
Abstract
Background
Atopic dermatitis (AD) is a chronic inflammatory skin disease common among infants and children. It is associated with a high risk of allergies, asthma, and mental health problems. Attempts have been made to use probiotics in clinical interventions for AD.
Objective
Our objective was to perform an updated meta-analysis of recently published studies to evaluate the effect of probiotics in the prevention and treatment of AD in children and to further understand the role of probiotics in AD interventions in the clinic.
Method
We searched the PubMed/MEDLINE, Embase, Cochrane Central Register of Controlled Trials, China National Knowledge Infrastructure, and Wanfang databases with prespecified selection criteria from inception of each database to 11 January 2020. No language restrictions were applied.
Results
A total of 25 studies were included in our meta-analysis. Of these, 14 were prevention studies (with 3049 children enrolled) and 11 were treatment studies (with 816 children enrolled). One treatment study was excluded after the sensitivity analysis. From the 14 prevention studies included, the pooled relative risk ratio of AD in those treated with probiotics versus placebo was 0.70 [95% confidence interval (CI) 0.57–0.84; P = 0.0002]. Subgroup analyses showed that only mixed strains of probiotics had a significant effect on lowering the incidence of AD. Probiotics administered solely to infants did not prevent the development of AD, but effects were significant when probiotics were administered to both pregnant mothers and their infants or solely to pregnant mothers. In studies with treatment durations > 6 months, the incidence of AD decreased significantly; a similar effect was achieved when the treatment duration was < 6 months. Meta-analysis of the ten treatment studies showed a significant decrease in the weighted mean difference (WMD) in Scoring Atopic Dermatitis (SCORAD) index values in the probiotics group compared with the control group (WMD, − 7.23; 95% CI − 10.59 to − 3.88; P < 0.0001). Subgroup analyses showed that both single-strain and mixed-strain probiotics had a significant effect on improving SCORAD values. Studies with participants aged < 1 year (P = 0.07) reported no significant results. In studies with treatment periods > 8 weeks, SCORAD values seemed to decrease more than in studies with treatment periods < 8 weeks. However, the subgroup difference was only statistically significant when the analysis was performed according to participant age in prevention studies.
Conclusion
Our updated meta-analysis demonstrates that interventions with probiotics potentially lower the incidence of AD and relieve AD symptoms in children, particularly when treating infants and children aged ≥ 1 year with AD. Interventions with mixed-strain probiotics tended to have better preventive and curative effects. Probiotics administered solely to infants appeared to produce negative preventive effects. Different intervention durations might also affect clinical outcomes. However, given the insignificant subgroup differences, except for treatment by participant age, and the moderate heterogeneity among the studies, these conclusions should be interpreted with caution, and more powerful randomized controlled trials using standardized measurements should be conducted to assess the long-term effects of probiotics.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Interventions with probiotics not only decreased the risk of atopic dermatitis (AD) but also relieved the symptoms of AD in children. |
Using mixed probiotic strains, longer treatment durations, pre-delivery administration, and treating infants and children aged ≥ 1 year tended to have better effects on the prevention and treatment of AD in children. |
1 Introduction
Atopic dermatitis (AD), a chronic inflammatory skin disease characterized by itching and recurrent eczematous lesions, is common among infants and children. It generally increases the risk of allergies, asthma, and mental health issues [1, 2]. The incidence of AD has increased globally over recent decades, and approximately 10–20% of infants and children experience the disease in developed countries [3]. Numerous nonpharmacological interventions (e.g., bathing practices, moisturizers) and topical pharmacotherapies (e.g., topical corticosteroids, calcineurin inhibitors, antihistamines) have been used routinely as first-line therapies to manage the disease [4]. However, nonpharmacological interventions mainly aim to reduce transepidermal water loss, thereby increasing skin hydration, and are used to treat mild disease. Furthermore, the safety issues related to the long-term use of topical corticosteroids (the first-line topical pharmacotherapy in treating AD) are gaining increasing attention, especially when the subjects are children. Other therapies such as antihistamines have been tried for the treatment of AD but unfortunately have demonstrated little utility [5]. Given the high prevalence of AD, its potential long-term health effects, and the safety concerns surrounding existing AD medicines, it is worth developing new therapies with promising effects and safety for use in both prevention and treatment.
According to the hygiene hypothesis, reduced exposure to infections in early childhood may result in the development of allergic diseases [6, 7]. In addition, some researchers have found that gut microbiota composition differs between infants with and without AD [8, 9]. Such evidence supports the idea that appropriate microbial colonization of the gut might lower the risk of developing atopic diseases. Probiotics, defined as living microorganisms that confer a health effect on the host when consumed in adequate amounts [10], are becoming increasingly attractive in the treatment of some gastrointestinal diseases (e.g., necrotizing enterocolitis and diarrhea) [11, 12]. Results from studies of the prevention and treatment of pediatric AD have been inconsistent [13,14,15,16]. Some related meta-analyses were published before 2017 [17,18,19,20,21,22,23] but concentrated on either the prevention of AD or the treatment effect of probiotics on AD. The conclusions differed, and no updated meta-analysis has been conducted to evaluate both effects simultaneously. Furthermore, some recent studies were omitted from previous meta-analyses. Our objective was to conduct a systematic literature review and a meta-analysis of randomized controlled trials (RCTs) investigating the effect of oral probiotics in the prevention and treatment of AD in children.
2 Methods
The current systematic review and meta-analysis was conducted following the Cochrane Handbook for Systematic Reviews of Interventions and conforms with PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analyses) guidelines [24].
2.1 Eligibility Criteria
We included all RCTs evaluating the effect of probiotics on AD, for either prevention or treatment of the disease. The inclusion criteria were as follows: (1) subjects were aged < 18 years; (2) probiotics were administered orally and the species, dosage, and duration of administration was clearly reported; (3) the control arm received placebo or other alternative interventions except prebiotics and synbiotics; (4) the primary endpoint was defined as the first follow-up time point after finishing the interventions, and studies from the same population with an extended follow-up period were excluded; (5) for prevention RCTs, the incidence of AD was assessed as an outcome measure and, for treatment RCTs, Scoring Atopic Dermatitis (SCORAD) index scores, widely used to assess AD severity, were reported to assess the effect of the intervention [25],and (6) the AD diagnosis was in accordance with standard searchable criteria.
Conference abstracts, letters, and comments were excluded because they provide limited information that would not allow us to properly evaluate the whole study.
2.2 Search Strategy
The following databases were searched without language restriction from the inception of each database to 11 January 2020: PubMed/MEDLINE, Embase, Cochrane Central Register of Controlled Trials, China National Knowledge Infrastructure, and Wanfang. All possible combinations of keywords for probiotics, AD, and RCTs in the title or abstract field were searched (the search strategies used in the English databases are provided in the electronic supplementary material [ESM]). Two individuals independently evaluated all retrieved articles according to the eligibility criteria. If opinions differed, we consulted the team leader and the issue was discussed until we reached consensus.
2.3 Data Extraction
Data from each study were independently extracted by two individuals who then checked the other’s results to avoid errors. Study details were recorded using a standardized data extraction form and included author names, year of publication, study country and area, population studied, inclusion and exclusion criteria, details of the intervention (specific probiotics, dose), specific placebo (dose, administration route), numbers of participants in each arm (included in analyses, noncompliant, and lost to follow-up), outcome measures, and duration of follow-up after the intervention. For RCTs designed to study the effect of more than one probiotic, we divided the whole intervention arm into subgroups according to the probiotic species administered and analyzed them as independent trials.
2.4 Risk-of-Bias Assessment
We used the Cochrane risk-of-bias tool to evaluate the included studies. Evaluation criteria included random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other biases, and each was categorized as low, unclear, or high risk of bias according to information provided by the original publications.
2.5 Statistical Analysis
Review Manager version 5.3 (Cochrane Collaboration, Nordic Cochrane Center, Copenhagen, Denmark) and the meta-analysis package STATA version 15.1 (STATA Corporation, College Station, TX, USA) were used to perform data analyses. For the prevention studies, the primary outcomes reported were the incidence of AD in the intervention and placebo groups. For the treatment studies, the primary outcomes reported were the mean change in SCORAD values from baseline in both groups. Relative risk ratios or pooled weighted mean differences (WMDs) and 95% confidence intervals (CIs) were estimated using a random-effects model based on the Der Simonian–Laird method. In studies that did not report the mean change, we used standard statistical techniques to calculate this information from the data reported. Forest plots were generated to visualize the interpretation of the individual study-specific and pooled estimates with respective 95% CIs. We used the χ2 test to identify statistical heterogeneity and the I2 statistic to quantify inconsistency. The level of heterogeneity was interpreted as modest (I2 ≤ 40%), moderate (40% < I2 ≤ 75%), or extreme (I2 > 75%). A funnel plot was constructed for the visual assessment of asymmetry, along with statistical estimates from Egger’s test to evaluate publication bias. A two-tailed P < 0.05 was regarded as a statistically significant difference.
2.6 Further Analysis
We decided to perform subgroup assessments in advance according to the type of probiotics used (mixed vs. single) and the treatment duration (≤ 6 vs. > 6 months or ≤ 8 vs. > 8 weeks) for both the prevention and the treatment studies, subject (both pregnant mothers and infant, pregnant mothers only, infants only) for prevention studies, and participant age (only those aged ≥ 1 year vs. includes infants aged < 1 year) for treatment studies. Extreme inconsistency (I2 > 75) led us to conduct a sensitivity analysis excluding studies one by one to find the cause of the inconsistency [26].
3 Results
3.1 Study Selection
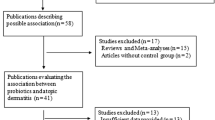
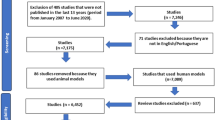
Our literature search resulted in 805 records; 372 duplicates were removed, leaving 433 records for the first stage of screening. A further 377 records were excluded because they were unrelated to the question, animal experiments, not clinical trials, reviews, were excluded publication types, or data were unavailable. In total, 56 records remained for full-text assessment. Of these, 31 articles were removed after careful review: six were not RCTs and 25 did not report the outcomes of interest (including those with an extended follow-up period from the same studies). Finally, 14 prevention studies (with 3049 children enrolled) [13, 14, 27,28,29,30,31,32,33,34,35,36,37,38] and 11 treatment studies (with 816 children enrolled) [15, 16, 39,40,41,42,43,44,45,46,47] were included in the final meta-analysis (Fig. 1).

Flow chart of the stepwise procedure for study selection
3.2 Study Characteristics
Table 1 summarizes the characteristics of each included study. Prevention studies consisted of two each from New Zealand, Finland, and Australia, with the remaining eight conducted in Korea, Taiwan, mainland China, Singapore, Norway, UK, Germany, or the Netherlands. Probiotics were administered to women in the mid or late stage of pregnancy and/or to their newborns soon after birth. Seven trials used single-strain probiotics. Treatment studies included two each from Korea and Ukraine, with others conducted in Spain, Turkey, Australia, Taiwan, Finland, Germany, and Japan. The subjects were all infants and children ranging in age from 0 to 17 years. Six trials used single-strain probiotics, and one used either single or mixed strains in two probiotic arms. For both prevention and treatment studies, Lactobacillus rhamnosus and Bifidobacterium were the most frequently used probiotics, whereas the dosage and duration varied among studies. All the included studies were published between 2001 and 2019.
3.3 Risk of Bias in the Included Studies
Figures S1A and S1B in the EMS summarize the risk-of-bias assessments and show both the individual risk of bias and the risk of bias within all included RCTs, respectively. Most studies adhered to high standards: 19 (76%) appropriately generated random sequences, 16 (64%) used adequate methods for allocation concealment, 18 (72%) blinded participants and personnel, and 17 (68%) blinded outcome assessors.
3.4 Probiotics for the Prevention of Atopic Dermatitis (AD)
3.4.1 Overall Clinic Effects
In total, 16 comparisons from 14 studies (with 3049 children included) were assessed using a random-effects model, and Fig. 2 shows the outcome of the meta-analysis. A significantly lower incidence of AD was found in the probiotics group, with a pooled relative risk ratio (RR) of AD in those treated with probiotics relative to those treated with placebo of 0.70 (95% CI 0.57–0.84; P = 0.0002). However, heterogeneity among the studies was significant (I2 = 65%; P = 0.0001).

Forest plot for pooled relative risk ratio of AD in those treated with probiotics
3.4.2 Clinical Effect by Type of Probiotic Bacterial Species
A total of 16 comparisons from 14 studies with different probiotics administered to the treatment group were divided into two subgroups according to whether a single (n = 7) or mixed (n = 9) strain of probiotics was used. Mixed-strain probiotics had a significant effect on lowering the incidence of AD (pooled RR 0.61; 95% CI 0.47–0.78; P = 0.004; I2 = 65%), but single-strain probiotics did not (pooled RR 0.84; 95% CI 0.66–1.09; P = 0.19; I2 = 50%) (Table 2; Fig. S2 in the ESM).
3.4.3 Clinical Effect by Subject
The subjects in the studies included in our meta-analysis varied. In eight comparisons from seven studies, probiotics were administered to both pregnant mothers and infants; four other comparisons treated only pregnant mothers, and the remaining four comparisons treated only infants. In the subgroup analyses, probiotics administered to both pregnant mothers and infants had a significant effect on reducing the incidence of AD (pooled RR 0.71; 95% CI 0.58–0.86; P = 0.0006; I2 = 18%), and a similar effect was achieved when probiotics were administered to mothers only (pooled RR 0.54; 95% CI 0.38–0.78; P = 0.001; I2 = 68%). However, when probiotics were administered to infants only, there was no significant effect on preventing the development of AD (pooled RR 0.88; 95% CI 0.59–1.33; P = 0.56; I2 = 74%) (Table 2; Fig. S3 in the ESM).
3.4.4 Clinical Effect by Duration of Treatment
A subgroup analysis was also performed to detect the effect of different treatment durations. For studies in which probiotics were administered to both mothers and infants, we combined the intervention durations of mothers and infants and calculated the total durations, selecting 6 months as the cut-off time point. For studies with treatment durations > 6 months, probiotics showed a significant effect on reducing the incidence of AD (pooled RR 0.73; 95% CI 0.61–0.87; P = 0.0003; I2 = 12%), and a similar effect was achieved with treatment durations < 6 months (pooled RR 0.67; 95% CI 0.46–0.97; P = 0.03; I2 = 82%); however, the subgroup difference was not statistically significant (P = 0.68) (Table 2; Fig. S4 in the ESM).
3.5 Probiotics for the Treatment of AD
3.5.1 Overall Clinical Effects
We assessed 12 comparisons from 11 studies (with 816 children included), and a random-effects model meta-analysis of all trials showed a significant decrease in the WMD of the SCORAD values in the probiotics group compared with the control group (WMD − 6.11; 95% CI − 10.62 to − 1.61; P = 0.008). However, the heterogeneity was extremely high (I2 = 90%; P < 0.00001) (Fig. S5 in the ESM). To better understand the origin of the heterogeneity, we performed a sensitivity analysis. After removing the study by Chernyshov [47], the heterogeneity decreased significantly (I2 = 72%), so we reviewed this study again and found that their results demonstrated that probiotics were inferior to placebo in terms of reducing SCORAD values (mean difference 14.4 vs. 18.1). On the other hand, in the same study, probiotics showed a superior effect on symptoms remission compared with placebo (remission rate 63.3 vs. 32.1%). The inconsistency in outcome measures may have contributed to the extremely high heterogeneity of the meta-analysis. After discussion, our team decided to remove the study, and the meta-analysis result of the remaining studies is shown in Fig. 3, from which it can be seen that the effect of probiotics on decreasing SCORAD values remains significant (WMD − 7.23; 95% CI − 10.59 to − 3.88; P < 0.0001).

Forest plot for WMD in change in SCORAD values in those treated with probiotics
3.5.2 Clinical Effect by Type of Probiotic Bacterial Species
Seven comparisons from six studies used single-strain probiotics (526 children), and four trials used mixed strains (290 children). For both the single-strain (WMD − 6.21; 95% CI − 9.35 to − 3.07; P = 0.0001; I2 = 38%) and the mixed-strain (WMD − 8.90; 95% CI − 16.13 to − 1.68; P = 0.02; I2 = 72%) groups, probiotics had a significant effect on improving SCORAD values, but no subgroup difference was found (P = 0.50) (Table 2; Fig. S6 in the ESM).
3.5.3 Clinical Effect by Participant Age
Five studies enrolled participants aged ≥ 1 year, and six comparisons from five other studies also included infants aged < 1 year. Probiotics showed a significant effect on improving SCORAD values for children aged ≥ 1 year with AD (WMD − 10.27; 95% CI − 14.49 to − 6.05; P < 0.00001; I2 = 74%) but had no effect in the comparisons that also included infants aged < 1 year (WMD − 3.67; 95% CI − 7.59 to 0.25; P = 0.07; I2 = 42%). It is of interest that the subgroup difference was significant (P = 0.02) (Table 2; Fig. S7 in the ESM).
3.5.4 Clinical Effect by Duration of Treatment
The treatment duration for each of the ten studies ranged from 4 to 24 weeks, so we decided to explore whether different treatment durations resulted in different effects. We selected 8 weeks, the median treatment period, as the cut-off time point. For trials with treatment periods < 8 weeks (531 children), probiotics significantly decreased SCORAD values (WMD − 5.13; 95% CI − 8.52 to − 1.74; P = 0.003; I2 = 57%). Trials with treatment durations > 8 weeks appeared to report a better effect in terms of decreasing SCORAD values (WMD − 11.02; 95% CI − 17.19 to − 4.84; P = 0.0005; I2 = 76%) than those with treatment durations < 8 weeks. However, no statistically significant difference between these two subgroups was found (P = 0.10). Hence, according to our results, prolonging treatment durations to > 8 weeks does not provide additional benefit (Table 2; Fig. S8 in the ESM).
3.6 Publication Bias
The funnel plots (Figs. S9 and S10 in the ESM) and Egger’s test results for both the prevention and the treatment studies revealed no evidence of publication bias. Both funnel plots were nearly symmetrical, and Egger’s test for the prevention (t − 0.90, P = 0.382) and the treatment studies (t − 0.73, P = 0.483) were not significant, indicating a low risk of bias.
4 Discussion
This systematic review summarized the updated evidence on the effects of probiotics for the prevention and treatment of AD among children. The pooled results demonstrated that, when compared with placebo, probiotics significantly reduced the incidence of AD (pooled RR 0.70; 95% CI 0.57–0.84; P = 0.0002) among healthy children and decreased SCORAD values (pooled WMD − 7.23; 95% CI − 10.59 to − 3.88; P < 0.0001) among children with AD. Subgroup analyses identified several interesting findings.
First, a significant effect of probiotics in preventing the development of AD was only found for the mixed-strain subgroup (RR 0.61). Previous meta-analyses by Doege et al. [23] and Zuccotti et al. [18] discussed the clinical effects of the type of probiotics but yielded inconsistent results, with Doege et al. [23] concluding that supplementation with probiotics significantly reduced the risk of AD [risk difference (RD) 0.057,P = 0.022]. However, this effect was significant only for single-strain probiotics (RD 0.106; P = 0.045) and not for mixed strains (RD 0.031; P = 0.204), whereas Zuccotti et al. [18] found that studies using a mixture of probiotics showed better results in a fixed-effect model (RR 0.54; 95% CI 0.43–0.68; P < 0.000). Our results correspond with those of Zuccotti et al. [18] and not those of Doege et al. [23]. It is worth noting that Zuccotti et al. [18] included outcomes in the same population at different follow-up time points. However, Doege et al. [23] focused solely on studies administering probiotics to expectant mothers so cannot provide a comprehensive understanding of the role of probiotics and may have underestimated the effects. We also found that remission of AD was achieved regardless of which probiotics were offered, and the treatment effect for the mixed-strain subgroup (WMD − 8.90) appeared better than that for the single-strain subgroup (WMD − 6.21). This conflicts with the results from the study by Huang et al. [22], who found that SCORAD values decreased significantly only in the mixed probiotics group (WMD − 3.52,95% CI − 5.61 to − 1.44; P = 0.006). We did not perform a further subgroup analysis according to the specific single-strain probiotics administered because only one prevention study used Bifidobacterium alone. A meta-analysis by Kim et al. [48], which included adult subjects, showed that mixed-strain probiotics had the greatest effect on decreasing SCORAD values (WMD − 6.60, P < 0.001), followed by Lactobacillus species (WMD − 3.81; P = 0.004), but Bifidobacterium species alone (WMD 1.75) showed a negative effect. The better effect of mixed-strain probiotics in preventing and treating AD may have resulted from a possible synergistic effect of multiple strains of bacteria in regulating the intestinal microbiome and thus the immune system, an effect that a single strain cannot achieve [49]. However, further research is needed to test this hypothesis.
Second, our meta-analysis found that different subjects manifested different preventive effects with probiotics. Whether probiotics were given to both pregnant mothers and their infants after birth or just to pregnant mothers, the incidence of AD decreased significantly in the treatment groups compared with the placebo groups, whereas no significant difference in the incidence of AD was observed when probiotics were given only to infants in the intervention group. Our results support the conclusions reached by Panduru et al. [19] and Pelucchi et al. [20]. Panduru et al. [19] found that prenatal administration of probiotics followed by postnatal administration was protective [odds ratio (OR) 0.61; P < 0.001], but administration in the postnatal period alone was not (OR 0.95; P = 0.82). Pelucchi et al. [20] also found that probiotics administered solely to the child had no effect on preventing AD (RR 0.85; 95% CI 0.61–1.19). This may be because the probiotics were administered for an insufficient duration. Evidence has shown that fetal production of immune factors may occur before delivery, which means that an earlier intervention might maximize the probiotic effects [50, 51]. However, more convincing evidence for understanding the establishment of the immune system and interactions between probiotics and fetal immunology is needed.
From our study, it seems that the effect of probiotics in the treatment of AD was influenced by participants’ age, as probiotics significantly improved SCORAD values only in participants aged ≥ 1 year (WMD − 10.27). Our conclusions are aligned with those of Kim et al. [48], who reported that probiotics had a significant effect in decreasing SCORAD values compared with placebo for children aged 1–18 years (WMD − 5.74; 95% CI − 7.27 to − 4.20), but the effectiveness of probiotics for infants (aged < 1 year) with AD was not observed. Huang et al. [22] also reported that the effectiveness of probiotics for infants (aged < 1 year) with AD was not significant. The transition of intestinal microbiota in infants has been proven to take 3–5 years after birth [52], during which the diversification of microbiota progressively continues and progresses toward an adult-like gut microbiota [53, 54]. A more complex and stable gut microbiome reacts better to nutrients and other ingested substances, which leads to different health outcomes [55]. In addition, studies have reported that the fetus receives immunity from the mother until the age of approximately 1 year, after which their own immune system develops [50]. An increasing number of studies has shown that the intestinal microbiome helps maintain physical health by modulating the immune system [56], and lower levels of Lactobacillus and Bifidobacterium are detected in infants with eczema [57, 58]. As a result, the administration of probiotics to infants aged > 1 year may relieve the severity of AD by regulating immune functions [59]. This evidence may explain the interesting phenomena we and other studies have found. Other factors, such as the specific types of probiotics administered, treatment duration, dosage, and so on, can also affect the results [52].
We explored the effect of treatment duration on both the prevention and the treatment of AD, which has rarely been discussed in other meta-analyses. For treatment studies, we found that probiotics administered for > 8 weeks decreased SCORAD values (WMD − 11.02) more than when the intervention period was < 8 weeks (WMD − 5.13). In other words, a longer treatment duration has tended toward better relief from AD, but this trend was not significant (P = 0.09). Some reviews concluded that the duration of probiotic administration may affect the clinical outcome of diseases [60], but the course of treatment in all studies included in our meta-analysis continued for at least 4 weeks, and SCORAD values decreased significantly in the probiotic groups. Therefore, we cannot determine the shortest valid treatment duration, and new studies with shorter treatment durations are needed to answer this question. For prevention studies, our analysis showed that intervention durations < 6 months achieved a better effect on decreasing the incidence of AD (RR 0.67) than the other subgroup (RR 0.73). Although the difference was not statistically significant, the results should be interpreted with caution because several factors may have contributed to the difference: first, the incidence of AD was measured immediately in only one study at the end of the intervention, whereas the remaining studies measured the incidence after follow-up of > 6 months after probiotic administration stopped, second, an assessment bias may exist when calculating the treatment durations for studies that administered probiotics to both mothers and infants.
It has been shown that intestinal microbiota play a vital role in regulating immune function and ensuring physical health [61], especially in infants and young children, whose intestinal microbiota are immature and easily affected by various environmental factors such as diet and antibiotics [55, 62, 63]. Therefore, scientists have been working to develop various new therapeutic schedules, such as probiotics, prebiotics, synbiotics, and fecal microbiota transplantation [64, 65], to regulate the gut microbiome, create a healthy intestinal environment, and further prevent and treat such diseases. Probiotics are the most commonly used of these therapeutics, and clinical trials have proven the curative effect of probiotics. However, the underlying mechanism remains unclear, especially for long-term effects. One hypothesis proposes that probiotics strengthen the gut epithelial barrier via competitive adherence to the mucosa and epithelium, and another proposes that probiotics modulate immune function and produce bioactive compounds [66]. Additionally, whether probiotics have long-term effects on regulating the gut microbiota is debatable because some studies concluded that probiotic administration did not influence the overall composition of the gut microbiota, and the probiotic bacteria did not persist once administration stopped [67, 68]. In addition, prebiotics, which are defined as food components or ingredients that are not digestible by the human body but specifically or selectively nourish beneficial colonic microorganisms [69], combined with probiotics, theoretically work better than probiotics alone [70]. For these reasons, the use of probiotics for the prevention and treatment of AD has not yet been established.
To the best of our knowledge, the only previous meta-analysis of the effect of probiotics in the treatment and prevention of AD was published in 2008 by Lee et al. [17]. No related meta-analysis has discussed the effect of the duration of probiotic administration in treating AD. Thus, an updated meta-analysis was necessary. In addition, unlike Lee et al. [17], we selected the first follow-up time point after finishing the interventions in each study as the outcome measuring point and excluded repetitive measurements in the same population with an extended follow-up period. As mentioned, the long-term effects of probiotics on AD are questionable, and many factors occurring after the probiotic interventions (e.g., diversification of microbiota and various environmental factors) can also affect the incidence and severity of AD. As a result, measuring outcomes as soon as possible after the intervention can better control bias related to known and unknown factors. Such a meta-analysis can strengthen and provide reliable evidence for the use of probiotics to prevent and treat AD in children.
Our meta-analysis has some limitations. First, heterogeneity between studies varied from modest to moderate. The different populations studied, species of probiotics used, dosages, and intervention durations may all have contributed to this heterogeneity. Second, a statistically significant difference between subgroups was only found for the treatment of AD by participant age, and further studies are needed before concluding that probiotics are more effective when mixed strains are used, interventions are prolonged, or both pregnant women and infants receive probiotics for the prevention of AD. Third, our meta-analysis cannot provide evidence for the long-term effects of probiotics in the prevention and treatment of AD; this would require more studies. Fourth, a common problem in probiotic intervention studies is a failure to assess adverse events [55]. Studies included in this meta-analysis reported no obvious adverse outcomes, so the safety of probiotics cannot be evaluated, further research should therefore focus on safety assessments. Moreover, although we found no evidence of publication bias, we did exclude some treatment RCTs because they did not administer probiotics orally or used different scales to assess the degree of AD, which may have affected our evaluation of the effects. Finally, the incidence of AD and SCORAD values are widely used to assess the effect of probiotics in clinical trials, but they are not enough to build a bridge between observation and mechanism. Some immune indicators and biomarkers, such as intestinal flora, have been used to illustrate this [39], but more work is required.
5 Conclusion
Our updated meta-analysis demonstrates that intervention with probiotics potentially lowers the incidence of AD and relieve AD symptoms in children, particularly in infants and children aged ≥ 1 year. Interventions using mixed-strain probiotics tended to show better preventive and curative effects. Probiotics administered solely to infants appeared to produce negative preventive effects. Different intervention durations might also affect clinical outcomes. However, these conclusions should be interpreted with caution because subgroup differences were insignificant (except for treatment by participant age) and heterogeneity was moderate among the studies. More powerful RCTs using standardized measurements should be conducted to assess the long-term effects of probiotics.
References
Sung M, Lee KS, Ha EG, Lee SJ, Kim MA, Lee SW, et al. An association of periostin levels with the severity and chronicity of atopic dermatitis in children. Pediatr Allerg Immunol. 2017;28(6):543–50.
Boguniewicz M, Schmid-Grendelmeier P, Leung DY. Atopic dermatitis. J Allergy Clin Immunol. 2006;118(1):40–3.
Weidinger S, Novak N. Atopic dermatitis. Lancet. 2016;387(10023):1109–22.
Eichenfield LF, Ahluwalia J, Waldman A, Borok J, Udkoff J, Boguniewicz M. Current guidelines for the evaluation and management of atopic dermatitis: a comparison of the Joint Task Force Practice Parameter and American Academy of Dermatology guidelines. J Allergy Clin Immunol. 2017;139(4S):S49–57.
Eichenfield LF, Tom WL, Berger TG, Krol A, Paller AS, Schwarzenberger K, et al. Guidelines of care for the management of atopic dermatitis: section 2. Management and treatment of atopic dermatitis with topical therapies. J Am ACad Dermatol. 2014;71(1):116–32.
Lewis MC, Inman CF, Patel D, Schmidt B, Mulder I, Miller B, et al. Direct experimental evidence that early-life farm environment influences regulation of immune responses. Pediatr Allergy Immunol. 2012;23(3):265–9.
Okada H, Kuhn C, Feillet H, Bach JF. The 'hygiene hypothesis' for autoimmune and allergic diseases: an update. Clin Exp Immunol. 2010;160(1):1–9.
Zheng H, Liang H, Wang Y, Miao M, Shi T, Yang F, et al. Altered gut microbiota composition associated with eczema in infants. PLoS ONE. 2016;11(11):e166026.
Hong P, Lee BW, Aw M, Shek LPC, Yap GC, Chua KY, et al. Comparative analysis of fecal microbiota in infants with and without eczema. PLoS ONE. 2010;5(4):e9964.
Guarner F, Schaafsma GJ. Probiotics. Int J Food Microbiol. 1998;39(3):237–8.
Vongbhavit K, Underwood MA. Prevention of necrotizing enterocolitis through manipulation of the intestinal microbiota of the premature infant. Clin Ther. 2016;38(4):716–32.
Binns C, Lee MK. The use of probiotics to prevent diarrhea in young children attending child care centers: a review. J Exp Clin Med. 2010;2(6):269–73.
Wickens K, Barthow C, Mitchell EA, Stanley TV, Purdie G, Rowden J, et al. Maternal supplementation alone with Lactobacillus rhamnosus HN001 during pregnancy and breastfeeding does not reduce infant eczema. Pediatr Allergy Immunol. 2018;29(3):296–302.
Dotterud CK, Storro O, Johnsen R, Oien T. Probiotics in pregnant women to prevent allergic disease: a randomized, double-blind trial. Br J Dermatol. 2010;163(3):616–23.
Navarro-Lopez V, Ramirez-Bosca A, Ramon-Vidal D, Ruzafa-Costas B, Genoves-Martinez S, Chenoll-Cuadros E, et al. Effect of oral administration of a mixture of probiotic strains on SCORAD index and use of topical steroids in young patients with moderate atopic dermatitis a randomized clinical trial. JAMA Dermatol. 2018;154(1):37–433.
Folster-Holst R, Muller F, Schnopp N, Abeck D, Kreiselmaier I, Lenz T, et al. Prospective, randomized controlled trial on Lactobacillus rhamnosus in infants with moderate to severe atopic dermatitis. Br J Dermatol. 2006;155(6):1256–61.
Lee J, Seto D, Bielory L. Meta-analysis of clinical trials of probiotics for prevention and treatment of pediatric atopic dermatitis. J Allergy Clin Immunol. 2008;121(1):116–21.
Zuccotti G, Meneghin F, Aceti A, Barone G, Callegari ML, Di Mauro A, et al. Probiotics for prevention of atopic diseases in infants: systematic review and meta-analysis. Allergy. 2015;70(11):1356–71.
Panduru M, Panduru NM, Salavastru CM, Tiplica GS. Probiotics and primary prevention of atopic dermatitis: a meta-analysis of randomized controlled studies. J Eur Acad Dermatol Venereol. 2015;29(2):232–42.
Pelucchi C, Chatenoud L, Turati F, Galeone C, Moja L, Bach JF, et al. Probiotics supplementation during pregnancy or infancy for the prevention of atopic dermatitis: a meta-analysis. Epidemiology. 2012;23(3):402–14.
Michail SK, Stolfi A, Johnson T, Onady GM. Efficacy of probiotics in the treatment of pediatric atopic dermatitis: a meta-analysis of randomized controlled trials. Ann Allergy Asthma Immunol. 2008;101(5):508–16.
Huang R, Ning H, Shen M, Li J, Zhang J, Chen X. Probiotics for the treatment of atopic dermatitis in children: a systematic review and meta-analysis of randomized controlled trials. Front Cell Infect Microbiol. 2017;7:392.
Doege K, Grajecki D, Zyriax BC, Detinkina E, Zu EC, Buhling KJ. Impact of maternal supplementation with probiotics during pregnancy on atopic eczema in childhood—a meta-analysis. Br J Nutr. 2012;107(1):1–6.
Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gotzsche PC, Ioannidis JP, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ. 2009;339:b2700.
Atherton J, Bieber T, Bonilazi E, Broberg A, Calza A, et al. Severity scoring of atopic dermatitis: the SCORAD index. Consensus Report of the European Task Force on Atopic Dermatitis. Dermatology. 1993;186(1):23–31.
Copas J, Shi JQ. Meta-analysis, funnel plots and sensitivity analysis. Biostatistics. 2000;1(3):247–62.
Wickens K, Black PN, Stanley TV, Mitchell E, Fitzharris P, Tannock GW, et al. A differential effect of 2 probiotics in the prevention of eczema and atopy: a double-blind, randomized, placebo-controlled trial. J Allergy Clin Immunol. 2008;122(4):788–94.
Kim JY, Kwon JH, Ahn SH, Lee SI, Han YS, Choi YO, et al. Effect of probiotic mix (Bifidobacterium bifidum, Bifidobacterium lactis, Lactobacillus acidophilus) in the primary prevention of eczema: a double-blind, randomized, placebo-controlled trial. Pediatr Allergy Immunol. 2010;21(2 Pt 2):e386–e393393.
Rautava S, Kainonen E, Salminen S, Isolauri E. Maternal probiotic supplementation during pregnancy and breast-feeding reduces the risk of eczema in the infant. J Allergy Clin Immunol. 2012;130(6):1355–60.
Plummer EL, Chebar LA, Tobin JM, Uebergang JB, Axelrad C, Garland SM, et al. Postnatal probiotics and allergic disease in very preterm infants: sub-study to the ProPrems randomized trial. Allergy. 2020;75(1):127–36.
Ou CY, Kuo HC, Wang L, Hsu TY, Chuang H, Liu CA, et al. Prenatal and postnatal probiotics reduces maternal but not childhood allergic diseases: a randomized, double-blind, placebo-controlled trial. Clin Exp Allergy. 2012;42(9):1386–96.
Taylor AL, Dunstan JA, Prescott SL. Probiotic supplementation for the first 6 months of life fails to reduce the risk of atopic dermatitis and increases the risk of allergen sensitization in high-risk children: a randomized controlled trial. J Allergy Clin Immunol. 2007;119(1):184–91.
Soh SE, Aw M, Gerez I, Chong YS, Rauff M, Ng YPM, et al. Probiotic supplementation in the first 6 months of life in at risk Asian infants—effects on eczema and atopic sensitization at the age of 1 year. Clin Exp Allergy. 2009;39(4):571–8.
Kalliomaki M, Salminen S, Arvilommi H, Kero P, Koskinen P, Isolauri E. Probiotics in primary prevention of atopic disease: a randomised placebo-controlled trial. Lancet. 2001;357(9262):1076–9.
Allen SJ, Jordan S, Storey M, Thornton CA, Gravenor MB, Garaiova I, et al. Probiotics in the prevention of eczema: a randomised controlled trial. Arch Dis Child. 2014;99(11):1014–9.
Kopp MV, Hennemuth I, Heinzmann A, Urbanek R. Randomized, double-blind, placebo-controlled trial of probiotics for primary prevention: no clinical effects of Lactobacillus GG supplementation. Pediatrics. 2008;121(4):e850–e856856.
Niers L, Martin R, Rijkers G, Sengers F, Timmerman H, van Uden N, et al. The effects of selected probiotic strains on the development of eczema (the PandA study). Allergy. 2009;64(9):1349–58.
Zhengchun G, et al. Probiotics have an early preventitive effect on the occurrence of atopic disease in children. Chin J Matern Child Health. 2004;11:120–1.
Nakata J, Hirota T, Umemura H, Nakagawa T, Kando N, Futamura M, et al. Additive effect of Lactobacillus acidophilus L-92 on children with atopic dermatitis concomitant with food allergy. Asia Pac Allergy. 2019;9(2):e18.
Woo SI, Kim JY, Lee YJ, Kim NS, Hahn YS. Effect of Lactobacillus sakei supplementation in children with atopic eczema-dermatitis syndrome. Ann Allergy Asthma Immunol. 2010;104(4):343–8.
Yesilova Y, Calka O, Akdeniz N, Berktas M. Effect of probiotics on the treatment of children with atopic dermatitis. Ann Dermatol. 2012;24(2):189–93.
Kim J, Han Y, Kim B, Ban J, Lee J, et al. Effects of Lactobacillus plantarum CJLP133 on pediatric atopic dermatitis: a double-blind, placebo-controlled trial. Allergy Eur J Allergy Clin Immunol. 2012;67:140–1.
Weston S, Halbert A, Richmond P, Prescott SL. Effects of probiotics on atopic dermatitis: a randomised controlled trial. Arch Dis Child. 2005;90(9):892–7.
Wu YJ, Wu WF, Hung CW, Ku MS, Liao PF, Sun HL, et al. Evaluation of efficacy and safety of Lactobacillus rhamnosus in children aged 4–48 months with atopic dermatitis: an 8-week, double-blind, randomized, placebo-controlled study. J Microbiol Immunol Infect. 2017;50(5):684–92.
Gerasimov SV, Vasjuta VV, Myhovych OO, Bondarchuk LI. Probiotic supplement reduces atopic dermatitis in preschool children: a randomized, double-blind, placebo-controlled, clinical trial. Am J Clin Dermatol. 2010;11(5):351–61.
Viljanen M, Savilahti E, Haahtela T, Juntunen-Backman K, Korpela R, Poussa T, et al. Probiotics in the treatment of atopic eczema/dermatitis syndrome in infants: a double-blind placebo-controlled trial. Allergy. 2005;60(4):494–500.
Chernyshov PV. Randomized, placebo-controlled trial on clinical and immunologic effects of probiotic containing Lactobacillus rhamnosus R0011 and L. helveticus R0052 in infants with atopic dermatitis. Microbl Ecol Health Dis. 2009;21(3/4):228–32.
Kim SO, Ah YM, Yu YM, Choi KH, Shin WG, Lee JY. Effects of probiotics for the treatment of atopic dermatitis: a meta-analysis of randomized controlled trials. Ann Allergy Asthma Immunol. 2014;113(2):217–26.
Chang YS, Trivedi MK, Jha A, Lin YF, Dimaano L, Garcia-Romero MT. Synbiotics for prevention and treatment of atopic dermatitis: a meta-analysis of randomized clinical trials. JAMA Pediatr. 2016;170(3):236–42.
Jones CA, Holloway JA, Warner JO. Does atopic disease start in foetal life? Allergy. 2000;55(1):2–10.
Landreth KS. Critical windows in development of the rodent immune system. Hum Exp Toxicol. 2002;21(9–10):493–8.
Zhuang L, Chen H, Zhang S, Zhuang J, Li Q, Feng Z. Intestinal microbiota in early life and its implications on childhood health. Genom Proteom Bioinform. 2019;17:13–25.
Valles Y, Artacho A, Pascual-Garcia A, Ferrus ML, Gosalbes MJ, Abellan JJ, et al. Microbial succession in the gut: directional trends of taxonomic and functional change in a birth cohort of Spanish infants. PLoS Genet. 2014;10(6):e1004406.
Rodriguez JM, Murphy K, Stanton C, Ross RP, Kober OI, Juge N, et al. The composition of the gut microbiota throughout life, with an emphasis on early life. Microb Ecol Health Dis. 2015;26:26050.
Milani C, Duranti S, Bottacini F, Casey E, Turroni F, Mahony J, et al. The first microbial colonizers of the human gut: composition, activities, and health implications of the infant gut microbiota. Microbiol Mol Biol Rev. 2017;81(4):e00036-17.
Gensollen T, Iyer SS, Kasper DL, Blumberg RS. How colonization by microbiota in early life shapes the immune system. Science. 2016;352(6285):539–44.
Björkstén B, Sepp E, Julge K, Voor T, Mikelsaar M. Allergy development and the intestinal microflora during the first year of life. J Allergy Clin Immunol. 2001;108(4):516–20.
Sjögren YM, Jenmalm MC, Böttcher MF, Björkstén B, Sverremark-Ekström E. Altered early infant gut microbiota in children developing allergy up to 5 years of age. Clin Exp Allergy. 2009;39(4):518–26.
Suzuki S, Kubota N, Kakiyama S, Miyazaki K, Sato K, Harima-Mizusawa N. Effect of Lactobacillus plantarum YIT 0132 on Japanese cedar pollinosis and regulatory T cells in adults. Allergy. 2020;75(2):453–6.
La Rosa PS, Warner BB, Zhou Y, Weinstock GM, Sodergren E, Hall-Moore CM, et al. Patterned progression of bacterial populations in the premature infant gut. Proc Natl Acad Sci USA. 2014;111(34):12522–7.
Thaiss CA, Zmora N, Levy M, Elinav E. The microbiome and innate immunity. Nature. 2016;535(7610):65–74.
Cantey JB, Wozniak PS, Pruszynski JE, Sanchez PJ. Reducing unnecessary antibiotic use in the neonatal intensive care unit (SCOUT): a prospective interrupted time-series study. Lancet Infect Dis. 2016;16(10):1178–84.
Gregory KE, Samuel BS, Houghteling P, Shan G, Ausubel FM, Sadreyev RI, et al. Influence of maternal breast milk ingestion on acquisition of the intestinal microbiome in preterm infants. Microbiome. 2016;4(1):68.
Passeron T, Lacour JP, Fontas E, Ortonne JP. Prebiotics and synbiotics: two promising approaches for the treatment of atopic dermatitis in children above 2 years. Allergy. 2006;61(4):431–7.
Costello SP, Hughes PA, Waters O, Bryant RV, Vincent AD, Blatchford P, et al. Effect of fecal microbiota transplantation on 8-week remission in patients with ulcerative colitis: a randomized clinical trial. JAMA. 2019;321(2):156–64.
Fontana L, Bermudez-Brito M, Plaza-Diaz J, Munoz-Quezada S, Gil A. Sources, isolation, characterisation and evaluation of probiotics. Br J Nutr. 2013;109(Suppl 2):S35–50.
Mah KW, Chin VI, Wong WS, Lay C, Tannock GW, Shek LP, et al. Effect of a milk formula containing probiotics on the fecal microbiota of Asian infants at risk of atopic diseases. Pediatr Res. 2007;62(6):674–9.
Kristensen NB, Bryrup T, Allin KH, Nielsen T, Hansen TH, Pedersen O. Alterations in fecal microbiota composition by probiotic supplementation in healthy adults: a systematic review of randomized controlled trials. Genome Med. 2016;8(1):52.
Bindels LB, Delzenne NM, Cani PD, Walter J. Towards a more comprehensive concept for prebiotics. Nat Rev Gastroenterol Hepatol. 2015;12(5):303–10.
Guarner F, Khan AG, Garisch J, Eliakim R, Gangl A, Thomson A, et al. World Gastroenterology Organisation Global Guidelines: probiotics and prebiotics October 2011. J Clin Gastroenterol. 2012;46(6):468–81.
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Funding
The study was funded by Major Scientific and Technological Projects for Collaborative Prevention and Control of Birth Defects in Hunan Province (2019SK1012), Major Research and Development Projects in Hunan Province (2018SK2060), and Scientific and Technological Department Projects in Hunan Province (2017SK50802).
Conflict of interest
Wen Jiang, Bin Ni, Zhiyu Liu, Xuan Liu, Wanqin Xie, Irene X.Y. Wu, and Xingli Li have no conflicts of interest that are directly relevant to the content of this review.
Data availability
All data generated or analyzed during this study are included in this published article and its supplementary information files.
Author contributions
WJ and XL developed the research question. WX and ZL conducted the literature search. WJ, BN, WX, and XL selected the literature, extracted the data, and assessed the risk of bias. IXYW and WX analyzed the data, and IXYW and WJ interpreted the results. WJ, IXYW, and XL wrote the manuscript. All authors contributed to the interpretation and revision of the manuscript.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Jiang, W., Ni, B., Liu, Z. et al. The Role of Probiotics in the Prevention and Treatment of Atopic Dermatitis in Children: An Updated Systematic Review and Meta-Analysis of Randomized Controlled Trials. Pediatr Drugs 22, 535–549 (2020). https://doi.org/10.1007/s40272-020-00410-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40272-020-00410-6