
Abstract
Background
Relapsing–remitting multiple sclerosis (RRMS) is an incurable disease characterised by relapses (periods of function loss) followed by full or partial recovery, and potential permanent disability over time. Many disease-modifying treatments (DMTs) exist that help reduce relapses and slow disease progression. Most are contraindicated during conception/pregnancy and some require a discontinuation period before trying to conceive. Although around three-quarters of people with RRMS are women, there is limited knowledge about how reproductive issues impact DMT preference.
Objective
The aim of this study was to measure the preferences for DMTs of women with RRMS who are considering pregnancy.
Design
An online discrete choice experiment (DCE).
Methods
Participants chose between two hypothetical DMTs characterised by a set of attributes, then indicated if they preferred their choice to no treatment. Attributes were identified from interviews and focus groups with people with RRMS and MS professionals, as well as literature reviews, and included the probability of problems with pregnancy, discontinuation of DMTs, and breastfeeding safety. In each DCE task, participants were asked to imagine making decisions in three scenarios: now; when trying to conceive; and when pregnant.
Analysis
Two mixed logit models were estimated, one to assess the statistical significance between scenarios and one in maximum acceptable risk space to allow comparison of the magnitudes of parameters between scenarios.
Sample
Women with RRMS who were considering having a child in the future, recruited from a UK MS patient register.
Results
Sixty respondents completed the survey. Participants preferred no treatment in 12.6% of choices in the ‘now’ scenario, rising significantly to 37.6% in the ‘trying to conceive’ scenario and 60.3% in the ‘pregnant’ scenario (Kruskal–Wallis p < 0.001). This pattern corresponds with results from models that included a no-treatment alternative-specific constant (ASC) capturing differences between taking and not taking a DMT not specified by the attributes. The ASC was lower in the trying to conceive scenario than in the now scenario, and lower still in the pregnant scenario, indicating an intrinsic preference for no treatment. Participants also placed relatively less preference on reducing relapses and avoiding disease progression in the trying to conceive and pregnant scenarios compared with a lower risk of problems with pregnancy. In the trying to conceive scenario, participants’ preference for treatments with shorter washout periods increased.
Conclusion
Women with RRMS considering having a child prefer DMTs with more favourable reproduction-related attributes, even when not trying to conceive. Reproductive issues also influenced preferences for DMT attributes not directly related to pregnancy, with preferences dependent on the life circumstances in which choices were made. The design of the DCE highlights the benefits of considering the scenario in which participants make choices, as they may change over time.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
We used a discrete choice experiment to study the preferences for disease-modifying treatments of women with relapsing–remitting multiple sclerosis who may be considering having a child. |
Using an innovative design, we elicited preferences in three scenarios: now, when trying to conceive, and when pregnant. |
In the trying to conceive and pregnant scenarios, participants were more likely to choose no treatment, with participants having both a greater intrinsic preference for no treatment and considering the benefits of treatment relatively less important compared with potential problems with pregnancy. |
1 Introduction
Multiple sclerosis (MS) is an incurable inflammatory and degenerative disease of the central nervous system [1,2,3] that affects an estimated 150 people in every 100,000 [4]. Around 75% of people with MS are women [5] and the disease typically first appears in younger people, with a mean age of diagnosis at around 30 years [6, 7]. The most common form of the disease at diagnosis is relapsing–remitting MS (RRMS), which affects around 85% of patients [1]. RRMS is characterised by temporary episodes of loss of function (termed relapses), followed by full or partial recovery, with a wide range of symptoms, including loss of vision, mobility problems, pain, fatigue and cognitive impairment [1].
No cure exists for MS but many disease-modifying treatments (DMTs) are available for RRMS that can reduce the frequency of relapses and lower the risk of accumulating disability [8, 9]. Individuals’ choices as to which DMT to take, or whether to take a DMT at all, can be complex as treatments vary in efficacy and adverse effect profile. They also vary in mode of administration, with tablet, self-injection and infusion-based treatments all available [10, 11].
Reproductive choices have an impact on the decision of which (if any) DMT to take (and vice versa) [12,13,14]. Although some DMTs (e.g. glatiramer acetate) are well tolerated in pregnancy [15] others are contraindicated due to problems with conception, pregnancy and/or breastfeeding, and there is a lack of evidence for some DMTs as to whether they are well tolerated during conception/pregnancy or not [16,17,18,19,20]. The risks associated with some DMTs include increased risks of miscarriage, premature birth, low birth weight and congenital anomalies. Further complicating the decision-making context is the fact that pregnancy and childbirth can affect the course of women’s MS. For example, some evidence suggests women may experience a reduction in their relapse rate when pregnant but an increased risk of relapse in the postpartum period [21,22,23,24], although more recent evidence does not support the hypothesis of an increase in disease activity postpartum [25]. Finally, there is evidence that some women with RRMS (wwRRMS) have concerns about the impact of their disease on their ability to care for a newborn [26, 27], which has the potential to influence preferences for treatment. Nonetheless, the influence of reproductive issues on women’s preferences is still not well understood. Clinician advice around reproduction and DMTs may vary due to the lack of an evidence base on treatment safety, particularly for newer treatments [28,29,30,31]. A better understanding of how reproduction influences women’s preferences for DMTs could help to develop more effective strategies to support their decision-making process.
This study uses a discrete choice experiment (DCE) to investigate the impact reproductive issues have on women’s DMT preferences [32,33,34]. It is part of a wider project entitled Considering RIsk and benefits in Multiple Sclerosis treatment selection (CRIMSON), which examined the preferences for and attitudes towards DMTs of people with RRMS, using a variety of approaches. The project included qualitative studies [35], literature reviews [12, 34] and two linked DCEs, one without reproduction-related attributes and the current study, which specifically examined reproduction. The evidence from these studies was then used in the development of a patient decision aid [36] for people with RRMS making DMT choices [37].
Previous DCE studies have explored people’s preferences for MS treatments [34, 38,39,40], but only one has explored how reproductive issues impact treatment preferences [41]; reproduction has been highlighted as a neglected area in the DCE literature in MS [34].
This study’s primary aim was to examine reproduction-related attributes of DMTs in detail. We recruited women considering having a child in the future, for whom reproductive issues were assumed to be most relevant [12]. The study also aimed to capture the dynamic nature of DMT decision making and how reproduction influences choices at different points in people’s lives. Participants were asked to imagine making their choices between DMTs in three different scenarios: now, when trying to conceive, and when pregnant. An additional aim of the study was to assess the feasibility of using such a design and whether participants would make systematically different choices in different scenarios.
2 Methods
2.1 Sample
The target population was wwRRMS who indicated they intended to have children in the future. Recruitment was undertaken online using the MS Register (ukmsregister.org), a large UK panel of people with MS who are regularly invited to participate in research surveys. The MS Register has over 15,000 people registered, although, at the time of recruitment, only a fraction had consented to receive invitations from third parties to take part in research such as this study. No payment was given for participation.
2.2 Materials
In line with good practice [42, 43], the survey instrument was developed using a qualitative process and following established guidelines [44,45,46]. This involved interviews (n = 30) with people with RRMS [35] and three focus groups (n = 17) including people with RRMS, neurologists and MS nurses to generate candidate attributes.
A finding that emerged from the qualitative data collection was that reproduction-related aspects of DMTs were important factors in many participants’ decision making. Reproductive issues were also identified as a neglected topic in DCEs in MS [12, 34]. However, including reproduction-specific attributes in a DCE targeted at all people with RRMS would not give an appropriate measure of their importance, since they would only be relevant to a subset of the target population. The original study design of a single DCE was hence changed in response to the emerging qualitative findings. This resulted in two DCEs, one without reproduction-specific attributes with a target population of all people with RRMS, and one with wwRRMS who were considering having a child in the future.
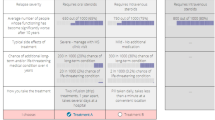
A ranking exercise was conducted with four workshops (n = 33) of people with RRMS to prioritise which attributes to include. In order not to overburden participants, two attributes included in the general DCE were excluded from the reproduction DCE. Participants were asked to assume that all DMTs in the reproduction DCE were identical in terms of the two attributes from the main DCE that were dropped.Footnote 1 A draft survey was refined in an iterative process of 28 think-aloud interviews with people with RRMS. This process addressed whether the survey was understandable, whether attributes and levels were interpreted as intended, whether the tasks presented an acceptable burden, and general presentation and usability issues. Probabilistic risk information was presented using simple numerical formats accompanied by visual aids (see Fig. 1), following evidence-based principles to facilitate understanding [47, 48]. The final list of attributes and levels for the reproduction DCE is shown in Table 1, and the attributes and levels included in the general DCE only are shown in the electronic supplementary material (ESM), along with a copy of the survey that shows how attributes and levels were explained to participants.

Example choice task. MS multiple sclerosis
The reproduction DCE had a dual response, multiple scenario design. Participants first chose which of two DMTs they preferred, and then indicated whether they preferred the DMT to no treatment. They were also asked to imagine making decisions in three scenarios. First, they were asked to imagine making their choice now, then making their choice when trying to conceive, and, finally, making their choice when pregnant. Figure 1 gives screenshots of a sample question, while Fig. 2 shows how each individual subquestion was presented sequentially.

Illustration of how scenarios were presented sequentially. Each subfigure shows the additional task that was presented after participants responded to the previous task
A Bayesian D-efficient statistical design for the reproduction DCE was created using Ngene,Footnote 2 with a main effects model with zero priors. Choices where one treatment was superior on all levels apart from mode of administration were excluded. The final design had 10 blocks of five questions each. The Ngene code is available in the ESM. The order the attributes were presented in was randomised between participants, but was consistent across questions for a given participant, and pregnancy-specific attributes were grouped together.
2.3 Procedure
Participants completed a DCE without reproduction-related attributes, then a short series of questions about themselves, their RRMS and their treatment history. Both male and female participants were asked “Are you or your partner thinking about having a child, either soon or in the next few years? (yes/no).” If they responded yes, they were asked to complete the reproduction DCE. Male participants completed a reproduction DCE without the attribute ‘safe to breastfeed’ scenario or the ‘pregnant’ scenario. These data were not analysed due to a small sample size (n = 7). Participants were asked if they were currently trying to conceive or were currently pregnant, with the aim of incorporating this information into the modelling.
2.4 Analysis
The fraction of times each participant chose no treatment as their most preferred option in each scenario was calculated. The statistical significance of differences between scenarios was assessed using a Kruskal–Wallis test.
Two models were estimated. One was designed to assess whether differences between scenarios were statistically significant and the other was designed to allow comparison of the magnitudes of participants’ preferences between scenarios. The utility individual \(i\) receives from choosing treatment \(j\) over the alternative treatment in choice situation \(k\) was assumed to take the form of Eq. 1:
where \(\varvec{x}_{ijk}\) is a vector indicating the levels of each attribute for treatment \(j\) in situation \(k\), \(\varvec{\beta}_{ik}\) is a vector describing \(i\)’s preferences, and \(\varepsilon_{ijk}\) is an independent and identically distributed extreme valued error term. The utility that \(i\) receives from choosing no treatment over treatment is assumed to take the same form as the above equation, with the addition of an alternative-specific constant (ASC). The ‘no treatment’ ASC is interpreted as capturing all aspects of taking no treatment compared with taking a DMT not explicitly captured by the attributes. For example, it might include an intrinsic desire for treatment, due to taking a DMT giving a sense of control over an individual’s disease, over and above any benefits it brings [12]. Alternatively, it might include an intrinsic preference for avoiding treatment to prevent it affecting an unborn child, over and above any explicitly stated risk.
The probability of choosing treatment \(j \in \left\{ {1,2} \right\}\) over treatment \(l \ne j\) in the first stage, and then preferring \(n \in \left\{ {j,{\text{no treatment}}} \right\}\) in the second stage is shown in Eq. 2:
where \(V_{j} = \varvec{\beta}_{ik} \varvec{x}_{ijk}\) is the deterministic component of utility.
A mixed logit model was used, with coefficients, including the no treatment ASC, assumed to be normally distributed, i.e. for coefficient \(m\), \(\beta_{imk}\sim N\left( {\mu_{mk} ,\sigma_{m}^{2} } \right)\). Both normally and log-normally distributed parameters are common assumptions [49]. The former was chosen as normal distributions allow the possibility of a parameter having no influence of average preferences, which was considered a plausible possibility. The influence of scenarios is captured by letting (Eq. 3):
where the dummy variables \(t_{k}^{{{\text{conceive}}}}\) and \(t_{k}^{{{\text{pregnant}}}}\) take the value 1, either if choice situation \(k\) is in the trying to conceive/pregnant scenario or if \(i\) indicated the participant was currently trying to conceive/pregnant, otherwise take the value 0. The term \(\mu_{m}^{now}\) gives the parameter mean in the now scenario, and the terms \(\mu_{m}^{{{\text{conceive}}}}\) and \(\mu_{m}^{{{\text{pregnant}}}}\) show how the parameter mean changes in the trying to conceive and pregnant scenarios. An analogous expression describes how the standard deviation of parameters varied across scenarios. For participants who reported they were trying to conceive/pregnant, preferences were assumed to be identical in the conceive/pregnant scenario and the now scenario.
The model above was designed to maximise the chances of seeing if differences in preferences across scenarios were statistically significant. However, comparing the magnitudes of model parameters in different scenarios may result in problems, as changes may be due to a shift in response scale rather than different preferences [50]. The influence of the response scale can be eliminated by choosing one parameter as a numeraire, and the magnitude of other parameters compared with it. Here, problems with pregnancyFootnote 3 was chosen as the numeraire, so that other attributes were expressed in terms of the maximum acceptable risk (MAR) of problems with pregnancy.
The utility to person \(i\) of choosing treatment \(j\) in choice situation \(k\) was modelled as shown in Eq. 4:
where \(r_{jk}\) is the risk of problems with pregnancy for \(j\), \(\lambda_{i}\) represents \(i\)’s preferences for risk of problems with pregnancy, \({\varvec{\alpha}}_{ik}\) is a vector representing the participant’s preferences for other attributes and \(\eta_{ijk}\) is an error term. This may be rearranged to give (Eq. 5):
where \({\varvec{\gamma}}_{ik} = {\raise0.7ex\hbox{${{\varvec{\alpha}}_{{{ik}}} }$} \!\mathord{\left/ {\vphantom {{{\varvec{\alpha}}_{{{\varvec{ik}}}} } {\lambda_{i} }}}\right.\kern-\nulldelimiterspace} \!\lower0.7ex\hbox{${\lambda_{i} }$}}\) gives \(i\)’s MAR of problems with pregnancy to receive an extra unit of other attributes. This formulation is analogous to models estimated in willingness-to-pay space [53, 54] and has the advantage that a distribution can be directly assumed for MAR. Calculating MAR from the results of the previous model would require taking the ratio of two normal distributions, which has undefined moments.
The influence of different scenarios was captured by letting \({\varvec{\gamma}}_{ik} = \mathop \sum \limits_{s} {\varvec{\gamma}}_{i}^{s} t_{k}^{s}\), \(s \in \left\{ {\text{now, conceive, pregnant}} \right\}\), therefore, in contrast to the previous model, coefficients in the conceive and pregnant scenarios were not interaction terms. The parameter \(\lambda_{i}\) was modelled as following a log-normal distribution, and the \(\gamma_{i}^{s}\)’s were modelled as following normal distributions. Means were allowed to vary over scenarios (with the exception of \(\lambda_{i}\) to ensure the model was identified) but variances were not, as it was not possible to robustly estimate a model without this restriction.
Models were estimated using the Apollo choice modelling package for R [55]. Statistical significance of model coefficients was assessed using t-tests and was judged at the 5% level.
3 Results
Invitations to take part were sent to approximately 1500 people. A total of 675 of 845 (80%) participants who completed the survey reported being female. Of these, 61 indicated they (or their partner) were considering having a child, either in the present or in the future. A total of 60 completed the reproduction DCE. Of these, 14 were currently trying to conceive, and none reported currently being pregnant. Table 2 summarises participants’ demographics and their experiences with DMTs.
Most participants had been living with MS for some years (median 4 years) and almost 90% had experience of taking a DMT at some point. As few participants were treatment-naïve, the DCE tasks of choosing between DMTs were relevant to them. Around one-quarter of participants reported having a child/children in their household, therefore many will also have had previous experience of pregnancy.
In the now scenario, no treatment was chosen 12.6% of the time, which rose to 37.6% in the trying to conceive scenario and 60.3% in the pregnant scenario.Footnote 4 A Kruskal–Wallis test confirmed the differences across scenarios were statistically significant (p < 0.001).
The results of model estimation are given in Table 3. In the now scenario, participants were significantly more likely to choose treatments giving fewer relapses, a lower probability of progression and without severe side effects. Daily pills were the most preferred mode of administration, although the difference in preference between two infusions a year apart and a daily pill was not significant. Injections and monthly infusions were significantly less popular than pills. Participants preferred treatments with a lower chance of problems with pregnancy. There were indications that participants preferred treatments with shorter washout times (i.e. a shorter time for the treatment to leave their system once they stop treatment) and which were safe to take while breastfeeding, as the means of those parameters were negative. However, neither was statistically significant. They were also significantly more likely to choose treatments with a lower chance of problems with pregnancy and which were safe to take while breastfeeding. The mean no treatment ASC (which captured preferences for taking no treatment not explicitly captured by the attributes) was negative, indicating a preference for taking a DMT over and above the properties captured by the attributes, but not significant.
The coefficients for the trying to conceive and pregnant scenarios are interaction terms, and represent changes in preferences relative to the now scenario. There were seven significant interactions for the trying to conceive scenario. For number of relapses, probability of progression, moderate and severe side effects, injections and monthly infusions, the interactions reduced the absolute magnitude of the parameter, indicating a lesser importance in decision making. The interaction for the washout period increased the absolute magnitude of the parameter, indicating greater importance in decision making compared with the now scenario (Table 3).
There were six significant interactions in the pregnant scenario. Five interactions reduced the absolute magnitude of the parameter, meaning lower importance in decision making: number of relapses, chance of progression, moderate and severe side effects, and monthly infusions. The interaction for the no treatment ASC was positive and sufficiently large to increase the absolute magnitude of the parameter. This implies that the differences between no treatment and treatment not explicitly captured by the attributes had greater importance in decision making compared with the now scenario, and that in the pregnant scenario, participants preferred no treatment.
Table 4 reports the results of the model in MAR space. To aid comparison between scenarios, the results are illustrated in Fig. 3. Unlike Table 3, the figure shows absolute preferences for the trying to conceive and pregnant scenarios, not changes relative to the now scenario, and preferences in different scenarios may be compared as they are measured in terms of the MAR of problems with pregnancy. The MAR of problems with pregnancy was lower in the trying to conceive and pregnant scenarios than in the now scenario for reducing the number of relapses, lowering the chance of progression, and avoiding moderate and severe side effects. There was also a lower MAR of problems with pregnancy to obtain a daily pill rather than an injection or a monthly infusion. There was little difference in the MAR for the above attributes between the trying to conceive and pregnant scenarios. The MAR was similar across scenarios for a shorter washout period and having a treatment that is safe to take while breastfeeding. The greatest changes across scenarios were seen for the no treatment ASC. Participants had a MAR of problems with pregnancy of 33.7% in the now scenario, which reduced to 19.0% in the trying to conceive scenario and − 14.7% in the pregnant scenario, with the negative sign implying a preference for no treatment over treatment.

Maximum acceptable risks of problems with pregnancy for other attributes. Error bars show 95% confidence intervals
4 Discussion
Considering the now scenario and the non-pregnancy-related attributes, results are as expected and in line with previous DCE findings (e.g. Bottomley et al. [39] and Johnson et al. [40]). Participants were more likely to choose treatments that reduced the number of relapses experienced and the probability of future loss of function, with less severe adverse effects. As has been previously observed [56,57,58,59], participants preferred a daily pill over other modes of administration. The daily pill may fit better into participants’ daily lives, despite its increased frequency compared with other modes of administration. This notion is in accordance with findings from the qualitative data gathered during attribute development suggesting that pills were easier to incorporate into a normal routine; for example, taking them alongside vitamins [60]. The similarities between previous studies that recruited from the population of all people with RRMS and this study, which elicited the views of wwRRMS considering pregnancy, suggests there are few fundamental differences between the two populations in attitudes towards the non-pregnancy-specific attributes of DMTs.
In the now scenario, even when not actively trying to conceive, the risk of problems with pregnancy influenced participants’ choices. Two possible explanations for this finding are, first, participants may have recognised the possibility of an unplanned pregnancy, given that the rate of unplanned pregnancies has been estimated to be as high as 50% [61], leading them to choose pregnancy-friendly treatments in case of this eventuality. Corroboration for this was found in the qualitative attribute development work, where some interview participants identified unplanned pregnancy as a worry about taking DMTs [35, 60]. Alternatively, participants may have wished to avoid the disruption associated with switching or stopping treatment and to choose a DMT that they would be happy to continue taking when trying to conceive or when pregnant. Both explanations have the underlying rationale of the safety of a potential foetus and are not mutually exclusive.
Participants’ preferences varied according to scenario type. There was a dramatic increase in the number of times no treatment was the most preferred option, from just over 10% in the now scenario, to just under 40% when trying to conceive, to around 60% when pregnant. A large driver of this change was interactions with the no treatment ASC, which had the largest relative magnitude in both the trying to conceive and pregnant scenarios. The ASC captured general preferences for no treatment over any DMT not captured by preferences for the attributes, therefore the interactions can be interpreted as participants being more reluctant to take any sort of treatment while pregnant, irrespective of the particular properties of the treatment. The above results are in line with previous findings that many women cease taking DMTs when trying to conceive or when pregnant, with the aim of resuming treatment at some point after childbirth.
The shift in preferences towards no treatment was also driven by the relatively lower importance of the non-reproduction-specific attributes of treatments. In both the trying to conceive and pregnant scenarios, number of relapses, chance of future progression, adverse effect severity and having a preferred mode of administration became relatively less important. This may indicate that when participants began actively trying to conceive, they would change the trade-offs they would make between their own current/future health and risks to a foetus. It also suggests that in those scenarios, participants were more willing to take treatments that are less convenient and more disruptive to their lifestyle as long as they experience a safer pregnancy; however, these trade-offs appear to be stable between the trying to conceive and pregnant scenarios.
In Table 3, the interactions for the chance of problems with pregnancy were insignificant in both the trying to conceive and pregnant scenarios. However, Fig. 3 reveals that what individuals considered an acceptable risk of problems with pregnancy for beneficial attributes of treatments changes across scenarios, in line with the patterns discussed above.
The term ‘problems with pregnancy’ encompasses several conditions with varying severity, such as low birth weight and congenital abnormalities. Hence, different participants may have had different perceptions of how severe problems may be. A single attribute was used partly to ensure the number of attributes was not so large as to overburden participants and partly because in pretesting participants showed an aversion to terms such as congenital abnormalities. Future research could elicit more details about preferences and trade-offs between the specific risks of DMTs.
Participants had similar relative preferences for different modes of administration across all scenarios. Nonetheless, Fig. 3 shows that the MARs of problems with pregnancy were reduced by similar amounts in the trying to conceive and pregnant scenarios. This may suggest that in those scenarios, participants were more willing to take treatments that are less convenient and more disruptive to their lifestyle as long as they experience a safer pregnancy.
The results for the washout period can also be interpreted in line with a behavioural pattern of not wanting to take a DMT when pregnant. Participants were most likely to choose treatments with shorter washout periods in the trying to conceive scenario, which could indicate that if they were willing to take a DMT in this period, they would place a premium on being able to stop as soon as possible when they became pregnant.
This study has some innovative features. This was the first stated preference study to examine the reproduction-related attributes of DMTs in detail. It was also the first to focus on wwRRMS who may consider having a child, the population for whom reproductive issues are most pertinent.
Another innovative feature of this study is that it reflected the dynamic nature of DMT decision making, especially when considering pregnancy, by asking participants to imagine completing the DCE tasks in multiple scenarios. The feasibility of such a design has been demonstrated here—results were logical and in line with expectations and previous results. Participants responded to the different scenarios, changing their behaviour both in regard to the relative importance of DMT attributes and whether to take a DMT or not.
This study also has limitations. Scenarios were presented in the same order in each task (i.e. now, trying to conceive, pregnant). This design was chosen based on pretesting, which identified difficulties in communicating the concept of the task to participants. Presenting the scenarios in their logical order was important to make the tasks understandable to participants; however, this set order implies that order effects may have affected the results to some extent. Future methodological work could usefully investigate the trade-offs between avoiding possible order effects by randomising the order of scenarios and the increased complexity of the tasks for participants.
Choices in the trying to conceive and pregnant scenarios were (for the majority of participants) being made for the future. There is a large body of evidence that individuals’ preferences can be time-inconsistent [58,59,60], and that individuals are generally poor at predicting what their experiences of future health states will be [61]. The current study measures people’s intentions as to what they will choose in the future, which may not correspond to their actual decisions when the time comes. While this is not necessarily a limitation in itself, as studying individuals’ intentions is still important and relevant, there may be a gap between intention and action.
The sample size was small, although many DCEs have smaller sample sizes (e.g. Spinks et al., [62]). Relatively few questions were asked due to the necessity of minimising respondent burden after already having answered several DCE questions. This means there may be significant differences across scenarios which the DCE does not have sufficient power to detect.
Another drawback to the low sample size was that it was difficult to explore heterogeneity. People were invited to complete the DCE if they reported they were “considering having a child, either now or in the next few years”. Respondents who answered yes may have had various underlying reasons for doing so, ranging from currently trying to conceive, to a general aspiration to have a child at some point in the future. The choice situations may hence have had differing relevance for participants. Although mixed logit models were used to account for heterogeneity, it is difficult to know why preferences differed across respondents. Future research could usefully explore potential sources of preference heterogeneity, such as previous experience of pregnancy, disease severity, or when an individual is planning to have a child in the future.
The small sample size indicates that the population of wwRRMS who are considering pregnancy is both relatively small and/or relatively difficult to engage; however, this does not imply that issues relating to reproduction and DMTs are unimportant. Newly diagnosed wwRRMS are typically aged in their 20 s, and the number for whom reproduction-related attributes of DMTs are relevant at any given time point is lower than the number for whom they were/will be important at some point in their lives. Women who have not yet received an RRMS diagnosis, who have children and do not wish for more, who are no longer able to have children, or whose disease has become progressive, may not have found the DCE tasks meaningful to complete, yet each group would find them meaningful at some time.
Another weakness of this study was that it was performed as an addition to another DCE. A consequence of this is that although, in line with best practice [42, 43], qualitative methods were used to develop the survey instrument, some qualitative participants were not part of the target population of this DCE. It is also not possible to know how many were part of the target population, since the inclusion criteria for this DCE emerged relatively late in the study. On the other hand, the fact that the relationship between reproduction and DMTs was an important, complex and time-sensitive topic to investigate was only revealed due to the extensive qualitative process used to develop the survey instrument, which could be regarded as a strength of the research project. In addition, as attributes and levels draw upon a large amount of qualitative data, there is a greater certainty than in many MS stated preference studies [34] that they were relevant to participants, were understandable, and were interpreted by participants in the way researchers intended.
The sample was self-selected from an online panel used to regularly completing surveys related to their disease, and may not be representative of the wider population of wwRRMS who were considering having a child in future. In addition, it is a limitation that some participants may not have found the included reproduction attributes relevant if, for example, they were planning to adopt.
There is opportunity for further work in this area. For example, future studies could explore heterogeneity of preferences, as decisions around reproduction are extremely personal. It would be instructive to investigate whether wwRRMS who are not currently considering having a child in future also consider reproduction-related factors in DMT decision making. Given the difficulties of recruiting wwRRMS who were considering having a child, future studies could consider eliciting the preferences of wwRRMS who have previously had children. One drawback of that approach is that their preferences may be affected by recall bias [63]. Future studies may wish to study the preferences for men as well as women. Reproduction-related issues also affect men’s DMT choices [64], and it is difficult to know to what extent the findings for women would be replicated with men. However, this project highlighted challenges in recruiting sufficient numbers of men.
More generally, this study has demonstrated that reproduction-specific attributes of non-reproduction treatments can have great importance to individuals. Many treatments for conditions other than RRMS, such as antidepressants, seizure medication and steroids, can have risks for a foetus if taken during pregnancy [7, 65]; however, the impact of reproduction-related risks of treatments is often neglected in the DCE literature. Some research has been carried out into preferences for reproduction-specific treatments such as in vitro fertilisation [66,67,68], obstetric care [69], perinatal depression [70], and smoking cessation during pregnancy [71]; however, these do not involve trade-offs between treatment benefits and reproduction risks. Several studies on prenatal testing [72,73,74,75] elicit trade-offs between the beneficial aspects of tests and risks to the foetus. Future DCEs looking at preferences for treatments with reproduction-related risks may wish to use an approach similar to the current study to examine the importance of such risks in patients’ decision making.
5 Conclusion
The results of this study indicate that wwRRMS considering having a child in the future have preferences for reproduction-related attributes of DMTs, even when not actively trying to conceive. They also indicate that DMT decision making in relation to reproduction is complex and depends heavily on context. The findings from this study and the wider research project have been used as evidence to inform the content and structure of a patient decision aid for people making decisions about starting, switching and stopping treatment with DMTs for RRMS [37]. This study demonstrates that using multiple scenarios in a DCE is feasible and understandable by survey participants, and can improve the insight a study gives into complex decision-making situations in which participants’ preferences may change over time. Future DCEs may wish to consider adopting a similar approach.
Data Availability Statement
Data are not publicly available as consent was not obtained from participants, however, data may be shared on a case-by-case basis if a formal data sharing agreement is entered into, by contacting either the corresponding author or the Leeds Institute of Health Sciences.
Notes
The two attributes were relapse severity and chance of additional long-term and/or life-threatening medical condition over 4 years.
ChoiceMetrics.
Participants who were currently trying to conceive and who were making choices in the now scenario were modelled as being in the trying to conceive scenario.
References
Reich DS, Lucchinetti CF, Calabresi PA. Multiple sclerosis. N Engl J Med. 2018;378:169–80.
Thompson AJ, Banwell BL, Barkhof F, Carroll WM, Coetzee T, Comi G, et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 2018;17:162–73.
Bove RM, Hauser SL. Diagnosing multiple sclerosis: art and science. Lancet Neurol. 2018;17:109–11.
Wallin MT, Culpepper WJ, Nichols E, Bhutta ZA, Gebrehiwot TT, Hay SI, et al. Global, regional, and national burden of multiple sclerosis 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019;18:269–85.
Kingwell E, Marriott JJ, Jetté N, Pringsheim T, Makhani N, Morrow SA, et al. Incidence and prevalence of multiple sclerosis in Europe: a systematic review. BMC Neurol. 2013;13:128.
World Health Organization. Atlas: multiple sclerosis resources in the world 2008. Geneva: World Health Organization; 2008.
Brownlee WJ, Hardy TA, Fazekas F, Miller DH. Diagnosis of multiple sclerosis: progress and challenges. Lancet. 2017;389:1336–46.
Comi G, Radaelli M, Soelberg Sørensen P. Evolving concepts in the treatment of relapsing multiple sclerosis. Lancet. 2017;389:1347–56.
Castro-Borrero W, Graves D, Frohman TC, Flores AB, Hardeman P, Logan D, et al. Current and emerging therapies in multiple sclerosis: a systematic review. Ther Adv Neurol Disord. 2012;5:205–20.
Rae-Grant A, Day GS, Marrie RA, Rabinstein A, Cree BA, Gronseth GS, et al. Comprehensive systematic review summary: disease-modifying therapies for adults with multiple sclerosis: report of the guideline development, dissemination, and implementation subcommittee of the American Academy of Neurology. Neurology. 2018;90:789–800.
Torkildsen Ø, Myhr KM, Bø L. Disease-modifying treatments for multiple sclerosis: a review of approved medications. Eur J Neurol. 2016;23:18–27.
Eskyte I, Manzano A, Pepper G, Pavitt S, Ford H, Bekker H, et al. Understanding treatment decisions from the perspective of people with relapsing remitting multiple sclerosis: a critical interpretive synthesis. Mult Scler Relat Disord. 2019;27:370–7.
Coyle PK. Management of women with multiple sclerosis through pregnancy and after childbirth. Ther Adv Neurol Disord. 2016;9:198–21010.
Payne D, McPherson KM. Becoming mothers. Multiple sclerosis and motherhood: a qualitative study. Disabil Rehabil. 2010;32:629–38.
Sandberg-Wollheim M, Neudorfer O, Grinspan A, Weinstock-Guttman B, Haas J, Izquierdo G, et al. Pregnancy outcomes from the branded glatiramer acetate pregnancy database. Int J MS Care. 2018;20:9–14.
Lu E, Wang BW, Guimond C, Synnes A, Sadovnick D, Tremlett H. Disease-modifying drugs for multiple sclerosis in pregnancy: a systematic review. Neurology. 2012;79:1130–5.
Coyle PK, Sinclair S, Scheuerle A, Thorp J, Albano J, Rametta M. Final results from the Betaseron (interferon β-1b) Pregnancy Registry: a prospective observational study of birth defects and pregnancy-related adverse events. BMJ Open. 2014;4:e004536.
Fares J, Nassar AH, Gebeily S, Kobeissy F, Fares Y. Pregnancy outcomes in Lebanese women with multiple sclerosis (the LeMS study): a prospective multicentre study. BMJ Open. 2016;6:e011210.
Alroughani R, Altintas A, Al Jumah M, Sahraian M, Alsharoqi I, Al Tahan A, et al. Pregnancy and the use of disease-modifying therapies in patients with multiple sclerosis: benefits versus risks. Mult Scler Int. 2016;2016:1034912.
Dobson R, Dassan P, Roberts M, Giovannoni G, Nelson-Piercy C, Brex PA. UK consensus on pregnancy in multiple sclerosis: ‘Association of British Neurologists’ guidelines. Pract Neurol. 2019;19:106–14.
Hughes SE, Spelman T, Gray OM, Boz C, Trojano M, Lugaresi A, et al. Predictors and dynamics of postpartum relapses in women with multiple sclerosis. Mult Scler J. 2014;20:739–46.
Confavreux C, Hutchinson M, Hours MM, Cortinovis-Tourniaire P, Moreau T. Pregnancy in Multiple Sclerosis Group. Rate of pregnancy-related relapse in multiple sclerosis. N Engl J Med. 1998;339:285–91.
AL Phillips, MK Houtchens, NC Edwards. Multiple sclerosis relapse rates, before, during, and after pregnancy: a US retrospective claims database analysis (P1. 361). Neurology. 2017;88(16 Suppl).
Vukusic S, Marignier R. Multiple sclerosis and pregnancy in the'treatment era'. Nat Rev Neurol. 2015;11:280.
Langer-Gould A, Smith JB, Albers KB, Xiang AH, Wu J, Kerezsi EH, et al. Pregnancy-related relapses and breastfeeding in a contemporary multiple sclerosis cohort. Neurology. 2020;94:e1939–e19491949.
Pakenham KI, Tilling J, Cretchley J. Parenting difficulties and resources: the perspectives of parents with multiple sclerosis and their partners. Rehabil Psychol. 2012;57:52.
Kosmala-Anderson J, Wallace LM. A qualitative study of the childbearing experience of women living with multiple sclerosis. Disabil Rehabil. 2013;35:976–81.
Wundes A, Pebdani RN, Amtmann D. What do healthcare providers advise women with multiple sclerosis regarding pregnancy? Mult Scler Int. 2014;2014:819216.
Borisow N, Döring A, Pfueller CF, Paul F, Dörr J, Hellwig K. Expert recommendations to personalization of medical approaches in treatment of multiple sclerosis: an overview of family planning and pregnancy. EPMA J. 2012;3:9.
Borisow N, Paul F, Ohlraun S, Pach D, Fischer F, Dörr J. Pregnancy in multiple sclerosis: a questionnaire study. PLoS ONE. 2014;9:e99106.
Lee M, O’Brien P. Pregnancy and multiple sclerosis. J Neurol Neurosurg Psychiatry. 2008;79:1308–11.
Soekhai V, de Bekker-Grob EW, Ellis AR, Vass CM. Discrete choice experiments in health economics: past, present and future. PharmacoEconomics. 2019;37:201–26.
Clark MD, Determann D, Petrou S, Moro D, de Bekker-Grob EW. Discrete choice experiments in health economics: a review of the literature. PharmacoEconomics. 2014;32:883–902.
Webb EJ, Meads D, Eskyte I, King N, Dracup N, Chataway J, et al. A systematic review of discrete-choice experiments and conjoint analysis studies in people with multiple sclerosis. Patient. 2018;11:391–402.
Manzano A, Eskytė I, Ford HL, Bekker H, Potrata B, Chataway J, et al. Impact of communication on first treatment decisions in people with relapsing-remitting multiple sclerosis. Patient Educ Couns. 2020. https://doi.org/10.1016/j.pec.2020.05.014.
Sepucha KR, Abhyankar P, Hoffman AS, Bekker HL, LeBlanc A, Levin CA, et al. Standards for UNiversal reporting of patient Decision Aid Evaluation studies: the development of SUNDAE Checklist. BMJ Qual Saf. 2018;27:380–8.
A Manzano, HL Ford, B Potrata, I Eskyte, D Meads, E Webb, et al. Treatment Decision Making and Relapsing Remitting Multiple Sclerosis. The CRIMSON Project Decision Aid Booklet. Leeds: University of Leeds; 2019. Available at: https://crimson.leeds.ac.uk/wp-content/uploads/sites/51/2019/12/UOL169_CRIMSON-A4-Brochure_WEB.pdf.
Poulos C, Kinter E, van Beek J, Christensen K, Posner J. Preferences of patients with multiple sclerosis for attributes of injectable multiple sclerosis treatments in the United Kingdom and France. Int J Technol Assess Health Care. 2018;34:425–33.
Bottomley C, Lloyd A, Bennett G, Adlard N. A discrete choice experiment to determine UK patient preference for attributes of disease modifying treatments in Multiple Sclerosis. J Med Econ. 2017;20:863–70.
Johnson FR, Van Houtven G, Ozdemir S, Hass S, White J, Francis G, et al. Multiple sclerosis patients' benefit-risk preferences: serious adverse event risks versus treatment efficacy. J Neurol. 2009;256:554–62.
Wicks P, Brandes D, Park J, Liakhovitski D, Koudinova T, Sasane R. Preferred features of oral treatments and predictors of non-adherence: two web-based choice experiments in multiple sclerosis patients. Interact J Med Res. 2015;4:e6.
Coast J, Al-Janabi H, Sutton EJ, Horrocks SA, Vosper AJ, Swancutt DR, et al. Using qualitative methods for attribute development for discrete choice experiments: issues and recommendations. Health Econ. 2012;21:730–41.
Kløjgaard ME, Bech M, Søgaard R. Designing a stated choice experiment: the value of a qualitative process. J Choice Model. 2012;5:1–18.
Janssen EM, Segal JB, Bridges JFP. A framework for instrument development of a choice experiment: an application to type 2 diabetes. Patient. 2016;9:465–79.
Bridges JF, Hauber AB, Marshall D, Lloyd A, Prosser LA, Regier DA, et al. Conjoint analysis applications in health—a checklist: a report of the ISPOR Good Research Practices for Conjoint Analysis Task Force. Value Health. 2011;14:403–13.
Hollin IL, Craig BM, Coast J, Beusterien K, Vass C, DiSantostefano R, et al. Reporting formative qualitative research to support the development of quantitative preference study protocols and corresponding survey instruments: guidelines for authors and reviewers. Patient. 2020;13:121–36.
Trevena LJ, Zikmund-Fisher BJ, Edwards A, Gaissmaier W, Galesic M, Han PK, et al. Presenting quantitative information about decision outcomes: a risk communication primer for patient decision aid developers. BMC Med Inform Decis Mak. 2013;13:S7.
Zipkin DA, Umscheid CA, Keating NL, Allen E, Aung K, Beyth R, et al. Evidence-based risk communication: a systematic review. Ann Intern Med. 2014;161:270–80.
Lancsar E, Fiebig DG, Hole AR. Discrete choice experiments: a guide to model specification, estimation and software. Pharmacoeconomics. 2017;35:697–716.
Hess S, Rose JM. Can scale and coefficient heterogeneity be separated in random coefficients models? Transportation. 2012;39:1225–399.
Amato M, Portaccio E, Ghezzi A, Hakiki B, Zipoli V, Martinelli V, et al. Pregnancy and fetal outcomes after interferon-β exposure in multiple sclerosis. Neurology. 2010;75:1794–802.
Boskovic R, Wide R, Wolpin J, Bauer D, Koren G. The reproductive effects of beta interferon therapy in pregnancy: a longitudinal cohort. Neurology. 2005;65:807–11.
Train K, Weeks M. Discrete choice models in preference space and willingness-to-pay space. In: Scarpa R, Alberini A, editors. Applications of simulation methods in environmental and resource economics. Springer; 2005. p. 1–16.
Hole AR, Kolstad JR. Mixed logit estimation of willingness to pay distributions: a comparison of models in preference and WTP space using data from a health-related choice experiment. Empir Econ. 2012;42:445–69.
Hess S, Palma D. Apollo: a flexible, powerful and customisable freeware package for choice model estimation and application. J Choice Model. 2019;32:100170.
Garcia-Dominguez JM, Munoz D, Comellas M, Gonzalbo I, Lizan L, Polanco Sanchez C. Patient preferences for treatment of multiple sclerosis with disease-modifying therapies: a discrete choice experiment. Patient Prefer Adherence. 2016;10:1945–56.
Lynd LD, Traboulsee A, Marra CA, Mittmann N, Evans C, Li KH, et al. Quantitative analysis of multiple sclerosis patients' preferences for drug treatment: a best-worst scaling study. Ther Adv Neurol Disord. 2016;9:287–96.
Wilson LS, Loucks A, Gipson G, Zhong L, Bui C, Miller E, et al. Patient preferences for attributes of multiple sclerosis disease-modifying therapies: development and results of a ratings-based conjoint analysis. Int J MS Care. 2015;17:74–82.
Wilson L, Loucks A, Bui C, Gipson G, Zhong L, Schwartzburg A, et al. Patient centered decision making: use of conjoint analysis to determine risk-benefit trade-offs for preference sensitive treatment choices. J Neurol Sci. 2014;344:80–7.
A Manzano, HL Ford, G Pepper, J Chataway, K Schmierer, D Meads, et al. CRIMSON—Considering Risk and benefits In Multiple Sclerosis treatment selectiON. 2019.
Henshaw SK. Unintended pregnancy in the United States. Fam Plann Perspect. 1998;30(24–9):46.
Spinks J, Janda M, Soyer HP, Whitty JA. Consumer preferences for teledermoscopy screening to detect melanoma early. J Telemed Telecare. 2016;22:39–46.
Schmier JK, Halpern MT. Patient recall and recall bias of health state and health status. Expert Rev Pharmacoecon Outcomes Res. 2004;4:159–63.
Pecori C, Giannini M, Portaccio E, Ghezzi A, Hakiki B, Pastò L, et al. Paternal therapy with disease modifying drugs in multiple sclerosis and pregnancy outcomes: a prospective observational multicentric study. BMC Neurol. 2014;14:114.
Hardy JR, Leaderer BP, Holford TR, Hall GC, Bracken MB. Safety of medications prescribed before and during early pregnancy in a cohort of 81,975 mothers from the UK General Practice Research Database. Pharmacoepidemiol Drug Saf. 2006;15:555–64.
Van Den Wijngaard L, Van Wely M, Dancet EA, Van Mello NM, Koks CA, Van Der Veen F, et al. Patients' preferences for gonadotrophin-releasing hormone analogs in in vitro fertilization. Gynecol Obstetr Investig. 2014;78:16–211.
Landfeldt E, Jablonowska B, Norlander E, Persdotter-Eberg K, Thurin-Kjellberg A, Wramsby M, et al. Patient preferences for characteristics differentiating ovarian stimulation treatments. Hum Reprod. 2012;27:760–9.
van Empel IW, Dancet EA, Koolman XH, Nelen WL, Stolk EA, Sermeus W, et al. Physicians underestimate the importance of patient-centredness to patients: a discrete choice experiment in fertility care. Hum Reprod. 2011;26:584–93.
Pavlova M, Hendrix M, Nouwens E, Nijhuis J, van Merode G. The choice of obstetric care by low-risk pregnant women in the Netherlands: implications for policy and management. Health Policy. 2009;93:27–34.
Ride J, Lancsar E. Women’s preferences for treatment of perinatal depression and anxiety: a discrete choice experiment. PLoS ONE. 2016;11:e0156629.
Morgan H, Hoddinott P, Thomson G, Crossland N, Farrar S, Yi D, et al. Benefits of Incentives for Breastfeeding and Smoking cessation in pregnancy (BIBS): a mixed-methods study to inform trial design. Health Technol Assess. 2015;19:1–522, vii–viii.
Beulen L, Grutters JP, Faas BH, Feenstra I, Groenewoud H, van Vugt JM, et al. Women's and healthcare professionals' preferences for prenatal testing: a discrete choice experiment. Prenat Diagn. 2015;35:549–57.
Carroll FE, Al-Janabi H, Flynn T, Montgomery AA. Women and their partners' preferences for Down's syndrome screening tests: a discrete choice experiment. Prenat Diagn. 2013;33:449–56.
Hill M, Fisher J, Chitty LS, Morris S. Women’s and health professionals’ preferences for prenatal tests for Down syndrome: a discrete choice experiment to contrast noninvasive prenatal diagnosis with current invasive tests. Genet Med. 2012;14:905–13.
Chan YM, Sahota DS, Leung TY, Choy KW, Chan OK, Lau TK. Chinese women's preferences for prenatal diagnostic procedure and their willingness to trade between procedures. Prenat Diagn. 2009;29:1270–6.
Author information
Authors and Affiliations
Contributions
All authors conceived the study, defined the study aims and contributed to the survey design. EW and DM collected the data. EW conducted the statistical analysis and wrote the first draft of the manuscript, and all authors contributed to and approved the final version.
Corresponding author
Ethics declarations
Funding
This study was funded by the UK Multiple Sclerosis Society (grant no. 30). The research is supported by the National Institute for Health Research (NIHR) infrastructure at Leeds. The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care. YO acknowledges support from a Population Research Fellowship awarded by Cancer Research UK (reference C57775/A22182). JC is supported in part by the National Institute for Health Research, University College London Hospitals, Biomedical Research Centre, London, UK.
Conflict of interest
Jeremy Chataway has received support from the Efficacy and Mechanism Evaluation Programme and Health Technology Assessment Programme (NIHR); UK Multiple Sclerosis Society and National Multiple Sclerosis Society; and the Rosetrees Trust. In the last 3 years, he has been a local principal investigator for trials in MS funded by Receptos, Novartis and Biogen Idec, and has received an investigator grant from Novartis outside this work. He has taken part in Advisory Boards/consultancy for Roche, Merck, MedDay, Biogen and Celgene. Klaus Schmierer has received consulting fees from Biogen, Merck, Novartis and Roche, and has received payments for lecturing activities from Biogen, Merck, Novartis, Roche and Teva. Hilary L. Bekker provides guidance, based on her academic expertise in medical decision making, to health policy organisations, patient advocacy groups, health professionals and health scientists on research methods and techniques to develop and evaluate patient decision aids and shared decision making interventions. Her time and expenses in attending meetings, carrying out evaluations and collaborating with other projects are remunerated. She does not gain financially from the outcomes or outputs of these collaborations. Helen Ford has received support from the Health Technology Assessment Programme (NIHR) and the UK MS Society. In the past 3 years, Helen Ford has been a local principal investigator for trials in MS funded by Novartis, Roche, and Biogen Idec and has taken part in advisory boards and consultancy for Merck, Teva, Biogen, and Novartis. Edward Webb, David Meads, Ieva Eskytė, George Pepper, Joachim Marti, Yasmina Okan, Sue Pavitt, and Ana Manzano have no conflicts of interest to declare.
Informed consent
All participants gave informed consent before completing the survey, as well as consent to merge their responses with data from the UK MS Register.
Ethics Approval
Approval for this study was given by a National Health Service (NHS) Research Ethics Committee.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Webb, E.J.D., Meads, D., Eskytė, I. et al. The Impact of Reproductive Issues on Preferences of Women with Relapsing Multiple Sclerosis for Disease-Modifying Treatments. Patient 13, 583–597 (2020). https://doi.org/10.1007/s40271-020-00429-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40271-020-00429-4