the 31 individual RE-AIM MDIC items (ESM Table S1) was reported. Results for the individual items are grouped according to the corresponding RE-AIM dimensions of ‘reach’, ‘efficacy/effectiveness’, ‘adoption’ (at both setting and delivery agent levels), ‘implementation’ and ‘maintenance’ (at both individual and setting levels).

Percentage of 52 team ball sport injury-prevention exercise programme (IPEP) trials with reporting of the 31 individual items in the Reach Efficacy Adoption Implementation Maintenance (RE-AIM) Model Dimension Items Checklist (MDIC)
For each RE-AIM MDIC dimension, the average level of reporting across individual items in the dimension, and range across items, are summarised below:
-
Reach: 34 %, range 12–60 %
-
Efficacy/effectiveness: 58 %, range 19–100 %
-
Adoption-setting level: 1 %, range 0–2 %
-
Adoption-delivery agent level: 7 %, range 4–10 %
-
Implementation: 36 %, range 13–63 %
-
Maintenance – individual level: 1 %, range 0–4 %
-
Maintenance-setting level: 0 %, range 0 %
3.5 Reporting of Individual RE-AIM Dimensions
3.5.1 Reach
The percentage of participants excluded by the researchers (MDIC item 1) was reported in 60 % of the trials, and the percentage of eligible participants agreeing to participate (MDIC item 2) was reported in 48 % of trials. A summary of the reported percentage of participants excluded, and the reported percentage of participants agreeing to participate is shown in Table 3. A comparison of the characteristics of participants with non-participants (MDIC item 3) was addressed in 13 % of the eligible trials, and included comparisons of sex [30, 31] and language [32]. The use of qualitative methods (MDIC item 4) was reported in 12 % of trials, with a number of reports identifying the time cost associated with performing the IPEP and recording injury data as barriers to participation:
Many eligible coaches did not enrol, primarily owing to lack of time or interest in collecting AE [athletic exposure] and injury data, suggesting that the programme may be more broadly and effectively disseminated if data collection is not required. [33] page 1038
The reason four teams chose not to participate was lack of practice time. All four teams had only 1 or 2 h of practice per week. [34] page 374
In other cases, the reporting listed reasons for non-participation or exclusion without specifying the use of qualitative methods. A summary of all the reported reasons for exclusion and non-participation is shown in Table 3.
3.5.2 Efficacy/Effectiveness
All trials reported a measure of the primary outcome (MDIC item 5), which in most cases was a measure of injury incidence (fuller detail in ESM Table S3). Broader outcomes (MDIC item 6) were addressed in 35 % of trials and included measures of physiological parameters, team success and negative side effects. Examples of negative side effects were delayed onset muscle soreness (DOMS) in participants performing eccentric hamstring exercises [35, 36, 45] and a fracture resulting directly from performing the IPEP [41]:
Early in the season, an athlete tripped during the program while doing a lateral hop over the ball resulting in a tibia/fibula fracture. Immediate steps were taken to ensure that all intervention teams used short cones or other flexible devices for hopping drills rather than a ball. [41] page 1481
A comparison between different sub-groups (MDIC item 7) was reported in 94 % of trials, and included comparisons between the intervention and control groups, and players with or without previous injuries. Differential attrition rates (MDIC item 8) were reported in 42 % of trials. The reasons reported for attrition included participants leaving the team or club [31, 38, 40, 47, 55], leaving the sport [38, 40, 47, 56] and lack of time or motivation [29, 31, 34]. The use of qualitative methods (MDIC item 9) was reported in 19 % of trials. This information related either to participants’ perceptions on the effectiveness of the IPEP or the reasons for attrition:
At least some of these players had a previous history of hamstring strains and believed this exercise could reduce their risk of recurrent strains. This may have reduced the incidence of hamstring strains among these teams … [53] page 45
… one of the participating teams withdrew in the middle of the season due to lack of practice time. They only practised once a week and they felt that the ankle disc training took up too much time at practice. [34] page 374
3.5.3 Adoption-Setting Level
The exclusion of settings (MDIC item 10) was reported in only one (2 %) trial [27]. Female soccer clubs were excluded if they trained less than twice per week. In the same trial, the number of settings agreeing to participate (125 of 181 clubs) was also addressed (MDIC item 11) [27]. In other trials, settings were not targeted with an intervention, but information on the involvement of settings during the recruitment of subjects was reported [6, 28, 29, 54].
3.5.4 Adoption-Delivery Agent Level
The exclusion of delivery agents (MDIC item 14) was addressed in only three (6 %) trials. One study involving the nationwide implementation of an IPEP in Switzerland [49] reported the exclusion as follows:
Coaches of the national team, the Super and Challenge League, the first and second inter-regional leagues, and of teams for players younger than 14 years of age … [49] page 59
In two other trials, no delivery agents were excluded [33, 57]. The percentage of delivery agents agreeing to participate (MDIC 15) was reported in two (4 %) trials. LaBella et al. [33] reported 95 of 258 (37 %) high school coaches agreeing to participate, while Junge et al. [49] reported 1,027 Swiss coaches from an initial sample of 1,574 (65 %) consenting to an interview, and 705 from a second sample of 1,015 coaches (69 %). A description of the characteristics of participating and non-participating delivery agents (MDIC item 16) was addressed in four (8 %) trials, and included descriptions of coach attitudes towards injury prevention [27]:
We think it is unlikely that the excluded clubs had coaches who were less ‘safety conscious’ than the coaches in the clubs that completed the study. Our experience with this and several other studies is that, at the outset, few coaches consider injuries as a factor they can influence. [27] page 6
The use of qualitative methods (MDIC item 17) was reported in five (10 %) trials and frequently highlighted barriers to delivery agent adoption:
A general problem of prevention strategies that include training modifications is to convince the coaches of the need for it. In the beginning of the present study many coaches were not convinced that the exercises suggested in the initial program may help to prevent injuries. Instead they were concerned that the exercises would steal valuable preseason training time A frequent demand was that the exercises should be combined with handball specific throwing exercises. [52] page 620
… the most common barrier to participation that coaches reported was the additional work of registering and reporting data weekly. Other less common reasons for non-participation included a reluctance to use the same warm-up programme for every training session and match and low priority for injury prevention. [27] page 5
Other studies did not specify the use of qualitative methods, but proposed potential facilitators or barriers to staff adoption. A complete listing of all reported facilitators and barriers to staff adoption is shown in Table 4.
3.5.5 Implementation
The proportion of injury-prevention sessions completed (MDIC item 18) was reported in 37 % of trials (summarised in Table 5). Authors frequently reported this item as ‘compliance’ or ‘adherence’.
Adaptations to the injury-prevention programme (MDIC item 19), including omitting certain exercises or modifying them, were reported in six (12 %) trials [32, 33, 43, 47, 51, 65]:
Some modifications were made to some of the training exercises before the second intervention season based on feedback from players and coaches after the first season. The changes aimed to make the exercises more specific to team handball, as well as more challenging. [43] page 73
A measure of the time or cost of the programme (MDIC item 20) was reported in 33 (63 %) trials, but the amount and type of detail varied considerably. In the majority of cases, this item was reported as the length of the programme in minutes (e.g. an IPEP taking 20 min to perform). Verhagen et al. [66] dedicated an entire paper to the economical evaluation of a balance board training programme. A cost analysis was also reported by LaBella et al. [33]:
To avoid 1 injury resulting in surgery, 189 athletes would need to be exposed to the warm-up, which equates to training 16 basketball coaches or 11 soccer coaches. The cost of training 16 coaches ($1280) is substantially less than the estimated treatment cost for 1 ACL [anterior cruciate ligament] injury treated surgically ($17 000–$25 000). [33] page 1038
The consistency of implementation across staff/time/settings/subgroups (MDIC item 21) was reported in 17 (33 %) trials. Frequently, reporting against this item was fulfilled by authors providing a range of the number of completed injury-prevention sessions:
The teams in the intervention group performed a mean of 91% of the 27 intended training sessions (mean 24.6; standard deviation [SD] 2.3; range 18–27 sessions) [45] page 2300
The use of qualitative methods related to implementation (MDIC item 22) was reported in 19 (37 %) trials. The most extensive qualitative information was reported by Soligard et al. [59]:
The probability of having low compliance with the injury-prevention programme was 87% higher if the coach believed that the programme was too time-consuming (OR [odds ratio] 0.13, 95% CI 0.03 to 0.60, p = 0.009). The opinion that this injury-prevention programme did not include enough football-specific activities resulted in an 81% higher probability of low compliance with the programme (OR 0.19, 95% CI 0.40 to 0.92, p = 0.038). Whether the coach had previously utilised injury-prevention training in a similar group of players did not influence the compliance with the injury-prevention programme (OR 0.60, 95% CI 0.14 to 2.47, p = 0.47). [59] page 790
Other trial reports summarised the attitudes of players towards the implemented programme:
A majority of the players (11/15) considered the extra hamstring training meaningful and were positive towards a continuation; five players would prefer whole season extra training; whereas six recommended that it be a part of the preseason schedule only [35] page 247
We were somewhat surprised by the low compliance in the study because the problem of ACL injuries has received a lot of attention from the media and within the handball community. Despite the high incidence of injury, the dire future consequences to knee function in injured players, and close follow-up of the teams by physical therapists, acceptable compliance was achieved in less than half of the players [43] page 76
In some cases, authors proposed facilitators and barriers to implementation without specifying the use of the qualitative methods used to identify them. A summary of all the reported facilitators and barriers to implementation is presented in Table 6.
3.5.6 Maintenance : Individual Level
A measure of the primary outcome at ≥6 months (MDIC item 23) was reported in a nationwide implementation of the coach-led FIFA 11 programme [49]. After 4 years, 80 % of sampled coaches were aware of the programme, and 57 % reported performing most parts of it [49]. Broader outcomes at ≥6 months (MDIC item 24) were reported for only two (4 %) trials [48, 49]:
16 of 36 teams (44%) reported that they had spontaneously continued performing components of the exercise program and 7 teams (19%) reported using the entire exercise program. The program was continued despite the fact that none of the teams had knowledge of the study results [48] page 48
3.5.7 Maintenance: Setting Level
No trial reported any items in the ‘maintenance – setting level’ dimension.
4 Discussion
This is the first systematic review focusing on the specific implementation components of team ball sport IPEP trials. The reporting of 52 IPEP trial details was assessed using the 31-item RE-AIM MDIC. The results highlight the current paucity of reported information relating to the key RE-AIM dimensions of ‘reach’, ‘efficacy/effectiveness’, ‘adoption’, ‘implementation’ and ‘maintenance’. In particular, major knowledge gaps exist relating to the adoption and maintenance of team ball sport IPEPs. Clear reporting of all aspects of programme delivery is important to enhance the ultimate impact of these interventions, and their generalisability, translatability and/or upscale to other groups and settings.
We successfully applied the RE-AIM MDIC to reviewing the reporting of team ball sport IPEPs. Key to this was our adoption of a staged process in which we first summarised the reporting of each trial according to five specific screening questions. We previously reported very low levels of reviewer consensus when this screening was not used [24], and its use in the present review led to substantially higher agreement levels. We recommend completing the screening worksheet prior to application of the full RE-AIM MDIC to guide reviewers as to which RE-AIM MDIC items are not applicable, and how the RE-AIM terminology of ‘participants’, ‘delivery agents’ and ‘settings’ applies to the reporting of individual IPEP trials. A trend towards increasing agreement across the five sequential batches of trial reports suggests a learning effect over time. This suggests that training in the use of the RE-AIM MDIC for reviewing published trial reports would be valuable. Additionally, developing detailed guidelines for the application of the RE-AIM MDIC to this team ball sport IPEP context could enhance both independent review agreement levels and the process of reaching final consensus [68].
No IPEP will achieve its full potential if it is not adopted, correctly executed and maintained by the end users (e.g. coaches and players). This is the first systematic review focusing specifically on the implementation of team ball sport IPEPs. Previous systematic reviews on team ball sport IPEPs have focused primarily on efficacy [69–71]. The results of three reviews have supported the preventive effect of IPEPs on sports injuries, while another review focusing on soccer found conflicting evidence [71]. In addition to the need for further research into the efficacy of IPEPs, attention must now be focused on enhancing the real-world impact of IPEPs through high-quality implementation. The results of several of the trials included in this review highlight the importance of adequate compliance in achieving the desired reduction in injuries [6, 27, 43, 59, 62]. A number of authors attributed high levels of compliance to the fact that the IPEP was incorporated into team training sessions [48, 50, 58, 60]; in contrast, low levels of compliance were frequently reported for IPEPs performed in addition to team training [28, 32, 42, 57]. A number of papers also reported a decrease in compliance over time [36, 41, 59, 63]. While the recent increase in attention to compliance with IPEPs is important and welcomed, researchers must also appreciate that compliance is only one of many important implementation considerations. In this regard, the RE-AIM framework, and use of the RE-AIM MDIC, is useful for outlining a full spectrum of important factors, including multiple items, relating to compliance.
The first major barrier to successfully preventing injuries with an IPEP under real-life conditions is convincing the intended users, such as coaches and players, to adopt the programme in the first place. The requirement for data collection and the time cost of the programme were the most commonly cited barriers to adoption identified in this review. Further considerations are the attitudes and beliefs of users towards injury prevention in general, and the effectiveness, degree of variation and sport specificity of individual IPEPs. Accordingly, adoption could be enhanced by investing sufficient time to fully understand the attitudes and beliefs of end users such as coaches and players, educating them about IPEPs, minimising programme length, minimising the burden of data collection and increasing programme variation. Studies in team ball sport settings have also illustrated the importance of educating coaches in the latest injury-prevention evidence [72], and how evaluating coach and player perspectives on injury-prevention programmes can inform and enhance future implementation effort [73–76].
Having convinced the targeted IPEP users (e.g. coaches, sports team staff, players) to adopt the programme, a further barrier to achieving the desired outcomes is ensuring correct performance of the IPEP. Based on the results of this review, important considerations are the length of the programme, its sport specificity, potential side effects, the support available from staff and educational material. Accordingly, more successful implementation could be facilitated by employing a relatively short, sport-specific programme supported by sufficient staffing and education, including education regarding potential side effects. When considering the extent to which IPEP users execute injury-prevention programmes as intended, it is important to acknowledge that adaptations can be necessary in order to successfully translate programmes to different groups and settings. However, the requirement for any such adaptations must be balanced against the requirement to preserve programme fidelity [77, 78]. Further research is needed to identify which specific elements of team ball sport IPEPs are critical in achieving the desired injury-prevention outcomes, and to what extent programme variation and progression is possible without negatively impacting on them.
Should the barriers to adoption and implementation be successfully overcome, there remains the challenge of facilitating sufficient maintenance of the IPEP for longer-term prevention gains. As the individual RE-AIM MDIC items in the dimension of ‘maintenance’ were reported in fewer than 1 % of the 52 trials, no reasonable conclusions on how to enhance the maintenance of team ball sport IPEPs can be formed at this stage. This is a major gap that needs addressing for long-term prevention goals that rely on sustained behaviour change.
While this review clearly demonstrates the lack of reporting on a range of specific implementation components in team ball sport IPEP trials across all RE-AIM dimensions, the paucity of information relating to the dimensions of ‘adoption’ and ‘maintenance’ is particularly concerning. The number of trials for which individual RE-AIM MDIC items in these two dimensions were reported ranged from just 0 to 10 %. In addition to the lack of reported information on delivery agent adoption, it is worrying that in 44 % of trials it was unclear whether or not delivery agents were involved at all. To address this gap and facilitate the translation of IPEPs to other groups and settings, authors must provide detailed information on the selection, participation, characteristics and actual behaviour of the delivery agents.
The paucity of reported information on adoption by settings is also a concern, because the adoption of IPEPs by settings such as sports clubs and schools is seen to be an important step in enhancing the wide-scale impact of these programmes. Successfully engaging settings could enhance both the adoption and maintenance of team ball sport IPEPs, particularly if they are incorporated into policy. Only one of the 52 trials fulfilled any component in the dimension ‘adoption – setting level’. This may have resulted, in part, from our definition of setting involvement. In some cases, information about the involvement of settings during the recruitment of subjects was reported, but the settings were not identified as a target of the research intervention [6, 28, 29, 54]. However, even when the reporting in these trials is included, there remains a distinct lack of reported information on settings.
Certain RE-AIM MDIC items within the dimensions of ‘efficacy/effectiveness’ and ‘reach’ were reported in a relatively high proportion of trials. In particular, more recently published trial reports frequently addressed RE-AIM items in these two dimensions. This could be a reflection of the recent increased use of the CONSORT (Consolidated Standards of Reporting Trials) statement [79, 80], which requires the reporting of some similar elements (e.g. eligibility criteria, group comparisons and attrition rates).
Finally, the results of this review clearly illustrate the scarcity of reported information on specific implementation components in team ball sport IPEPs. Considering the critical role of these factors in enhancing the ultimate impact of team ball sport IPEPs, the lack of evidence in this area is a concern. Future reporting must clearly identify specific implementation components in order to enhance the development of IPEPs, and efforts to translate them into other groups and settings.
4.1 Limitations
The eligibility criteria and search strategy employed in this review may have excluded potentially relevant papers, such as trial reports published in other languages. Reports of other trials, or additional reporting of included trials, may have been published since the completion of the search strategy. The reporting of eligible trials was only assessed against the RE-AIM MDIC, which does not cover all methodological aspects of intervention trials, especially issues related to internal validity. It is possible that some authors collected information relevant to RE-AIM MDIC items, but did not report this information due to the restrictions set by publishers. The screening questions used in this review have not been formally tested for reliability and validity, but they have been previously published. The use of more than two independent reviewers may have strengthened the methodology of this review.
5 Conclusion
Information on specific implementation components in the reporting of team ball sport IPEP trials is scarce. In particular, major knowledge gaps exist regarding the adoption and maintenance of these programmes. This is a problem because the successful adoption and maintenance of any injury-prevention programme are key factors in achieving the desired outcome. To enhance the ultimate impact of team ball sport IPEPs, the future reporting of IPEP trials must clearly address all aspects of programme delivery, as outlined by the RE-AIM framework. The RE-AIM MDIC can be successfully applied to reviewing literature in this context.
References
Fédération Internationale de Football Association (FIFA). Big count. http://www.fifa.com/worldfootball/bigcount/. Accessed 12 Oct 2013.
EuroSafe. Injuries in the European Union: summary of injury statistics for the years 2008–2010. http://ec.europa.eu/health/data_collection/docs/idb_report_2013_en.pdf. Accessed 10 Dec 2013.
Lohmander LS, Ostenberg A, Englund M, et al. High prevalence of knee osteoarthritis, pain, and functional limitations in female soccer players twelve years after anterior cruciate ligament injury. Arthritis Rheum. 2004;50(10):3145–52.
von Porat A, Roos EM, Roos H. High prevalence of osteoarthritis 14 years after an anterior cruciate ligament tear in male soccer players: a study of radiographic and patient relevant outcomes. Ann Rheum Dis. 2004;63(3):269–73.
Kuijt MT, Inklaar H, Gouttebarge V, et al. Knee and ankle osteoarthritis in former elite soccer players: a systematic review of the recent literature. J Sci Med Sport. 2012;15(6):480–7.
Walden M, Atroshi I, Magnusson H, et al. Prevention of acute knee injuries in adolescent female football players: cluster randomised controlled trial. BMJ. 2012;344:e3042.
Steffen K, Emery CA, Romiti M, et al. High adherence to a neuromuscular injury prevention programme (FIFA 11+) improves functional balance and reduces injury risk in Canadian youth female football players: a cluster randomised trial. Br J Sports Med. 2013;47(12):794–802.
Myklebust G, Skjolberg A, Bahr R. ACL injury incidence in female handball 10 years after the Norwegian ACL prevention study: important lessons learned. Br J Sports Med. 2013;47(8):476–9.
Finch CF. Implementing studies into real life. In: Verhagen E, van Mechelen W, editors. Sports injury research. Oxford: Oxford University Press; 2010. p. 213–35.
Finch C. A new framework for research leading to sports injury prevention. J Sci Med Sport. 2006;9(1–2):3–9.
Donaldson A, Finch CF. Applying implementation science to sports injury prevention. Br J Sports Med. 2013;47(8):473–5.
Finch CF. Implementation and dissemination research: the time has come! Br J Sports Med. 2011;45(10):763–4.
Hanson D, Allegrante JP, Sleet DA, et al. Research alone is not sufficient to prevent sports injury. Br J Sports Med. 2014;48(8):682–4.
Finch CF. Implementing and evaluating interventions. In: Baker S, Li G, editors. Injury research: theories, methods, and approaches. New York: Springer; 2012. p. 619–39.
Finch CF, Donaldson A. A sports setting matrix for understanding the implementation context for community sport. Br J Sports Med. 2010;44(13):973–8.
Gaglio B, Shoup JA, Glasgow RE. The RE-AIM framework: a systematic review of use over time. Am J Public Health. 2013;103(6):e38–46.
Virginia Polytechnic Institute and State University. What is RE-AIM? http://www.re-aim.org. Accessed 21 Aug 2013.
Fogarty International Center. Frequently asked questions about implementation science. http://www.fic.nih.gov/News/Events/implementation-science/Pages/faqs.aspx. Accessed 20 Aug 2013.
White SM, McAuley E, Estabrooks PA, et al. Translating physical activity interventions for breast cancer survivors into practice: an evaluation of randomized controlled trials. Ann Behav Med. 2009;37(1):10–9.
Allen K, Zoellner J, Motley M, et al. Understanding the internal and external validity of health literacy interventions: a systematic literature review using the RE-AIM framework. J Health Commun. 2011;16(Suppl 3):55–72.
Akers JD, Estabrooks PA, Davy BM. Translational research: bridging the gap between long-term weight loss maintenance research and practice. J Am Diet Assoc. 2010;110(10):1511–22, 22.e1-3.
Kessler RS, Purcell EP, Glasgow RE, et al. What does it mean to “employ” the RE-AIM model. Eval Health Prof. 2013;36(1):44–66.
O’Brien J, Finch CF. A systematic review of core implementation components in team ball sport injury prevention trials. Inj Prev. Published Online First 4 April 2014. doi:10.1136/injuryprev-2013-041087.
O’Brien J, Donaldson A, Barbery G, et al. The three must-do’s of intervention reporting: enhancing sports injury prevention research. Br J Sports Med. Published Online First 3 Sept 2013. doi:10.1136/bjsports-2013-092913.
Hides JA, Stanton WR, Mendis MD, et al. Effect of motor control training on muscle size and football games missed from injury. Med Sci Sports Exerc. 2012;44(6):1141–9.
Scase E, Cook J, Makdissi M, et al. Teaching landing skills in elite junior Australian football: evaluation of an injury prevention strategy. Br J Sports Med. 2006;40(10):834–8.
Soligard T, Myklebust G, Steffen K, et al. Comprehensive warm-up programme to prevent injuries in young female footballers: cluster randomised controlled trial. BMJ. 2008;337:a2469.
Emery CA, Rose MS, McAllister JR, et al. A prevention strategy to reduce the incidence of injury in high school basketball: a cluster randomized controlled trial. Clin J Sport Med. 2007;17(1):17–24.
Holmich P, Larsen K, Krogsgaard K, et al. Exercise program for prevention of groin pain in football players: a cluster-randomized trial. Scand J Med Sci Sports. 2010;20(6):814–21.
Bahr R, Lian O, Bahr IA. A twofold reduction in the incidence of acute ankle sprains in volleyball after the introduction of an injury prevention program: a prospective cohort study. Scand J Med Sci Sports. 1997;7(3):172–7.
Verhagen E, van der Beek A, Twisk J, et al. The effect of a proprioceptive balance board training program for the prevention of ankle sprains: a prospective controlled trial. Am J Sports Med. 2004;32(6):1385–93.
Engebretsen AH, Myklebust G, Holme I, et al. Prevention of injuries among male soccer players: a prospective, randomized intervention study targeting players with previous injuries or reduced function. Am J Sports Med. 2008;36(6):1052–60.
LaBella CR, Huxford MR, Grissom J, et al. Effect of neuromuscular warm-up on injuries in female soccer and basketball athletes in urban public high schools: cluster randomized controlled trial. Arch Pediatr Adolesc Med. 2011;165(11):1033–40.
Wedderkopp N, Kaltoft M, Holm R, et al. Comparison of two intervention programmes in young female players in European handball-with and without ankle disc. Scand J Med Sci Sports. 2003;13(6):371–5.
Askling C, Karlsson J, Thorstensson A. Hamstring injury occurrence in elite soccer players after preseason strength training with eccentric overload. Scand J Med Sci Sports. 2003;13(4):244–50.
Gabbe BJ, Branson R, Bennell KL. A pilot randomised controlled trial of eccentric exercise to prevent hamstring injuries in community-level Australian Football. J Sci Med Sport. 2006;9(1–2):103–9.
Mohammadi F. Comparison of 3 preventive methods to reduce the recurrence of ankle inversion sprains in male soccer players. Am J Sports Med. 2007;35(6):922–6.
Cumps E, Verhagen EA, Duerinck S, et al. Effect of a preventive intervention programme on the prevalence of anterior knee pain in volleyball players. Eur J Sports Sci. 2008;8(4):183–92.
Eils E, Schroter R, Schroder M, et al. Multistation proprioceptive exercise program prevents ankle injuries in basketball. Med Sci Sports Exerc. 2010;42(11):2098–105.
van Beijsterveldt AM, van de Port IG, Krist MR, et al. Effectiveness of an injury prevention programme for adult male amateur soccer players: a cluster-randomised controlled trial. Br J Sports Med. 2012;46(16):1114–8.
Gilchrist J, Mandelbaum BR, Melancon H, et al. A randomized controlled trial to prevent noncontact anterior cruciate ligament injury in female collegiate soccer players. Am J Sports Med. 2008;36(8):1476–83.
Emery CA, Meeuwisse WH. The effectiveness of a neuromuscular prevention strategy to reduce injuries in youth soccer: a cluster-randomised controlled trial. Br J Sports Med. 2010;44(8):555–62.
Myklebust G, Engebretsen L, Braekken IH, et al. Prevention of anterior cruciate ligament injuries in female team handball players: a prospective intervention study over three seasons. Clin J Sport Med. 2003;13(2):71–8.
Cahill BR, Griffith EH. Effect of preseason conditioning on the incidence and severity of high school football knee injuries. Am J Sports Med. 1978;6(4):180–4.
Petersen J, Thorborg K, Nielsen MB, et al. Preventive effect of eccentric training on acute hamstring injuries in men’s soccer: a cluster-randomized controlled trial. Am J Sports Med. 2011;39(11):2296–303.
Hagglund M, Walden M, Atroshi I. Preventing knee injuries in adolescent female football players-design of a cluster randomized controlled trial. BMC Musculoskelet Disord. 2009;10:75.
Junge A, Rosch D, Peterson L, et al. Prevention of soccer injuries: a prospective intervention study in youth amateur players. Am J Sports Med. 2002;30(5):652–9.
Kiani A, Hellquist E, Ahlqvist K, et al. Prevention of soccer-related knee injuries in teenaged girls. Arch Intern Med. 2010;170(1):43–9.
Junge A, Lamprecht M, Stamm H, et al. Countrywide campaign to prevent soccer injuries in Swiss amateur players. Am J Sports Med. 2011;39(1):57–63.
Longo UG, Loppini M, Berton A, et al. The FIFA 11+ program is effective in preventing injuries in elite male basketball players: a cluster randomized controlled trial. Am J Sports Med. 2012;40(5):996–1005.
Hagglund M, Walden M, Ekstrand J. Lower reinjury rate with a coach-controlled rehabilitation program in amateur male soccer: a randomized controlled trial. Am J Sports Med. 2007;35(9):1433–42.
Petersen W, Braun C, Bock W, et al. A controlled prospective case control study of a prevention training program in female team handball players: the German experience. Arch Orthop Trauma Surg. 2005;125(9):614–21.
Arnason A, Andersen TE, Holme I, et al. Prevention of hamstring strains in elite soccer: an intervention study. Scand J Med Sci Sports. 2008;18(1):40–8.
Pfeiffer RP, Shea KG, Roberts D, et al. Lack of effect of a knee ligament injury prevention program on the incidence of noncontact anterior cruciate ligament injury. J Bone Jt Surg Am. 2006;88(8):1769–74.
Cumps E, Verhagen E, Meeusen R. Efficacy of a sports specific balance training programme on the incidence of ankle sprains in basketball. J Sports Sci Med. 2007;6(2):212–9.
Soderman K, Werner S, Pietila T, et al. Balance board training: prevention of traumatic injuries of the lower extremities in female soccer players? A prospective randomized intervention study. Knee Surg Sports Traumatol Arthrosc. 2000;8(6):356–63.
Fredberg U, Bolvig L, Andersen NT. Prophylactic training in asymptomatic soccer players with ultrasonographic abnormalities in Achilles and patellar tendons: the Danish Super League Study. Am J Sports Med. 2008;36(3):451–60.
Gatterer H, Ruedl G, Faulhaber M, et al. Effects of the performance level and the FIFA “11” injury prevention program on the injury rate in Italian male amateur soccer players. J Sports Med Phys Fit. 2012;52(1):80–4.
Soligard T, Nilstad A, Steffen K, et al. Compliance with a comprehensive warm-up programme to prevent injuries in youth football. Br J Sports Med. 2010;44(11):787–93.
Kraemer R, Knobloch K. A soccer-specific balance training program for hamstring muscle and patellar and achilles tendon injuries: an intervention study in premier league female soccer. Am J Sports Med. 2009;37(7):1384–93.
McHugh MP, Tyler TF, Mirabella MR, et al. The effectiveness of a balance training intervention in reducing the incidence of noncontact ankle sprains in high school football players. Am J Sports Med. 2007;35(8):1289–94.
Pasanen K, Parkkari J, Pasanen M, et al. Neuromuscular training and the risk of leg injuries in female floorball players: cluster randomised controlled study. Br J Sports Med. 2008;42(10):502–5.
Steffen K, Myklebust G, Olsen OE, et al. Preventing injuries in female youth football-a cluster-randomized controlled trial. Scand J Med Sci Sports. 2008;18(5):605–14.
Olsen OE, Myklebust G, Engebretsen L, et al. Exercises to prevent lower limb injuries in youth sports: cluster randomised controlled trial. BMJ. 2005;330(7489):449.
Verrall GM, Slavotinek JP, Barnes PG. The effect of sports specific training on reducing the incidence of hamstring injuries in professional Australian Rules football players. Br J Sports Med. 2005;39(6):363–8.
Verhagen EA, van Tulder M, van der Beek AJ, et al. An economic evaluation of a proprioceptive balance board training programme for the prevention of ankle sprains in volleyball. Br J Sports Med. 2005;39(2):111–5.
Bixler B, Jones RL. High-school football injuries: effects of a post-halftime warm-up and stretching routine. Fam Pract Res J. 1992;12(2):131–9.
Lauersen JB, Bertelsen DM, Andersen LB. The effectiveness of exercise interventions to prevent sports injuries: a systematic review and meta-analysis of randomised controlled trials. Br J Sports Med. 2014;48(11):871-7.
Herman K, Barton C, Malliaras P, et al. The effectiveness of neuromuscular warm-up strategies, that require no additional equipment, for preventing lower limb injuries during sports participation: a systematic review. BMC Med. 2012;10(75):1–12.
Hubscher M, Zech A, Pfeifer K, et al. Neuromuscular training for sports injury prevention: a systematic review. Med Sci Sports Exerc. 2010;42(3):413–21.
van Beijsterveldt AM, van der Horst N, van de Port IG, et al. How effective are exercise-based injury prevention programmes for soccer players? A systematic review. Sports Med. 2013;43(4):257–65.
Twomey D, Finch C, Roediger E, et al. Preventing lower limb injuries: is the latest evidence being translated into the football field? J Sci Med Sport. 2009;12(4):452–6.
White PE, Ullah S, Donaldson A, et al. Encouraging junior community netball players to learn correct safe landing technique. J Sci Med Sport. 2012;15(1):19–24.
Saunders N, Otago L, Romiti M, et al. Coaches’ perspectives on implementing an evidence-informed injury prevention programme in junior community netball. Br J Sports Med. 2010;44(15):1128–32.
Finch CF, Doyle TL, Dempsey AR, et al. What do community football players think about different exercise-training programmes? Implications for the delivery of lower limb injury prevention programmes. Br J Sports Med. 2014;48(8):702-7.
White PE, Otago L, Saunders N, et al. Ensuring implementation success: how should coach injury prevention education be improved if we want coaches to deliver safety programmes during training sessions? Br J Sports Med. 2014;48(5):402–3.
Fixsen DL, Naoom SF, Blase KA, et al. Implementation research: a synthesis of the literature. The National Implementation Research Network (FMHI Publication #231): Tampa: University of South Florida, Louis de la Parte; 2005.
Durlak J. The Importance of quality implementation for research, practice, and policy. http://aspe.hhs.gov/hsp/13/KeyIssuesforChildrenYouth/ImportanceofQuality/rb_QualityImp.pdf. Accessed 01 Jan 2013.
Campbell MK, Piaggio G, Elbourne DR, et al. Consort 2010 statement: extension to cluster randomised trials. BMJ. 2012;345:e5661.
Schulz KF, Altman DG, Moher D, et al. CONSORT 2010 statement: updated guidelines for reporting parallel group randomized trials. Open Med. 2010;4(1):e60–8.
Acknowledgments
JO’B was supported by a University of Ballarat Postgraduate Scholarship. CFF was supported by a National Health and Medical Research Council (NHMRC) Principal Research Fellowship (ID:565900 and APP1058737). This work was led by JO’B as part of his PhD studies, supervised by CFF. The Australian Centre for Research into Injury in Sport and its Prevention (ACRISP) is one of the International Research Centres for Prevention of Injury and Protection of Athlete Health supported by the International Olympic Committee (IOC). The authors have no conflicts of interest that are directly relevant to the content of this review. JO’B designed the study, led its conduct, performed the systematic search and had the major role in paper writing. CFF independently reviewed the eligible full-text papers, participated in the consensus discussions and contributed to the writing of the paper.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
O’Brien, J., Finch, C.F. The Implementation of Musculoskeletal Injury-Prevention Exercise Programmes in Team Ball Sports: A Systematic Review Employing the RE-AIM Framework. Sports Med 44, 1305–1318 (2014). https://doi.org/10.1007/s40279-014-0208-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40279-014-0208-4