
Abstract
Avibactam (formerly NXL104, AVE1330A) is a synthetic non-β-lactam, β-lactamase inhibitor that inhibits the activities of Ambler class A and C β-lactamases and some Ambler class D enzymes. This review summarizes the existing data published for ceftazidime-avibactam, including relevant chemistry, mechanisms of action and resistance, microbiology, pharmacokinetics, pharmacodynamics, and efficacy and safety data from animal and human trials. Although not a β-lactam, the chemical structure of avibactam closely resembles portions of the cephem bicyclic ring system, and avibactam has been shown to bond covalently to β-lactamases. Very little is known about the potential for avibactam to select for resistance. The addition of avibactam greatly (4-1024-fold minimum inhibitory concentration [MIC] reduction) improves the activity of ceftazidime versus most species of Enterobacteriaceae depending on the presence or absence of β-lactamase enzyme(s). Against Pseudomonas aeruginosa, the addition of avibactam also improves the activity of ceftazidime (~fourfold MIC reduction). Limited data suggest that the addition of avibactam does not improve the activity of ceftazidime versus Acinetobacter species or most anaerobic bacteria (exceptions: Bacteroides fragilis, Clostridium perfringens, Prevotella spp. and Porphyromonas spp.). The pharmacokinetics of avibactam follow a two-compartment model and do not appear to be altered by the co-administration of ceftazidime. The maximum plasma drug concentration (Cmax) and area under the plasma concentration-time curve (AUC) of avibactam increase linearly with doses ranging from 50 mg to 2,000 mg. The mean volume of distribution and half-life of 22 L (~0.3 L/kg) and ~2 hours, respectively, are similar to ceftazidime. Like ceftazidime, avibactam is primarily renally excreted, and clearance correlates with creatinine clearance. Pharmacodynamic data suggest that ceftazidime-avibactam is rapidly bactericidal versus β-lactamase-producing Gram-negative bacilli that are not inhibited by ceftazidime alone.
Clinical trials to date have reported that ceftazidime-avibactam is as effective as standard carbapenem therapy in complicated intra-abdominal infection and complicated urinary tract infection, including infection caused by cephalosporin-resistant Gram-negative isolates. The safety and tolerability of ceftazidime-avibactam has been reported in three phase I pharmacokinetic studies and two phase II clinical studies. Ceftazidime-avibactam appears to be well tolerated in healthy subjects and hospitalized patients, with few serious drug-related treatment-emergent adverse events reported to date.
In conclusion, avibactam serves to broaden the spectrum of ceftazidime versus ß-lactamase-producing Gram-negative bacilli. The exact roles for ceftazidime-avibactam will be defined by efficacy and safety data from further clinical trials. Potential future roles for ceftazidime-avibactam include the treatment of suspected or documented infections caused by resistant Gram-negative-bacilli producing extended-spectrum ß-lactamase (ESBL), Klebsiella pneumoniae carbapenemases (KPCs) and/or AmpC ß-lactamases. In addition, ceftazidime-avibactam may be used in combination (with metronidazole) for suspected polymicrobial infections. Finally, the increased activity of ceftazidime-avibactam versus P. aeruginosa may be of clinical benefit in patients with suspected or documented P. aeruginosa infections.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
Broad-spectrum activity, well characterized pharmacokinetic and pharmacodynamic properties, and proven efficacy and safety have made cephalosporins an important part of the antimicrobial armamentarium for decades [1]. However, the worldwide spread of extended-spectrum β-lactamases (ESBLs) [2], Klebsiella pneumoniae carbapenemases (KPCs) [3], metallo-β-lactamases (MBLs) [3] as well as the presence of chromosomal AmpC β-lactamases [4] in Gram-negative bacilli has reduced the utility of the cephalosporins and contributed to the increase in difficult-to-treat multidrug-resistant (MDR) organisms [5]. Ceftazidime is a well described third-generation cephalosporin with broad-spectrum activity against Gram-positive cocci and Gram-negative bacilli, including Pseudomonas aeruginosa; however, resistance—especially with Gram-negative bacilli—is increasing globally [6–8].
Avibactam (NXL104, AVE1330A), patented in 2011, is a non-β-lactam (diazabicyclooctane) [10] β-lactamase inhibitor, is active in vitro against Ambler class A and C β-lactamases and possesses activity versus some Ambler class D enzymes [9, 10]. Avibactam is being developed in combination with ceftazidime as well as in combination with ceftaroline, with the aim of broadening the spectra of these cephalosporins by inhibiting Ambler class A and C β-lactamases. Ceftazidime-avibactam is currently in phase III clinical trials for treatment of complicated urinary tract infection and complicated intra-abdominal infection (http://clinicaltrials.gov, identifiers NCT01595438, NCT01599806, NCT01499290 and NCT01500239).
This article reviews the existing published data for ceftazidime-avibactam, including relevant chemistry, mechanisms of action, mechanisms of resistance, microbiology, pharmacokinetics, pharmacodynamics, and efficacy and safety data from animal and human trials. Literature for this review was obtained via a comprehensive search of MEDLINE, SCOPUS and databases of scientific meetings from 2005 to September 2012 for all materials containing the name ‘ceftazidime’ and any of ‘avibactam’, ‘NXL104’ or ‘AVE1330A’. These results were supplemented by bibliographies obtained from Novexel (http://www.novexel.com/NXL104.htm) and AstraZeneca.
2 Chemistry
The cephem nucleus is a bicyclic ring system composed of a four-member β-lactam ring fused with a six-member dihydrothiazine ring, with a sulfur atom at position 1, a double-bond between carbon 2 and carbon 3, and a carboxylic acid at position 4 [1, 11]. The distinct properties of individual cephalosporins arise from side-chains attached to the cephem nucleus at positions 3 and 7. The properties conferred by particular cephalosporin side-chains have been extensively reviewed [12–14].
Ceftazidime’s position 7 side-chain is an amino-acyl group with an aminothiadiazole ring and a carboxypropyl-oxyimino chain attached at the α-carbon (Fig. 1). The aminothiadiazole ring, common to many extended-spectrum cephalosporins, confers increased activity against Gram-negative bacilli. In comparison with the methoxyimino group frequently found in other third-generation cephalosporins, the carboxypropyl-oxyimino group confers similar stability to many β-lactamases, slightly decreased activity towards the Enterobacteriaceae, but much-increased activity versus P. aeruginosa [13–15]. The methyl-pyridinium group at position 3 enhances activity versus P. aeruginosa [12], and provides ceftazidime with zwitterionic properties that enhance its water solubility [11].

Chemical structure of ceftazidime
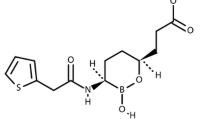
The chemical structure of avibactam is (1R,2S,5R)-7-oxo-6-(sulfoxy)-1,6-diazabicyclo[3.2.1]octan-2-carboxamide [9] (Fig. 2) and it has a molecular weight of 265.25 Da. Avibactam is a synthetic compound produced by an enantio-selective process [9, 16]. Although not a β-lactam, avibactam closely resembles β-lactams in key areas: the carbonyl at avibactam position 7 mimics the β-lactam carbonyl of a cephalosporin such as ceftazidime; the sulfate at position 6 of avibactam takes the place of the carboxyl group at ceftazidime position 4; and the carboxamide at position 2 of avibactam aligns with the amino-acyl side-chain at ceftazidime position 7 (Fig. 3). Avibactam is synthesized as a sodium salt that is water soluble and stable in aqueous solution at room temperature [17], but detailed chemical data have not been published to date.

Chemical structure of avibactam

Structural comparison of avibactam to ceftazidime
3 Mechanism of Action
Ceftazidime, like other β-lactams, inhibits peptidoglycan synthesis by inhibiting penicillin-binding proteins (PBPs) [18–20]. Inactivation of a sufficient fraction of the PBPs leads to an unstable peptidoglycan cell wall, ultimately resulting in cell death. Ceftazidime, by inhibiting peptidoglycan synthesis, inhibits growth of Escherichia coli and P. aeruginosa at low concentrations and induces rapid lysis in both species at higher concentrations [21].
β-lactamases are the most widespread and clinically important contributor toward β-lactam resistance, particularly among Gram-negative bacilli [4, 22, 23]. The β-lactamases are commonly classified into groups A, B, C and D based on similarity and difference in primary amino acid sequence as described by Ambler and colleagues [24–27]. A second system that classifies the β-lactamases by spectrum of activity and resistance to β-lactamase inhibitors was described by Bush and colleagues [28, 29], though the molecular (Ambler) classification system is referred to in this paper. The basic mechanism of action of β-lactamases has been well described [30–32]. A common strategy to inactivate β-lactamase activity is alteration of side-chains to create a molecule for which the β-lactamase has poor affinity (e.g. the 3 and 7 side-chains of the cephem nucleus). A second effective strategy is the pairing of a β-lactam with a β-lactamase inhibitor, a mechanistic or suicide substrate that inactivates the β-lactamase in much the same manner as the PBP is inactivated by a β-lactam. As new β-lactams and β-lactamase inhibitors have been introduced, selective pressure on clinical species expressing β-lactamases has driven their evolution such that for any given β-lactam, a β-lactamase now exists that is capable of inactivating it [28, 29]. A wide variety of mutations alter the spectrum of existing β-lactamases to increase their affinity for previously unaffected β-lactams or render them resistant to existing β-lactamase inhibitors [30, 33] (http://www.lahey.org/Studies/).
Avibactam has been shown to bond covalently to β-lactamases through the formation of a carbamate bond between avibactam’s position 7 carbonyl carbon and the same active-site serine that participates in acyl bonding with β-lactam substrates. The covalent nature of the bond has been confirmed via determination of the x-ray crystal structure of avibactam bound to a variety of β-lactamases [34–38], representing all three molecular classes of serine active site β-lactamases. Mass spectroscopy studies provide evidence that avibactam/β-lactamase binding involves a simple reaction mechanism with no rearrangement like that observed for molecules containing a β-lactam moiety [39–41].
Studies assessing the half maximal inhibitory concentration (IC50) values for avibactam have been measured and compared with clavulanic acid and tazobactam for a variety of class A and C β-lactamases (Table 1) [40]. Although IC50 values are time dependent [40], the values compiled in Table 1 originate from experiments using similar methodology, allowing for useful comparison. Avibactam has activity similar to that of clavulanic acid against SHV-4 and similar to that of both clavulanic acid and tazobactam against CTX-M-15, but shows greater activity than (i.e. is a more potent inhibitor) comparator inhibitors in all other cases, particularly against the carbapenemase KPC-2 and the class C β-lactamases.
A turnover value (indicating the number of inhibitor molecules required to deactivate a single enzyme) of 1 has been uniformly reported for avibactam (with one exception [42]). The turnover rate of clavulanic acid is greater than 100-fold that of avibactam against TEM-1 [40], while that of tazobactam is more than tenfold that of avibactam against P99, and 50-fold that of avibactam when inhibiting TEM-1 [40–42]. Initial studies reported an enzyme kinetic model where inactivation of the β-lactamase enzyme involved two binding steps: non-covalent association of avibactam with the binding site followed by covalent acylation of avibactam to the enzyme (along with opening of the 5-member urea ring) [34, 40–42].
A recent paper by Ehmann et al. proposes that the enzyme kinetics of avibactam are in fact that of a covalently-binding reversible inhibitor with a two-step binding process (as described above) and a slow deacylation phase that restores avibactam’s 5-membered urea ring [39]. The work of Ehmann et al. supports the notion that avibactam is released from the β-lactam in its original form. This experiment was repeated with each of CTX-M-15, KPC-2, P99 and the chromosomal AmpC of P. aeruginosa inhibited by avibactam serving as a donor to uninhibited TEM-1, with similar results [39]. Details of reaction mechanism leading to the restoration of avibactam as it is cleaved from the β-lactamase active site remain to be discovered.
4 Mechanism of Resistance
Limited data exist regarding the potential for avibactam to select for resistance and no data are available for ceftazidime-avibactam. Avibactam has been reported to not induce chromosomal ampC expression in Enterobacter cloacae [43]. Livermore et al. [44] studied the consequences of exposing Enterobacteriaceae to varying concentrations of avibactam when used along with ceftaroline (an oxyimino-cephalosporin). Single- and multi-step selection (where the concentration of ceftaroline was doubled each step) was performed and mutations were characterized by polymerase chain reaction (PCR), DNA sequencing and SDS-PAGE (sodium dodecyl sulfate polyacrylamide gel electrophoresis). Minimum inhibitory concentrations (MICs) of the pre- and post-selection organisms were compared for a large panel of β-lactam antibacterials. Single-step selection experiments found that isolated colonies occurred at a frequency of <10−9. An E. coli expressing a mutant CTX-M-15 was found to have gained resistance to ceftaroline-avibactam but lost resistance to all non-ceftaroline oxyimino cephalosporins through a point mutation in bla CTX-M-15 leading to a Lys237Gln substitution. Two AmpC-derepressed E. cloacae isolates were found to have identical deletions in ampC, gaining resistance to ceftaroline-avibactam with no loss of resistance to other agents. The MICs for three derepressed-AmpC E. cloacae were doubled six times against ceftaroline plus 1 mg/L avibactam, and four or five times against ceftaroline plus 4 mg/L avibactam. One E. cloacae mutant lacked the porins OmpC and OmpF but showed no other mutation, while the remaining mutants showed point mutations at the same location in ampC leading to Asn366His (in a mutant also showing reduced porin expression) and Asn366Ile substitutions. In experiments assessing the activity of several β-lactamase inhibitors against functional CMY-2 β-lactamase mutants, the affinity of avibactam for mutant enzymes was found to decrease, but this did not result in a reduction of in vitro antimicrobial activity [45, 46]. Clearly, information on potential mechanisms of resistance to avibactam are limited and no data exist with ceftazidime-avibactam, thus work is required in this area.
5 Microbiology
The MIC50, MIC90 and MIC range values (mg/L) presented in Tables 2, 3 and 4 are modal values derived from a review of available published literature for ceftazidime-avibactam and comparators to date. Table 2 shows the activity of ceftazidime-avibactam and comparators against Gram-negative bacteria [47–66]. These data demonstrate that the addition of avibactam greatly improves (4-1024-fold MIC reduction) the activity of ceftazidime versus most Enterobacteriaceae species depending on the presence or absence of a β-lactamase enzyme(s). Against P. aeruginosa, the addition of avibactam improves the activity of ceftazidime (~fourfold MIC90 reduction) [Table 2]. Limited data suggest that the addition of avibactam does not improve the activity of ceftazidime versus Acinetobacter species (Table 2).
Table 3 shows the activity of ceftazidime-avibactam compared with ceftazidime alone against E. coli and K. pneumoniae isolates producing specific β-lactamase enzymes [42, 47, 57, 58, 67–83]. It should be noted that, except where indicated, MIC values are based on results from fewer than ten isolates. Although the effect of avibactam was consistent when larger sample sizes were available, results derived from smaller numbers of isolates should be interpreted cautiously. Avibactam significantly improved the activity of ceftazidime against both E. coli and K. pneumoniae-producing ESBLs from Ambler classes A (4-1024-fold MIC reduction) and D (2-512-fold MIC reduction), KPC carbapenemases (32-8192-fold MIC reduction) and both chromosomal and mobile Ambler class C β-lactamases (2-512-fold MIC reduction). As expected, given its mechanism of action, avibactam does not improve the activity of ceftazidime against organisms producing MBLs such as New Delhi MBL (NDM) [Table 3]. It needs to be stated that the majority of Enterobacteriaceae with elevated ceftazidime-avibactam MIC values will likely contain multiple resistance mechanisms, which may include β-lactamases not inhibited by avibactam (i.e. some OXA-types and MBLs), porin alterations and overexpression of efflux pumps.
The activity of ceftazidime-avibactam and comparators against anaerobic bacteria is presented in Table 4 [84–86]. Versus Bacteroides fragilis, Clostridium perfringens and organisms from the Prevotella and Porphyromonas genera, ceftazidime-avibactam significantly increased the activity compared with ceftazidime alone. For other anaerobes, ceftazidime-avibactam showed little or no improvement over that of ceftazidime alone; most MIC50 values and all MIC90 values remained above the Clinical and Laboratory Standards Institute (CLSI) resistant breakpoint for ceftazidime (≥32 mg/L). No data have been published on the activity of ceftazidime-avibactam versus Gram-positive bacteria.
6 Pharmacokinetics
The pharmacokinetics of ceftazidime are well known. Following a 1 g dose (infused over 30 min), the concentration profile is best described by a two-compartment model with a rapid distribution phase, a maximum plasma drug concentration (Cmax) of ~100 mg/L, and a volume of distribution (Vd) of ~0.3 L/kg [1, 87]. Ceftazidime is approximately 17 % protein bound, is 80–90 % renally cleared with an elimination half-life (t½) of approximately 1.8 h in patients with normal renal function [1, 87]. Data on the interaction of ceftazidime with avibactam was published for 16 healthy volunteers [88]. Two cohorts of eight subjects were administered single doses of 250 mg or 500 mg of avibactam, followed (after a 7-day washout period) by a ceftazidime-avibactam dose of 1,000/250 mg and 2,000/500 mg, respectively. The presence of ceftazidime was not found to affect the pharmacokinetics of avibactam and, in the presence of avibactam, the pharmacokinetics of ceftazidime were unchanged.
The results of three phase I trials examining the single-dose pharmacokinetics of avibactam ranging from 50 mg to 2,000 mg are summarized in Table 5. In a single dose escalation study involving 70 subjects, the pharmacokinetics of avibactam were reported as linear for doses from 50 mg to 2,000 mg (Table 5) [88, 89, 91]. Following a 100-mg dose (infused over 30 min), the concentration profile of avibactam is best described by a two-compartment model with a rapid distribution phase, a Cmax of ~5.0 mg/L and a Vd at steady state (Vss) of ~22.5 L [88, 91]. To date, the protein binding of avibactam is unknown; avibactam, like ceftazidime, is primarily (95 %) renally cleared, with clearance correlating well with creatinine clearance (CLCR) [89]. The phase I studies in healthy volunteers describe an average half-life of 1.7–2.1 h. The study of avibactam in complicated intra-abdominal infection reported a 62 % increase in avibactam clearance compared with healthy subjects [90].
In six anuric patients, a pharmacokinetic study of 100 mg of avibactam administered over 30 mins prior to haemodialysis (4-h session) found a mean extraction coefficient of 0.77, with a total clearance of 9.29 L/h (155 mL/min), and approximately 54 % of the drug removed during dialysis, which is similar to ceftazidime [91]. In the same patient cohort, the average clearance off-dialysis was 1.02 L/h (17 mL/min) with a t½ of 22.2 h.
In summary, the pharmacokinetics of avibactam and ceftazidime appear to be very complementary, with similar Vd, t½ and clearance. The administration of ceftazidime does not impact the pharmacokinetics of avibactam.
7 Pharmacodynamics
The comparative results of an in vitro time kill study examining the bactericidal activity of ceftazidime in combination with avibactam against a variety of β-lactamase-producing genotypes are summarized in Table 6 [70]. In this study, ceftazidime alone was not bactericidal except at 256 mg/L against the K. pneumoniae expressing SHV-11, a non-ESBL. The comparator ceftazidime-clavulanic acid (ratio of 4:1) was only bactericidal against one E. cloacae isolate (at 32 mg/L), while the comparator piperacillin/tazobactam (ratio 8:1) was not bactericidal against any isolate at concentrations between 16 mg/L and 256 mg/L. In contrast, ceftazidime-avibactam proved to be bactericidal versus all strains at concentrations ranging from 2 to 8 mg/L (Table 6).
The bactericidal activity of two ceftazidime-avibactam dosing regimens was studied against a variety of β-lactamase-producing genotypes, in an in vitro pharmacodynamic hollow-fibre model [67]. Both regimens maintained a continuous infusion of ceftazidime at 16 mg/L, with regimen 1 adding a continuous infusion of avibactam at 4 mg/L, while regimen 2 added a single dose of avibactam (both with a 2-h half-life). Both regimens were tested against an E. cloacae isolate expressing AmpC, a K. pneumoniae isolate expressing CTX-M-15, and two K. pneumoniae isolates expressing SHV-5 and TEM-10, respectively. With ceftazidime alone, all four isolates demonstrated MICs >128 mg/L, ceftazidime-avibactam MICs were ≤4 mg/L for all isolates. For all isolates, the total area under the plasma concentration-time curve (AUC) of avibactam was either similar for both regimens or higher in regimen 2. Versus all isolates studied, both combinations of ceftazidime-avibactam were bactericidal (>3 log10 bacterial kill) within 2 h. Regarding regrowth, no regrowth was observed with regimen 1; however, regrowth was observed for all four isolates with regimen 2 after the concentration of avibactam dropped below the limit of detection of 0.5 mg/L. No change in pre- and post-experiment MIC occurred with any isolate treated with ceftazidime-avibactam.
An in vitro study examined the bactericidal activity of 2,000 mg ceftazidime dosed three times per day plus avibactam dosed as a continuous infusion with concentrations of 0.5, 1, 2, 4, 6, 8 or 10 mg/L over the course of 72 h versus a strain of Amp-C hyperproducing E. cloacae (ceftazidime-avibactam MIC of 0.5 mg/L, avibactam fixed at 2 mg/L) [92]. Bactericidal activity was monitored by change in viable colony counts and area under the bacterial kill curve. Ceftazidime-avibactam was bactericidal (≥3 log10) for all concentrations of avibactam. Regrowth was observed with all concentrations of avibactam. Whether this was due to low ceftazidime or avibactam concentrations was unknown; however, sigmoid curves fit at 12, 24, 48 and 72 h for change in viable colony count, and at 24, 48 and 72 h for area under the bacterial kill curve (r2 0.67 to 0.99), indicated that no additional benefit was gained from avibactam concentrations >2 mg/L.
Human plasma samples containing ceftazidime-avibactam were collected from a phase I pharmacokinetic and safety evaluation study and assessed in vitro for bactericidal activity against 5 × 105 colony-forming units (CFUs) of two K. pneumoniae strains: one ceftazidime-susceptible and one ceftazidime-resistant expressing AmpC and SHV-11 β-lactamases [88]. Plasma samples from eight subjects dosed with 1,000/250 mg ceftazidime-avibactam and eight subjects dosed with 2,000/500 mg ceftazidime-avibactam were found to be bactericidal (minimum of 3 log10 reduction from the initial inoculum count) versus both strains.
8 Animal Studies
Two studies have reported the efficacy of ceftazidime-avibactam in murine septicaemia. In the first study, female CD-1 mice were infected with 3.3 to 3.6 × 105 CFU of two strains of KPC-producing K. pneumoniae (strain VA-361 expressing KPC-2, TEM-1 and SHV-11 with ceftazidime MIC 256 mg/L, or strain VA-406 expressing KPC-2, TEM-1, SHV-11 and SHV-12 with ceftazidime MIC ≥512 mg/L) via intraperitoneal injection [93]. Single doses of ceftazidime-avibactam (ratios of 2:1, 4:1, 8:1 and 16:1; ceftazidime doses, depending on strain and ratio, from 1 to 64 mg/kg by twofold steps) or ceftazidime alone (512, 1,024 or 2,048 mg/kg) were administered subcutaneously 30 minutes after infection. Five mice were tested per dose, survival rate was monitored twice daily for 5 days, and all tests were performed in triplicate. Untreated mice died within 24 to 48 hours. For ceftazidime alone, effective dose in 50% (ED50) was 1,578 mg/kg for strain VA-261 and 709 mg/kg for strain VA-406, whereas for ceftazidime-avibactam, ED50 values were significantly reduced at 8.1, 15.1, 16.9 and 29.5 mg/kg (ceftazidime component) for strain VA-261, and 3.5, 3.8, 7.2 and 12.1 mg/kg for strain VA-406 for ceftazidime-avibactam ratios of 2:1, 4:1, 8:1 and 16:1, respectively. At any given dose, animal survival was observed to increase as the proportion of avibactam in ceftazidime-avibactam increased.
In the second septicaemia study, male CD-1 mice were infected with 108 CFU of one of four ceftazidime-resistant strains (E. coli expressing CTX-M-16 and TEM-1; E. coli expressing CTX-M-2 and TEM-1; K. pneumoniae expressing CTX-M-2, SHV-2 and TEM-12; K. pneumoniae expressing CTX-M-2 and TEM-1B, all with ceftazidime MICs from 32 to >128 mg/L) by intraperitoneal injection [71]. Infected mice were administered subcutaneous doses at 1 and 4 h post-infection with one of ceftazidime-avibactam (4:1 ratio, ceftazidime doses 3, 10 and 30 mg/kg), ceftazidime (doses 3, 10, 30 and 60 mg/kg), cefotaxime (doses 3, 10, 30, 60 and 90 mg/kg) or piperacillin/tazobactam (4:1 ratio, piperacillin doses 30, 60 and 90 mg/kg). Ten to twenty mice were infected per strain per dose regimen, and survival was monitored for 5 days. Untreated mice died within 2 days. For ceftazidime-avibactam, ED50 values were reported as 11 mg/kg/dose (for the ceftazidime component) for the E. coli strain expressing CTX-M-16 and TEM-1, 27 mg/kg/dose for the E. coli strain expressing CTX-M-2 and TEM-1, 27 mg/kg/dose for the K. pneumoniae strain expressing CTX-M-2, SHV-2 and TEM-12, and 18 mg/kg/dose for the K. pneumoniae strain expressing CTX-M-2 and TEM-1B. ED50 values for all comparators for all strains were >90 mg/kg/dose except for ceftazidime alone against the E. coli strain expressing CTX-M-16 and TEM-1, with an ED50 of 74 mg/kg/dose.
In a murine kidney infection model study, male CD-1 mice were infected with approximately 104 CFU of one of six ceftazidime-resistant strains (E. coli expressing SHV-4, E. coli expressing AmpC, E. cloacae expressing AmpC, K. pneumoniae expressing AmpC and SHV-11, Morganella morganii expressing AmpC, or Citrobacter freundii expressing AmpC, all with ceftazidime MICs from 16 to >128 mg/L) via direct injection to the left kidney [68]. Infected mice were treated at 4, 8, 24 and 32 h after infection with one of ceftazidime-avibactam (ratio 4:1), ceftazidime alone, ceftazidime/clavulanic acid (ration 4:1, 10 or 25 mg/kg/dose for all ceftazidime components) or imipenem (10 or 25 mg/kg/dose). Four mice were infected per dose group or control group, control groups were euthanized at 4 and 48 h, and test mice were euthanized at 48 h. At 10 mg/kg/dose, ceftazidime was ineffective at eradicating the pathogen from the kidney versus the E. coli strain expressing AmpC and the C. freundii strain. Ceftazidime-avibactam (10 mg/kg/dose) was significantly more effective than ceftazidime alone against the AmpC-expressing E. coli. Ceftazidime-avibactam (10 mg/kg/dose) and imipenem (10 mg/kg/dose) were significantly more effective than ceftazidime alone against the C. freundii strain. At 25 mg/kg/dose, ceftazidime was ineffective against the SHV-4-expressing E. coli strain and the E. cloacae, K. pneumoniae and M. morganii strains. Ceftazidime/clavulanic acid (25 mg/kg/dose) was significantly more effective than ceftazidime alone against the SHV-4-expressing E. coli strain and the M. morganii strain, and both ceftazidime-avibactam (25 mg/kg/dose) and imipenem (25 mg/kg/dose) were significantly more effective than ceftazidime alone against all four strains. Bacterial load in the kidney in mice receiving ceftazidime-avibactam was 2.6 to 4.5 log10 lower than the bacterial load in mice receiving ceftazidime alone.
In a neutropenic murine thigh infection model study, female CD-1 mice were infected with 106 CFU of two strains of KPC-producing K. pneumoniae (strain VA-361 expressing KPC-2, TEM-1 and SHV-11 with ceftazidime MIC 256 mg/L, and strain VA-406 expressing KPC-2, TEM-1, SHV-11 and SHV-12 with ceftazidime MIC ≥512 mg/L) via intramuscular injection in the right thigh [93]. Mice were treated 1.5 hours after infection with a single subcutaneous dose of ceftazidime-avibactam (4:1 ratio with doses of the ceftazidime component ranging by twofold steps from 32 to 1,024 mg/kg for strain VA-361, and 8 to 1,024 mg/kg for strain VA-406) or ceftazidime alone (1,024 mg/kg or 2,048 mg/kg). Three mice were tested per dose and control group, treatment mice were euthanized and analysed 24 h after infection, and control mice were euthanized and analysed 1.5 and 24 h after infection. Doses resulting in bacteriostasis using ceftazidime-avibactam were 216/54 mg for strain VA-361 and 116/29 mg for strain VA-406.
In a second human-simulated study of murine thigh infection in both immunocompromised (cyclophosphamide-induced neutropenia) and immunocompetent mice, immunocompromised mice were infected with one of 27 strains of P. aeruginosa in triplicate, and immunocompetent mice were infected with one of 15 strains in triplicate [94]. Ceftazidime-avibactam MICs ranged from 4 to 32 mg/L and all but one isolate was non-susceptible to ceftazidime alone (MICs ranging from 8 to >128 mg/L). Human simulated regimens of ceftazidime or ceftazidime-avibactam beginning 2 h after inoculation were administered. Simulated regimens were pharmacokinetically assessed to closely match human dosing of 2 g ceftazidime or 2 g ceftazidime plus 500 mg avibactam every 8 h. By analysis of post-treatment bacterial loads, the authors reported that the in vivo activity was pharmacodynamically predictable based on the MIC of the strain to the drug tested. Ceftazidime decreased bacterial counts by ≥0.5 log10 in only 10/27 isolates; while ceftazidime avibactam did so in 22/27 of the P. aeruginosa strains. In the immunocompetent mice, ceftazidime achieved reductions of ≥0.3 log10 in 10/15 isolates, while ceftazidime-avibactam did so against all 15 isolates [94].
In a murine pneumonia model study, immunosuppressed female Swiss OF1 mice were infected intratracheally with 108 to 109 CFU of a LAT-4 and SHV-11-producing strain of K. pneumoniae [75]. Mice were treated twice per day for 2 days with subcutaneous doses of 2:1 ceftazidime-avibactam (150/75 mg/kg), 4:1 ceftazidime-avibactam (150/37.5 mg/kg), ceftazidime (150 mg/kg), 2:1 ceftazidime/clavulanic acid (150/75 mg/kg), 4:1 ceftazidime/clavulanic acid (150/37.5 mg/kg) or 1:1 imipenem/cilastatin (150 mg/kg each) beginning 16–18 hours after infection. Thirty mice were tested per treatment group, 20 mice were tested per control group, and lung bacterial burden was assessed at 24 and 48 h after initiation of treatment. Untreated mice died within 48 h of infection. Compared with treatment with ceftazidime alone, lung bacterial burden was significantly reduced at 48 h by the 2:1 and 4:1 ceftazidime-avibactam regimens and the imipenem/cilastatin regimen (p < 0.05 in all cases). A CFU reduction of 6.6 ± 1.0 log10 was found for the 2:1 ceftazidime-avibactam regimen and 7.9 ± 0.1 log10 for the 4:1 ceftazidime-avibactam regimen compared with a 0.7 ± 1 log10 reduction for ceftazidime alone.
In a rabbit meningitis model study, pathogen-free New Zealand rabbits were infected via direct injection to the subarachnoid space of approximately 105 CFU of an AmpC-producing K. pneumoniae strain (ceftazidime MIC >128 mg/L) [69]. Rabbits were treated starting 8 h post-infection with an intravenous regimen of 150 mg/kg ceftazidime at h 0 and 4, 150/37.5 mg/kg ceftazidime-avibactam at h 0 followed by 150 mg/kg ceftazidime at h 4, or 125 mg/kg meropenem at h 0 and 4. Five rabbits were used per treatment and control group and cerebrospinal fluid (CSF) was sampled at 0, 1, 2, 4, 6 and 8 h following start of treatment. Both the ceftazidime-avibactam regimen and the meropenem regimen were found to be bactericidal (>3 log10 CFU reduction in CSF from initial values) 5 h after start of treatment. Eight h after start of treatment, CSF CFU levels were reduced by 0.10 ± 0.45 for ceftazidime, 4.23 ± 0.60 for meropenem, and 5.66 ± 0.83 for the ceftazidime-avibactam regimen. By two-tailed Fisher exact test, the meropenem and ceftazidime-avibactam regimens were reported as significantly different from the ceftazidime regimen (p < 0.05) and the ceftazidime-avibactam regimen was reported as significantly different from the meropenem regimen (p < 0.05).
In summary, these animal studies show that ceftazidime-avibactam is effective in a variety of animal infection models including murine septicaemia, murine kidney infection, neutropenic murine thigh infection, neutropenic murine pneumonia and rabbit meningitis, infected with a variety of β-lactamase-producing organisms including ESBL, KPC and AmpC. More studies are required to assess the optimal way to administer ceftazidime-avibactam and the optimal pharmacodynamic parameters to optimize efficacy and minimize resistance selection.
9 Clinical Trials
The results of two ceftazidime-avibactam phase II clinical trials have been published to date (Table 7) and are reviewed. A prospective, international, multicentre, double-blinded, randomized (1:1) trial compared safety and efficacy of ceftazidime-avibactam (2,000/500 mg) plus metronidazole (500 mg) with meropenem (1,000 mg), each administered intravenously three times daily for the treatment of complicated intra-abdominal infection in hospitalized adults (NCT00752219) [95]. Male and female patients aged 18–90 years with indications of complicated intra-abdominal infection (including infection in the appendix 47.3 %, stomach/duodenum 25.6 %, colon or small bowel 17.2 %, gall bladder, liver or spleen 9.4 %) caused by organisms determined to be susceptible to either treatment arm and requiring surgery and antibacterial therapy, were recruited if they were free of sepsis, did not have abnormal liver function tests (ALT, AST alkaline phosphatase [AP] or bilirubin >3 times the upper limit of normal) or impaired renal function (CLCR <50 mL/min), were not immunocompromised, had Acute Physiology and Chronic Health Evaluation (APACHE)-II scores ≤25, were expected to survive for the entire study period, and had not had systemic antibacterials within 72 h pre-study (with the exception of previous failed therapy or surgical prophylaxis for less than 24 h). Both ceftazidime-avibactam plus metronidazole and meropenem regimens (Table 7) were administered for 5–14 days. A total of 203 patients were initially enrolled in the study, with 68 patients clinically evaluable for ceftazidime-avibactam plus metronidazole and 76 for meropenem at the end of the study. Patients did not finish the study for a variety of reasons, including patient withdrawal, protocol violation, lost to follow-up and adverse effects (no differences between treatment arms). Favourable clinical response rates (complete resolution or significant improvement of the signs and symptoms of infection 2 weeks after the last treatment dose) were 91.2 % (62/68) for patients receiving ceftazidime-avibactam plus metronidazole and 93.4 % (71/76) for patients receiving meropenem. Response rates were not significantly different (p = 0.60). Microbiological eradication was considered equivalent to favourable clinical response. The most common pathogens isolated included Enterobacteriaceae (89.7 % in the ceftazidime-avibactam plus metronidazole arm) and 92.1 % in the meropenem arm. For patients found to have one or more ceftazidime-resistant (MIC >8 mg/L) Gram-negative bacilli, a favourable microbiological response was achieved in 96.2 % (25 of 26) of patients in the ceftazidime-avibactam plus metronidazole arm and 94.1 % (16 of 17) of patients in the meropenem arm. Adverse effects occurred in 15 % of patients in the ceftazidime-avibactam plus metronidazole arm and 17 % of patients in the meropenem arm.
A prospective, international, multicentre, investigator-blinded, randomized (1:1) study compared safety and efficacy of ceftazidime-avibactam (500/125 mg) administered three times daily (30-min infusion) to imipenem/cilastatin (500 mg) administered four times daily (30-min infusion), for the treatment of complicated urinary tract infections, including acute pyelonephritis in hospitalized adults (NCT00690378) [96]. Recruited patients were males and females aged 18–90 years with documented acute pyelonephritis (59.7 %) or other complicated urinary tract infection (40.3 %) caused by Gram-negative organisms not resistant to one or both study drugs. Patients were excluded if they had received more than one dose of a potentially effective antibacterial within 48 h prior to admission urine culture (or any doses after culture), had an ileal loop, vesicoureteral reflux, complete obstruction of any portion of the urinary tract, perinephric or intrarenal abscess, a permanent indwelling catheter or nephrostomy, or a history of hypersensitivity to either study medication. Both ceftazidime-avibactam and imipenem/cilastatin (Table 7) were administered for 7–14 days. Patients meeting pre-defined clinical criteria for improvement (afebrile ≥24 h, resolution of nausea and vomiting, improved signs and symptoms) after a minimum of 4 days of either therapy were switched to oral ciprofloxacin 500 mg every 12 h, or an appropriate oral alternative if necessary (maximum 14 days). A total of 135 patients received study therapy, of whom 62 were microbiologically evaluable (27 in the ceftazidime-avibactam arm and 356 in the imipenem arm). Clinically evaluable patients included 28 in the ceftazidime-avibactam arm and 36 in the imipenem arm. Patients were excluded from the clinical and microbiologically evaluable populations mainly due to lack of an isolated pathogen (23 in the ceftazidime-avibactam group, 19 in the imipenem/cilastatin group). Favourable microbiological response was the primary outcome, defined as both eradication of pathogens in the urinary tract (reduction of levels in the urine from ≥105 CFU/mL to <104 CFU/mL) and no pathogens in the blood at a follow-up 5–9 days after completion of therapy. Favourable clinical response was a secondary outcome, defined as resolution of all or most pre-therapy signs and symptoms, with no further (non-study) antibacterial required. Favourable microbiological response rates were 70.4 % for the ceftazidime-avibactam arm and 71.4 % for the imipenem/cilastatin arm. Favourable clinical response rates were 85.7 % for the ceftazidime-avibactam arm and 80.6 % for the imipenem/cilastatin arm. Microbiological response rates were not significantly different (95 % CI difference of −27.2 % to 25.0 %), but the significance of clinical response rate was not tested. Six of seven patients in the ceftazidime-avibactam arm and 9 of 11 patients in the imipenem/cilastatin arm had favourable microbiological outcomes against ceftazidime-resistant pathogens (MIC >8 mg/L). Adverse effects in this study were reported in 67.7 % of patients in the ceftazidime-avibactam arm and 76.1 % of patients in the imipenem/cilastatin arm.
Clinical trials to date suggest that ceftazidime-avibactam is as effective as standard carbapenem therapy in complicated intra-abdominal infection and complicated urinary tract infection, including infection caused by ceftazidime-resistant Gram-negative bacilli. At the time of writing, phase III trials are still in progress.
10 Adverse Effects
The safety and tolerability of ceftazidime-avibactam has been reported in three phase I pharmacokinetic studies and two phase II clinical studies. In these studies, assessment was conducted by physical examination, laboratory tests, vital sign monitoring, ECG recording and recording of treatment-emergent adverse events [88, 91, 95, 96], except in one phase I study where adverse events were assessed by subject interview [97].
In three phase I pharmacokinetic studies encompassing 119 subjects, treatment-emergent events were observed in 14 healthy subjects (one or more per subject). One event, orthostatic hypotension, was reported as moderate, while the remainder, including abdominal pain, anxiety, application site bruising, dry mouth, dysgeusia, feeling hot, feeling jittery, headache, hyperhidrosis, postural dizziness, sense of oppression, and somnolence, were reported as minor. Four treatment-related events were reported in three anuric subjects: general discomfort, stomach pain, ructus and symptoms of hypoglycaemia (in a diabetic patient) [91]. No subject withdrew from these studies as a result of an adverse event.
In a phase II study comparing the treatment of complicated intra-abdominal infection by ceftazidime-avibactam plus metronidazole (safety population 101) and meropenem (safety population 102), treatment-emergent events (drug related or not) reported by 5 % or more patients were nausea, vomiting, abdominal pain, pyrexia, wound secretion, cough, haematuria and increases in liver enzymes (ALT, AST, AP), platelet count and white blood cell count tests [95]. Drug-related adverse effects were reported in 15 % of the ceftazidime-avibactam plus metronidazole arm and 17 % of the meropenem arm. The types and frequency of all treatment-emergent adverse effects were similar for both arms, though it was noted that the ceftazidime-avibactam plus metronidazole arm had a higher number of gastrointestinal (GI)-tract events (nausea, vomiting, abdominal pain) and the meropenem arm had a higher number of liver enzyme elevation events (ALT, AST, AP). Serious adverse events were observed in nine patients in the ceftazidime-avibactam and 11 patients in the meropenem arm, though only one of these events (elevated liver enzymes in a ceftazidime-avibactam plus metronidazole patient) was considered drug related.
In a phase II study comparing the treatment of complicated urinary tract infection by ceftazidime-avibactam (safety population 68) and imipenem/cilastatin (safety population 67), treatment-emergent events (drug related or not) reported by 5 % or more patients were constipation, diarrhoea, abdominal pain, upper abdominal pain, abdominal distension, headache, dizziness, chest pain, anxiety, insomnia, injection/infusion site reaction, increased ALT levels, back pain and hypertension [96]. Drug-related adverse effects were reported by 35.3 % of patients in the ceftazidime-avibactam arm and 50.7 % of patients in the imipenem/cilastatin arm, though it should be noted that adverse events continued to be recorded after conversion to oral therapy following clinical improvement (see “Clinical Trials” section). Serious drug-related adverse events were reported for three patients in the ceftazidime-avibactam arm (accidental overdose, diarrhoea, renal failure) and one in the imipenem/cilastatin arm (increased serum creatinine). The overdose caused no sequelae.
A double-blind, randomized, placebo-controlled, four-way crossover, phase I study conducted in a single centre investigated the effect of a supra-therapeutic dose of ceftazidime-avibactam on cardiac depolarization [98]. Non-smoking male subjects (n = 51) with median age 26 years (range 18–45) and median body mass index (BMI) 26.5 kg/m2 (range 19.4–30.0) were enrolled in the study; 43 were evaluable. Subjects received four treatments in random order (with minimum 3-day washout between treatments): a 30-min infusion of 3,000/2,000 mg ceftazidime-avibactam following a 30-min infusion of saline placebo; a 60-min infusion of 1,500/2,000 mg ceftaroline fosamil-avibactam administered as two 30-min infusions; saline placebo administered as two 30-min infusions; a single, open-label, oral dose of 400 mg moxifloxacin as active control. Primary outcome was Fridericia-corrected QT interval; ECG values (heart rate and RR, PR, QRS and QT intervals) were also assessed at 0, 0.5, 1, 1.5, 2, 3, 4, 6, 8, 12 and 24 h. Ceftazidime-avibactam was found not to significantly elevate the Fridericia-corrected QT interval, and observed ECG values were similar for ceftazidime-avibactam and placebo. Compared with moxifloxacin, ceftazidime-avibactam was found to result in significantly lower elevations in the Fridericia-corrected QT interval. Urticaria (in one patient) was the only reported non-mild adverse event related to ceftazidime-avibactam. Eleven mild adverse events experienced by patients in the ceftazidime-avibactam group were reported by system-organ-class: four skin/soft tissue disorders, three GI tract disorders, three administration-site conditions and one cardiac palpitation. No abnormalities were observed in vital signs, laboratory tests or physical examinations.
To date, ceftazidime-avibactam appears to be well tolerated in healthy subjects as well as patients with infectious diseases, with few serious drug-related treatment-emergent adverse events reported.
11 Place of Ceftazidime/Avibactam in Therapy
The addition of avibactam restores the activity of ceftazidime against Gram-negative bacilli that achieve β-lactam resistance through expression of the Ambler class A ESBLs, chromosomal or mobile class C β-lactamases, serine carbapenemases, or some class D β-lactamases. Safety and pharmacokinetic results published to date suggest that no additional considerations need to be taken when dosing ceftazidime-avibactam compared with ceftazidime alone. Ceftazidime-avibactam has demonstrated clinical efficacy similar to that of carbapenem therapy in phase II studies of complicated intra-abdominal infection and complicated urinary tract infection (including acute pyelonephritis). The extensive clinical experience with ceftazidime and the knowledge that avibactam broadens the spectrum of ceftazidime versus ß-lactamase-producing Gram-negative bacilli, will provide clinicians with confidence in using this agent. To date, no data are available on the efficacy of ceftazidime-avibactam for the treatment of difficult-to-treat infections such as hospital-acquired and ventilator-acquired pneumonia. The exact roles for ceftazidime-avibactam in the treatment of infectious diseases will, in part, depend on the development of other β-lactam/β-lactamase inhibitor combinations including ceftaroline-avibactam, imipenem-MK7655 and ceftolozane-tazobactam. An important advantage of ceftazidime-avibactam is that its development is furthest along and it may be first to market.
Potential future roles for ceftazidime-avibactam include the treatment of suspected or documented infections caused by resistant Gram-negative bacilli-producing ESBL, KPC and/or AmpC β-lactamases. In addition, ceftazidime-avibactam may be used in combination (with metronidazole) for suspected polymicrobial infections. Finally, the increased activity of ceftazidime-avibactam versus P. aeruginosa may be of clinical benefit in patients with suspected or documented P. aeruginosa infections.
References
Andes D, Craig W. Cephalosporins. In: Mandell G, Bennett J, Dolin R, editors. Principles and practice of infectious diseases. 7th ed. Philadelphia: Churchill Livingstone Elsevier; 2010. p. 323–37.
Pitout JD. Infections with extended-spectrum beta-lactamase-producing enterobacteriaceae: changing epidemiology and drug treatment choices. Drugs. 2010;70(3):313–33.
Bush K. Alarming beta-lactamase-mediated resistance in multidrug-resistant Enterobacteriaceae. Curr Opin Microbiol. 2010;13(5):558–64.
Livermore DM, Woodford N. The beta-lactamase threat in Enterobacteriaceae, Pseudomonas and Acinetobacter. Trends Microbiol. 2006;14(9):413–20.
Livermore DM. Has the era of untreatable infections arrived? J Antimicrob Chemother. 2009;64(Suppl 1):i29–36.
Turner PJ. MYSTIC Europe 2007: activity of meropenem and other broad-spectrum agents against nosocomial isolates. Diagn Microbiol Infect Dis. 2009;63(2):217–22.
Hawser SP, Badal RE, Bouchillon SK, et al. Trending eight years of in vitro activity of ertapenem and comparators against Escherichia coli from intra-abdominal infections in North America–SMART 2002–2009. J Chemother. 2011;23(5):266–72.
Hoban DJ, Nicolle LE, Hawser S, et al. Antimicrobial susceptibility of global inpatient urinary tract isolates of Escherichia coli: results from the Study for Monitoring Antimicrobial Resistance Trends (SMART) program: 2009–2010. Diagn Microbiol Infect Dis. 2011;70(4):507–11.
Bhattacharya S, Bonnet A, Dedhiya M, et al. inventors; Novexel SA and Forest laboratories holdings, assignees. Polymorphic and pseudopolymorphic forms of a pharmaceutical compound. International patent WO 042560 A2. 2011 April 14.
Coleman K. Diazabicyclooctanes (DBOs): a potent new class of non-beta-lactam beta-lactamase inhibitors. Curr Opin Microbiol. 2011;14(5):550–5.
Beale J. Antibacterial antibiotics. In: Beale J, Block J, editors. Wilson and Gisvold’s textbook of organic medicinal and pharmaceutical chemistry. 12th ed. Baltimore: Lippincott Williams & Wilkins; 2011. p. 258–329.
Caprile KA. The cephalosporin antimicrobial agents: a comprehensive review. J Vet Pharmacol Ther. 1988;11(1):1–32.
Dunn GL. Ceftizoxime and other third-generation cephalosporins: structure-activity relationships. J Antimicrob Chemother. 1982;10(Suppl. C):1–10.
Neu HC. Beta-lactam antibiotics: structural relationships affecting in vitro activity and pharmacologic properties. Rev Infect Dis. 1986;8(Suppl. 3):S237–59.
Neu HC. Beta-lactamase stability of cefoxitin in comparison with other beta-lactam compounds. Diagn Microbiol Infect Dis. 1983;1(4):313–6.
Miossec C, Merdjan H, Hodgson J. Safety and toxicokinetics of NXL104, a broad spectrum β-lactamase inhibitor, in the rat [abstract no. F-1461 plus poster]. In: 45th Annual Interscience Conference on Antimicrobial Agents and Chemotherapy; 2005 Dec 16–19; Washington (DC).
Miossec C. NXL104 β-lactamase inhibitor [abstract no. plus oral presentation]. Challenge of antibacterial drug development; 2007 Mar 21–22; San Diego, CA.
Popham DL, Young KD. Role of penicillin-binding proteins in bacterial cell morphogenesis. Curr Opin Microbiol. 2003;6(6):594–9.
Vollmer W, Blanot D, de Pedro MA. Peptidoglycan structure and architecture. FEMS Microbiol Rev. 2008;32(2):149–67.
Sauvage E, Kerff F, Terrak M, et al. The penicillin-binding proteins: structure and role in peptidoglycan biosynthesis. FEMS Microbiol Rev. 2008;32(2):234–58.
Hayes MV, Orr DC. Mode of action of ceftazidime: affinity for the penicillin-binding proteins of Escherichia coli K12, Pseudomonas aeruginosa and Staphylococcus aureus. J Antimicrob Chemother. 1983;12(2):119–26.
Poole K. Resistance to beta-lactam antibiotics. Cell Mol Life Sci. 2004;61(17):2200–23.
Bush K, Fisher JF. Epidemiological expansion, structural studies, and clinical challenges of new beta-lactamases from gram-negative bacteria. Annu Rev Microbiol. 2011;65:455–78.
Ambler RP. The structure of beta-lactamases. Philos Trans R Soc Lond B Biol Sci. 1980;289(1036):321–31.
Ambler RP, Coulson AF, Frere JM, et al. A standard numbering scheme for the class A beta-lactamases. Biochem J. 1991;276(Pt 1):269–70.
Jaurin B, Grundstrom T. ampC cephalosporinase of Escherichia coli K-12 has a different evolutionary origin from that of beta-lactamases of the penicillinase type. Proc Natl Acad Sci USA. 1981;78(8):4897–901.
Ouellette M, Bissonnette L, Roy PH. Precise insertion of antibiotic resistance determinants into Tn21-like transposons: nucleotide sequence of the OXA-1 beta-lactamase gene. Proc Natl Acad Sci USA. 1987;84(21):7378–82.
Bush K, Jacoby GA. Updated functional classification of beta-lactamases. Antimicrob Agents Chemother. 2010;54(3):969–76.
Bush K, Jacoby GA, Medeiros AA. A functional classification scheme for beta-lactamases and its correlation with molecular structure. Antimicrob Agents Chemother. 1995;39(6):1211–33.
Majiduddin FK, Materon IC, Palzkill TG. Molecular analysis of beta-lactamase structure and function. Int J Med Microbiol. 2002;292(2):127–37.
Ghuysen JM. Serine beta-lactamases and penicillin-binding proteins. Annu Rev Microbiol. 1991;45:37–67.
Tamilselvi A, Mugesh G. Zinc and antibiotic resistance: metallo-beta-lactamases and their synthetic analogues. J Biol Inorg Chem. 2008;13(7):1039–53.
Knox JR. Extended-spectrum and inhibitor-resistant TEM-type beta-lactamases: mutations, specificity, and three-dimensional structure. Antimicrob Agents Chemother. 1995;39(12):2593–601.
Docquier J, Stachyra T, Benvenuti M, et al. High resolution crystal structure of CTX-M-15 in complex with the new β-lactamase inhibitor NXL104 [abstract no. C1-1098 plus oral presentation]. In: 49th Annual Interscience Conference on Antimicrobial Agents and Chemotherapy; 2009 Sep 12–15; San Francisco (CA).
Xu H, Hazra S, Blanchard JS. NXL104 irreversibly inhibits the beta-lactamase from Mycobacterium tuberculosis. Biochemistry. 2012;51(22):4551–7.
Docquier J, Benvenuti M, De Luca F, et al. Structure of the TRU-1 class C and OXA-10 class D β-lactamases in complex with NXL104: structural basis for broad-spectrum inhibition [abstract no. C1-1427 plus poster]. In: 50th Annual Interscience Conference on Antimicrobial Agents and Chemotherapy; 2010 Sep 12–15; Boston (MA).
Docquier J, Benvenuti M, De Luca F, et al. X-ray crystal structure of the Klebsiella pneumoniae OXA-48 class D carbapenemase inhibited by NXL104 [abstract no. C1-640 plus poster]. In: 50th Annual Interscience Conference on Antimicrobial Agents and Chemotherapy; 2010 Sep 12–15; Boston (MA).
Docquier J, Benvenuti M, Bruneau J, et al. X-ray crystal structure of the Acinetobacter baumannii OXA-24/40 Class D carbapenemase inhibited by NXL104 [abstract no. P609]. Clin Microbiol Infect. 2011;17(Suppl. 4):S125. Plus poster presented at 21st European Congress of Clinical Microbiology and Infectious Diseases; 2011 May 7–10; Milan.
Ehmann DE, Jahic H, Ross PL, et al. Avibactam is a covalent, reversible, non-beta-lactam beta-lactamase inhibitor. Proc Natl Acad Sci USA. 2012;109(29):11663–8.
Stachyra T, Pechereau M, Bruneau J, et al. The nature of inhibition of TEM-1 β-Lactamase by the non-β-Lactam inhibitor NXL104 [abstract no. C1-1374 plus poster]. In: 49th Annual Interscience Conference on Antimicrobial Agents and Chemotherapy; 2009 Sep 12–15; San Francisco (CA).
Stachyra T, Pechereau MC, Bruneau JM, et al. Mechanistic studies of the inactivation of TEM-1 and P99 by NXL104, a novel non-beta-lactam beta-lactamase inhibitor. Antimicrob Agents Chemother. 2010;54(12):5132–8.
Bonnefoy A, Dupuis-Hamelin C, Steier V, et al. In vitro activity of AVE1330A, an innovative broad-spectrum non-beta-lactam beta-lactamase inhibitor. J Antimicrob Chemother. 2004;54(2):410–7.
Miossec C, Claudon M, Platel D, et al. The β-lactamase inhibitor NXL104 does not induce ampC β-lactamase expression in Enterobacter cloacae: evaluation of ampC expression by quantitative polymerase chain reaction (Q-PCR) [abstract no. F-128 plus poster]. In: 46th Annual Interscience Conference on Antimicrobial Agents and Chemotherapy; 2006 Sep 27–30; San Francisco (CA).
Livermore DM, Mushtaq S, Barker K, et al. Characterization of beta-lactamase and porin mutants of Enterobacteriaceae selected with ceftaroline + avibactam (NXL104). J Antimicrob Chemother. 2012;67(6):1354–8.
Li M, Conklin B, Bonomo R, et al. Effect of N152G substitution of CMY-2 β-lactamase activity and inhibition [abstract no. A-1012 plus poster]. In: 111th General Meeting of the American Society of Microbiology; 2011 May 21–24; New Orleans (LA).
Skalweit M, Li M, Conklin B, et al. Effect of N152G, S and T substitution on CMY-2 β-lactamase activity and inhibition [abstract no. C1-601 plus poster]. In: 51st Annual Interscience Conference on Antimicrobial Agents and Chemotherapy; 2011 Sep 17–20; Chicago (IL).
Aktas Z, Kayacan C, Oncul O. In vitro activity of NXL104 in combination with β-lactams against Gram-negative bacteria, including OXA-48 beta-lactamase producing Klebsiella pneumoniae [abstract no. E-808 plus poster]. In: 50th Annual Interscience Conference on Antimicrobial Agents and Chemotherapy; 2010 Sep 12–15; Boston (MA).
Aktas Z, Kayacan C, Oncul O. In vitro activity of avibactam (NXL104) in combination with beta-lactams against Gram-negative bacteria, including OXA-48 beta-lactamase-producing Klebsiella pneumoniae. Int J Antimicrob Agents. 2012;39(1):86–9.
Biedenbach D, Konrardy M, Sader H, et al. In vitro activity of ceftazidime/NXL104 against pathogens collected during a phase II complicated urinary tract infection (cUTI) clinical trial [abstract no. E-137 plus poster]. In: 51st Annual Interscience Conference on Antimicrobial Agents and Chemotherapy; 2011 Sep 17–20; Chicago (IL).
Castanheira M, Rhomberg P, Jones R, et al. Potent activity of ceftazidime/NXL104 tested against Enterobacteriaceae isolates carrying multiple β-lactamase enzymes [abstract no. P 1265]. Clin Microbiol Infect. 2010;16(Suppl. 2):S355. Plus poster presented at 20th European Congress of Clinical Microbiology and Infectious Diseases; 2010 Apr 10–13; Vienna.
Crandon J, Banevicius M, Nicolau D. Comparative potency of ceftazidime (CAZ) and ceftazidime-NXL104 (CAZ104) against a resistant population of clinical Pseudomonas aeruginosa (PSA) isolates [abstract no. 585 plus poster]. In: 49th Annual Meeting of the Infectious Diseases Society of America; 2011 Sep 12–15; Boston (MA).
Endimiani A, Choudhary Y, Bonomo RA. In vitro activity of NXL104 in combination with beta-lactams against Klebsiella pneumoniae isolates producing KPC carbapenemases. Antimicrob Agents Chemother. 2009;53(8):3599–601.
Gin A, Dilay L, Karlowsky JA, et al. Piperacillin-tazobactam: a beta-lactam/beta-lactamase inhibitor combination. Expert Rev Anti Infect Ther. 2007;5(3):365–83.
Lagacé-Wiens P, Simner P, Tailor F, et al. Activity of ceftazidime (CAZ)/NXL104 (CAZ104) versus CAZ alone and other comparators against 4548 Gram-negative bacilli—results from CANWARD 2009-10 [abstract no. E-1816 plus poster]. In: 51st Annual Interscience Conference on Antimicrobial Agents and Chemotherapy; 2011 Sep 17–20; Chicago (IL).
Lagace-Wiens PR, Tailor F, Simner P, et al. Activity of NXL104 in combination with beta-lactams against genetically characterized Escherichia coli and Klebsiella pneumoniae isolates producing class A extended-spectrum beta-lactamases and class C beta-lactamases. Antimicrob Agents Chemother. 2011;55(5):2434–7.
Levasseur P, Girard AM, Claudon M, et al. In vitro antibacterial activity of the ceftazidime-avibactam (NXL104) combination against Pseudomonas aeruginosa clinical isolates. Antimicrob Agents Chemother. 2012;56(3):1606–8.
Levasseur P, Miossec C, Girard A, et al. In vitro antibacterial activity of ceftazidime (CAZ) in combination with the β-lactamase inhibitor, NXL104 [abstract no. E-186 plus poster]. In: 49th Annual Interscience Conference on Antimicrobial Agents and Chemotherapy; 2009 Sep 12–15; San Francisco (CA).
Livermore DM, Mushtaq S, Warner M, et al. Activities of NXL104 combinations with ceftazidime and aztreonam against carbapenemase-producing Enterobacteriaceae. Antimicrob Agents Chemother. 2011;55(1):390–4.
Mushtaq S, Warner M, Livermore DM. In vitro activity of ceftazidime + NXL104 against Pseudomonas aeruginosa and other non-fermenters. J Antimicrob Chemother. 2010;65(11):2376–81.
Sader H, Castanheira M, Farrell J, et al. Antimicrobial activity of ceftazidime/NXL104 tested against Gram-negative organisms, including multidrug-resistant subjects, causing infections in USA and European medical centers [abstract no. E-811 plus poster]. In: 50th Annual Interscience Conference on Antimicrobial Agents and Chemotherapy; 2010 Sep 12–15; Boston (MA).
Sader H, Farrell D, Bell J, et al. Antimicrobial activity of ceftazidime/NXL104 (CAZ104) tested against Gram-negative organisms causing infections in medical centers from Europe (EU), Latin America (LA) and the Asia-Pacific Region (APAC) [abstract no. C2-1251 plus poster]. In: 51st Annual Interscience Conference on Antimicrobial Agents and Chemotherapy; 2011 Sep 17–20; Chicago (IL).
Sahm D, Pillar C, Brown N, et al. Activity of ceftazidime/NXL104 and select comparators against geographically diverse clinical isolates of Pseudomonas aeruginosa [abstract no. E-194 plus poster]. In: 49th Annual Interscience Conference on Antimicrobial Agents and Chemotherapy; 2009 Sep 12–15; San Francisco (CA).
Tailor F, Lagacé-Wiens P, Simner P, et al. Activity of avibactam (NXL-104) in combination with β-lactams against molecularly characterized AmpC- and ESBL-producing Escherichia coli and Klebsiella pneumoniae for CANWARD 2007–2010 [abstract no. F1-165 plus poster]. In: 51st Annual Interscience Conference on Antimicrobial Agents and Chemotherapy; 2011 Sep 17–20; Chicago (IL).
Walkty A, DeCorby M, Lagace-Wiens PR, et al. In vitro activity of ceftazidime combined with NXL104 versus Pseudomonas aeruginosa isolates obtained from patients in Canadian hospitals (CANWARD 2009 study). Antimicrob Agents Chemother. 2011;55(6):2992–4.
Zhanel GG, Adam HJ, Low DE, et al. Antimicrobial susceptibility of 15,644 pathogens from Canadian hospitals: results of the CANWARD 2007–2009 study. Diagn Microbiol Infect Dis. 2011;69(3):291–306.
Zhanel GG, Sniezek G, Schweizer F, et al. Ceftaroline: a novel broad-spectrum cephalosporin with activity against meticillin-resistant Staphylococcus aureus. Drugs. 2009;69(7):809–31.
Borgonovi M, Merdjan H, Girard A, et al. Importance of NXL104 pharmacokinetics (PK) in the pharmacodynamics (PD) of ceftazidime + NXL104 combinations in an in vitro hollow fiber infection model [abstract no. A-023 plus poster]. In: 48th Annual Interscience Conference on Antimicrobial Agents and Chemotherapy; 2008 Oct 25–28; Washington (DC).
Borgonovi M, Miossec C, Lowther J. The efficacy of ceftazidime combined with NXL104, a novel β-lactamase inhibitor, in a mouse model of kidney infections induced by β-lactamase producing Enterobacteriaceae [abstract no. P794]. Clin Microbiol Infect. 2007;13(Suppl. 2):S199–200. Plus poster presented at 17th European Congress of Clinical Microbiology and Infectious Diseases; 2007 Mar 31–Apr 3; Munich.
Cottagnoud P, Merdjan H, Acosta F, et al. Pharmacokinetics of the new β-lactamase inhibitor NXL104 in an experimental rabbit meningitis model; restoration of the bacteriological efficacy of ceftazidime (CAZ) against a class C producing K. pneumoniae [abstract no. F1-321 plus poster]. In: 47th Annual Interscience Conference on Antimicrobial Agents and Chemotherapy; 2007 Sep 17–20; Chicago (IL).
Levasseur P, Girard A, Delachaume C, et al. NXL104, a novel β-lactamase inhibitor, restores the bactericidal activity of ceftazidime against ESBL and AmpC producing strains of Enterobacteriaceae [abstract no. F-127 plus poster]. In: 46th Annual Interscience Conference on Antimicrobial Agents and Chemotherapy; 2006 Sep 27–30; San Francisco (CA).
Levasseur P, Girard A, Lavallade L, et al. Efficacy of ceftazidime (CAZ)/NXL104 combination in murine septicaemia caused by CTX-M-producing Enterobacteriaceae species [abstract no. A1-005 plus poster]. In: 49th Annual Interscience Conference on Antimicrobial Agents and Chemotherapy; 2009 Sep 12–15; San Francisco (CA).
Levasseur P, Miossec C, Girard A, et al. Use of NXL104, a β-lactamase inhibitor, to detect Klebsiella pneumoniae carbapenemase (KPC) in Enterobacteriaceae [abstract no. D-291b plus poster]. In: 48th Annual Interscience Conference on Antimicrobial Agents and Chemotherapy; 2008 Oct 25–28; Washington (DC).
Livermore DM, Mushtaq S, Warner M, et al. NXL104 combinations versus Enterobacteriaceae with CTX-M extended-spectrum beta-lactamases and carbapenemases. J Antimicrob Chemother. 2008;62(5):1053–6.
Mendes R, Woosley L, Deshpande L, et al. Characterization of resistance mechanisms and epidemiology of Enterobacteriaceae collected during a phase II clinical trial for ceftazidime-avibactam [abstract no. P1676]. Clin Microbiol Infect. 2012;18(Suppl 3):464. Plus poster presented at 22nd European Congress of Clinical Microbiology and Infectious Diseases; 2012 Mar 31–Apr 3; London.
Merdjan H, Girard A, Miossec C, et al. Pharmacokinetics (PK) and efficacy of ceftazidime (CAZ)/NXL104 combination in a murine pneumonia model caused by an AmpC-producing Klebsiella pneumoniae [abstract no. A1-006 plus poster]. In: 49th Annual Interscience Conference on Antimicrobial Agents and Chemotherapy; 2009 Sep 12–15; San Francisco (CA).
Miossec C, Poirel L, Livermore D, et al. In vitro activity of the new β-lactamase inhibitor NXL104: restoration of ceftazidime (CAZ) efficacy against carbapenem-resistant Enterobacteriaceae strains [abstract no. F1-318 plus poster]. In: 47th Annual Interscience Conference on Antimicrobial Agents and Chemotherapy; 2007 Sep 17–20; Chicago (IL).
Mushtaq S, Warner M, Miossec C, et al. NXL104/cephalosporin combinations vs. Enterobacteriaceae with CTX-M ESBLs [abstract no. F1-319 plus poster]. In: 47th Annual Interscience Conference on Antimicrobial Agents and Chemotherapy; 2007 Sep 17–20; Chicago (IL).
Pechereau M, Claudon M, Black M, et al. Activité in vitro de NXL104 sur CTX-M-15 et KPC-2: un nouvel inhibiteur de β-lactamases à spectre étendu (BLSE) et de carbapénèmases de classe A [abstract no. 468 plus poster]. 28ème Réunion Interdisciplinaire de Chimiothérapie Anti-infectieuse; 2008 Dec 3–4; Paris.
Pechereau M, Claudon M, Black M, et al. Activité in vitro de NXL104 sur SHV-4: un nouvel inhibiteur des β-lactamases à spectre étendu [abstract no. 382 plus poster]. 26ème Réunion Interdisciplinaire de Chimiothérapie Anti-infectieuse; 2006 Dec 7–8; Paris.
Shackcloth J, Williams L, Northwood J, et al. In vitro activity of AVE1330A, a novel β-lactamase inhibitor, in combination with aztreonam or ceftazidime against ceftazidime-resistant isolates of species of the Enterobacteriaceae [abstract no. P1571]. Clin Microbiol Infect. 2005;11(Suppl. 2):S511. Plus poster presented at 15th European Congress of Clinical Microbiology and Infectious Diseases; 2005 Apr 2–5; Copenhagen.
Stachyra T, Levasseur P, Pechereau MC, et al. In vitro activity of the {beta}-lactamase inhibitor NXL104 against KPC-2 carbapenemase and Enterobacteriaceae expressing KPC carbapenemases. J Antimicrob Chemother. 2009;64(2):326–9.
Stachyra T, Pechereau M, Petrella S, et al. Activity of the new β-lactamase inhibitor NXL104 against KPC β-lactamases [abstract no. F1-320 plus poster]. In: 47th Annual Interscience Conference on Antimicrobial Agents and Chemotherapy; 2007 Sep 17–20; Chicago (IL).
Weiss W, Pulse M, Endimiani A, et al. Efficacy of NXL104 in combination with ceftazidime in murine infection models [abstract no. B-1339 plus poster]. In: 49th Annual Interscience Conference on Antimicrobial Agents and Chemotherapy; 2009 Sep 12–15; San Francisco (CA).
Citron D, Goldstein E. In vitro activity of NXL104/ceftazidime against β-lactamase producing anaerobic bacteria [abstract no. E-192 plus poster]. In: 49th Annual Interscience Conference on Antimicrobial Agents and Chemotherapy; 2009 Sep 12–15; San Francisco (CA).
Citron DM, Tyrrell KL, Merriam V, et al. In vitro activity of ceftazidime-NXL104 against 396 strains of beta-lactamase-producing anaerobes. Antimicrob Agents Chemother. 2011;55(7):3616–20.
Dubreuil LJ, Mahieux S, Neut C, et al. Anti-anaerobic activity of a new beta-lactamase inhibitor NXL104 in combination with beta-lactams and metronidazole. Int J Antimicrob Agents. 2012;39(6):500–4.
Zhanel G, Brunham R. Third-generation cephalosporins. Can J Hosp Pharm. 1988;41(4):183–94.
Merdjan H, Tarral A, Girard A, et al. Safety, single dose pharmacokinetics, and pharmacodynamics of β-lactamase inhibitor NXL104 in healthy young male adults [abstract no. A-809 plus poster]. In: 47th Annual Interscience Conference on Antimicrobial Agents and Chemotherapy; 2007 Sep 17–20; Chicago (IL).
Felices M, Gualano V, Tarral A, et al. Combined population pharmacokinetic analysis of four phase 1 studies with NXL104 [abstract no. P 1599]. Clin Microbiol Infect. 2010;16(Suppl. 2):S466. Plus poster presented at 20th European Congress of Clinical Microbiology and Infectious Diseases; 2010 Apr 10–13; Vienna.
Li J, Knebel W, Riggs M, et al. Population pharmacokinetic modeling of ceftazidime (CAZ) and avibactam (AVI) in healthy volunteers and patients with complicated intra-abdominal Infection (cIAI) [abstract no. A-634 plus poster]. In: 52nd Annual Interscience Conference on Antimicrobial Agents and Chemotherapy; 2012 Sep 9–12; San Francisco (CA).
Merdjan H, Tarral A, Haazen W, et al. Pharmacokinetics and tolerability of NXL104 in normal subjects and patients with varying degrees of renal insufficiency. [abstract no. P 1598]. Clin Microbiol Infect. 2010;16(Suppl. 2):S465. Plus poster presented at 20th European Congress of Clinical Microbiology and Infectious Diseases; 2010 Apr 10–13; Vienna.
Bowker K, Noel A, MacGowan A. Pharmacodynamics of NXL104 plus either ceftaroline or ceftazidine against an AmpC producing Enterobacter spp [abstract no. A2-556 plus poster]. In: 51st Annual Interscience Conference on Antimicrobial Agents and Chemotherapy; 2011 Sep 17–20; Chicago (IL).
Endimiani A, Hujer KM, Hujer AM, et al. Evaluation of ceftazidime and NXL104 in two murine models of infection due to KPC-producing Klebsiella pneumoniae. Antimicrob Agents Chemother. 2010;55(1):82–5.
Crandon JL, Schuck VJ, Banevicius MA, et al. Comparative in vitro and in vivo efficacy of human simulated exposures of ceftazidime and ceftazidime-avibactam against Pseudomonas aeruginosa. Antimicrob Agents Chemother. 2012;56(12):6137–46.
Lucasti C, Popescu I, Ramesh M, et al. Efficacy and safety of ceftazidime/NXL104 plus metronidazole vs. meropenem in the treatment of complicated intra-abdominal infections in hospitalised adults [abstract no. P1532]. Clin Microbiol Infect. 2011;17(Suppl. 4):S437. Plus poster presented at 21st European Congress of Clinical Microbiology and Infectious Diseases; 2011 May 7–10; Milan.
Vazquez J, González Patzán L, Stricklin D, et al. Efficacy and safety of ceftazidime avibactam versus imipenem cilastatin for complicated urinary tract infections including acute pyelonephritis, in hospitalized adults: results of a prospective investigator-blinded randomized study. Curr Med Res Opin. 2012;28(12):1921–31.
Tarral A, Lipka J, Gyaw S, et al. Effect of age and gender on the pharmacokinetics (PK) and safety of NXL104 in healthy subjects (protocol NXL104/1004) [abstract no. A1-007 plus poster]. In: 49th Annual Interscience Conference on Antimicrobial Agents and Chemotherapy; 2009 Sep 12–15; San Francisco (CA).
Li J, Edeki T, Das S, et al. Effect of a supratherapeutic dose of ceftazidime-avibactam on the QTc interval in a thorough QT study [abstract no. P1417]. Clin Microbiol Infect. 2012;18(Suppl. 3):372. Plus poster presented at 22nd European Congress of Clinical Microbiology and Infectious Diseases; 2012 Mar 31–Apr 3; London.
Acknowledgments
Dr George G. Zhanel has received research funding from AstraZeneca. No other conflicts are reported for the other authors. Chris Lawson was supported by a summer studentship paid in part by the University of Manitoba and AstraZeneca. The authors would like to thank AstraZeneca for their assistance in developing the ceftazidime-avibactam bibliography.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Zhanel, G.G., Lawson, C.D., Adam, H. et al. Ceftazidime-Avibactam: a Novel Cephalosporin/β-lactamase Inhibitor Combination. Drugs 73, 159–177 (2013). https://doi.org/10.1007/s40265-013-0013-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40265-013-0013-7