
Abstract
Background
International Conference on Harmonization of Technical Requirements for Registration of Pharmaceuticals for Human Use (ICH) guidelines emphasize the need for better understanding of the influence of ethnicity on drug response to minimize duplication of clinical studies, thereby expediting drug approval.
Objectives
We have developed a Chinese database for the prediction of differences in the population kinetics of drugs mainly metabolized by cytochromes P450 (CYPs) relative to Caucasian populations. Such predictions should help to inform the need for duplication of in vivo pharmacokinetic studies in the two ethnic groups and the design of such studies.
Methods
Demographic and physiological data for Chinese, along with information on CYP abundances and the frequencies of associated genetic polymorphisms in Chinese, were collated from literature sources and incorporated within the Simcyp Population-based Simulator® (v11.1). Default Simcyp parameter values for a virtual Caucasian population and for model compounds metabolized principally by specific CYPs were used as the point of reference. The drugs and the main CYPs involved in their metabolism were phenacetin (CYP1A2), desipramine (CYP2D6), tolbutamide (CYP2C9), omeprazole (CYP2C19), and alprazolam and midazolam (CYP3A). Hydroxy bupropion formation was used as a more sensitive marker of CYP2B6 activity than bupropion kinetics. Observed plasma drug concentration–time profiles and pharmacokinetic parameters after oral and, where possible, intravenous dosing were obtained from published in vivo studies in both Chinese and Caucasian subjects. Virtual subjects generated within Simcyp were matched to the subjects used in the in vivo studies with respect to age, sex, dosage and, where possible, CYP phenotype frequency. Predicted and observed plasma drug concentrations and weight-normalized clearances were compared between the ethnic groups.
Results
Significant differences were identified between Chinese and Caucasian populations in the frequency of CYP2C19 poor metabolizers (PMs) [Chinese 13 %; Caucasian 2.4 %], CYP2D6 PMs and intermediate metabolizers (IMs) [Chinese PMs 0.3 %, IMs 39 %; Caucasian PMs 8 %, IMs <1 %], the hepatic abundance of CYP2C19 (mean values: Chinese 8 pmol/mg; Caucasian 14 pmol/mg) and liver weight (mean values: Chinese 1198 g; Caucasian 1603 g). The observed plasma drug concentration–time profiles and weight-normalized clearances were predicted with reasonable accuracy (100 % within twofold; 89 % within 1.5-fold) in both ethnic groups. The predicted phenacetin, tolbutamide, omeprazole, desipramine, midazolam (intravenous), midazolam (oral), alprazolam (intravenous) and alprazolam (oral) clearances were 36, 25, 51, 43, 24, 17, 21 and 22 % lower, respectively, in Chinese than in Caucasians; the observed clearances were 28, 2, 75, 42, 19, 62, 20 and 21 % lower, respectively. Predicted and observed formation of hydroxy bupropion was lower in Caucasians than in Chinese (6 and 20 %, respectively). Differences between ethnic groups were less after normalization for body weight.
Conclusion
The results of this study indicate the value of simulation based on mechanistic physiologically based pharmacokinetic modelling (PBPK) in anticipating the likely extent of any differences in the kinetics of CYP substrates in Chinese and Caucasian populations arising from demographic, physiological and genetic differences.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
1 Introduction
The number of clinical drug trials conducted in China doubled between 2000 and 2007 [1], and this country is poised to become the world’s third largest market for pharmaceuticals [2]. However, a lack of harmonization in legislation between regulatory bodies in the USA, Europe and Asia often results in duplication of studies, resulting in lengthy approval times and delayed access to new medicines. A major reason for this delay is concern that there may be significant ethnic differences in pharmacokinetics and pharmacodynamics affecting safety, efficacy and, therefore, dosage [3], resulting in requests for duplication of all or many of the foreign data in populations different from those where the primary clinical development has taken place. With regard to potential pharmacokinetic differences, one way forward is to assess the ability to predict such differences in virtual populations from prior demographic, physiological, genetic and environmental information, using mechanistic physiologically based pharmacokinetic modelling (PBPK), thereby informing the need for and design of real studies [4, 5], While several studies have documented differences in the kinetics of individual drugs between Caucasian and Asian [6] subjects, and in vitro–in vivo extrapolation has been used to predict differences in the clearance of drugs predominantly metabolized by cytochromes P450 (CYPs) between Caucasians and Japanese populations [7], systematic attempts to predict inter-ethnic differences in full plasma drug concentration–time profiles, using PBPK modelling, are lacking. The aim of this study was to determine whether this approach is able to capture any significant differences between Chinese and Caucasians with respect to the pharmacokinetics of model substrates of each of the major human CYPs, namely phenacetin (CYP1A2), bupropion (CYP2B6), tolbutamide (CYP2C9), omeprazole (CYP2C19), desipramine (CYP2D6) and alprazolam and midazolam (CYP3A).
2 Methods
2.1 Model Development
Plasma drug concentration–time profiles in virtual Caucasian and Chinese populations were predicted using the Simcyp Population-based Simulator® (version 11.1), which estimates drug clearance from in vitro data (in vitro–in vivo extrapolation) and distribution from physico-chemical properties and tissue composition, using correlated Monte Carlo methods and a PBPK model [8]. Differential equations describing the kinetics of substrates have been described previously [9]. Although the program allows for a full PBPK model of drug disposition, all organs except for the liver were lumped in the current analysis. Where the drugs investigated were known to undergo complete release from a solid formulation and rapid dissolution following oral dosing, a simple first-order absorption model was used. To estimate intestinal availability (FG), a model of ‘first-pass’ metabolism similar to the ‘well-stirred liver’ [10] was used for CYP2C9, 2C19, 2D6 and 3A substrates (Eq. 1):
where CLuG,int is unbound gut intrinsic clearance. In contrast to the liver model case, the flow term (Qgut) represents nominal blood flow and is a hybrid parameter reflecting the drug absorption rate from the gut lumen, removal of drug from the enterocyte by its blood supply and the volume of enterocytes. The free fraction of drug within the enterocyte is represented by the fugut term, which was assumed to be 1 for all drugs in the current analysis.
For the modelling of drugs dosed in an enteric-coated formulation (omeprazole), the segmental advanced dissolution absorption metabolism (ADAM) model [11] within the Simcyp Simulator® was used. Drug absorption from each segment is described as a function of release from the formulation, dissolution, precipitation, luminal degradation, permeability, metabolism, transport and transit from one segment to the next.
2.1.1 Population Parameters
Based on extensive demographic, physiological and genetic information, the Simcyp Population-based Simulator® allows prediction of pharmacokinetics in North European Caucasian and Japanese populations. Corresponding databases were constructed to extend simulation to Chinese populations. As a basic assumption, the intrinsic catalytic activity per unit amount of enzyme variant was assumed to be the same in Chinese and Caucasians, as was tissue composition. Differences in pharmacokinetics were assumed to manifest through differences in organ size and blood flow (in proportion to body size) and any variability in the abundance of enzymes and the expression of genetic variants. Wherever possible, data from Han Chinese individuals, who constitute about 92 % of the total Chinese population, were used in development of the database. In the absence of Chinese-specific data for a parameter, Japanese data were the primary default. Where Japanese data were not available, data from North European Caucasian individuals were used. The variables and procedures considered in modifying the Caucasian default population to represent the Chinese population were as follows.
2.1.2 Demographics
Data on age, sex, height and weight for 8118 Han Chinese were taken from The China Health and Nutrition Survey 2006 [12], and for 594 healthy Chinese from a volunteer database kindly provided by Pfizer Ltd (Sandwich, UK). The two data sets were analysed separately. The mean ages and weights of the general population were 47 years and 61 kg, respectively, and those of the healthy volunteers were 31 years and 68 kg, respectively; males and females were equally represented in the former, whereas the latter comprised 95 % males. As the female healthy volunteer data set comprised only 31 individuals, a uniform age distribution was assumed. All of the other age distributions were fitted by Weibull functions, and relationships between age, weight and height were sought using both linear and non-linear regression analysis. Yu et al. [13] showed that measured body surface area (BSA) in Chinese adults is compatible with that predicted using the DuBois and DuBois equation [14], which provides the default relationship between height and weight in the Simcyp Simulator®. The average values of BSA of the general Chinese population were 1.73 and 1.55 m2 for males and females, respectively. The average values of BSA of the volunteer Chinese population were 1.79 and 1.56 m2 for males and females, respectively. These values compare with BSA values of 1.95 and 1.75 m2 in healthy male and female Caucasians. Equations used within the Simulator relating height with age, weight with height, and BSA with height and weight have been described previously [15, 16].
2.1.3 Liver Weight
An equation linking liver volume to BSA (liver volume (L/m2) = 0.722 × BSA1.176), developed using data from both Caucasian and Japanese children and adults [17], is incorporated into the Simcyp Simulator® with conversion of liver weight by liver density (1.08 g/L [18]). However, extensive data from the literature indicate that Chinese have significantly smaller livers than Caucasians and Japanese (Fig. 1) [19–22], such that liver weights simulated using the Johnson et al. equation [17] were about 15 % lower than observed values. Therefore, in simulating Chinese populations, a scalar of 0.85 was used for liver volume. Computed tomography was used to measure liver volume in all of the Chinese studies that were identified. These studies were done in equal numbers of males and females. Caucasian and Japanese liver weights were determined at autopsy, using computed tomography or ultrasound techniques. Previous reports have indicated that the measurement of liver volume by ultrasound or computed tomography correlates well with measurements taken at autopsy or after transplantation [17].

2.1.4 Hepatic Blood Flow
Blood flow to individual organs is calculated within the Simcyp Simulator® as a percentage of cardiac output which, in turn, is based upon BSA and age. Portal vein blood flow, measured using either duplex ultrasound or computed tomography, is not significantly different in Chinese and Caucasians [23, 24]. Therefore, Caucasian values of hepatic blood flow expressed as a percentage of cardiac output were assumed in the Chinese population (19 % portal vein, 5.5 % hepatic artery). This resulted in simulated hepatic blood flows that were about 16 % lower in Chinese compared with Caucasians, reflecting the lower BSA in Chinese.
2.1.5 Microsomal Protein
There are currently no data for milligrams of microsomal protein per gram of liver (MPPGL) and milligrams of microsomal protein per intestine (MPPI) and their variability in either Chinese or Japanese. Therefore, age-related values of MPPGL were generated using the relationships determined previously from Caucasian data [25, 26]. MPPI values determined for Caucasians [27] were assumed.
2.1.6 CYP Abundances
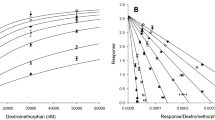
Hepatic abundance values and their variances for specific CYPs in Caucasian and Chinese populations are summarized in Fig. 2a (supplementary data are shown in Table 1 in the Electronic Supplementary Material). The data for Caucasians were compiled by Rowland Yeo et al. [28] and Cubitt et al. [29], and are incorporated into the Simcyp Simulator®. Limited abundance data for Chinese are available for CYPs 1A2, 2C9, 2C19 and 3A4 from Shu et al. [30, 31]. The value for CYP2B6 was assumed to be the same as that in Caucasians, based on the observation of no significant difference in formation of hydroxy bupropion from bupropion by microsomes prepared from 30 Caucasian and 30 Chinese livers [32]. The study by Yang et al. [32] also reported no significant difference in the formation of dextrorphan from the CYP2D6 probe substrate dextromethorphan in the same liver microsomal samples. However, lower CYP2D6 expression in Japanese [33] and decreased in vivo conversion of morphine to codeine in Chinese compared with Caucasians [34] have been reported. Due to uncertainty in this parameter, the following assumptions were investigated: (a) CYP2D6 abundance in Chinese is 70 % of that in Caucasians; and (b) CYP2D6 abundance in Chinese is the same as that in Caucasians. The relationship between hepatic CYP3A4 and CYP3A5 expression reported previously for Caucasians [35] was used to generate values of CYP3A5 abundance in the Chinese populations. No data are available regarding intestinal CYP abundances in Chinese. Therefore, the relationship between Caucasian and Chinese hepatic CYP abundances was applied to reported Caucasian intestinal CYP abundances [27, 36] to estimate those in Chinese (Fig. 2b; see also the supplementary data in Table 2 in the Electronic Supplementary Material). Variability in Chinese intestinal CYP abundance was assumed to be the same as that in Caucasian individuals (CV 60 %).

Comparison of mean a hepatic and b gut cytochrome P450 (CYP) abundance values in Caucasian individuals (black bars) and in Chinese individuals (grey bars). With the exception of CYP2D6 levels (indicated by a triangle) and CYP2B6 levels in Chinese (indicated by an asterisk), which were estimated from relative in vitro and in vivo CYP activity in Caucasian and Chinese individuals, all hepatic abundance values were determined by Western blotting. Uncertainty in the values of hepatic CYP2D6 abundance resulted in the investigation of two values. Caucasian gut abundance values were also determined by Western blotting. Owing to a lack of experimental data, Chinese gut abundances were estimated as described in Sect. 2.1. A full bibliography of the studies used to compile the abundance data is provided in Tables 1 and 2 in the Electronic Supplementary Material
2.1.7 CYP Phenotype Frequencies
Frequencies of genetic variants of CYP2B6, CYP2C9, CYP2C19, CYP2D6 and CYP3A5 in Caucasians were provided in the Simcyp Simulator® as documented from Lamba et al. [37], Scordo et al. [38], Zackrisson et al. [39] and Lin et al. [40]. These values are summarized in Fig. 3 (supplementary data are shown in Table 3 in the Electronic Supplementary Material), along with Chinese values obtained by meta-analysis of literature data.

Comparison of cytochrome P450 (CYP) polymorphism frequencies in Caucasians and Chinese. Phenotype frequencies [purple: ultra-rapid metabolizer (UM); green: extensive metabolizer (EM); red: intermediate metabolizer (IM); blue: poor metabolizer (PM)] are expressed as percentages. A full bibliography of the studies used to compile the data is provided in Table 3 in the Electronic Supplementary Material
Common genotypes for CYP2B6, 2C9, 2C19, 2D6 and 3A5 were assigned to poor metabolizer (PM), intermediate metabolizer (IM) or ultra-rapid metabolizer (UM) phenotypes in both populations. PM phenotypes were assigned as follows: CYP2B6 *5/*5, *5/*6 and *6/*6; CYP2C9 and CYP2C19 *2/*2, *2/*3 and *3/*3; any CYP2D6 genotype containing a *3, *4, *5, *6, *7, *8, *11, *14, *15, *19 or *20 allele; and CYP3A5 *3/*3. Individuals having CYP2D6 *9, *10, *17, *29, *36 or *41 alleles were assigned as IM phenotype. Individuals with duplicate CYP2D6 EM alleles were assigned a UM phenotype. All remaining genotypes were assumed to translate to an extensive metabolizer (EM) phenotype.
2.1.8 Plasma Proteins
The ratio of mean plasma α1-acid glycoprotein (AAG) concentrations in Chinese and Caucasian males, reported by Zhou et al. [41] (0.62:0.77 g/L), was applied to male Caucasian values of AAG concentrations (mean 0.811 g/L) within the Simcyp Simulator® to provide Chinese values. Female Chinese values were estimated using the previously established relationship in Caucasians (females having a 2.5 % lower AAG concentration than males). As the variability in AAG reported by Zhou et al. [41] was the same for Chinese and Caucasians, the coefficient of variation (CV) of 15 % for males and 13 % for females, previously applied in the Caucasian database, was also applied in the Chinese database. Since Zhou et al. [41] found no differences in serum albumin levels between Chinese and Caucasians, the Caucasian values were used by default.
2.1.9 Haematocrit
A study by Miao et al. [42] of different Chinese populations reported haematocrit values of 45 and 41 % in males and females from the northern (Beijing) area of China. These values are similar to the values of 43 and 38 % for male and female Caucasian individuals, respectively.
2.1.10 Renal Function
The glomerular filtration rate is calculated within the Simcyp Simulator® from age, weight and serum creatinine levels, either using the Cockcroft–Gault equation or the modified diet in renal disease (MDRD) equation [43, 44]. The length of the kidney has been reported to be similar in Chinese and Caucasians [45]. In addition, Yue et al. [34] showed no significant differences in the weight-normalized renal clearances of codeine and its metabolites in healthy Chinese and Caucasians. Therefore, Caucasian values for the simulation of population renal clearances were applied to the Chinese population. This resulted in simulated glomerular filtration rates 12 % lower in Chinese than in Caucasians, reflecting the lower body weight of Chinese.
2.2 Model Application
2.2.1 Prediction of Plasma Drug Concentration–Time Profiles
The model was tested using drugs metabolized predominantly by specific CYPs with minimal impact of transporters and low biliary and renal clearances [phenacetin (CYP1A2); bupropion (CYP2B6); tolbutamide (CYP2C9); omeprazole (CYP2C19); desipramine (CYP2D6), alprazolam and midazolam (CYP3A)] and for which predictions could be compared against available in vivo data obtained following either intravenous and/or oral administration in both Caucasian and Chinese subjects. Observed pharmacokinetic data were selected using the PubMed online database. The initial criteria for selection included only studies performed in both Caucasian and Chinese healthy volunteer subjects. However, due to a scarcity of studies, the inclusion criteria were widened to include comparison of data from unmatched studies. Compound files established within the Simcyp Simulator® (v.11.1) verified to simulate the kinetics of phenacetin, tolbutamide, omeprazole, alprazolam and midazolam in Caucasian populations were used. The main CYP enzyme and its contribution to the clearance of each model substrate is listed in Table 1.
Modifications were made to the Simcyp compound file for bupropion in order to accommodate administration of a sustained-release formulation and modelling of its hydroxy metabolite (produced mainly by CYP2B6) [46, 47]. An additional sulphation pathway for desipramine was incorporated into the file for this compound [48, 49]. The use of in vitro metabolism data has been shown previously to result in significant overprediction of the observed clearance of alprazolam [29]. Therefore, a top-down approach involving estimation of CYP3A4 intrinsic clearance from in vivo clearance data [50–52] was applied. For midazolam, the single adjusting compartment (SAC) in the Simcyp Simulator® was included in the PBPK model in order to improve recovery of the plasma drug concentration–time profile. Details of the modified metabolic parameters for hydroxy bupropion, desipramine and alprazolam and modified distribution parameters for midazolam used in the models are shown in Table 4 in the Electronic Supplementary Material. Simulations in Chinese and Caucasian individuals differed with respect to system parameters only, as described in Sect. 2.1; drug data within the compound files were identical for both sets of simulations. Simulations were run in Chinese and Caucasian healthy volunteers matched to those used in the in vivo studies with respect to the numbers of subjects, age range and sex. Where information on the CYP genotype or phenotype of individuals was available, the frequencies were used in the simulations. In those cases where information on CYP genetic polymorphism frequency was lacking, population frequencies (shown in Table 3 in the Electronic Supplementary Material) were used. Details of the number of subjects, age range, sex, weight, dose and dosage route for each in vivo study are shown in Table 5 in the Electronic Supplementary Material. For each simulation, ten separate trials were generated to assess variability across groups.
The outcomes of simulations of the kinetics of midazolam and omeprazole were compared for the general Chinese population and the healthy Chinese volunteer group. For the general Chinese population, two thousand male subjects, ranging in age from 20 to 70 years, were simulated. All subjects were EMs of CYP2C19, and 39 % were EMs of CYP3A5.
2.2.2 Phenacetin
Simulated plasma drug concentration–time profiles were compared with those reported from an in vivo study of 20 Chinese (8 female; 26 ± 5 years) and 20 Caucasians (6 female; 25 ± 4 years) [53].
2.2.3 Bupropion
Simulated plasma bupropion and hydroxy bupropion area under the plasma concentration–time curve (AUC) and maximum concentration (Cmax) values were compared with those from an in vivo study of 9 Chinese (20–32 years) and 9 Caucasian males (19–23 years) [54]. All individuals in the in vivo study had CYP2B6 genotypes associated with an EM phenotype.
2.2.4 Tolbutamide
No studies were identified in the literature that directly compared the kinetics of tolbutamide in Chinese and Caucasians. Therefore, simulated plasma drug concentration–time profiles were compared with those reported separately for 10 Chinese CYP2C9*1*1 (EMs; 3 female; 35 ± 4 years) [55] and 14 Caucasian males (21–30 years) of unknown CYP2C9 geno/phenotype [56]. The CYP2C9 PM and EM frequencies for Caucasians within the Simcyp Population Library were assumed (see Table 3 in the Electronic Supplementary Material).
2.2.5 Omeprazole
No suitable studies were identified in the literature that directly compared the kinetics of omeprazole in Chinese and Caucasians. Therefore, simulated plasma drug concentration–time profiles were compared with those reported separately for 12 Chinese (23 ± 2 years) [57] and 12 Caucasian males (22–32 years) [58]. Both of these studies recruited healthy EMs of CYP2C19.
2.2.6 Desipramine
Simulated plasma drug concentration–time profiles were compared with those reported for an in vivo study with 14 Chinese (7 female; 19–55 years) and 16 Caucasians (8 female; 22–58 years) [59]. All individuals in this study showed a level of desipramine hydroxylation. Therefore, it was assumed that no CYP2D6 PMs were included in the study. CYP2D6 IM, EM and UM frequencies of 0.28, 0.72 and 0, respectively, in virtual Chinese subjects and 0, 0.75 and 0.25, respectively, in virtual Caucasian subjects were assigned based on the trimodal distribution of desipramine clearance reported in the study. For CYP2D6 abundance, two assumptions were investigated: (a) CYP2D6 abundance in Chinese is 70 % that in Caucasians; and (b) CYP2D6 abundance in Chinese is the same as that in Caucasians (Fig. 2).
2.2.7 Alprazolam
Simulated plasma concentration–time profiles of alprazolam were compared with those reported for an in vivo study with 10 Chinese, 3 Filipino and 1 Japanese individual (25–35 years) and 14 Caucasian males (20–30 years) [50]. The CYP3A5 PM and EM frequencies for Caucasians and Chinese within the Simcyp Population Library were assumed.
2.2.8 Midazolam
No studies were identified in the literature that directly compared the kinetics of midazolam in Chinese and Caucasians. However, separate reports of midazolam kinetics in Chinese and Caucasian following intravenous and oral dosing were collated from the literature. Simulated dose-normalized plasma drug concentration–time profiles following intravenous dosing of midazolam were compared with those reported separately for 22 Chinese males (age 20–28 years; 27 % CYP3A5 EMs) [60] and 39 Caucasians (12 female; age 19–41 years; unknown CYP3A5 geno/phenotypes) [61–64]. The CYP3A5 PM and EM frequencies for Caucasians within the Simcyp Population Library were assumed.
Simulated dose-normalized plasma drug concentration–time profiles following oral dosing of midazolam were compared with those reported separately for 76 Chinese males (age 19–31 years; 39 % CYP3A5 EMs) [60, 65–67] and 65 Caucasians (24 female; age 18–41 years; unknown CYP3A5 geno/phenotypes) [61–64, 68–70]. The CYP3A5 PM and EM frequencies for Caucasians within the Simcyp Population Library were assumed.
2.3 Statistical Analysis
Clearance data were analysed with and without correction for body weight. The frequency distributions of simulated clearance values were consistent with a log-normal (Ln) distribution. Hence, values of geometric mean (GM) clearance (CL) and 95 % confidence intervals (CIs) were calculated from the log-transformed data [population mean of μ and standard deviation (SD) of σ].
Two of the clinical studies also reported data in terms of the GM and CI. For comparison purposes, data published as mean values and SDs were transformed into GMs and 95 % CIs, using Eqs. 2–5.
Ratios (± SDs) of drug clearance in Caucasians relative to Chinese were defined by Eq. 6.
where the CV is calculated by Eq. 7.
90 % CIs for the ratios were calculated using Eq. 8.
Differences between ethnic groups were deemed significant if the 90 % CI of the ratio data did not include unity.
3 Results
3.1 Demography
The demography of simulated individuals was consistent with observed data for both male healthy volunteers and the general male and female Chinese populations (Figs. 4, 5). Although the size of the female healthy volunteer cohort (n = 31) precluded a robust assessment of model performance, the age range of virtual healthy female individuals was in agreement with the observed data. Height and weight relationships generated using the Simcyp models were also in line with the observed data.

Simulated age distributions (black bars) [n = 1000] and observed age distributions (grey bars) [n = 8118] in a general Chinese population (a male, b female), and simulated relationships (circle symbols) and observed relationships (cross symbols) between height and age (male c, female d) and between weight and height (male e, female f)

Simulated age distributions (black bars) and observed age distributions (grey bars) [n = 594] in a cohort of healthy Chinese volunteers (a male, b female), and simulated relationships (circle symbols) and observed relationships (cross symbols) between height and age (male c, female d) and between weight and height (male e, female f)
3.2 Simulation of Plasma Drug Concentration–Time Profiles
Simulated and observed plasma concentration–time profiles are shown in Figs. 6, 7 and 8.

Simulated mean plasma concentration–time profiles (data lines) and observed mean plasma concentration–time profiles (data points) of phenacetin, tolbutamide, omeprazole and desipramine in healthy Caucasian and Chinese individuals after oral dosage. The grey lines represent simulations of individual trials (10 × study number). The dotted lines represent the 5th and 95th percentiles for the total virtual population. The observed data are from Bartoli et al. [53] (phenacetin); Madsen et al. [56] and Chen et al. [55] (tolbutamide); Andersson et al. [58] and Hu et al. [57] (omeprazole); and Rudorfer et al. [59] (desipramine). CYP cytochrome P450, EM extensive metabolizer, IM intermediate metabolizer, PM poor metabolizer, UM ultra-rapid metabolizer

Simulated dose-normalized mean plasma concentration–time profiles (data lines) and observed dose-normalized mean plasma concentration–time profiles (data points) of alprazolam in healthy Caucasian subjects (a, c) and in Chinese subjects (b, d) after intravenous dosing (a, b) and after oral dosing (c, d). The grey lines represent simulations of individual trials (10 × study number). The dotted lines represent the 5th and 95th percentiles for the total virtual population. The observed data are from Lin et al. [50]. CYP cytochrome P450, PM poor metabolizer

Simulated dose-normalized mean plasma concentration–time profiles (data lines) and observed dose-normalized mean plasma concentration–time profiles (data points) of midazolam in healthy Caucasian subjects (a, c) and in Chinese subjects (b, d) after intravenous dosing (a, b) and after oral dosing (c, d). The grey lines represent simulations of individual trials (10 × study number). The dotted lines represent the 5th and 95th percentiles for the total virtual population. The observed data are from Kharasch et al. [61], Kupferschmidt et al. [62], Tsunoda et al. [63], Mandema et al. [64], Backman et al. [68], Fayer et al. [69] and Olkkola et al. [70] (a, c); and from Yang et al. [60], Guo et al. [65], Shih and Huang [66] and Duan et al. [67] (b, d). CYP cytochrome P450, PM poor metabolizer
Use of the Simcyp dynamic minimal PBPK model resulted in reasonable recovery of reported plasma concentration–time profiles for phenacetin, tolbutamide, omeprazole, desipramine and midazolam in both Caucasian and Chinese healthy volunteer subjects. The Cmax of alprazolam after oral administration was under-predicted, but its AUC values following both intravenous and oral dosing were recovered accurately. Plasma hydroxy bupropion concentration–time profiles were not reported in the study by Loboz et al. [54]. However, the simulated GM hydroxy bupropion AUC from time zero to infinity (AUC∞) values of 13.2 and 12.4 μg·h/mL for Chinese and Caucasian individuals, respectively, were in good agreement with the reported values of 15.2 and 12.7 μg·h/mL, respectively [54]. The predicted Cmax values of hydroxy bupropion were 304 and 235 ng/mL for Chinese and Caucasians, respectively, compared with observed values of 400 and 354 ng/mL, respectively.
3.3 Prediction of Clearance
With the exception of the predicted oral clearances of omeprazole and midazolam in Chinese healthy volunteers (2.1- and 2.0-fold over-prediction, respectively), the predicted values of clearance (or AUC in the case of hydroxy bupropion) were within 1.5-fold of observed values for all of the other model CYP substrates (see Table 5 in the Electronic Supplementary Material) in both populations. Use of a CYP2D6 abundance value of 8 pmol per mg in Chinese (the same value used for the Caucasian population) resulted in a more accurate prediction of desipramine clearance compared with predictions made using the lower value of 5.5 pmol per mg. After normalization for body weight, all predicted clearances were within 2-fold of the observed values and 89 % of the predictions were within 1.5-fold.
3.4 Caucasian:Chinese Clearance Ratios
Simulated and observed GM ratios of Caucasian and Chinese plasma clearances (and the ratio for the AUC of hydroxy bupropion) are shown in Fig. 9.

Simulated geometric mean (GM) fold differences (white data points) and observed GM fold differences (black data points) in a clearance (CL) and b weight-normalized CL between healthy Caucasian and Chinese subjects ±90 % confidence intervals (CIs). Those ratios where the 90 % CIs do not include 1 are indicated by an asterisk. Further details of the data are given in Table 5 in the Electronic Supplementary Material. i.v. intravenous, p.o. oral
With the exception of the observed and predicted ratios for hydroxy bupropion, tolbutamide and alprazolam (intravenous) and the predicted ratio for alprazolam (oral), values significantly greater than 1 were observed. Following correction for body weight, only differences in the ratios for omeprazole (observed and predicted) and oral midazolam (observed) remained significantly different from 1. With the exception of omeprazole, hydroxy bupropion, tolbutamide and orally dosed midazolam (1.5-fold under-prediction, 3.1-fold under-prediction, 11.6-fold over-prediction and 3.7-fold over-prediction, respectively), the predicted percentage differences in clearance (or AUC in the case of hydroxy bupropion) between Chinese and Caucasians were within 1.5-fold of observed values for all of the other model CYP substrates (Table 2). The corresponding weight-normalized values of differences in clearance are also provided in Table 2. The observed and predicted variances in the ratios were generally similar.
Although the predicted geometric mean oral clearances of midazolam and omeprazole were similar in the general virtual Chinese population compared with those in the healthy Chinese volunteer virtual population [65 (95 % CI 8–1026) vs. 81 (95 % CI 10–450) L/h and 25 (95 % CI 6–118) vs. 29 (95 % CI 8–100) L/h, respectively], they were significantly different by t test (p = 0.007 and 0.003, respectively) (Fig. 10).

Comparison of simulated (a) midazolam clearance (CL) and (b) omeprazole CL after oral dosage in a general Chinese virtual population and in a healthy Chinese volunteer virtual population. The data points represent geometric mean values and the error bars represent minimum and maximum values
4 Discussion and Conclusion
Studies exploring ethnic differences in pharmacokinetics often fail to consider Japanese, Korean and Chinese individuals as distinct ethnic groups, instead combining data and reporting results for an ‘Asian’ population. The current study focussed on the development of a specific Chinese population database. Key differences identified between Chinese and Caucasians were those in liver size, the frequency of allelic variants of CYPs 2D6 and 2C19 and the hepatic abundance of CYP2C19. The available data also indicated that Chinese individuals have smaller liver volumes than Japanese individuals. Across the compounds chosen to mark each main individual CYP, the predicted mean percentage difference in clearance (uncorrected for body weight) was 26 % (range −6 to 51 %) compared with a value of 28 % (range −20 to 75 %) for observed data. Data collation focussed on parameters required for the prediction of clearance and, although the model recovered the mean percentage difference in clearance, some deviations from the observed plasma concentration–time profiles in Chinese and hence percentage differences in clearance were noted, particularly for tolbutamide, omeprazole and orally dosed midazolam. Differences in absorption and distribution parameters in the Chinese population were assumed to manifest through differences in organ size and blood flow (in proportion to body size). Other potential differences that may influence absorption and distribution parameters such as the intestinal transit time, stomach emptying time, formulation differences and non-body-size–related variation in organ size and blood flow were not considered in the model and may explain differences between simulated and observed values of Cmax and time to reach Cmax (tmax).
Consistent with reportedly lower hepatic CYP2C9 abundance [31], in vitro activity [32] and liver size, the Simcyp model predicted a 25 % lower tolbutamide clearance in Chinese relative to Caucasians. Although observed tolbutamide data reported by Chen et al. [55] and phenytoin data (not shown) indicate comparable in vivo clearance in Chinese and Caucasians, a study by Gross et al. [71], involving ethnic Chinese individuals living in Australia, reported a 29 % lower tolbutamide clearance in Chinese relative to Caucasians. Based on data from Andersson et al. [58] and Hu et al. [57], the model underestimated differences in omeprazole clearance between Chinese and Caucasians. However, smaller differences (1.4-fold lower) have been reported by Caraco et al. [72] and Zhang et al. [73] for the CYP2C19 substrates omeprazole and diazepam. Clinical studies aimed at comparing the kinetics of CYP3A4 substrates such as alprazolam [50], adinazolam [74], reboxetine [75], nifedipine and erythromycin [76] have reported variable results ranging from no significant ethnic difference to 65 % higher clearances in Caucasians than in Chinese. Generally, smaller differences have been observed following intravenous administration compared with oral dosing, and larger differences with increasing CYP3A clearance and thus gut first-pass metabolism (nifedipine and erythromycin > alprazolam and reboxetine). Given the knowledge gaps in Chinese gut physiology and enzymology highlighted previously, it is perhaps not surprising that the model appears to more accurately predict the pharmacokinetics of a low-clearance CYP3A substrate (alprazolam) than that of a higher-clearance substrate (midazolam) after oral dosing.
In addition to the limited size of studies documenting hepatic enzyme abundance in Chinese, other limitations associated with the predictions include incomplete information on the abundances of all of the enzymes in Chinese, the fact that there are relatively few published reports comparing the kinetics of the model drugs in both Chinese and Caucasians within the same study, the inability to separate Chinese individuals from individuals of other Asian origin in some studies [51] and appreciable inter-study variability in the outcome of some of the real studies (especially those with midazolam in Chinese). Nevertheless, the analysis provides some expectation that the prediction of any significant pharmacokinetic differences between Chinese and Caucasians for other drugs (including new compounds) metabolized by a mix of the various CYPs can usefully inform the need for and design of real pharmacokinetic bridging studies. In extending the current study, it will be important to consider differences in drug metabolism by phase II enzymes, differences in the abundances and activity of drug transporters, and the impact of differences in diet and exposure to herbal and other traditional Chinese medicines. Further evaluation of the significance of possible differences in tissue composition and in the physiology of the gastrointestinal tract is also indicated.
References
Kudrin A. Challenges in the clinical development requirements for the marketing authorization of new medicines in southeast Asia. J Clin Pharmacol. 2009;49(3):268–80.
Emerging pharmaceutical market in China—forecast to become the world’s third-largest pharmaceutical market by 2013. http://www.marketresearch.com/GBI-Research-v3759/Emerging-Pharmaceutical-China-Forecast-Largest-6564799/. Accessed 23 May 2013.
Malinowski HJ, Westelinck A, Sato J, Ong T. Same drug, different dosing: differences in dosing for drugs approved in the United States, Europe, and Japan. J Clin Pharmacol. 2008;48(8):900–8.
Rostami-Hodjegan A, Tucker GT. Simulation and prediction of in vivo drug metabolism in human populations from in vitro data. Nat Rev Drug Discov. 2007;6(2):140–8.
Rowland M, Peck C, Tucker G. Physiologically-based pharmacokinetics in drug development and regulatory science. Annu Rev Pharmacol Toxicol. 2011;51:45–73.
Kim K, Johnson JA, Derendorf H. Differences in drug pharmacokinetics between East Asians and Caucasians and the role of genetic polymorphisms. J Clin Pharmacol. 2004;44(10):1083–105.
Inoue S, Howgate EM, Rowland-Yeo K, Shimada T, Yamazaki H, Tucker GT, et al. Prediction of in vivo drug clearance from in vitro data. II: Potential inter-ethnic differences. Xenobiotica. 2006;36(6):499–513.
Jamei M, Marciniak S, Feng K, Barnett A, Tucker G, Rostami-Hodjegan A. The Simcyp population-based ADME simulator. Expert Opin Drug Metab Toxicol. 2009;5(2):211–23.
Rowland Yeo K, Jamei M, Yang J, Tucker GT, Rostami-Hodjegan A. Physiologically based mechanistic modelling to predict complex drug–drug interactions involving simultaneous competitive and time-dependent enzyme inhibition by parent compound and its metabolite in both liver and gut—the effect of diltiazem on the time-course of exposure to triazolam. Eur J Pharm Sci. 2010;39(5):298–309.
Rostami-Hodjegan A, Tucker GT. ‘In silico’ simulations to assess the ‘in vivo’ consequences of ‘in vitro’ metabolic drug–drug interactions. Drug Discov Today Technol. 2004;1:441–8.
Jamei M, Turner D, Yang J, Neuhoff S, Polak S, Rostami-Hodjegan A, et al. Population-based mechanistic prediction of oral drug absorption. AAPS J. 2009;11(2):225–37.
CHNS. China Health and Nutrition Survey. http://www.cpc.unc.edu/projects/china. Accessed 23 May 2013.
Yu CY, Lo YH, Chiou WK. The 3D scanner for measuring body surface area: a simplified calculation in the Chinese adult. Appl Ergon. 2003;34(3):273–8.
DuBois D, DuBois E. A formula to estimate the approximate surface area if height and weight be known. Arch Intern Med. 1916;17:863.
Howgate EM, Rowland Yeo K, Proctor NJ, Tucker GT, Rostami-Hodjegan A. Prediction of in vivo drug clearance from in vitro data. I: Impact of inter-individual variability. Xenobiotica. 2006;36(6):473–97.
Jamei M, Dickinson GL, Rostami-Hodjegan A. A framework for assessing inter-individual variability in pharmacokinetics using virtual human populations and integrating general knowledge of physical chemistry, biology, anatomy, physiology and genetics: a tale of ‘bottom-up’ vs ‘top-down’ recognition of covariates. Drug Metab Pharmacokinet. 2009;24(1):53–75.
Johnson TN, Tucker GT, Tanner MS, Rostami-Hodjegan A. Changes in liver volume from birth to adulthood: a meta-analysis. Liver Transplant. 2005;11(12):1481–93.
Heinemann A, Wischhusen F, Puschel K, Rogiers X. Standard liver volume in the Caucasian population. Liver Transplant Surg. 1999;5(5):366–8.
Chan SC, Liu CL, Lo CM, Lam BK, Lee EW, Wong Y, et al. Estimating liver weight of adults by body weight and gender. World J Gastroenterol. 2006;12(14):2217–22.
Shi ZR, Yan LN, Li B, Wen TF. Evaluation of standard liver volume formulae for Chinese adults. World J Gastroenterol. 2009;15(32):4062–6.
Yuan D, Lu T, Wei YG, Li B, Yan LN, Zeng Y, et al. Estimation of standard liver volume for liver transplantation in the Chinese population. Transplant Proc. 2008;40(10):3536–40.
Fu-Gui L, Lu-Nan Y, Bo L, Yong Z, Tian-Fu W, Ming-Qing X, et al. Estimation of standard liver volume in Chinese adult living donors. Transplant Proc. 2009;41(10):4052–6.
Chou YH, Tiu CM, Pan HB, Chang T, Su YG. The measurement of spleno-portal venous and hepatic arterial blood flow in normal adults using duplex ultrasound—a preliminary report. Chin Med J. 1985;35:343–9.
Li J, Yang J, Jiang L. Hepatic blood flow in liver: clinical application of CT dynamic perfusion. J Clin Radiol. 2005;24(2):130–4.
Barter ZE, Bayliss MK, Beaune PH, Boobis AR, Carlile DJ, Edwards RJ, et al. Scaling factors for the extrapolation of in vivo metabolic drug clearance from in vitro data: reaching a consensus on values of human microsomal protein and hepatocellularity per gram of liver. Curr Drug Metab. 2007;8(1):33–45.
Barter ZE, Chowdry JE, Harlow JR, Snawder JE, Lipscomb JC, Rostami-Hodjegan A. Covariation of human microsomal protein per gram of liver with age: absence of influence of operator and sample storage may justify interlaboratory data pooling. Drug Metab Dispos. 2008;36(12):2405–9.
Paine MF, Khalighi M, Fisher JM, Shen DD, Kunze KL, Marsh CL, et al. Characterization of interintestinal and intraintestinal variations in human CYP3A-dependent metabolism. J Pharmacol Exp Ther. 1997;283(3):1552–62.
Rowland Yeo K, Rostami-Hodjegan A, Tucker GT. Abundance of cytochromes P450 in human liver: a meta-analysis. Br J Clin Pharmacol. 2004;57:687–8.
Cubitt HE, Yeo KR, Howgate EM, Rostami-Hodjegan A, Barter ZE. Sources of interindividual variability in IVIVE of clearance: an investigation into the prediction of benzodiazepine clearance using a mechanistic population-based pharmacokinetic model. Xenobiotica. 2011;41(8):623–38.
Shu Y, Wang LS, Xiao WM, Wang W, Huang SL, Zhou HH. Probing CYP2C19 and CYP3A4 activities in Chinese liver microsomes by quantification of 5-hydroxyomeprazole and omeprazole sulphone. Acta Pharmacol Sin. 2000;21(8):753–8.
Shu Y, Cheng ZN, Liu ZQ, Wang LS, Zhu B, Huang SL, et al. Interindividual variations in levels and activities of cytochrome P-450 in liver microsomes of Chinese subjects. Acta Pharmacol Sin. 2001;22(3):283–8.
Yang J, He MM, Niu W, Wrighton SA, Li L, Liu Y, et al. Metabolic capabilities of cytochrome P450 enzymes in Chinese liver microsomes compared with those in Caucasian liver microsomes. Br J Clin Pharmacol. 2012;73(2):268–84.
Shimada T, Yamazaki H, Mimura M, Inui Y, Guengerich FP. Interindividual variations in human liver cytochrome P-450 enzymes involved in the oxidation of drugs, carcinogens and toxic chemicals: studies with liver microsomes of 30 Japanese and 30 Caucasians. J Pharmacol Exp Ther. 1994;270(1):414–23.
Yue QY, Svensson JO, Sjoqvist F, Sawe J. A comparison of the pharmacokinetics of codeine and its metabolites in healthy Chinese and Caucasian extensive hydroxylators of debrisoquine. Br J Clin Pharmacol. 1991;31(6):643–7.
Barter ZE, Perrett HF, Yeo KR, Allorge D, Lennard MS, Rostami-Hodjegan A. Determination of a quantitative relationship between hepatic CYP3A5*1/*3 and CYP3A4 expression for use in the prediction of metabolic clearance in virtual populations. Biopharm Drug Dispos. 2010;31(8–9):516–32.
Paine MF, Hart HL, Ludington SS, Haining RL, Rettie AE, Zeldin DC. The human intestinal cytochrome P450 “pie”. Drug Metab Dispos. 2006;34(5):880–6.
Lamba V, Lamba J, Yasuda K, Strom S, Davila J, Hancock ML, et al. Hepatic CYP2B6 expression: gender and ethnic differences and relationship to CYP2B6 genotype and CAR (constitutive androstane receptor) expression. J Pharmacol Exp Ther. 2003;307(3):906–22.
Scordo MG, Aklillu E, Yasar U, Dahl ML, Spina E, Ingelman-Sundberg M. Genetic polymorphism of cytochrome P450 2C9 in a Caucasian and a black African population. Br J Clin Pharmacol. 2001;52(4):447–50.
Zackrisson AL, Holmgren P, Gladh AB, Ahlner J, Lindblom B. Fatal intoxication cases: cytochrome P450 2D6 and 2C19 genotype distributions. Eur J Clin Pharmacol. 2004;60(8):547–52.
Lin YS, Dowling AL, Quigley SD, Farin FM, Zhang J, Lamba J, et al. Co-regulation of CYP3A4 and CYP3A5 and contribution to hepatic and intestinal midazolam metabolism. Mol Pharmacol. 2002;62(1):162–72.
Zhou HH, Adedoyin A, Wilkinson GR. Differences in plasma binding of drugs between Caucasians and Chinese subjects. Clin Pharmacol Ther. 1990;48(1):10–7.
Miao G, Yan Y, Chuanmin Z, Naiying L. Discussion on the relationship between normal hematocrit and geographical factors in China. Clin Hemorheol Microcirc. 1997;17(6):459–65.
Cockcroft DW, Gault MH. Prediction of creatinine clearance from serum creatinine. Nephron. 1976;16(1):31–41.
Levey AS, Bosch JP, Lewis JB, Greene T, Rogers N, Roth D. A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Modification of Diet in Renal Disease Study Group. Ann Intern Med. 1999;130(6):461–70.
Hsiu K. Kidney size in normal Chinese adults: assessment by renosonogram and plain roentgenogram. Chang Gung Med J. 1983;6:93–9.
Hesse LM, Venkatakrishnan K, Court MH, von Moltke LL, Duan SX, Shader RI, et al. CYP2B6 mediates the in vitro hydroxylation of bupropion: potential drug interactions with other antidepressants. Drug Metab Dispos. 2000;28(10):1176–83.
Kirchheiner J, Klein C, Meineke I, Sasse J, Zanger UM, Murdter TE, et al. Bupropion and 4-OH-bupropion pharmacokinetics in relation to genetic polymorphisms in CYP2B6. Pharmacogenetics. 2003;13(10):619–26.
Romiti P, Giuliani L, Pacifici GM. Interindividual variability in the N-sulphation of desipramine in human liver and platelets. Br J Clin Pharmacol. 1992;33(1):17–23.
Senggunprai L, Yoshinari K, Yamazoe Y. Selective role of sulfotransferase 2A1 (SULT2A1) in the N-sulfoconjugation of quinolone drugs in humans. Drug Metab Dispos. 2009;37(8):1711–7.
Lin KM, Lau JK, Smith R, Phillips P, Antal E, Poland RE. Comparison of alprazolam plasma levels in normal Asian and Caucasian male volunteers. Psychopharmacology. 1988;96(3):365–9.
Fleishaker JC, Phillips JP, Eller MG, Smith RB. Pharmacokinetics and pharmacodynamics of alprazolam following single and multiple oral doses of a sustained-release formulation. J Clin Pharmacol. 1989;29(6):543–9.
Smith RB, Kroboth PD, Vanderlugt JT, Phillips JP, Juhl RP. Pharmacokinetics and pharmacodynamics of alprazolam after oral and IV administration. Psychopharmacology. 1984;84(4):452–6.
Bartoli A, Xiaodong S, Gatti G, Cipolla G, Marchiselli R, Perucca E. The influence of ethnic factors and gender on CYP1A2-mediated drug disposition: a comparative study in Caucasian and Chinese subjects using phenacetin as a marker substrate. Ther Drug Monit. 1996;18(5):586–91.
Loboz KK, Gross AS, Williams KM, Liauw WS, Day RO, Blievernicht JK, et al. Cytochrome P450 2B6 activity as measured by bupropion hydroxylation: effect of induction by rifampin and ethnicity. Clin Pharmacol Ther. 2006;80(1):75–84.
Chen K, Wang R, Wen SY, Li J, Wang SQ. Relationship of P450 2C9 genetic polymorphisms in Chinese and the pharmacokinetics of tolbutamide. J Clin Pharm Ther. 2005;30(3):241–9.
Madsen H, Enggaard TP, Hansen LL, Klitgaard NA, Brosen K. Fluvoxamine inhibits the CYP2C9 catalyzed biotransformation of tolbutamide. Clin Pharmacol Ther. 2001;69(1):41–7.
Hu XP, Xu JM, Hu YM, Mei Q, Xu XH. Effects of CYP2C19 genetic polymorphism on the pharmacokinetics and pharmacodynamics of omeprazole in Chinese people. J Clin Pharm Ther. 2007;32(5):517–24.
Andersson T, Holmberg J, Rohss K, Walan A. Pharmacokinetics and effect on caffeine metabolism of the proton pump inhibitors, omeprazole, lansoprazole, and pantoprazole. Br J Clin Pharmacol. 1998;45(4):369–75.
Rudorfer MV, Lane EA, Chang WH, Zhang MD, Potter WZ. Desipramine pharmacokinetics in Chinese and Caucasian volunteers. Br J Clin Pharmacol. 1984;17(4):433–40.
Yang G, Fu Z, Chen X, Yuan H, Yang H, Huang Y, et al. Effects of the CYP oxidoreductase Ala503Val polymorphism on CYP3A activity in vivo: a randomized, open-label, crossover study in healthy Chinese men. Clin Ther. 2011;33(12):2060–70.
Kharasch ED, Walker A, Hoffer C, Sheffels P. Intravenous and oral alfentanil as in vivo probes for hepatic and first-pass cytochrome P450 3A activity: noninvasive assessment by use of pupillary miosis. Clin Pharmacol Ther. 2004;76(5):452–66.
Kupferschmidt HH, Ha HR, Ziegler WH, Meier PJ, Krahenbuhl S. Interaction between grapefruit juice and midazolam in humans. Clin Pharmacol Ther. 1995;58(1):20–8.
Tsunoda SM, Velez RL, von Moltke LL, Greenblatt DJ. Differentiation of intestinal and hepatic cytochrome P450 3A activity with use of midazolam as an in vivo probe: effect of ketoconazole. Clin Pharmacol Ther. 1999;66(5):461–71.
Mandema JW, Tuk B, van Steveninck AL, Breimer DD, Cohen AF, Danhof M. Pharmacokinetic–pharmacodynamic modeling of the central nervous system effects of midazolam and its main metabolite alpha-hydroxymidazolam in healthy volunteers. Clin Pharmacol Ther. 1992;51(6):715–28.
Guo T, Mao GF, Xia DY, Su XY, Zhao LS. Pharmacokinetics of midazolam tablet in different Chinese ethnic groups. J Clin Pharm Ther. 2011;36(3):406–11.
Shih PS, Huang JD. Pharmacokinetics of midazolam and 1′-hydroxymidazolam in Chinese with different CYP3A5 genotypes. Drug Metab Dispos. 2002;30(12):1491–6.
Duan KM, Wang SY, Ouyang W, Mao YM, Yang LJ. Effect of quercetin on CYP3A activity in Chinese healthy participants. J Clin Pharmacol. 2012;52(6):940–6.
Backman JT, Kivisto KT, Olkkola KT, Neuvonen PJ. The area under the plasma concentration-time curve for oral midazolam is 400-fold larger during treatment with itraconazole than with rifampicin. Eur J Clin Pharmacol. 1998;54(1):53–8.
Fayer JL, Zannikos PN, Stevens JC, Luo Y, Sidhu R, Kirkesseli S. Lack of correlation between in vitro inhibition of CYP3A-mediated metabolism by a PPAR-gamma agonist and its effect on the clinical pharmacokinetics of midazolam, an in vivo probe of CYP3A activity. J Clin Pharmacol. 2001;41(3):305–16.
Olkkola KT, Backman JT, Neuvonen PJ. Midazolam should be avoided in patients receiving the systemic antimycotics ketoconazole or itraconazole. Clin Pharmacol Ther. 1994;55(5):481–5.
Gross AS, Bridge S, Shenfield GM. Pharmacokinetics of tolbutamide in ethnic Chinese. Br J Clin Pharmacol. 1999;47(2):151–6.
Caraco Y, Wilkinson GR, Wood AJ. Differences between white subjects and Chinese subjects in the in vivo inhibition of cytochrome P450s 2C19, 2D6, and 3A by omeprazole. Clin Pharmacol Ther. 1996;60(4):396–404.
Zhang A, Xing Q, Qin S, Du J, Wang L, Yu L, et al. Intra-ethnic differences in genetic variants of the UGT-glucuronosyltransferase 1A1 gene in Chinese populations. Pharmacogenomics J. 2007;7(5):333–8.
Ajir K, Smith M, Lin KM, Fleishaker JC, Chambers JH, Anderson D, et al. The pharmacokinetics and pharmacodynamics of adinazolam: multi-ethnic comparisons. Psychopharmacology. 1997;129(3):265–70.
Hendershot PE, Fleishaker JC, Lin KM, Nuccio ID, Poland RE. Pharmacokinetics of reboxetine in healthy volunteers with different ethnic descents. Psychopharmacology. 2001;155(2):148–53.
Yu KS, Cho JY, Shon JH, Bae KS, Yi SY, Lim HS, et al. Ethnic differences and relationships in the oral pharmacokinetics of nifedipine and erythromycin. Clin Pharmacol Ther. 2001;70(3):228–36.
Acknowledgments
We thank Pfizer Ltd (Sandwich, UK) for providing the demographic information on their cohort of healthy Chinese volunteers, and James Kay for his assistance with the preparation of this manuscript.
Conflicts of Interest
No sources of funding were used to conduct this study. Zoe E. Barter, Geoffrey T. Tucker and Karen Rowland-Yeo have no conflicts of interest that are directly relevant to the content of this study.
Author information
Authors and Affiliations
Corresponding author
Electronic Supplementary Material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article
Cite this article
Barter, Z.E., Tucker, G.T. & Rowland-Yeo, K. Differences in Cytochrome P450-Mediated Pharmacokinetics Between Chinese and Caucasian Populations Predicted by Mechanistic Physiologically Based Pharmacokinetic Modelling. Clin Pharmacokinet 52, 1085–1100 (2013). https://doi.org/10.1007/s40262-013-0089-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40262-013-0089-y