
Abstract
Background
Rugby Union has one of the highest reported incidences of match injuries amongst all professional team sports. The majority of research within this field has focused on elite male cohorts; in this study we present the first meta-analytic review of these data.
Objective
The aim of this study was to summarise the incidence and severity of injuries in senior men’s professional Rugby Union, and determine the overall effects of level of play, new versus recurrent injuries, playing position, type of injuries, location of injuries, severity of injuries, period of match, and injury incident.
Methods
Electronic databases were searched using keywords ‘Rugby Union’ and ‘inj*’. Fifteen papers addressing injuries in senior men’s professional Rugby Union (from 1995 through September 2012) were included in the review. A maximum of ten of these papers provided incidence data that could be modelled via a Poisson mixed-effects generalised linear model, while up to nine studies provided severity data that could be modelled via a general linear mixed model. Magnitude based inferences were used to assess differences between factors. A descriptive analysis was provided for studies that could not be included in the pooled analysis due to incongruent injury definitions.
Results
The overall incidence of injuries in senior men’s professional Rugby Union matches was 81 per 1,000 player hours (95 % CI 63–105), and 3 per 1,000 player hours (95 % CI 2–4) during training. Estimated mean severity for match injuries was 20 days (95 % CI 14–27), and 22 days (95 % CI 19–24) for training injuries. A higher level of play was associated with a greater incidence of injuries in matches, with no clear difference in severity. New injuries occurred substantially more often than recurrent injuries, while the severity of recurrent injuries was, on average, 10 days (95 % CI 4–17) greater than new injuries. Trivial differences were found in injury incidence and severity between forwards and backs. Muscle/tendon and joint (non-bone)/ligament injuries were the two most prevalent injury groups, whereas fractures and bone stress injuries had the highest average severity. The lower limb was the body region with the highest injury incidence, while upper limb injuries were most severe. The third quarter (40–60 min) of matches had the highest injury rate, and injuries most commonly occurred as a result of being tackled.
Conclusions
This meta-analysis confirms match injury incidence rates in professional Rugby Union can be considered high in comparison with other team sports, but similar to other collision sports. In order to markedly reduce overall injury burden, efforts should target lower-limb injury prevention strategies and technique during contact, as these may render the largest effect.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
Rugby Union is now amongst the most played and watched sports in the world, with approximately 5 million registered players in over 117 countries, and a 19 % annual increase in player numbers since 2007 [1]. The game is physically demanding, with frequent bouts of high intensity activity such as running, sprinting, rucking, mauling and tackling, interspersed by periods of low intensity work, such as walking and jogging [2]. A range of physical attributes are necessary for elite Rugby Union players, including strength, power, speed, agility and endurance [3]. The combination of high physical demands, alongside exposure to collisions and contacts, means the inherent risk of injury whilst playing Rugby Union is substantial. Indeed, Rugby Union has one of the highest reported incidences of match injury amongst all professional team sports [4], although rates are comparable with other full-contact sports such as ice hockey [5], Rugby League [6], American Football [7] and Australian Rules Football [8]. There have been a number of prospective cohort studies investigating the injuries sustained in senior men’s professional Rugby Union since professionalism was introduced in 1995, and the publication of a consensus statement on injury definitions and data collection procedures in 2007 has improved the consistency and quality of research within the field [9]. To enhance the information provided by such epidemiological data, information from several studies may be combined to give more precise effect estimates and increased statistical power [10, 11]. Full understanding of the incidence and aetiology of injuries in professional Rugby Union are the initial steps in the injury prevention model [12]. To that end, a meta-analytic review of senior men’s professional Rugby Union injuries was undertaken to collate and summarise the injury data to date, and identify risk factors for injury.
1.1 Objective
The aim of this study was to review and collate the epidemiological data of injuries in senior men’s professional Rugby Union as reported in the literature, and to make magnitude-based inferences regarding level of play, new versus recurrent injuries, playing position, period of match, type of injuries, location of injuries, severity of injuries, and injury incident.
2 Methods
Guidelines for reporting meta-analysis of observational studies in epidemiology (MOOSE guidelines) [13] were followed. The checklist contains specifications for reporting of meta-analyses of observational studies in epidemiology, including background, search strategy, methods, results, discussion and conclusion.
2.1 Literature Search
Web of Knowledge, SportsDiscus, PubMed and Google Scholar databases were searched from 1995 through September 2012 using keywords ‘Rugby Union’ and ‘inj*’. Furthermore, the reference lists of included studies, and relevant ‘grey literature’ (e.g. conference proceedings) were searched to identify additional articles. Inclusion criteria for retrieved studies were set at (i) prospective cohort studies; (ii) study population comprising of 15-a-side senior male professional Rugby Union teams; (iii) studies must give a clear definition of what constituted a reportable injury; and (iv) studies must report one or more of the following epidemiological data: (a) injury incidence rates for match or training injuries; (b) incidence of new and recurrent injuries; (c) incidence of injuries in forwards and backs; (d) period of match incidence; (e) type of injuries; (f) location of injuries; (g) severity of injuries; or (h) injury incident. Duplicate records were identified and removed. Titles and abstracts of the remaining studies were assessed for relevance, with non-relevant articles being discarded. Full-text versions of the outstanding articles were then retrieved and evaluated against the inclusion criteria by two independent reviewers.
2.2 Assessment of Study Quality
Two reviewers independently assessed the reporting quality of included studies using the ‘Strengthening the Reporting of Observational Studies in Epidemiology’ (STROBE) statement [14]. This 22-item checklist provides guidance on the reporting of observational studies in order to facilitate critical appraisal and interpretation of results. As per Olmos et al. [15], studies were categorised as either poor, moderate or good based on the percentage of fulfilled items from the STROBE checklist, with cut-off values of <50, 50–80, and >80 % respectively.
2.3 Data Extraction
For studies meeting the inclusion criteria, general information pertaining to the level of play, number of participants involved, length of follow-up, and injury definition used within each study was extracted and compiled into a spreadsheet (see Table 1). The aim of the present meta-analysis was to determine the overall effects of (i) level of play (international vs. level one clubs vs. level two clubs); (ii) new versus recurrent injuries; (iii) playing position (forwards vs. backs); (iv) period of match; (v) type of injuries; (vi) location of injuries; (vii) severity of injuries; and (viii) injury incident. Thus, multiple rows of data were included for each study to allow for the various combinations of counts and exposures required for each fixed effect. Additionally, a descriptive analysis was provided to describe trends in injury risk over time. Note, shoulder injuries are recorded as ‘upper limb’ injuries within the literature.
The International Rugby Board (IRB) organises its member unions into six tiers according to playing strength and potential [16]; tier one teams participate in the Six Nations Championship (England, France, Ireland, Italy, Scotland, Wales) or the Rugby Championship (Argentina, Australia, New Zealand, South Africa) while tier two currently consists of Canada, Fiji, Japan, Romania, Samoa, Tonga and the US. For ‘level of play’, teams were considered to be ‘level one’ if they played in the highest league within a tier one-ranked nation, and ‘level two’ if they played below the top league within a tier one-ranked nation, or in the highest league within a tier two-ranked nation. Where required, authors were contacted to obtain any additional data that was not available in the full-text versions.
2.4 Analysis and Interpretation of Results
Only studies utilising a ‘time-loss’ injury definition, as outlined by Fuller et al. [9], were included in the pooled meta-analysis. A descriptive analysis was provided for studies that could not be included because of incongruent injury definitions. Incidence rate data were modelled using a generalised linear mixed model, with a Poisson distribution and loglinear link function, as previously described [17]. The response variable was the number of observed injuries, offset by the log of the number of exposure hours. Severity data were modelled using a general linear mixed model. A random effects term was included to account for the correlation arising from using multiple rows of data from the same study. Factors of interest were included as fixed effects. The weighting factor used was: (study exposure time [h])/mean study exposure time [h]). Statistical modelling was performed using IBM SPSS Statistics for Windows, Version 20.0 (IBM Corporation, Armonk, NY, USA).
For injury incidence data, the overall estimated means for each fixed-effect factor were obtained from the model and then back-transformed to give incidence rates, along with 95 % confidence intervals (CIs). Comparisons between factors were then made using a spreadsheet for combining effect statistics [18], whereby the incidence rate ratio (and its associated confidence limits) was assessed against pre-determined thresholds. An incidence rate ratio of 0.91 represented a substantially lower injury risk, while an incidence rate ratio of 1.10 indicated a substantially higher injury risk [19]. For injury severity data, a spreadsheet for deriving a confidence interval and clinical inference from a p-value was used [20]. The smallest practically important effect was a mean difference of 4 days, which was agreed upon by the authors as being likely to impact on team selection. An effect was deemed unclear if its confidence interval overlapped the thresholds for substantiveness; that is, if the effect could be substantial in both a positive and negative sense. Otherwise the effect was clear and deemed to have the magnitude of the largest observed likelihood value. This was qualified with a probabilistic term using the following scale [21]: <0.5 %, most unlikely; 0.5–5 %, very unlikely; 5–25 %, unlikely; 25–75 %, possible; 75–95 %, likely; 95–99.5 %, very likely; >99.5 %, most likely [20].
3 Results
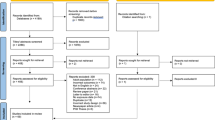
See Fig. 1 for a summary of the study collection process. The electronic searches returned 355 results. After removing duplicate and non-relevant records, 52 potentially relevant studies were assessed for inclusion in this review, based on the criteria outlined above. Fifteen prospective cohort studies were included, with a methodological quality ranging from poor to good. Older studies tended to have poorer methodological quality than more recent studies (see Table 1).

Summary of the study collection process
3.1 Level of Play
Ten studies [22–31] provided an overall injury incidence for either match or training injuries that could be combined in the meta-analysis. The ten studies encompassed a total of 8,929 injuries amongst senior male professional Rugby Union players exposed to 656,990 h of match or training time. The overall incidence of injuries in senior men’s professional rugby matches was 81 per 1,000 player hours (95 % CI 63–105) and 3 per 1,000 player hours (95 % CI 2–4) during training. See Fig. 2 for a summary of the reported match injury incidences of the analysed studies. For level of play, the mean incidence rates per 1,000 player hours with 95 % CI were, in descending order: international match: 123 (85–177); level one club match: 89 (75–104); level two club match: 35 (27–45); international training: 3 (2–4); and level one club training: 3 (2–4). The incidence rate during international matches was likely higher (87 % likelihood) than during level one club matches, and most likely higher (100 % likelihood) than level two club matches. Level one club match injury incidence was also most likely higher (100 % likelihood) than level two club matches. There was no clear difference in incidence rates between international and level one club training injuries. The five studies [32–36] that could not be included in the meta-analysis reported highly variable incidence rates (32–120 per 1,000 player hours) but, in general, incidence rates tended to increase with level of play.

Incidence of match injuries (with 95 % confidence intervals) by playing level
Nine studies [22–28, 30, 31] provided match injury severity data that could be included in the meta-analysis. The mean severities with 95 % CIs for each playing level were, in descending order: level two club: 23 days (11–34); level one club: 21 days (19–23); and international: 20 days (11–28). Differences between levels were unclear.
3.2 New Versus Recurrent Injuries
Seven studies [22–24, 26, 28–30] were included in an analysis comparing the incidence of new versus recurrent injuries. The incidence of new injuries (78 per 1,000 player hours, 95 % CI 74–83) was most likely higher (100 % likelihood) than that of recurrent injuries (11 per 1,000 player hours, 95 % CI 10–12). Two studies [32, 34], which could not be included in the pooled analysis but reported data for new and recurrent injuries, reported similar incidence rate ratios for new versus recurrent injuries (~7.0–9.0).
Four studies [22–24, 30] provided new and recurrent injury severity data that could be included in the general linear mixed model. Recurrent injuries (30 days, 95 % CI 26–35) were very likely (98 % likelihood) more severe than new injuries (20 days, 95 % CI 15–24).
3.3 Playing Position
Six studies [22–24, 26–28] that reported match injury incidences for both forwards and backs were combined in the pooled analysis. There was a 76 % likelihood that the difference in the incidence of injuries between forwards (94 per 1,000 player hours, 95 % CI 84–101) and backs (99 per 1,000 player hours, 95 % CI 92–106) was trivial. Two studies [32, 33] that could not be included in the pooled analysis due to disparate injury definitions reported trends towards higher injury incidence in forwards compared with backs. These studies included injuries that required the player to leave the field of play (e.g. minor skin and laceration injuries); this may account for the observed trend towards a higher injury incidence in forwards compared with backs.
Five studies [22–26] also provided severity data for these grouped playing positions that could be included in the general linear mixed model. There was a likely trivial (80 % likelihood) difference in average injury severity between forwards (23 days, 95 % CI 20–26) and backs (21 days, 95 % CI 18–26).
3.4 Type of Injuries
An analysis was undertaken to determine the most frequent type of match injury sustained (see Fig. 3). Seven studies [22–28] were included in the pooled analysis. Muscle/tendon (40 per 1,000 player hours, 95 % CI 21–76) and joint (non-bone)/ligament injuries (34 per 1,000 player hours, 95 % CI 18–65) were the most common time-loss injury types (with no clear difference between them), followed by central/peripheral nervous system injuries (8 per 1,000 player hours, 95 % CI 4–15), fractures and bone stresses (4 per 1,000 player hours, 95 % CI 2–8), unclassified/other (2 per 1,000 player hours, 95 % CI 1–4), and laceration and skin injuries (1 per 1,000 player hours, 95 % CI 1–3). Three studies [32, 33, 35] that could not be included in the meta-analysis reported incidence rates similar to those in our pooled analysis above, although a higher proportion of laceration and skin injuries (23–27 %) were found (likely due to the fact that the injury definition used in these studies included injuries that forced a player to leave the field during a match). Note, muscle/tendon and joint (non-bone)/ligament injuries have previously been referred to in extant literature as ‘strains’ and ‘sprains’, respectively.

Injury incidence (with 95 % confidence intervals) by injury type
Four studies [23, 24, 26, 28] also provided severity data for injury types that could be included in the general linear mixed model. Analysis showed that fractures and bone stress injuries (42 days, 95 % CI 32–51) were most severe, with comparisons to all other injury types being clear. The mean severities with 95 % CIs of the remaining injury types were, in descending order: joint and ligament: 29 days (19–39); central/peripheral nervous system: 25 days (16–35); muscle and tendon: 15 days (5–24); other: 12 (2–22), and laceration and skin: 6 days (1–15). Comparisons between these injury types were all clinically clear, with the exception of ‘joint and ligament versus central/peripheral nervous system’, ‘muscle and tendon versus other’ and ‘other versus laceration and skin’, for which inferences were unclear.
3.5 Location of Injuries
Seven studies [22–28] reporting the location of match injuries were pooled in the meta-analysis. Lower-limb injuries occurred more often than injuries to other body regions [incidence rate most likely higher (>99.5 % likelihood) for all comparisons]. Differences between the remaining body regions were unclear (see Fig. 4). The mean incidence rates per 1,000 player hours with 95 % CIs of each body region were, in descending order: lower limb, 47 (26–84); upper limb, 14 (8–25); head, 13 (7–23); and trunk, 9 (5–16). The five studies [32–36] that could not be included in the pooled analysis also found the lower limb to be the most frequently injured body region.

Injury incidence (with 95 % confidence intervals) by location of injury
Five studies [22–26] also provided severity data for injury locations that could be included in the general linear mixed model. Analysis showed that upper limb injuries (32 days, 95 % CI 26–38) were most severe, with comparisons to all other body regions being clear. The mean severities with 95 % CIs of the remaining body regions were, in descending order: lower limb, 19 days (13–26); trunk, 16 days (9–22); and head/neck, 12 days (6–18). There was a 76 % likelihood that the lower-limb injuries were more severe than head/neck injuries, but the remaining comparisons were unclear.
3.6 Severity of Injuries
An analysis was undertaken to determine the most frequent severity of injury sustained in senior men’s professional Rugby Union matches. Injuries were graded based on time lost from competition and training: minimal (2–3 days), mild (4–7 days), moderate (8–28 days) and severe (>28 days). Five studies [25–28, 30] reporting data on the incidence of each level of severity were pooled in the meta-analysis. The most common injury severity was ‘moderate’ (28 per 1,000 player hours, 95 % CI 25–31), followed by ‘mild’ (23 per 1,000 player hours, 95 % CI 20–26), minimal (17 per 1,000 player hours, 95 % CI 15–19) and ‘severe’ (15 per 1,000 player hours, 95 % CI 13–17). Comparisons between each severity level were all clear. Three studies that could not be included in the pooled analysis [32, 33, 36] classified injuries as mild (one game missed), moderate (two to three games missed) or severe (more than three games missed). Mild injuries were consistently the most common severity (64–70 %), with similar incidences of moderate and severe injuries (14–22 %). Holtzhausen et al. [34] graded injuries according to the number of sessions missed: minor (1–3 missed), intermediate (4–9 missed) and severe (>9 missed). Minor injuries accounted for 39 % of all injuries, 27 % were of intermediate severity and 34 % were severe injuries.
Nine studies [22–28, 30, 31] reported severity data that could be included in the general linear mixed model. Estimated mean severity for match injuries was 20 days (95 % CI 14–27), and 22 days (95 % CI 19–24) for training injuries; differences between these factors were possibly trivial (70 % likelihood). One catastrophic injury (cervical ligament injury) was reported in the reviewed studies [35].
3.7 Period of Match
Four studies [23, 26, 28, 30] reported injury incidences for each match period that could be combined in the pooled analysis (see Fig. 5). The mean incidence rates per 1,000 player hours with 95 % CIs of each match period were, in descending order: 40–60 min, 119 (108–127); 20–40+ min, 112 (103–121); 60–80+ min, 108 (100–117); and 0–20 min, 57 (51–62). There was a >99.5 % likelihood that the incidence rate in the first quarter was most likely lower than the three other match periods. Injuries occurred more often in the third quarter of matches (40–60 min) than other match periods, although the incidence rate was only possibly greater than the second (20–40+ min) and final (60–80+ min) quarters, with likelihoods of 28 and 52 %, respectively. There was an 83 % likelihood that the difference between the incidence rate in the second and final quarters was trivial. Three studies [32–34] that could not be included in the pooled analysis, but provided period of match incidence data, also reported a substantially lower incidence rate in the first quarter compared with the three other match periods, and the highest incidence of injury in the third quarter.

Injury incidence (with 95 % confidence intervals) by period of match
3.8 Injury Incident
Five studies [22, 23, 26–28] reporting on the incident resulting in match injuries were included in the meta-analysis. Analysis showed that being tackled (29 per 1,000 player hours, 95 % CI 19–46) resulted in more injuries than any other incident, with all comparisons being clear (see Fig. 6). Tackling was the second most frequent injury incident (19 per 1,000 player hours, 95 % CI 12–29), which was substantially higher than all other match incidents except the ruck/maul (17 per 1,000 player hours, 95 % CI 11–26), the comparison with which was unclear. The mean incidence rates per 1,000 player hours with 95 % CIs of the remaining match incidents were, in descending order: collisions, 11 (7–17); scrums, 7 (5–12); other, 6 (3–9); and lineouts, 1 (0–3). Note, exposure to forward-specific scrum and lineout injuries was adjusted for appropriately in the analysis. All the remaining comparisons were substantially different, with the exception of ‘other versus scrums’, which was unclear. The five studies [32–36] that could not be combined in the meta-analysis also reported that the majority of injuries occurred in the tackle phase.

Injury incidence (with 95 % confidence intervals) by injury incident
3.9 Trends in Injury Risk Over Time
Bathgate et al. [32] reported that incidence rates in the periods before (1994–1995) and after (1996–2000) the start of the professional era in the Australian international team were 47 per 1,000 player hours and 74 per 1,000 player hours, respectively. Garraway et al. [29] reported an increase in the proportion of players injured in senior rugby clubs in the Scottish Borders district, from 27 % in 1993–1994 to 47 % in 1997–1998. The England Rugby Premiership Injury Surveillance Project has been used to monitor injuries in Premiership teams since 2002 [30]. During this period, the incidence of match injuries has remained relatively constant, varying between 75 per 1,000 player hours (2005–2006) to an upper limit of 100 per 1,000 player hours (2002–2003 and 2008–2009), with no clear trends apparent. However, a small increasing trend in overall match injury burden (days absence per 1,000 player hours) was evident, with an average increase of ~53 days per season over this period.
4 Discussion
This meta-analysis confirms match injury incidence rates in professional Rugby Union can be considered high in comparison with other team sports, but similar to other collision sports. For example, the incidence of injuries in international ice hockey was reported to be 79 per 1,000 player hours [5], while Gabbett [37] reported an incidence rate of 68 per 1,000 player hours in semi-professional Rugby League players (using a ‘missed match’ injury definition). The incidence of training injuries in Rugby Union is comparable with sports such as soccer [38] and American football [39]. By pooling data from several studies that use comparable methodologies, overall estimates of injury data were produced that more accurately reflect the injury incidence present amongst this elite population than data provided in individual studies. A higher level of play was associated with a greater incidence of injuries in matches, while trivial differences were found in injury incidence and severity between forwards and backs. The severity of recurrent injuries was, on average, 10 days greater than new injuries. Muscle/tendon and joint (non-bone)/ligament injuries were the two most prevalent injury groups, whereas fractures and bone stress injuries had the highest average severity. The lower limb was the body region with the highest injury incidence, while upper limb injuries were most severe. The third quarter (40–60 min) of matches had the highest injury incidence, and injuries most commonly occurred as a result of being tackled.
In agreement with extant literature [35, 36, 40], a higher level of play was associated with a greater incidence of injuries. International matches had the highest incidence of injuries, although this was inflated somewhat by one study following the England 2003 Rugby World Cup squad that reported an incidence rate of 218 injuries per 1000 player hours [22]. When this study was excluded from the analysis, differences in incidence rates between international and level one club levels became unclear, with incidence rates per 1,000 player hours with 95 % CIs of 90 (75–110) and 91 (84–97), respectively. The overall incidence rate for matches in senior men’s professional rugby was also substantially higher than rates previously reported in community rugby (17 per 1,000 player hours, 95 % CI 16–19) [41], women’s elite rugby (36 per 1,000 player hours, 95 % CI 26–49) [42] and youth elite academy rugby (47 per 1,000 player hours, 95 % CI 39–57) [43]. Proposed explanations for the greater incidence of injuries at higher levels of play include increased size and strength of players, longer seasons, higher levels of competitiveness, more efficient injury reporting regimes, greater distance covered by players at relatively fast running speeds (in excess of 5 m/s) and greater ball-in-play time [22, 35, 36, 44]. Moreover, data relating to international teams is typically collected in a tournament setting, which may be inherently different to matches played throughout a seasonal competition. There were no clear differences in the mean severity of injuries between these levels of play. Factors that may influence the reported number of days absence due to injury include the level of medical and rehabilitative care available and the pressure to return to play [45].
New injuries occur substantially more often than recurrent injuries, with the typical incidence rate ratio of new to recurrent injuries being 7:1. There was an exception to this finding among a small sample of players (n = 30) during one season in the Border Reivers District club competition in Scotland, where an incidence rate ratio of 0.8 (56 % of all injuries were recurrences) was reported [29]. While recurrent injuries appear to account for a relatively small proportion of all injuries (~12 %), the severity of recurrent injuries appears to be considerably greater than new injuries. This highlights the need to ensure players are fully and effectively rehabilitated before returning to play. However, it should be noted that no studies have directly compared the severity of recurrent injuries to their index injuries; it may be that some types of injury are more likely to reoccur, and if these tend to result in substantial time-loss then the recurrent injury severity figure may be skewed. This warrants investigation in future studies. Fuller et al. [46] noted the need to differentiate between ‘exacerbations’ and ‘re-injuries’, based on whether a player was fully recovered from the preceding index injury. These authors (Fuller et al.) believe this will enable researchers to investigate risk factors for these two types of recurrent injuries separately, and will also allow them to determine how well players have been rehabilitated before returning to full participation. Further developments in the taxonomy of recurrent injuries have recently been proposed, with the intention to fully explore the extent to which subsequent injuries (multiple, recurrent, exacerbation or new) are related to previous index injuries [47, 48]. These proposed developments are yet to appear in published studies.
A trivial difference was found in injury rates and severity between forwards and backs. It may be that greater homogeneity in the nature of involvement in contact events across positions [49] has narrowed the gap between these grouped playing positions with regards to injury risk, which had previously been reported to be higher amongst forwards [32, 33, 36]. However, while no clear differences appear to exist in overall injury profile between these grouped playing positions, Brooks and Kemp [50] found a number of significant differences in injury profile for players in individual playing positions. Thus, there are likely to be position-specific differences in match injury profiles, determined by the physical and technical requirements of each position [51], which may be used to design more targeted injury-prevention programmes.
The clear finding of a lower incidence of injuries in the first quarter in comparison with other match periods may indicate that fatigue is implicated in injury aetiology [52]; factors contributing to this (e.g. hydration, nutrition, and biomechanical alterations to technique) require further investigation. For instance, in elite Rugby League players, the quality of tackling technique has been shown to diminish under fatigue [53], which may in turn be responsible for fatigue-related tackling injuries. The third quarter (40–60 min) appears to have the greatest incidence of injury. Incomplete warm up or reduced concentration following the half-time break may be factors that are implicated in this trend [32], and so efforts should be made to improve player preparation and to develop strategies for player substitution to alleviate this risk factor. However, the proportion of third-quarter injuries sustained by players that started the match versus replacement players has not been reported in the literature; such information may influence any injury prevention strategies.
Muscle/tendon and joint (non-bone)/ligament injuries were the two most prevalent injury groups, whereas fractures and bone stress injuries had the highest average severity; joint (non-bone)/ligament injuries had the highest overall injury burden (a product of incidence and severity [54]). The lower limb was the body region with the highest injury incidence, while upper limb injuries were most severe; overall injury burden was highest for lower-limb injuries. Thigh haematomas and hamstring injuries have been identified as the most common Rugby Union injuries in a previous study [23], and so these may account for the high burden of lower-limb injuries identified in the present review. Thigh haematomas are likely a result of the contact events that are common to Rugby Union [55], while the requirement for high-speed running, accelerations and decelerations within Rugby Union matches may be responsible for the incidence of hamstring injuries [23]. Being tackled was the most common injury incident, which is expected given that the tackle is by far the most common contact event in Rugby Union matches [55]. Injuries were most commonly of moderate (8–28 days) severity, which would usually result in players missing between one and four matches.
While there is some evidence to suggest that injury incidence increased following the introduction of professionalism in 1995 [29, 32], these studies have noteworthy methodological limitations. Bathgate et al. [32] reported that incidence rates in the periods before (1994–1995) and after (1996–2000) the start of the professional era in the Australian international team were 47 per 1,000 player hours and 74 per 1,000 player hours, respectively. However, no confidence limits were reported for these rates, and this study was limited to just one team. Garraway et al. [29] reported an increase in the proportion of players injured in senior rugby clubs in the Scottish Borders district, from 27 % in 1993–1994 to 47 % in 1997–1998. However, only 30 professional players were included in this sample, and results are likely to be confounded by rule changes. A small trend towards an increase in overall match injury burden since 2002/2003 was found within the England Rugby Premiership Injury Surveillance Project [30]. However, this finding may not necessarily represent an increase in injury risk for players as injury severity is influenced by multiple ‘return-to-play’ factors. Indeed, increasing trends in the number of first-team squad players [56] and reductions in the injury burden caused by recurrent injuries [30] may indicate more effective rehabilitation of injured players, and/or reduced external pressure to return to play. The question of whether injuries in Rugby Union are becoming more common or severe warrants further investigation, across a varied cohort of players.
In order to bring about worthwhile reductions in overall injury burden, efforts should target aspects of the game causing the greatest total absence from playing and training [4]. For example, strategies targeting lower-limb injury prevention and methods for increasing safe behaviour in contact situations should be considered. Provision of evidence-based information about injury risks and injury prevention strategies to coaches and referees has been successful in reducing injury incidence in community rugby [57]; it would be interesting to determine whether such strategies could be effective in increasing safe behaviour in contact situations at the elite level. However, at the elite level there is typically a fine balance to be made between performance optimization and safety considerations, which may make interventions that directly alter the nature of the game difficult to implement. Efforts to minimise fatigue-induced reductions in tackling technique may be useful in reducing the incidence of tackle-related injuries [53]. Moreover, promising effects of Nordic hamstring strengthening exercises in reducing hamstring injuries have been observed in professional Rugby Union players [58], and so the effectiveness of a large-scale intervention warrants further study.
Methodological limitations were associated with many of the older studies included in this review, namely variations in injury and severity definitions, a lack of uniform data collection methods, and inclusion of players from only one team (i.e. small sample sizes). Since the 2007 consensus statement [9], the methodological quality of published studies has improved, allowing for more effective interpretation and comparison of findings across studies. Nonetheless, it is difficult to ensure consistency in reporting and data collection practices across studies and teams. Factors such as the level of motivation, support and time available to data collectors within each team will influence the reported injury rates, particularly when considering minor injuries. Providing a breakdown of injury rates by team in multi-team injury surveillance studies would at least allow for some consideration of this effect. A recognised limitation of the present review is that the sample size of studies included was not sufficient to investigate interactive effects within factors (e.g. playing position by level of play). It may be that differences exist between such levels, but these were not accounted for in the present analysis. With continuing injury surveillance amongst this elite population, it is hoped that future studies can add to this data set so that such effects may be investigated. Additionally, while a recent review of tools for assessing the quality of observational studies stated that qualitative checklists were more appropriate than quantitative scales, and that the STROBE statement was a suitable starting point [59], it should be noted that the STROBE statement was not designed to evaluate the methodological quality of studies, and so may not have been appropriate for assessing the risk of bias in the included studies [14]. A further limitation of the present review is that the analysis was weighted towards data provided by the England Rugby Premiership Injury Surveillance Project, which may differ substantially to rugby played in other leagues.
The data presented in this review on the incidence and nature of injuries in senior men’s professional Rugby Union summarises information relating to the initial steps of the injury prevention model [12]. During the next step, relevant preventative measures are introduced and evaluated. Large-scale injury prevention programmes have been successfully implemented in community level rugby (e.g. Rugby Smart [57]) and other football codes (e.g. FIFA 11+ [60]); the application of such measures in an elite professional Rugby Union population should be a priority for future research.
5 Conclusions
By combining data from a number of prospective cohort studies, it was possible to calculate accurate estimates of injury incidence in senior men’s professional Rugby Union. The combined analysis reduces potential biases associated with individual studies and variability associated with imprecise estimates [11], and so provides an effective overview of the epidemiological data.
The overall incidence of match injuries in senior men’s professional Rugby Union matches was comparable with rates reported in other team collision sports, while a higher level of play was associated with a greater reported incidence of injuries in matches. Recurrent injuries were typically of greater severity than new injuries, and so should be a target for future injury prevention studies. Joint (non-bone)/ligament injuries and lower-limb injuries had the highest injury burden for injury group and body region, respectively. The third quarter (40–60 min) of matches had the highest injury incidence, and injuries most commonly occurred as a result of being tackled. Future studies should focus on introducing and evaluating preventative measures that target the risk factors highlighted in this meta-analysis, in order to reduce the injury burden within senior men’s professional Rugby Union.
References
Chadwick S, Semens A, Schwarz EC, et al. Economic impact report on global rugby. Part III: Strategic and emerging markets. 2010; http://www.irb.com/mm/document/newsmedia/mediazone/02/04/22/88/2042288_pdf.pdf (Accessed 31 Aug 2012).
Roberts SP, Trewartha G, Higgitt RJ, et al. The physical demands of elite English rugby union. J Sports Sci. 2008;26(8):825–33.
Macqueen AE, Dexter WW. Injury trends and prevention in rugby union football. Curr Sports Med Rep. 2010;9(3):139–43.
Brooks JHM, Kemp SPT. Recent trends in rugby union injuries. Clin Sports Med. 2008;27(1):51–73.
Lorentzon R, Wedren H, Pietila T, et al. Injuries in international ice hockey—a prospective, comparative-study of injury incidence and injury types in international and Swedish elite ice hockey. Am J Sports Med. 1988;16(4):389–91.
Phillips LH, Standen PJ, Batt ME. Effects of seasonal change in rugby league on the incidence of injury. Br J Sports Med. 1998;32(2):144–8.
Meyers MC, Barnhill BS. Incidence, causes, and severity of high school football injuries on FieldTurf versus natural grass—a 5-year prospective study. Am J Sports Med. 2004;32(7):1626–38.
Orchard J, Seward H. Epidemiology of injuries in the Australian Football League, seasons 1997–2000. Br J Sports Med. 2002;36(1):39–44.
Fuller CW, Molloy MG, Bagate C, et al. Consensus statement on injury definitions and data collection procedures for studies of injuries in rugby union. Br J Sports Med. 2007;41(5):328–31.
Blettner M, Sauerbrei W, Schlehofer B, et al. Traditional reviews, meta-analyses and pooled analyses in epidemiology. Int J Epidemiol. 1999;28(1):1–9.
Checkoway H. Data pooling in occupational studies. J Occup Environ Med. 1991;33(12):1257–60.
Van Mechelen W, Hlobil H, Kemper HCG. Incidence, severity, etiology and prevention of sports injuries—a review of concepts. Sports Med. 1992;14(2):82–99.
Stroup DF, Berlin JA, Morton SC, et al. Meta-analysis of observational studies in epidemiology—a proposal for reporting. J Am Med Assoc. 2000;283(15):2008–12.
Von Elm E, Altman DG, Egger M, et al. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Prev Med. 2007;45(4):247–51.
Olmos M, Antelo M, Vazquez H, et al. Systematic review and meta-analysis of observational studies on the prevalence of fractures in coeliac disease. Dig Liver Dis. 2008;40(1):46–53.
International Rugby Board. Men’s Next Senior National Represntative Team. 2012; http://www.irb.com/mm/Document/LawsRegs/Regulations/02/06/29/68/nsrt.pdf (Accessed 10 Oct 2012).
Lystad RP, Pollard H, Graham PL. Epidemiology of injuries in competition taekwondo: a meta-analysis of observational studies. J Sci Med Sport. 2009;12(6):614–21.
Hopkins WG. A spreadsheet for combining outcomes from several subject groups. Sportscience. 2006;10:51–3.
Hopkins WG. Linear models and effect magnitudes for research, clinical and practical applications. Sportscience. 2010;14:49–57.
Hopkins WG. A spreadsheet for deriving a confidence interval, mechanistic inference and clinical inference from a p value. Sportscience. 2007;11:16–20.
Batterham AM, Hopkins WG. Making meaningful inferences about magnitudes. Int J Sports Physiol Perform. 2006;1(1):50–7.
Brooks JHM, Fuller CW, Kemp SPT, et al. A prospective study of injuries and training amongst the England 2003 Rugby World Cup squad. Br J Sports Med. 2005;39(5):288–93.
Brooks JHM, Fuller CW, Kemp SPT, et al. Epidemiology of injuries in English professional rugby union: part 1 match injuries. Br J Sports Med. 2005;39(10):757–66.
Brooks JHM, Fuller CW, Kemp SPT, et al. Epidemiology of injuries in English professional rugby union: part 2 training Injuries. Br J Sports Med. 2005;39(10):767–75.
Fuller CW, Clarke L, Molloy MG. Risk of injury associated with rugby union played on artificial turf. J Sports Sci. 2010;28(5):563–70.
Fuller CW, Laborde F, Leather RJ, et al. International Rugby Board Rugby World Cup 2007 injury surveillance study. Br J Sports Med. 2008;42(6):452–9.
Fuller CW, Raftery M, Readhead C, et al. Impact of the International Rugby Board’s experimental law variations on the incidence and nature of match injuries in southern hemisphere professional rugby union. S Afr Med J. 2009;99(4):232–7.
Fuller CW, Sheerin K, Targett S. Rugby World Cup 2011: International Rugby Board injury surveillance study. Br J Sports Med. 2012 (in press).
Garraway WM, Lee AJ, Hutton SJ, et al. Impact of professionalism on injuries in rugby union. Br J Sports Med. 2000;34(5):348–51.
Kemp SPT, Brooks JHM, Fuller CW, et al. England Rugby Premiership Injury and Training Audit: 2010–2011 Season Report. 2011.
Takemura M, Okayama A, Takazawa Y, et al. Injury profile in the highest-level rugby union competition in Japan. In: 7th World congress on science and football (WCSF), 2011. Nagoya University, Japan; 2011.
Bathgate A, Best JP, Craig G, et al. A prospective study of injuries to elite Australian rugby union players. Br J Sports Med. 2002;36(4):265–9.
Best JP, Mcintosh AS, Savage TN. Rugby World Cup 2003 injury surveillance project. Br J Sports Med. 2005;39(11):812–7.
Holtzhausen LJ, Schwellnus MP, Jakoet I, et al. The incidence and nature of injuries in South African rugby players in the rugby Super 12 competition. S Afr Med J. 2006;96(12):1260–5.
Jakoet I, Noakes TD. A high rate of injury during the 1995 Rugby World Cup. S Afr Med J. 1998;88(1):45–7.
Targett SGR. Injuries in professional rugby union. Clin J Sport Med. 1998;8(4):280–5.
Gabbett TJ. Influence of playing position on the site, nature, and cause of rugby league injuries. J Strength Cond Res. 2005;19(4):749–55.
Ekstrand J. Epidemiology of football injuries. Sci Sports. 2008;23(2):73–7.
Feeley BT, Kennelly S, Barnes RP, et al. Epidemiology of National Football League training camp injuries from 1998 to 2007. Am J Sports Med. 2008;36(8):1597–603.
Bird YN, Waller AE, Marshall SW, et al. The New Zealand rugby injury and performance project: V. Epidemiology of a season of rugby injury. Br J Sports Med. 1998;32(4):319–25.
Roberts SP, Stokes KA, Trewartha G, et al. RFU Community Rugby Injury Surveillance Project: 2011–2012 Season Report; 2012.
Taylor AE, Fuller CW, Molloy MG. Injury surveillance during the 2010 IRB Women’s Rugby World Cup. Br J Sports Med. 2011;45(15):1243–5.
Palmer-Green DS, Stokes KA, Fuller CW, et al. Match injuries in English youth academy and schools rugby union—an epidemiological study. Am J Sports Med. 2013;41:749–55.
Quarrie KL, Hopkins WG, Anthony MJ, et al. Positional demands of international rugby union: Evaluation of player actions and movements. J Sci Med Sport. 2013;16:353–9.
Creighton DW, Shrier I, Shultz R, et al. Return-to-play in sport: a decision-based model. Clin J Sport Med. 2010;20(5):379–85.
Fuller CW, Bahr R, Dick RW, et al. A framework for recording recurrences, reinjuries, and exacerbations in injury surveillance. Clin J Sport Med. 2007;17(3):197–200.
Hamilton GM, Meeuwisse WH, Emery CA, et al. Subsequent injury definition, classification, and consequence. Clin J Sport Med. 2011;21(6):508–14.
Finch, CF, Cook, J. Categorising sports injuries in epidemiological studies: the subsequent injury categorisation (SIC) model to address multiple, recurrent and exacerbation of injuries. Br J Sports Med. 2013.
Quarrie KL, Hopkins WG. Changes in player characteristics and match activities in Bledisloe Cup rugby union from 1972 to 2004. J Sports Sci. 2007;25(8):895–903.
Brooks JHM, Kemp SPT. Injury-prevention priorities according to playing position in professional rugby union players. Br J Sports Med. 2011;45(10):765–75.
Cahill N, Lamb K, Worsfold P, et al. The movement characteristics of English Premiership rugby union players. J Sports Sci. 2013;31:229–37.
Hughes DC, Fricker PA. A prospective survey of injuries to first-grade rugby union players. Clin J Sport Med. 1994;4:249–56.
Gabbett TJ. Influence of fatigue on tackling technique in rugby league players. J Strength Cond Res. 2008;22(2):625–32.
Brooks JHM, Fuller CW. The influence of methodological issues on the results and conclusions from epidemiological studies of sports injuries—illustrative examples. Sports Med. 2006;36(6):459–72.
Fuller CW, Brooks JHM, Cancea RJ, et al. Contact events in rugby union and their propensity to cause injury. Br J Sports Med. 2007;41(12):862–7.
Fuller CW, Taylor AE, Brooks JHM, et al. Changes in the stature, body mass and age of English professional rugby players: a 10-year review. J Sports Sci. 2013;31:795–802.
Gianotti SM, Quarrie KL, Hume PK. Evaluation of RugbySmart: a rugby union community injury prevention programme. J Sci Med Sport. 2009;12(3):371–5.
Brooks JH, Fuller CW, Kemp SP, et al. Incidence, risk, and prevention of hamstring muscle injuries in professional rugby union. Am J Sports Med. 2006;34(8):1297–306.
Sanderson S, Tatt LD, Higgins JPT. Tools for assessing quality and susceptibility to bias in observational studies in epidemiology: a systematic review and annotated bibliography. Int J Epidemiol. 2007;36(3):666–76.
Steffen K, Emery CA, Romiti M, et al. High adherence to a neuromuscular injury prevention programme (FIFA 11+) improves functional balance and reduces injury risk in Canadian youth female football players: a cluster randomised trial. Br J Sports Med. 2013.
Acknowledgments
We thank Reidar Lystad from Macquarie University, Australia, for providing statistical advice.
Funding
Funding for this review was provided by the Rugby Football Union and University of Bath.
Conflict of interest
Simon Kemp was an author on some of the original studies reviewed, but was not involved in the assessment of study quality in the present meta-analysis.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Williams, S., Trewartha, G., Kemp, S. et al. A Meta-Analysis of Injuries in Senior Men’s Professional Rugby Union. Sports Med 43, 1043–1055 (2013). https://doi.org/10.1007/s40279-013-0078-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40279-013-0078-1