
Abstract
Background
There is little information available on health-related quality of life in patients with chemotherapy-naïve metastatic castration-resistant prostate cancer. This study aimed to develop a conceptual model that describes patients’ experiences of living with this condition.
Methods
This was a cross-sectional, non-interventional qualitative research study. Sixty-minute semi-structured interviews were conducted with physicians experienced in treating metastatic castration-resistant prostate cancer and with chemotherapy-naïve patients with metastatic castration-resistant prostate cancer. Interviews were audio-recorded and transcripts were analysed to identify the key symptoms and impacts on quality of life. Results were used to expand a previously published conceptual model for non-metastatic castration-resistant prostate cancer.
Results
Three physicians and 19 patients with metastatic castration-resistant prostate cancer were interviewed. Physicians identified several symptoms frequently mentioned by their patients: fatigue, bone pain, anxiety, stress, depression and interference with daily activities. The most salient symptoms emerging from the patient interviews were urinary frequency and urgency, fatigue, pain/stiffness and sexual dysfunction. The most salient impacts were interference with daily activities, frustration, anxiety and sleep problems. Compared with non-metastatic castration-resistant prostate cancer, some symptoms and impacts in metastatic castration-resistant prostate cancer were more common and rated as more disturbing (e.g. fatigue, pain, urinary frequency, interference with daily activities and frustration). New concepts that were added to the non-metastatic castration-resistant prostate cancer model, to more accurately reflect the experiences of patients with metastatic disease, were enlarged breasts, muscle loss/deconditioning, inability to focus/mental slowing, body image perception, interference with work and lack of ambition/motivation.
Conclusions
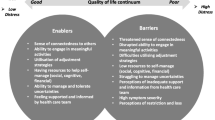
Chemotherapy-naïve patients with metastatic castration-resistant prostate cancer experience a substantial burden from their condition. Furthermore, as castration-resistant prostate cancer progresses from the non-metastatic stage to the early metastatic (pre-chemotherapy) stage, certain symptoms become more common and disturb patients’ lives to a greater extent. The resulting conceptual model for metastatic castration-resistant prostate cancer highlights areas that are not adequately assessed with current patient-reported outcome instruments.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
By highlighting the most salient symptoms and impacts on quality of life, the results of this study can help guide the management of patients with metastatic castration-resistant prostate cancer. |
The study also highlights some of the key changes in symptoms and impacts that may be observed as castration-resistant prostate cancer progresses from the non-metastatic stage to the early metastatic stage. |
1 Introduction
Prostate cancer (PC) is the second most common cancer among men worldwide [1, 2]. It was estimated that in 2012, there were 1.1 million new cases of PC worldwide and that 300,000 men with PC died [3]. Most PC-related deaths occur in patients whose PC has metastasized; 5-year mortality rates were 70% in those with metastatic disease compared with 0% in those with regional or localised PC [4].
Castration-resistant PC (CRPC) refers to a stage of the disease that is no longer controlled by primary androgen-deprivation therapy despite castration testosterone levels (< 50 ng/dL) [5, 6]. Based on the results of studies conducted in USA, Italy and the UK, it is estimated that 10–20% of patients with PC progress to CRPC within 5 years [7]. Most patients have metastatic disease when CRPC is diagnosed; [7] among those who do not, over 50% are expected to develop metastases within 3 years, based on data from a US study [8].
The aim of treating metastatic CRPC (mCRPC) is to delay biochemical progression, extend survival and provide palliation of symptoms. A number of treatments (enzalutamide, abiraterone, radium-223 and cabazitaxel) have been shown to improve overall survival and progression-free survival in patients with mCRPC when used before and/or after docetaxel chemotherapy [9, 10]. The value of any cancer treatment is also determined by patients’ experiences, which can be reflected by evaluating their health-related quality of life (HRQoL). Exploratory analyses using data from patients with mCRPC indicate that there was a significant association between improvement in HRQoL and reduced mortality risk [11].
The importance of assessing patients’ experiences of living with the disease and undergoing treatment is reflected in guidelines from the Prostate Cancer Clinical Trials Working Group [12], the European Medicines Agency [13] and the US Food and Drug Administration [14]. Furthermore, both the European Medicines Agency and the US Food and Drug Administration recommend that patient-reported instruments used in clinical trials should be informed not only by information from clinicians and the published literature but also, most importantly, by direct input from patients with the condition under study [13, 14].
There are a number of PC-specific tools used to assess patients’ experiences of living with PC; these include the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire PR25 [15], the Functional Assessment of Cancer Therapy-Prostate and the Expanded Prostate Cancer Index Composite [16]. However, these questionnaires do not separate symptoms or impacts based on the stage of disease and may not fully capture patients’ perspectives on the most salient symptoms and impacts of later stage PC [17,18,19].
Data on patients’ experiences of living with advanced PC are relatively scarce, but some studies have shown that patients are affected by general cancer-related symptoms such as fatigue and pain, as well as PC-specific symptoms or PC treatment-specific effects on urinary and sexual function [20,21,22]. The aim of the current study was to use a patient-centered approach to develop a conceptual model describing the salient symptoms and impacts of mCRPC in chemotherapy-naïve patients, building on a similar study in those with non-metastatic CRPC (nmCRPC) [23]. Patient and physician interviews were conducted to explore patients’ experiences of living with mCRPC, to determine the language used by patients to describe their condition, and to evaluate the impact of mCRPC on overall patient health and functioning. A conceptual model provides a framework for describing the proximal and distal impacts of a disease on patients [24]. The development of such models is a well-established method for creating or modifying patient-reported outcome instruments [25].
2 Materials and Methods
This cross-sectional, non-interventional qualitative research study was conducted according to the International Society for Pharmacoeconomics and Outcomes Research (ISPOR) Patient-Reported Outcomes Good Research Practices Task Force Report [26]. It comprised three separate stages: (1) physician concept elicitation interviews to provide the clinical expert viewpoint and help shape the semi-structured patient interview guides; (2) patient concept elicitation interviews; and (3) revision of a previously published nmCRPC conceptual model [23] to represent the experience of patients with chemotherapy-naïve mCRPC. The design of the study was based on grounded theory, adapted to incorporate expert opinion and scientific literature. This prior clinical knowledge was used to focus the design and interpretation of the study and is consistent with ISPOR guidelines for concept elicitation research [26].
2.1 Physician Concept Elicitation Interviews
Experts in the field of PC were initially selected based on having been an investigator in > 100 clinical trials, identified using an external database (Citeline SiteTrove). Three genitourinary oncologists, employed by leading academic institutions in USA, were contacted and asked to confirm that they treated patients with PC and were actively involved in research and publication in the field. Following confirmation, they were invited to participate and were interviewed over the telephone by two market research professionals experienced in concept elicitation interviews. Each interview lasted 60 min and was conducted using a semi-structured interview guide that allowed for open-ended questions and probing to expand on the responses provided. During the interview, the physicians were also asked to review a previously published conceptual model developed for patients with nmCRPC [23]. All interviews were recorded and transcribed verbatim and used to add or remove concepts from the nmCRPC conceptual model, to refine the model specifically for mCRPC. The physicians were reimbursed for their time at fair market value.
2.2 Patient Concept Elicitation Interviews
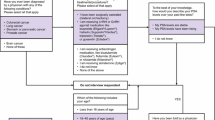
Patients were eligible to participate if they had a diagnosis of mCRPC, were chemotherapy naïve, and had self-reported experience of urinary symptoms, pain, sexual symptoms or hormonal symptoms. Chemotherapy-naïve patients were selected because there is a lack of data on patients’ experiences in this population, and also because the focus of the study was the symptoms and impacts of the disease; once chemotherapy is added, it can be more difficult to distinguish between the impact of the cancer and the side effects of chemotherapy (Fig. 1). Patients were excluded if they were receiving enzalutamide to avoid any perceived bias towards the sponsor’s product.

Screening and recruitment process for identifying and enrolling patients with metastatic castration-resistant prostate cancer. aPatients were excluded if they had received or were currently receiving enzalutamide treatment. LHRH luteinising hormone-releasing hormone, PSA prostate-specific antigen
Patients were identified from users of the HealthUnlocked social network (https://healthunlocked.com/) in USA. HealthUnlocked is the world’s largest social network for health, with over 650,000 members and more than 4.5 million people using the platform each month [27]. It, therefore, provides a valuable source for accessing patients to participate in health-related surveys. Patients join disease-specific forums by choice, although HealthUnlocked do contact patient advocacy groups to encourage patient participation. In the PC forum, pop-up graphics about the survey—produced using Health Graph™ technology (HealthUnlocked, London, UK)—appeared on screen. Patients electing to click on the pop-up graphics were directed to an online eligibility questionnaire. Eligible patients were requested to provide their contact details and online consent to be interviewed. Patients scheduled their interview time online and were contacted by the interviewer at the arranged time.
A discussion guide was developed to standardise the interviews and was tested in two pilot interviews. Sixty-minute semi-structured telephone interviews were conducted in English by the same market research professionals who conducted the physician interviews. Patients were asked a set of open-ended questions and probed to explore their experiences of living with mCRPC. These questions focused on the following topics: history of mCRPC; symptoms due to mCRPC; symptoms due to treatments for mCRPC; impacts of mCRPC on HRQoL; and impacts of mCRPC treatments on HRQoL. Patients were also asked to rate the extent to which the symptoms and impacts disturbed their everyday lives, on a scale of 0 (not at all disturbing) to 10 (extremely disturbing). Again, all interviews were recorded and transcribed verbatim and used to revise the conceptual model. Each patient was compensated for their time upon completion of the interview.
2.3 Collection and Analysis of Data from Patient Interviews
In accordance with industry standard practice, interview responses were analysed with a qualitative research software program (ATLAS.ti 7; ATLAS.ti Scientific Software Development GmbH, Berlin, Germany) in accordance with the ISPOR guidelines [26]. Responses were summarised to determine the frequency (number of mentions) of spontaneous vs. prompted (in response to probing) responses and mean scores for disturbance. Concepts elicited from patients with mCRPC were compared with those obtained during the development of the previously published nmCRPC conceptual model to identify key differences and similarities [23].
2.4 Assessing Concept Saturation
The transcripts of patient interviews were organised chronologically and pooled into groups of approximately five transcripts each. Spontaneously mentioned concepts derived from the second group of interviews were compared with those from the first group to determine if any new concepts were present. The comparison was repeated for all subsequent groups until the point at which saturation was achieved; this was deemed to have occurred when no new spontaneously mentioned concepts were identified from the data [28].
Concepts not mentioned by patients were not included in the final model, even if they were mentioned by physicians. There was no minimum number of mentions applied for inclusion of concepts in the model, but all members of the research team agreed on the concepts to be included.
3 Results
3.1 Physician Concept Elicitation Interviews
The physicians mentioned several symptoms frequently reported by their patients, including urinary symptoms, pain, fatigue, hot flushing and hair loss. After reviewing the previously published conceptual model for nmCRPC, the physicians suggested including a number of additional signs and symptoms associated with treatment [weak (urinary) stream, enlarged breasts, muscle loss/deconditioning, and inability to focus/mental slowing], as well as additional impacts (body image perception, interference with work and lack of ambition/motivation). The physicians indicated that the most important signs and symptoms for patients were fatigue and bone pain, while the most important impacts were anxiety, stress, interference with daily activities and depression, including thoughts of mortality.
3.2 Patient Concept Elicitation Interviews
Forty-three patients completed and passed the eligibility questionnaire and 19 completed the interview process between 4 August, 2016 and 20 March, 2017; the other 24 patients did not complete the consent form, did not schedule their interviews or were not available at the scheduled time. The characteristics of the 19 participating patients are shown in Table 1; patients had a median (range) age of 67 (51–78) years and a median (range) time since diagnosis of metastasis of 4.8 (1.0–13.0) years. Overall, 18 out of 19 patients (95%) were receiving ongoing hormonal therapy; the remaining patient had not received hormonal therapy or undergone an orchiectomy. All patients were English speaking. Concept saturation was achieved as no new concepts were identified in the final set of four interviews.
3.3 Symptom Burden
Patients mentioned over 40 distinct symptoms, which were categorised as PC related, sexual, urinary, hormonal, cognitive and other (e.g. muscular and gastrointestinal symptoms). These are summarised in Fig. 2a, and example patient statements are shown in Table 2.

Frequency and disturbance of a symptom burden and b disease impact on patients with metastatic castration-resistant prostate cancer. GI gastrointestinal
The most common urinary symptoms were frequency of urination [mentioned by 18 patients (95%), n = 11 spontaneously/n = 7 on prompting], urgency to urinate [n = 13 (68%), n = 7 spontaneously/n = 6 on prompting] and leaking [n = 7 (37%), n = 3 spontaneously/n = 4 on prompting]. The most disturbing urinary symptoms were incontinence and inability to urinate/empty bladder; mean (range) disturbance scores were 6.0 (4–7) for both. However, these symptoms were mentioned by only three and two patients, respectively.
The most common hormonal symptoms were hot flushing/night sweats [n = 18 (95%)], hair loss [n = 11 (58%)] and weight gain [n = 9 (47%)]. More patients mentioned hot flushing/night sweats spontaneously (n = 10 vs. n = 8 on prompting), whereas most mentions of hair loss (n = 9) and weight gain (n = 6) were made on prompting. Mean (range) disturbance scores were 4.7 (0–9) for hot flushing/night sweats, 2.5 (0–5) for hair loss and 5.6 (0–9) for weight gain.
The most frequently mentioned PC-related symptoms were fatigue [n = 17 (89%)] and pain/stiffness [n = 14 (74%)] and, in most cases, were mentioned spontaneously. Both of these symptoms were highly disturbing for patients; mean (range) disturbance scores were 6.4 (3–9) and 6.3 (1–10), respectively.
Much of the symptom burden experienced by patients was a result of previous or ongoing treatment for PC. Sexual symptoms (erectile dysfunction, loss of interest in sex, loss of penis length and inability to orgasm) resulting from hormonal therapy and previous radiotherapy and/or prostatectomy scored highly in the frequency of mentions and disturbance ratings. Muscular weakness/loss was identified as a new symptom for mCRPC (i.e. it was not included in the previously published nmCRPC model). It was mentioned by nine patients (47%), and the mean (range) disturbance rating was 6.7 (3–9).
The most salient symptoms of mCRPC (reported by over 50% of patients and with an average disturbance rating of 5 or more out of 10) were urinary frequency and urgency, fatigue, pain/stiffness, erectile dysfunction, loss of interest in sex, inability to orgasm and loss of penis length.
3.4 Patient Functioning and Well-Being
Overall, 21 distinct impacts were mentioned and categorised as emotional, physical/social, functional and other. These are summarised in Fig. 2b, and example patient statements are shown in Table 3.
The most common emotional impacts were depression [mentioned by 13 patients (68%)], frustration [n = 12 (63%)] and anxiety [n = 10 (53%)]. In most cases, depression was reported spontaneously (n = 9 vs. n = 4 on prompting), whereas frustration and anxiety were mentioned more often on prompting (n = 8 vs. n = 4 for frustration and n = 7 vs. n = 3 for anxiety). Frustration was the most disturbing emotional impact, with a mean (range) disturbance rating of 8.1 (3–10); this was related to a lack of treatment options, fatigue, pain or dissatisfaction with the care received from physicians. The most commonly reported physical/social and functional impacts were interference with daily activities [n = 14 (74%), n = 12 spontaneously/n = 2 on prompting] and sleep problems [n = 10 (53%), n = 7 spontaneously/n = 3 on prompting]. Both impacts were associated with high levels of disturbance; mean (range) disturbance ratings were 7.7 (4–10) and 7.3 (5–9), respectively. Effects on patients’ daily activities included a reduction in the ability to work and/or not being able to exercise or perform extracurricular activities (e.g. social, leisure, sports) as a result of fatigue, pain or urinary symptoms. Patients reported sleep problems that were not always a result of thinking about the disease or pain, but having to wake up two or three times a night to urinate (see Table 2 for an example of a patient quotation).
The most salient impacts of mCRPC (reported by over 50% of patients and with an average disturbance rating of 5 or more out of 10) were interference with daily activities, frustration, anxiety and sleep problems. Interestingly, despite the impacts of their disease, many of those interviewed seemed to have come to terms with their disease and were trying to maintain a positive outlook on life (see Table 2 for an example of a patient quotation).
3.5 Comparison of Symptom Concepts Obtained from Patients with Metastatic Castration-Resistant Prostate Cancer vs. Non-Metastatic Castration-Resistant Prostate Cancer
Nine symptoms reported by patients with mCRPC were mentioned more frequently and rated as more disturbing than in the previously published study in patients with nmCRPC; these were pain/stiffness, frequency of urination, fatigue, hot flushing/night sweats, body hair loss, inability to orgasm, diarrhea/gastrointestinal upset, erectile dysfunction and urinary urgency (Fig. 3a). Although more patients with mCRPC described weight gain, they ranked disturbance lower than those with nmCRPC. Conversely, fewer patients with mCRPC described incontinence/leaking issues and loss of interest in sex, but did rank these symptoms as more disturbing than did patients with nmCRPC.

Change in frequency and disturbance of a symptoms and b disease impact concepts in patients with metastatic castration-resistant prostate cancer (n = 19) compared with those with non-metastatic castration-resistant prostate cancer (n = 17). GI gastrointestinal
3.6 Comparison of Disease Impact Concepts Obtained from Patients with Metastatic Castration-Resistant Prostate Cancer vs. Non-Metastatic Castration-Resistant Prostate Cancer
Eight impact concepts were more frequent and were considered more disturbing to patients with mCRPC compared with those from the previously published study in patients with nmCRPC (Fig. 3b). These included both emotional impacts (frustration, embarrassment, loss of feeling of masculinity and anxiety) and physical/functional impacts (interference with daily activities and sleep problems). Treatment dissatisfaction was also mentioned by more patients with mCRPC and was associated with greater disturbance ratings. The greatest difference between mCRPC and nmCRPC, in terms of the number of mentions, was for depression but, interestingly, disturbance ratings were almost two points lower in patients with mCRPC.
3.7 Conceptual Model of the Impact of Metastatic Castration-Resistant Prostate Cancer
A conceptual model describing the symptoms and impacts of mCRPC on chemotherapy-naïve patients was developed (Fig. 4) by revising the previously published nmCRPC model according to the findings elicited from the physician and patient interviews. New concepts that were added to the model included symptoms (enlarged breasts, muscle loss/deconditioning and inability to focus/mental slowing) and impacts (body image perception, interference with work and lack of ambition/motivation). Conversely, low self-esteem, which was part of the nmCRPC model, was not included in the mCRPC model, as it was reported by only three patients. Weak (urinary) stream, which was suggested as an important symptom by physicians, was not included in the mCRPC model as it was not mentioned during the patient interviews. The symptoms of mCRPC interfered with daily activities, including the ability to work, and resulted in anxiety, depression, frustration and sleep problems.

Chemotherapy-naïve metastatic castration-resistant prostate cancer (mCRPC) conceptual model. Conceptual model of the impact of mCRPC adapted from the non-metastatic castration-resistant prostate cancer conceptual model [23] using physician and patient interviews. Concepts in bold text were the most salient to patients. Low self-esteem was removed from the conceptual model as it was not mentioned during the interviews or deemed unimportant. CRPC castration-resistant prostate cancer, GI gastrointestinal
4 Discussion
We developed a conceptual model, based on input from physicians and patients, which synthesizes the disease symptoms and impacts experienced by chemotherapy-naïve patients living with mCRPC. Based on in-depth patient interviews, patients at this stage of PC are experiencing a substantial burden from the condition, reflected by a number of salient symptoms and impacts associated with the disease. Overall, patients mentioned over 40 distinct symptoms associated with the underlying disease and/or previous or ongoing treatments. The extent to which these symptoms affect patients’ everyday lives does vary; however, certain urinary symptoms (frequency and urgency), PC-related symptoms (fatigue and pain/stiffness) and sexual symptoms related to hormone treatment (erectile dysfunction, loss of interest in sex, loss of penis length and inability to orgasm) were highly disturbing for most of the patients interviewed. Similarly, the emotional, physical/social and functional impacts of mCRPC were diverse, but most patients reported that anxiety, frustration, sleep problems and interference with daily activities as a result of fatigue, pain/stiffness or urinary symptoms substantially disturbed their lives. These results were echoed by the findings from the physician interviews, which identified pain, fatigue, urinary symptoms, anxiety and frustration as concepts reported frequently by their patients with mCRPC. In general, symptoms and impacts reported spontaneously by patients had higher disturbance ratings than those reported on prompting, as might be expected; however, it is notable that some (e.g. weight gain and frustration) had high disturbance scores but were mentioned by most patients only after prompting.
By building on data from the previously published nmCRPC conceptual model [23], the current study provides insights into how patients’ symptoms and impacts change when they develop metastatic disease. It adds to data indicating that patients’ experiences continue to deteriorate as CRPC progresses [29, 30] and supports the therapeutic goal of delaying time to metastases in patients with nmCRPC [31]. Comparing the two conceptual models, it is apparent that as patients move from the non-metastatic stage to the early metastatic (pre-chemotherapy) stage, certain symptoms become more common and disturb patients’ lives to a greater extent (e.g. fatigue, pain and urinary frequency) and various aspects of patients’ emotional, physical and functional well-being deteriorate (e.g. interference with daily activities and frustration). Muscle loss also becomes a salient symptom, which was not included in the previously published nmCRPC model as it was mentioned by only one patient [23]. In addition, satisfaction with treatment lessens in mCRPC compared with nmCRPC. Interestingly, almost 40% more patients with mCRPC mentioned depression, but the disturbance rating was almost 20% lower than in patients with nmCRPC. Some patients reflected that they had come to terms with their condition, and the lower disturbance rating for depression may reflect this acceptance.
Results of previous studies evaluating the symptoms and impacts of mCRPC provided results that are generally consistent with the current study. Eton et al. [25] conducted interviews in 15 patients with mCRPC and ten physicians, and identified 16 issues and outcomes that were important to these patients. In keeping with our findings, these included pain, urinary problems, fatigue and erectile dysfunction. Additional items were loss of appetite, constipation, diarrhea, peripheral neuropathy, prostate-specific antigen-related anxiety and changes in self-image, most of which were also reported by at least some patients in the current study. More recently, Sartor et al. [19] developed a conceptual model summarising symptoms and impacts in advanced PC (castration resistant or metastatic), based on physician and patient interviews. Once again, there is considerable overlap between the symptoms and impacts identified in this study and the current study. This includes symptoms that Sartor et al. [19] attribute to hormonal therapy (e.g. sexual dysfunction, loss of muscle, genital atrophy, breast enlargement, hot flushes and inability to concentrate) and the distal impact on manliness and body image. Finally, the Advanced Prostate Cancer Working Group of the International Consortium for Health Outcome Measurement, which comprised healthcare professionals and patient representatives, defined outcomes important to patients with advanced PC, by discussing the published literature on this topic [17]. The final shortlist included items related to pain, fatigue, sexual dysfunction, urinary and bowel symptoms, and physical and emotional functioning.
As discussed, a number of instruments are available and have been used to assess HRQoL in clinical trials in mCRPC. However, even those with a PC component (e.g. European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire PR25 and Functional Assessment of Cancer Therapy-Prostate) were not designed to evaluate specific stages of PC and there may be a focus on issues more relevant to patients treated for localised disease [18, 23]. This limitation of current HRQoL instruments was highlighted by Eton et al. [25], who identified a number of issues and outcomes that were important to patients with mCRPC but were not adequately covered by existing HRQoL questionnaires. Morgans et al. [17] failed to identify a single practical validated tool that adequately covered all of the HRQoL-related symptoms and impacts considered to be important in patients with advanced PC. Our data confirm there is a need for improved tools for assessing this patient population, and the conceptual model developed in the current study could help to facilitate this.
The current study is not without limitations. The semi-structured qualitative interviews were conducted on a relatively small sample of patients. Interviewing more patients might have resulted in a different conceptual model; however, in a study designed to evaluate sample sizes for this type of analysis, as few as 12 interviews were enough to achieve saturation in thematic content, and basic meta-themes were present as early as six interviews [28]. Notably, we achieved concept saturation in the final set of responses to be analysed. Another limitation of this type of study is that the information generated is largely dependent on how openly patients discuss topics and how well each interviewer elicits the information. To facilitate this, interviews were conducted by two market research professionals experienced in concept elicitation interviews, although it is acknowledged that the use of two professionals (rather than one) may have increased variability in the data elicited. Furthermore, the results are specific to patients with chemotherapy-naïve mCRPC. This population was chosen to avoid the potential for confounding effects of chemotherapy on patients’ experiences of living with mCRPC, and to evaluate the impact of the latter, it would be more appropriate to develop a separate model. Finally, all patients were recruited from USA via the Internet and therefore the patient selection process may have introduced bias (e.g. towards younger patients who are more comfortable with technology); the extent to which the subgroup recruited represents the wider mCRPC population outside USA is not clear.
5 Conclusions
We developed a conceptual model that characterises patients’ experiences of living with mCRPC. The model is primarily patient driven and informed by expert PC physicians. Encouragingly, physicians and patients identified similar symptoms and impacts associated with mCRPC. The results show that chemotherapy-naïve patients with mCRPC experience a substantial burden from their condition. Furthermore, as CRPC progresses from the non-metastatic stage to the early metastatic (pre-chemotherapy) stage, certain symptoms become more common and disturb patients’ lives to a greater extent. The resulting conceptual model helps to identify elements of existing patient-reported outcome instruments that are most informative when used in clinical trials of mCRPC, and highlights areas that are not adequately assessed with current instruments. Refining these instruments will ultimately help in the development of interventions that are better designed to support patients and their families.
Data availability
Access to anonymised individual participant-level data will not be provided for this trial as it meets one or more of the exceptions described on http://www.clinicalstudydatarequest.com under “Sponsor Specific Details for Astellas”.
References
Torre LA, Siegel RL, Ward EM, Jemal A. Global cancer incidence and mortality rates and trends: an update. Cancer Epidemiol Biomarkers Prev. 2016;25(1):16–27.
Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424.
Ferlay J, Soerjomataram I, Dikshit R, Eser S, Mathers C, Rebelo M, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136(5):E359–86.
National Cancer Institute. Cancer stat tacts: prostate cancer; 2018. https://seer.cancer.gov/statfacts/html/prost.html. Accessed 4 May 2018.
Anantharaman A, Small EJ. Tackling non-metastatic castration-resistant prostate cancer: special considerations in treatment. Expert Rev Anticancer Ther. 2017;17(7):625–33.
Cornford P, Bellmunt J, Bolla M, Briers E, De Santis M, Gross T, et al. EAU-ESTRO-SIOG guidelines on prostate cancer. Part II: treatment of relapsing, metastatic, and castration-resistant prostate cancer. Eur Urol. 2017;71(4):630–42.
Kirby M, Hirst C, Crawford ED. Characterising the castration-resistant prostate cancer population: a systematic review. Int J Clin Pract. 2011;65(11):1180–92.
Moreira DM, Howard LE, Sourbeer KN, Amarasekara HS, Chow LC, Cockrell DC, et al. Predictors of time to metastasis in castration-resistant prostate cancer. Urology. 2016;96:171–6.
Kapoor A, Wu C, Shayegan B, Rybak AP. Contemporary agents in the management of metastatic castration-resistant prostate cancer. Can Urol Assoc J. 2016;10(11–12):E414–23.
Nuhn P, De Bono JS, Fizazi K, Freedland SJ, Grilli M, Kantoff PW, et al. Update on systemic prostate cancer therapies: management of metastatic castration-resistant prostate cancer in the era of precision oncology. Eur Urol. 2018. https://doi.org/10.1016/j.eururo.2018.03.028.
Beer TM, Miller K, Tombal B, Cella D, Phung Holmstrom S, et al. The association between health-related quality-of-life scores and clinical outcomes in metastatic castration-resistant prostate cancer patients: exploratory analyses of AFFIRM and PREVAIL studies. Eur J Cancer. 2017;87:21–9.
Scher HI, Morris MJ, Stadler WM, Higano C, Basch E, Fizazi K, et al. Trial design and objectives for castration-resistant prostate cancer: updated recommendations from the Prostate Cancer Clinical Trials Working Group 3. J Clin Oncol. 2016;34(12):1402–18.
European Medicines Agency. Reflection Paper on the use of patient reported outcome (PRO) measures in oncology studies; 2014. https://www.ema.europa.eu/documents/scientific-guideline/draft-reflection-paper-use-patient-reported-outcome-pro-measures-oncology-studies_en.pdf. Accessed 7 Nov 2018.
US Department of Health and Human Services, Food and Drug Administration, Center for Drug Evaluation and Research (CDER), Center for Biologics Evaluation and Research (CBER), Center for Devices and Radiological Health (CDRH). Guidance for industry. patient-reported outcomes measures: use in medical product development to support labeling claims; 2009. http://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/UCM193282.pdf. Accessed 27 Jan 2017.
van Andel G, Bottomley A, Fosså SD, Efficace F, Coens C, Guerif S, et al. An international field study of the EORTC QLQ-PR25: a questionnaire for assessing the health-related quality of life of patients with prostate cancer. Eur J Cancer. 2008;44(16):2418–24.
Wei JT, Dunn RL, Litwin MS, Sandler HM, Sanda MG. Development and validation of the expanded prostate cancer index composite (EPIC) for comprehensive assessment of health-related quality of life in men with prostate cancer. Urology. 2000;56(6):899–905.
Morgans AK, van Bommel AC, Stowell C, Abrahm JL, Basch E, Bekelman JE, et al. Development of a standardized set of patient-centered outcomes for advanced prostate cancer: an international effort for a unified approach. Eur Urol. 2015;68(5):891–8.
Nussbaum N, George DJ, Abernethy AP, Dolan CM, Oestreicher N, Flanders S, et al. Patient experience in the treatment of metastatic castration-resistant prostate cancer: state of the science. Prostate Cancer Prostatic Dis. 2016;19(2):111–21.
Sartor O, Flood E, Beusterien K, Park J, Webb I, MacLean D, et al. Health-related quality of life in advanced prostate cancer and its treatments: biochemical failure and metastatic disease populations. Clin Genitourin Cancer. 2015;13(2):101–12.
Drummond FJ, Kinnear H, O’Leary E, Donnelly Gavin A, Sharp L. Long-term health-related quality of life of prostate cancer survivors varies by primary treatment. Results from the PiCTure (Prostate Cancer Treatment, your experience) study. J Cancer Surviv. 2015;9(2):361–72.
Eton DT, Lepore SJ. Prostate cancer and health-related quality of life: a review of the literature. Psychooncology. 2002;11(4):307–26.
Giannakopoulos X, Charalabopoulos K, Charalabopoulos A, Golias C, Peschos D, Sofikitis N. Quality of life survey in patients with advanced prostate cancer. Exp Oncol. 2005;27(1):13–7.
Tomaszewski EL, Moise P, Krupnick RN, Downing J, Meyer M, Naidoo S, et al. Symptoms and impacts in non-metastatic castration-resistant prostate cancer: qualitative study findings. Patient. 2017;10(5):567–78.
Taylor F, Reasner DS, Carson RT, Deal LS, Foley C, Iovin R, et al. Development of a symptom-based patient-reported outcome instrument for functional dyspepsia: a preliminary conceptual model and an evaluation of the adequacy of existing instruments. Patient. 2016;9(5):409–18.
Eton DT, Shevrin DH, Beaumont J, Victorson D, Cella D. Constructing a conceptual framework of patient-reported outcomes for metastatic hormone-refractory prostate cancer. Value Health. 2010;13(5):613–23.
Patrick DL, Burke LB, Gwaltney CJ, Leidy NK, Martin ML, Molsen E, et al. Content validity-establishing and reporting the evidence in newly developed patient-reported outcomes (PRO) instruments for medical product evaluation: ISPOR PRO Good Research Practices Task Force Report. Part 1: eliciting concepts for a new PRO instrument. Value Health. 2011;14(8):967–77.
HealthUnlocked; 2018. https://healthunlocked.com/about. Accessed 16 Oct 2018.
Guest G, Bunce A, Johnson L. How many interviews are enough? An experiment with data saturation and variability. Field Methods. 2006;18(1):59–82.
Merseburger AS, Bellmunt J, Jenkins C, Parker C, Fitzpatrick JM. Perspectives on treatment of metastatic castration-resistant prostate cancer. Oncologist. 2013;18(5):558–67.
Sullivan PW, Mulani PM, Fishman M, Sleep D. Quality of life findings from a multicenter, multinational, observational study of patients with metastatic hormone-refractory prostate cancer. Qual Life Res. 2007;16(4):571–5.
Tombal B. Non-metastatic CRPC and asymptomatic metastatic CRPC: which treatment for which patient? Ann Oncol. 2012;23(Suppl. 10):x251–8.
Acknowledgements
Medical writing assistance was provided by Jonathan Plumb and Nicola French from Bioscript Medical, and editorial assistance was provided by Lauren Smith and Stephanie Rippon from Complete HealthVizion.
Author information
Authors and Affiliations
Contributions
SH, JT, EH and JP contributed to the study design. JT and EH were involved in patient recruitment and data collection. JT, EH, JP and RM provided the data analysis. All authors contributed to the data interpretation. RM was involved in the writing of the manuscript. All of the authors provided critical reviews and approved the final manuscript.
Corresponding author
Ethics declarations
Funding
The study was funded by Astellas. Medical writing and editorial assistance was funded by Astellas Pharma Inc.
Conflict of interest
Stefan Holmstrom is an employee of Astellas. Shevani Naidoo was an employee of Astellas at the time the research was conducted. James Turnbull is an employee of Pfizer and was an employee of IQVIA at the time the research was conducted. Emily Hawryluk and Jean Paty are employees of IQVIA, which received consulting fees from Astellas. Robert Morlock received personal fees from Astellas during the conduct of the research; he has also received personal fees from Abbot Medical Optics, Ironwood and Genentech outside the submitted work.
Ethics approval
The study and all interview materials were reviewed and approved by the New England Independent Review Board (no. 20160817) and conducted in accordance with the Declaration of Helsinki and the regulations of the US Food and Drug Administration.
Consent to participate
All patients provided informed online consent that was verbally confirmed before the start of the interview. As part of the consent procedure, patients agreed that the results could be presented, provided that individual patient data could not be identified.
Rights and permissions
About this article

Cite this article
Holmstrom, S., Naidoo, S., Turnbull, J. et al. Symptoms and Impacts in Metastatic Castration-Resistant Prostate Cancer: Qualitative Findings from Patient and Physician Interviews. Patient 12, 57–67 (2019). https://doi.org/10.1007/s40271-018-0349-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40271-018-0349-x