
Abstract
Background
Chronic obstructive pulmonary disease (COPD) poses major challenges for health care systems. Previous studies suggest that telemonitoring could be effective in preventing hospitalisations and hence reduce costs.
Objective
The aim was to evaluate whether telemonitoring interventions for COPD are cost-effective from the perspective of German statutory sickness funds.
Methods
A cost-utility analysis was conducted using a combination of a Markov model and a decision tree. Telemonitoring as add-on to standard treatment was compared with standard treatment alone. The model consisted of four transition stages to account for COPD severity, and a terminal stage for death. Within each cycle, the frequency of exacerbations as well as outcomes for 2015 costs and quality adjusted life years (QALYs) for each stage were calculated. Values for input parameters were taken from the literature. Deterministic and probabilistic sensitivity analyses were conducted.
Results
In the base case, telemonitoring led to an increase in incremental costs (€866 per patient) but also in incremental QALYs (0.05 per patient). The incremental cost-effectiveness ratio (ICER) was thus €17,410 per QALY gained. A deterministic sensitivity analysis showed that hospitalisation rate and costs for telemonitoring equipment greatly affected results. The probabilistic ICER averaged €34,432 per QALY (95 % confidence interval 12,161–56,703).
Conclusion
We provide evidence that telemonitoring may be cost-effective in Germany from a payer’s point of view. This holds even after deterministic and probabilistic sensitivity analyses.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Telemonitoring may be cost-effective from the perspective of German statutory sickness funds. |
As uncertainties about actual intervention costs remain, those costs are a major factor of uncertainty. |
As long as telemonitoring services are not reimbursed by German statutory sickness funds, a broad use of telemonitoring is highly unlikely. |
1 Introduction
Chronic obstructive pulmonary disease (COPD) affects approximately 13 % of people older than 40 years in Germany [1] and about 64 million people worldwide [2]. The disease progressively decreases lung function. Because of its high prevalence rates, which are predicted to even increase due to demographic change, health care providers as well as government officials search for new strategies to adequately treat patients with COPD. One approach is the use of telemedicine technology, empowering physicians to remotely monitor diseased patients. Telemonitoring is supposed to identify exacerbations in a timely manner such that hospitalisations can be avoided and health care costs reduced.
However, the broad use of new interventions, like telemonitoring, is highly unlikely if its costs are not reimbursed by statutory sickness funds. To be reimbursed, the technology has to be considered adequate, appropriate and efficient [3]. Pilot projects of two major German statutory sickness funds are being conducted in order to evaluate the effectiveness of telemonitoring for COPD patients [4, 5]. A formal health technology assessment of telemonitoring for COPD has, however, not been performed yet. Also, studies evaluating the cost-effectiveness of telemonitoring services in a German context are absent. Findings of recently conducted cost-effectiveness studies in other European countries, such as Great Britain [6] and Denmark [7], cannot be directly applied to the German context. The British study includes COPD patients only among other chronic conditions such as heart failure and diabetes and does not report disease-specific cost-effectiveness [6]. The Danish results are not generalisable, because they are based on a small sample of 105 patients and may not be reproducible in “an actual implementing situation” [7]. Therefore, this study analyses whether a telemonitoring intervention for the treatment of COPD is cost-effective from the perspective of German statutory sickness funds.
2 Methods
COPD is characterised by constant progression as well as episodes of acute worsening that need further treatment and can end up with hospitalisation or death [8, 9]. To consider these different dimensions, a combination of a Markov model and a decision tree was constructed. Quality adjusted life years (QALYs) and costs were chosen as outcomes. The model was run for two separate but homogenous cohorts, i.e. standard care versus telemonitoring added to standard care.
Telemonitoring is assumed to be similar to the intervention described by Van der Heijden et al. [10]. More precisely, the patient transmits data about vital parameters to a network that is able to calculate the risk of exacerbations. The transmitted data can be accessed by a nurse or physician [10]. The intervention is only considered for COPD patients with Global Initiative for Obstructive Lung Disease (GOLD) stage III and IV. This is in alignment with the pilot projects of German statutory sickness funds for the use of telemonitoring in COPD patients [4]. Results were used to calculate an incremental cost-effectiveness ratio (ICER). QALYs as well as costs were discounted with an annual rate of 3 % [11].
2.1 Study Design
The Markov model simulates the disease progression over a time horizon of 20 years with a cycle length of 1 year. The Markov chain was designed following an earlier COPD model for Germany by Menn [12]. The model structure is also in alignment with other previously published studies, which modelled dynamic patient population models for COPD [13, 14]. At the beginning of the first period, each patient is assigned to one of the four GOLD stages [15] (representing disease severity, with GOLD IV being the most severe stage). The initial assignment is based on prevalence rates for COPD in Germany [1]. After a cycle, patients either remain in their current GOLD stage or move to the more severe stage (see Fig. 1). The model calculates cost of treatment according to GOLD stage, the occurrence of exacerbations in each stage, as well as mortality. Half-cycle correction was applied [16]. All calculations were conducted with Microsoft Excel©.

Markov Chain
Depending on the GOLD stage, a predefined number of exacerbations occurs per cycle. The treatment of exacerbations is modelled with a decision tree. The decision tree thus simulates the costs associated with exacerbation treatment dependent on the patient’s current GOLD stage. Exacerbations are assumed to become more frequent with increasing GOLD stage [17]. For each exacerbation, treatment is modelled in accordance to the recommendations of the German Respiratory League [18]. We differentiate between four treatments: (a) antibiotics, (b) systemic corticosteroids, (c) a combination of (a) and (b), and (d) hospitalisation (see Fig. 2). By varying the probabilities for each treatment option depending on the GOLD stage following Hurst et al. [17], the distribution of treatments also reflects the severity of exacerbations. Since GOLD I patients were not included in the study by Hurst et al. [17], we took data regarding exacerbation frequency of GOLD I patients from Borg et al. [19]. Furthermore, GOLD I patients are assumed to have the same probabilities for each treatment as GOLD II patients. Patients who experience an exacerbation that requires admission to a hospital are assumed (1) to be potentially rehospitalised within 1 year, (2) to be returned for treatment in the outpatient setting (no rehospitalisation), or (3) to die [8]. Decedents are transferred to the death state in the Markov model immediately to avoid double counts.

Treatment of exacerbations
To validate our model towards quality criteria, we used a checklist following suggestions of the International Society for Pharmacoeconomics and Outcomes Research (ISPOR) modelling task force [20]. The checklist was used to evaluate whether best practice suggestions were met. Unmet quality criteria (namely non-separation of mortality causes and possible confounding regarding our measurement of effectiveness) are discussed in the limitations section.
2.2 Model Parameters
2.2.1 Measurement of Costs
Standard treatment follows recommendations of the German Respiratory League and is dependent on the patients’ GOLD stage [18]. In their guideline, the German Respiratory League recommends an examination by a physician and an influenza vaccination at least once a year, regardless of disease severity. Furthermore, GOLD II patients are obliged to take long-acting bronchodilators once a day. In addition to bronchodilators, daily use of corticosteroids for inhalation is recommended for GOLD III and IV patients. Exacerbations should be treated by the use of systemic corticosteroids and antibiotics (one for GOLD I and II patients, two different antibiotics for GOLD III and IV patients), which have to be prescribed by a physician after a short examination.
For obtaining drug prices, we used official pharmacy retail prices [21]. After checking for their applicability to treat COPD, the cheapest pack size combination available for each active ingredient was selected to avoid overestimation of drug costs. For bronchodilators, we prefer aerosol sprays over oral forms, since sprays are easier to handle for the patient and are thus used more frequently. No co-payments are considered, as patients with chronic conditions usually exceed the income threshold above which they are exempted from co-payments in Germany. Costs for physician contacts are taken from the reimbursement catalogue for outpatient services [22]. We consider costs for a face-to-face physician visit (dependent on the patient’s age), spirometry, and an extra charge for chronically ill patients. Thus, costs for a physician contact total to €35.15.
Costs for hospitalisations are calculated from the hospital reimbursement catalogue, the German Diagnosis Related Groups (g-DRG) scheme [23]. For inpatient treatment of COPD, three DRGs are applicable: E65A (COPD, major complications, €4028), E65B [COPD, no complications, forced expiratory volume in 1 s (FEV1) <35 %, €2545], and E65C (COPD, no complications, FEV1 >35 %, €2058). We calculated the weighted average of the three DRG costs using the distribution of cases in 2015 [23]. Thus, hospitalisation costs are €2267.78 per visit.
Costs for telemonitoring interventions are taken from the literature. However, these are scarce and can range widely [6]. An Italian randomised controlled trial (RCT) reported average yearly intervention costs of €978 per patient (€1092, adjusted to prices in 2015) [24]. A Danish RCT reported intervention costs for a tele-rehabilitation programme of €677 per patient (€732, adjusted to prices in 2015) [7]. A telemonitoring RCT from the USA reported annual intervention costs of approximately US$983 (€696, converted using 1.48 as the exchange rate) [25]. A British RCT reported average intervention costs of £1847 (€2186, converted using 0.91 as the exchange rate) [6]. We thus set annual intervention costs to the mean of the four studies, at €1177. All prices/costs were inflated or deflated to reflect 2015 costs.
2.2.2 Measurement of Effectiveness
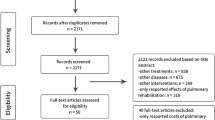
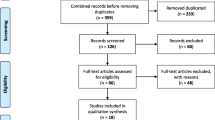
A recently conducted systematic review by Udsen et al. [26] found six studies measuring the (cost-)effectiveness of telemonitoring for COPD patients. We updated the review by conducting a literature search via PubMed and Google Scholar using the keywords “telemonitoring”, “telehealth”, and “tele” in combination with “COPD” and/or “effectiveness”. Seven additional studies were identified. We then excluded studies (a) with an observation period below 6 months, (b) those that did not report outcomes for COPD patients separately, and (c) studies that were based on the same dataset as a previously included study. Of the 13 studies, six studies met our inclusion criteria. Five studies reported on hospitalisation and/or severe exacerbation [24, 27–30]; one study reported on rehospitalisation [31]. Details on the inclusions and exclusions as well as on the data extracted from each study are provided in supplement A (see electronic supplementary material, online resource 1).
To estimate the effectiveness of telemonitoring to prevent hospitalisations, a random-effects meta-analysis of the five studies reporting on hospitalisations was conducted [32]. Two of the five studies were RCT trials. Three studies were non-randomised. According to the pooling results, telemonitoring is estimated to reduce the number of hospitalisations due to an exacerbation by 33.3 % (see supplement B, online resource 1). Since only one previously identified study reported on rehospitalisation, its data were used to estimate the effectiveness of telemonitoring in preventing rehospitalisations in our model. The study reported a reduction of rehospitalisations due to telemonitoring of 26.1 % [31].
2.2.3 Quality of Life Measurement
A patient’s quality of life is assumed to depend on GOLD stage at the end of every cycle. Therefore, we adjusted life years using data from Jones et al. [33], who evaluated the health status of 1817 European COPD patients using the St. Georges Respiratory Questionnaire-COPD (SGRQ-COPD). The SGRQ total scores derived by Jones et al. [33] were transformed to EQ-5D utilities using the algorithm developed by Starkie et al. [34]. Accordingly, being in GOLD I, GOLD II, GOLD III, and GOLD IV results in 0.778 QALYs, 0.762 QALYs, 0.662 QALYs, and 0.562 QALYs per cycle, respectively.
2.3 Sensitivity Analysis
To acknowledge uncertainty in our input parameters, deterministic and probabilistic sensitivity analyses were conducted. For the deterministic one-way sensitivity analysis, we assumed QALYs, hospitalisation, rehospitalisation, intervention costs, cost of hospitalisation, and the time horizon of our model to have a critical impact on outcomes. For QALYs, 95 % confidence intervals (CIs) of the originally reported scores were calculated and used as upper and lower boundaries [33]. Reduction in hospitalisations, reduction in rehospitalisations, and intervention costs were varied by 50 % points in both directions. For cost of hospitalisation, the two DRGs E65A and E65C represent the upper and the lower boundary. The time horizon was altered by ±10 years.
For probabilistic sensitivity analysis, a Monte Carlo simulation with 10,000 repetitions was performed. As listed in Table 1, input parameters were randomly drawn from either a beta or a gamma distribution [35]. Where possible, distributions were fitted to empirical data from the literature. Otherwise, distributional parameters were generated as recommended by Briggs et al. [35]. Costs for hospitalisation were not gamma distributed, since large variations of this parameter are unrealistic because of the German DRG scheme. Instead, the proportions used to calculate the mean of hospitalisation cost (see Sect. 2.2.1) were beta distributed.
3 Results
Over a lifetime, telemonitoring was able to prevent 0.07 hospitalisations, 0.01 rehospitalisations, and 0.02 exacerbation-related deaths per patient compared with standard care. Please be reminded that these results are intention-to-treat, i.e. our cohort also includes GOLD I and GOLD II patients who do not enter telemonitoring right away, but after the disease has progressed to GOLD III. The costs totalled to €4228 per patient for telemonitoring and to €3361 for standard treatment per patient. The higher cost of the telemonitoring intervention (€962 per patient) was thus not compensated by savings from reduced hospitalisations (€197 per patient). In addition, the avoidance of exacerbation-related deaths in the telemonitoring group was accompanied by higher costs for pharmaceuticals (€49 per patient). A surplus of 0.05 QALYs per patient was attained in the telemonitoring cohort, which resulted in an ICER of €17,410 per QALY.
As the tornado diagram shows (see Fig. 3), the rate of prevented hospitalisations and intervention costs influenced the ICER most. Varying their values within previously defined boundaries resulted in maximum ICERs of €36,900 and €27,072 and minimum ICERs of €11,133 and €7748 for reduction in hospitalisations and intervention costs, respectively. In contrast, the influence of the rate of prevented rehospitalisations was non-existent. The parameters “reduction in hospitalisations” and “intervention costs” have a high influence; Fig. 4 shows how changes in those two parameters affect the ICER. The probabilistic sensitivity analysis showed results comparable to the deterministic analyses (see Fig. 5). After 10,000 repetitions, the ICER averaged €34,432 (95 % CI 12,161–56,703). Telemonitoring was more effective but also more costly 69.10 % of the time. Furthermore, the ICER was less than zero in 3076 cases, of which, in 802 times, it dominated the standard therapy.

Tornado diagram for deterministic sensitivity analyses

Incremental cost-effectiveness ratio as a function of the reduction in hospitalisations and as a function of intervention costs

Results from Monte–Carlo simulation
4 Discussion
In this paper, we conducted a cost-utility-analysis of a telemonitoring intervention for COPD patients with GOLD stage III and IV in a German setting, resulting in an ICER of €17,410 per QALY compared with standard treatment. Although no threshold to judge the cost-effectiveness of a medical intervention has been defined in Germany, the ICER would be considered cost-effective for the treatment of COPD patients according to UK standards as the National Institute for Health and Care Excellence (NICE) recommends a maximum threshold of £30,000 (~€42,000) [36]. According to recently published data on the willingness to pay (WTP) for a QALY in Germany, i.e. between €8580 and €18,420 per QALY,Footnote 1 the ICER for telemonitoring appears to be in between the WTP thresholds [37]. In contrast, the World Health Organization recommends a threshold equal to the GDP per capita of a country [38]. Since the GDP per capita in Germany is approximately US$47,774 (~€39,486, converted using 1.21 as exchange rate), the intervention would be cost-effective [39]. Our results were confirmed by sensitivity analyses, showing the robustness of the model.
To our knowledge, this is the first study to evaluate cost-effectiveness of telemonitoring for COPD patients in a German context. Previously, a Danish cost-effectiveness study found a telemonitoring intervention for COPD patients cost-effective [7], while a British study did not [6]. However, a central assumption that is driving cost-effectiveness is intervention costs. True cost data for the telemonitoring intervention from the medical technology industry is hard to obtain, probably because of strategic reasons. As a result, the telemonitoring costs assumed in different studies vary widely [6]. The British study used £1847 (€2186, converted using 0.91 as the exchange rate and adjusted to prices in 2015), whereas the Danish study assumed €677 per patient (€732, adjusted to prices in 2015). Our cost of intervention was €1177. Using the intervention costs from the British study would have resulted in an ICER of €45,451, whereas the intervention costs of the Danish study would have resulted in an ICER of €13,517. This is why we also provided the ICER depending on intervention costs. We thus enable decision makers to compare specific programme costs within our framework.
The costs as well as effectiveness of a telemonitoring intervention may also depend on the organisational structures of health service provision, as a successful adoption of telemonitoring is likely to be linked to the adoption of new organisational forms [40]. Therefore, it may be difficult for physicians as well as patients to adapt telemonitoring, which might limit potential benefits in the early phase of its implementation. For example, telemonitoring service centres, which would be needed to collect and distribute relevant data [41], are not yet broadly established in Germany. Once they are, telemonitoring may be able to create synergies if used to treat nationwide (economies of scale) or to treat several chronic conditions for multi-morbid patients simultaneously (economies of scope).
Incremental effectiveness of telemonitoring may also be dependent on the current quality of care for COPD patients, as an RCT by Pinnock et al. [29] suggests. In their setting, standard care already included self-monitoring. Telemonitoring was just added to standard care as a supporting tool. In the end, no differences in hospitalisation rates to standard care were observed [29]. Therefore, if the quality of standard care for COPD is already provided at a very high level, the incremental benefits of telemonitoring may be small [42].
Finally, practical problems in implementation, such as usability issues among elderly patients, may occur [43]. A systematic review by Gorst et al. [44] found that one third of patients who were offered telemedicine refused to use it and that one fifth of those who accepted telemedicine abandoned it later. In fact, problems with handling telemonitoring equipment may even lower a patient’s quality of life, e.g. if they feel overstrained with the application.
Our model is based on several assumptions. First, the frequency of exacerbations and their treatment, the centrepieces of our study, was reported rather conservatively [17]. Other studies reported higher average exacerbation rates [45]. This would have led to the prevention of more hospitalisations by telemonitoring and thus to a lower ICER. Second, studies with potential confounding bias (i.e. observational studies) were taken into account within the random-effects pooling. However, Shrier et al. [46] concluded that the inclusion of observational studies may contribute to better parameter estimates within meta-analyses and pooling approaches. Third, as the tornado diagram shows, our model is sensitive for changes in the time horizon. This is highly related to assumptions about the mortality of patients in the different GOLD stages. A systematic review by Hoogendoorn et al. [47] identified mortality to have a critical influence on cost-effectiveness outcomes in previously published models regarding COPD. We did not differentiate between COPD-specific mortality and all-cause mortality, because of a lack of applicable data. Adding an all-cause mortality state would probably have increased the ICER. Fourth, some cost items could not be considered in this study. For example, there is evidence that costs of rehabilitation are reduced by telemonitoring [48]. Also, we did not consider costs for lung transplantations or comparable surgeries. Given the higher rate of survivors with severe COPD in the telemonitoring cohort, the intervention would have been potentially less cost-effective. Fifth, we may have overestimated costs for pharmaceutical care as German statutory sickness funds are able to negotiate discounts for their insurees. This would have equally affected both groups, however. Sixth, prevalence rates of COPD and GOLD stage were based on a study where participants were all recruited in a single region of Germany [1]. However, the prevalence rates we used for Germany are comparable to findings in other European countries, such as Poland, Norway, and Austria [49]. Seventh, recent studies suggested different risks of mortality between male and female COPD patients, who were not analysed separately in our setting [9]. The same applies for smokers and former smokers. Finally, the GOLD no longer recommends a classification of disease severity for COPD based on the GOLD stages I–IV alone. They rather suggest individualising the diagnosis of COPD by focussing on a combination of symptoms and exacerbation history [12]. However, for our cohort model, the population-based classification of GOLD stage I–IV is still sufficient.
5 Conclusion
In the setting of our study, telemonitoring for patients with severe COPD may be cost-effective from the view of the German statutory sickness funds. The results hold after a probabilistic sensitivity analysis with 10,000 draws. Eventually, telemonitoring creates the common dilemma for payers of balancing quality and cost of health care. If there is a need for telemonitoring interventions in Germany, it is necessary for telemedicine services to be reimbursed by German statutory sickness funds. Without reimbursement, a broad use of telemonitoring in Germany is highly unlikely, as patients would probably have to bear treatment costs directly or its use would remain limited to current pilot projects of German statutory sickness funds. Certainly, there may be options to improve COPD treatment by other means, such as with chronic care management programmes, which educate patients to better manage their disease by themselves. Comparable programmes were found to reduce the risk of hospitalisations and to improve quality of life [50]. Another approach is smoking cessation programmes [51], which would probably be less expensive to implement on a large scale. However, both approaches are—at least for those that participate on a voluntary basis—already part of standard care. Future studies could consider whether regional aspects may drive the cost-effectiveness of telemonitoring for COPD as the German government already considers the nationwide implementation of other telemedicine services in rural areas [52].
Notes
Results depended on the survey technique that was used.
References
Geldmacher H, Biller H, Herbst A, Urbanski K, Allison M, Buist AS, et al. The prevalence of chronic obstructive pulmonary disease (COPD) in Germany. Results of the BOLD study. Dtsch Med Wochenschr 1946. 2008;133:2609–14.
WHO | Burden of COPD [Internet]. Available from: http://www.who.int/respiratory/copd/burden/en/. Cited 21 Jun 2016.
Busse R, Stargardt T, Schreyögg J. Determining the “health benefit basket” of the statutory health insurance scheme in Germany. Eur J Health Econ. 2005;6:30–6.
Bayerische TelemedAllianz | Angewandte Telemedizin—Bayerische Projekte, Prävention—Modellvorhaben Telemedizin bei COPD [Internet]. Available from: http://www.telemedallianz.de/at_p_modell_copd.html. Cited 21 Jun 2016.
E-Health: Individuelle telemedizinische Betreuung von COPD-Patienten [Internet]. Available from: http://www.philips.de/a-w/about/news/archive/standard/news/healthcare/20150401_Philips_E-Health_Motiva.html. Cited 21 Jun 2016.
Henderson C, Knapp M, Fernández J-L, Beecham J, Hirani SP, Cartwright M, et al. Cost effectiveness of telehealth for patients with long term conditions (Whole Systems Demonstrator telehealth questionnaire study): nested economic evaluation in a pragmatic, cluster randomised controlled trial. BMJ. 2013;346:f1035.
Haesum LK, Soerensen N, Dinesen B, Nielsen C, Grann O, Hejlesen O, et al. Cost-utility analysis of a telerehabilitation program: a case study of COPD patients. Telemed E Health. 2012;18:688–92.
McGhan R, Radcliff T, Fish R, Sutherland ER, Welsh C, Make B. Predictors of rehospitalization and death after a severe exacerbation of COPD. CHEST J. 2007;132:1748–55.
Rodriguez-Roisin R. Toward a consensus definition for COPD exacerbations. CHEST J. 2000;117:398S–401S.
Van Der Heijden M, Lijnse B, Lucas PJ, Heijdra YF, Schermer TR. Managing COPD exacerbations with telemedicine. Artif Intell Med [Internet]. 2011:169–78. Available from: http://springerlink.bibliotecabuap.elogim.com/10.1007%2F978-3-642-22218-4_21. Cited 29 Feb 2016 (Springer).
iqwig.de—IQWiG publishes new version of its General Methods [Internet]. Available from: https://www.iqwig.de/en/press/pressemitteilungen/press-releases/iqwig-publishes-new-version-of-its-general-methods.5346.html. Cited 21 Jun 2016.
Menn P. Einsatz entscheidungsanalytischer Modelle für die ökonomische Evaluation medizinischer Verfahren am Beispiel chronisch obstruktiver Lungenerkrankungen [Internet]. lmu; 2009. Available from: https://edoc.ub.uni-muenchen.de/10315/. Cited 21 Mar 2016.
Hoogendoorn M, Rutten-van Mölken MP, Hoogenveen RT, Al MJ, Feenstra TL. Developing and applying a stochastic dynamic population model for chronic obstructive pulmonary disease. Value Health. 2011;14:1039–47.
Price D, Gray A, Gale R, Asukai Y, Mungapen L, Lloyd A, et al. Cost-utility analysis of indacaterol in Germany: a once-daily maintenance bronchodilator for patients with COPD. Respir Med. 2011;105:1635–47.
Global strategy for diagnosis, management, and prevention of COPD—2016—Global initiative for chronic obstructive lung disease—GOLD [Internet]. Available from: http://goldcopd.org/global-strategy-diagnosis-management-prevention-copd-2016/. Cited 21 Jun 2016.
Naimark DM, Bott M, Krahn M. The half-cycle correction explained: two alternative pedagogical approaches. Med Decis Making. 2008;28:706–12.
Hurst JR, Vestbo J, Anzueto A, Locantore N, Müllerova H, Tal-Singer R, et al. Susceptibility to exacerbation in chronic obstructive pulmonary disease. N Engl J Med. 2010;363:1128–38.
Vogelmeier C, Buhl R, Criee CP, Gillissen A, Kardos P, Köhler D, et al. Leitlinie der Deutschen Atemwegsliga und der Deutschen Gesellschaft für Pneumologie und Beatmungsmedizin zur Diagnostik und Therapie von Patienten mit chronisch obstruktiver Bronchitis und Lungenemphysem (COPD). Pneumologie. 2007;61:e1–40.
Borg S, Ericsson A, Wedzicha J, Gulsvik A, Lundbäck B, Donaldson GC, et al. A computer simulation model of the natural history and economic impact of chronic obstructive pulmonary disease. Value Health. 2004;7:153–67.
Caro JJ, Briggs AH, Siebert U, Kuntz KM, ISPOR-SMDM Modeling Good Research Practices Task Force. Modeling good research practices–overview: a report of the ISPOR-SMDM Modeling Good Research Practices Task Force–1. Value Health J Int Soc Pharmacoecon Outcomes Res. 2012;15:796–803.
Behandlung: COPD—Onmeda: Medizin and Gesundheit [Internet]. Available from: http://www.onmeda.de/Anwendungsgebiet/COPD.html. Cited 21 Jun 2016.
KBV—Online-version des EBM [Internet]. Available from: http://www.kbv.de/html/online-ebm.php. Cited 21 Jun 2016.
Report-Browser 2013/2015, InEK GmbH [Internet]. Available from: http://www.g-drg.de/cms/G-DRG-System_2015/Abschlussbericht_zur_Weiterentwicklung_des_G-DRG-Systems_und_Report_Browser/Report-Browser_2013_2015. Cited 21 Jun 2016.
Vitacca M, Bianchi L, Guerra A, Fracchia C, Spanevello A, Balbi B, et al. Tele-assistance in chronic respiratory failure patients: a randomised clinical trial. Eur Respir J. 2009;33:411–8.
Upatising B, Wood DL, Kremers WK, Christ SL, Yih Y, Hanson GJ, et al. Cost comparison between home telemonitoring and usual care of older adults: a randomized trial (Tele-ERA). Telemed E Health. 2015;21:3–8.
Udsen FW, Hejlesen O, Ehlers LH. A systematic review of the cost and cost-effectiveness of telehealth for patients suffering from chronic obstructive pulmonary disease. J Telemed Telecare. 2015;21:108–18.
Maiolo C, Mohamed EI, Fiorani CM, De Lorenzo A. Home telemonitoring for patients with severe respiratory illness: the Italian experience. J Telemed Telecare. 2003;9:67–71.
Paré G, Sicotte C, St.-Jules D, Gauthier R. Cost-minimization analysis of a telehomecare program for patients with chronic obstructive pulmonary disease. Telemed J E Health. 2006;12:114–21.
Pinnock H, Hanley J, McCloughan L, Todd A, Krishan A, Lewis S, et al. Effectiveness of telemonitoring integrated into existing clinical services on hospital admission for exacerbation of chronic obstructive pulmonary disease: researcher blind, multicentre, randomised controlled trial. BMJ. 2013;347:f6070.
Trappenburg JC, Niesink A, de Weert-van Oene GH, van der Zeijden H, van Snippenburg R, Peters A, et al. Effects of telemonitoring in patients with chronic obstructive pulmonary disease. Telemed E Health. 2008;14:138–46.
Casas A, Troosters T, Garcia-Aymerich J, Roca J, Hernández C, Alonso A, et al. Integrated care prevents hospitalisations for exacerbations in COPD patients. Eur Respir J. 2006;28:123–30.
DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986;7:177–88.
Jones PW, Brusselle G, Dal Negro RW, Ferrer M, Kardos P, Levy ML, et al. Health-related quality of life in patients by COPD severity within primary care in Europe. Respir Med. 2011;105:57–66.
Starkie HJ, Briggs AH, Chambers MG, Jones P. Predicting EQ-5D values using the SGRQ. Value Health. 2011;14:354–60.
Briggs A, Sculpher M, Claxton K. Decision modelling for health economic evaluation [Internet]. OUP Oxford; 2006. Available from: https://books.google.de/books?hl=de&lr=&id=NuYRBAAAQBAJ&oi=fnd&pg=PP1&dq=Decision+modelling+for+health+economic+evaluation&ots=JJR9ZTPCnm&sig=WF76M54HOMPdsWMvw-qISgs29Uk. Cited 21 Jun 2016.
Guide to the methods of technology appraisal 2013 | Foreword | Guidance and guidelines | NICE [Internet]. Available from: https://www.nice.org.uk/article/pmg9/chapter/Foreword. Cited 22 Jun 2016.
Ahlert M, Breyer F, Schwettmann L. How you ask is what you get: framing effects in willingness-to-pay for a QALY. Soc Sci Med. 2016;150:40–8.
WHO | Table: Threshold values for intervention cost-effectiveness by region [Internet]. Available from: http://www.who.int/choice/costs/CER_levels/en/. Cited 21 Jun 2016.
Länder and Regionen—Internationales—Daten nach Thema—Basistabelle—Statistisches Bundesamt (Destatis) [Internet]. Available from: https://www.destatis.de/DE/ZahlenFakten/LaenderRegionen/Internationales/Thema/Tabellen/Basistabelle_BIPproKopf.html. Cited 21 Jun 2016.
Bartoli L, Zanaboni P, Masella C, Ursini N. Systematic review of telemedicine services for patients affected by chronic obstructive pulmonary disease (COPD). Telemed E Health. 2009;15:877–83.
Müller A, Schweizer J, Helms TM, Oeff M, Sprenger C, Zugck C. Telemedical support in patients with chronic heart failure: experience from different projects in Germany. Int J Telemed Appl. 2010;2010:8.
Jordan R, Adab P, Jolly K, et al. Telemonitoring for patients with COPD. BMJ [Internet]. 2013;347. Available from: http://www.bmj.com/content/347/bmj.f5932.abstract. Cited 12 Jun 2016.
Cruz J, Brooks D, Marques A. Home telemonitoring in COPD: a systematic review of methodologies and patients’ adherence. Int J Med Inf. 2014;83:249–63.
Gorst SL, Armitage CJ, Brownsell S, Hawley MS. Home telehealth uptake and continued use among heart failure and chronic obstructive pulmonary disease patients: a systematic review. Ann Behav Med. 2014;48:323–36.
Seemungal TA, Donaldson GC, Paul EA, Bestall JC, Jeffries DJ, Wedzicha JA. Effect of exacerbation on quality of life in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1998;157:1418–22.
Shrier I, Boivin J-F, Steele RJ, Platt RW, Furlan A, Kakuma R, et al. Should meta-analyses of interventions include observational studies in addition to randomized controlled trials? A critical examination of underlying principles. Am J Epidemiol. 2007;166:1203–9.
Hoogendoorn M, Feenstra TL, Asukai Y, Borg S, Hansen RN, Jansson S-A, et al. Cost-effectiveness models for chronic obstructive pulmonary disease: cross-model comparison of hypothetical treatment scenarios. Value Health J Int Soc Pharmacoecon Outcomes Res. 2014;17:525–36.
Zanaboni P, Lien LA, Hjalmarsen A, Wootton R. Long-term telerehabilitation of COPD patients in their homes: interim results from a pilot study in Northern Norway. J Telemed Telecare. 2013;19:425–9.
Buist AS, McBurnie MA, Vollmer WM, Gillespie S, Burney P, Mannino DM, et al. International variation in the prevalence of COPD (the BOLD Study): a population-based prevalence study. Lancet. 2007;370:741–50.
Peytremann-Bridevaux I, Staeger P, Bridevaux P-O, Ghali WA, Burnand B. Effectiveness of chronic obstructive pulmonary disease-management programs: systematic review and meta-analysis. Am J Med. 2008;121:433–43.
Strassmann R, Bausch B, Spaar A, Kleijnen J, Braendli O, Puhan MA. Smoking cessation interventions in COPD: a network meta-analysis of randomised trials. Eur Respir J. 2009;34:634–40.
Namensartikel Bundesgesundheitsminister Gröhe—Bundesgesundheitsministerium [Internet]. Available from: http://www.bmg.bund.de/themen/krankenversicherung/e-health-initiative-und-telemedizin/namensartikel-bundesgesundheitsminister-groehe.html. Cited 21 Jun 2016.
koordinierte Bevölkerungsvorausberechnung [Internet]. Available from: https://www.destatis.de/bevoelkerungspyramide/#!y=2015. Cited 21 Jun 2016.
Lundbäck B, Eriksson B, Lindberg A, Ekerljung L, Muellerova H, Larsson L-G, et al. A 20-year follow-up of a population study-based COPD cohort-report from the obstructive lung disease in Northern Sweden studies. COPD J Chronic Obstr Pulm Dis. 2009;6:263–71.
Jenkins CR, Jones PW, Calverley PM, Celli B, Anderson JA, Ferguson GT, et al. Efficacy of salmeterol/fluticasone propionate by GOLD stage of chronic obstructive pulmonary disease: analysis from the randomised, placebo-controlled TORCH study. Respir Res. 2009;10:1.
Leivseth L, Brumpton BM, Nilsen TIL, Mai X-M, Johnsen R, Langhammer A. GOLD classifications and mortality in chronic obstructive pulmonary disease: the HUNT Study, Norway. Thorax. 2013;68:914–21.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Author contributions
FH contributed to the study design, statistical analysis, interpretation of the results, synthesis, and drafting of the manuscript. DA contributed to statistical analysis, interpretation of the results, and critical revision of the manuscript. TS contributed to statistical analysis, interpretation of the results, and critical revision of the manuscript. FH takes responsibility for accuracy of the data analysis and integrity of the data analysis.
Study funding
This study has not received any funding.
Conflict of interests
Florian Hofer, Dmitrij Achelrod, and Tom Stargardt declare that they have no conflicts of interest.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Hofer, F., Achelrod, D. & Stargardt, T. Cost-Utility Analysis of Telemonitoring Interventions for Patients with Chronic Obstructive Pulmonary Disease (COPD) in Germany. Appl Health Econ Health Policy 14, 691–701 (2016). https://doi.org/10.1007/s40258-016-0267-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40258-016-0267-9