
Abstract
Clinicians and public health experts make evidence-based decisions for individual patients, patient groups and even whole populations. In addition to the principles of internal and external validity (evidence), patient preferences must also influence decision making. Great Britain, Australia and Germany are currently discussing methods and procedures for valuing patient preferences in regulatory (authorization and pricing) and in health policy decision making. However, many questions remain on how to best balance patient and public preferences with physicians’ judgement in healthcare and health policy decision making. For example, how to define evaluation criteria regarding the perceived value from a patient’s perspective? How do physicians’ fact-based opinions also reflect patients’ preferences based on personal values? Can empirically grounded theories explain differences between patients and experts—and, if so, how? This article aims to identify and compare studies that used different preference elicitation methods and to highlight differences between patient and physician preferences. Therefore, studies comparing patient preferences and physician judgements were analysed in a review. This review shows a limited amount of literature analysing and comparing patient and physician preferences for healthcare interventions and outcomes. Moreover, it shows that methodology used to compare preferences is diverse. A total of 46 studies used the following methods—discrete-choice experiments, conjoint analyses, standard gamble, time trade-offs and paired comparisons—to compare patient preferences with doctor judgements. All studies were published between 1985 and 2011. Most studies reveal a disparity between the preferences of actual patients and those of physicians. For most conditions, physicians underestimated the impact of intervention characteristics on patients’ decision making. Differentiated perceptions may reflect ineffective communication between the provider and the patient. This in turn may keep physicians from fully appreciating the impact of certain medical conditions on patient preferences. Because differences exist between physicians’ judgement and patient preferences, it is important to incorporate the needs and wants of the patient into treatment decisions.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
∙ When doctors make decisions for their patients, they need to respect patients’ expectations and priorities. They also need to understand that doctors and patients differ in understanding medical issues because of existing information asymmetries
∙ Even with the growing importance of patient-centred healthcare in health policy decision making, the question of the congruence between patient preferences and physicians’ judgement remains unclear
∙ Patient as well as the public’s preferences should influence healthcare decision making, particularly when decision makers face the problem of prioritization of alternative treatment options
1 Background and Research Interest
Against the background of the consideration of patient and public preferences in health politics, the question of the congruence of patient preferences and doctor judgement remains unclear. This article provides a literature review on the state of agreement between patient preferences and physician judgement. To better promote patient-centred care, policy makers, experts and physicians need to understand patient priorities. Accordingly, this study intends to evaluate where there is agreement and where there are differences between patient preferences and physician judgement.
We are interested in whether different methods and techniques for eliciting patient preferences as well as attributes used in these studies show systematic disparities in agreement between patients and physicians.
Construal level theory describes the influence of psychological distance on individual thinking about technologies or interventions. The theory assumes that people’s decision making is abstract or concrete depending on psychological distance [1]. Preferences for healthcare or health technologies might change depending on psychological distance from a disease or illness. Psychological distance can be defined on several dimensions: temporal, spatial, social and hypothetical distance [2, 3]. Individuals’ decision making on more distant objects evokes more abstract thinking, while the opposite relation, decision making on close objects evokes more concrete thinking, is true as well.
An example of construal level effects in healthcare decision making would be that making decisions on one’s healthcare intervention 1 year in advance will result in rather abstract thoughts about the therapy characteristics or attributes (e.g., better life expectancy, reducing burden of disease, side effects), the very same interventions planned to occur in the next days or weeks will evoke more concrete expectations (e.g., mode of administration, like having an injection or oral treatment, reducing side effects).
The further away an event (treatment or disease) is, the easier it is for a person to make (abstract) decisions rationally and reasonably. The more concrete the event becomes, the more emotional the decision-making process. Peoples’ psychological distance depends on the experiences (hypothetical distance), whereby patients’ psychological distance depends on the time to intervention (temporal distance). The closer an event, the more concrete patients’ healthcare decision making gets. Due to social distance, we assume that doctors’ decision making will be more abstract and therefore rational and reasonable [1, 4–6]. We assume that the more concrete decision situations become (e.g., in acute conditions), the greater the differences between patients and doctors will be.
Following these assumptions, three research questions have been defined that should be answered:
-
1)
Do different elicitation techniques and methods cause different results concerning the congruence between patient preferences and physician judgements?
-
2)
Do different types of diseases (classifications) result in varying degrees of agreement concerning preferences and judgements?
-
3)
Does the congruence of preferences and judgements depend on the attributes? Is there a higher difference between patients and doctors in terms of quality of life?
2 Why Should Patient and Public Preferences Be Considered?
The goal of providing an adequate level of quality healthcare to all people [2] has many healthcare systems in western countries facing difficult decisions on reforming the systems. It is important that public and patient preferences are considered in decision making about how to allocate scarce resources [7]. If patient needs, values, priorities and preferences are taken into account, a healthcare system can be called patient-centred [8, 9].
2.1 International Developments
In recent years, consideration of public and patient preferences has increasingly been discussed. This has resulted in an agenda for public involvement in healthcare, not only in Australia [10] and Great Britain but also in Germany. Recent reforms promise a positive climate for a public engagement in the discussion about comparative efficiency, safety and cost effectiveness/efficacy [11]. Some countries routinely consider public as well as patient opinions in the process of health technology assessment and prioritization [12].
2.2 The Patient as an Expert
It is the patient who best knows his or her preferences regarding specific treatments as well as their preferences for outcomes [13]. After all, it is the patient who has to live with the consequences of treatment decisions [14]. So, it is important for the physician to be aware of patient preferences and to respect them [15]. Patient or public preferences should also be considered on the macro level and should help support decisions on the design of healthcare systems and the allocation of limited resources [16].
2.3 Healthcare Decision Making
The role of patients has changed significantly in recent years. Patients are encouraged to get involved in healthcare decision making and patient preferences are increasingly given weight [17]. Knowledge asymmetries between patient and physician can affect treatment planning and design. Importantly, information about consumer (patient) and provider preferences is essential to implementing evidence-based healthcare decision making [18]. Designing services that are sensitive to patient preferences in the context of limited resources may require policy and decision makers to choose between specific attributes and treatments with different features. Aligning clinical practice and health policy with patient preferences will improve the effectiveness/efficacy of health interventions [8].
2.4 Patient-Centred Healthcare Systems
Patient-centred healthcare systems should enable more effective interventions that also recognize patient expectations and needs. Patient priorities must factor into development of products and services. Healthcare providers can better inform and motivate patients, especially if they better understand patient thinking about perceived benefits. This will help change long-term patient behaviour. Care services and treatment processes should better align with patient preferences and expectations [8].
2.5 Shared Decision Making
Achieving this goal will require substantial reorganization of current practices and procedures related to the patient-physician relationship. According to Charles et al. [19], the traditional paternalistic model has to be redirected toward a model oriented to informed decision making. This model would be based on physicians actively educating patients by providing them with sufficient and reliable information about diseases and treatment options. This will enable patients to better make informed decisions on their own [20].
Shared decision making is a widely accepted feature of good healthcare delivery systems. It is a concept that respects the autonomous choices of a patient [13], and so can be called a major feature of patient-centred care. Patient-centredness and patient autonomy can be strengthened, while the responsibility for clinical decisions clearly remains with the attending physician [21]. Shared decision making consists of the simultaneous participation of physician and patient in all phases of the decision-making process. This includes giving equal consideration to patient preferences and physician responsibilities for providing reliable and easy to understand recommendations and guidance [20, 22]. Although research shows that shared decision making improves healthcare outcomes [1] by increasing patient satisfaction, compliance as well as adherence in terms of an improved psychological adjustment to the condition [23–26], the concept is not instituted comprehensively [27].
2.6 Physicians’ Preferences Versus Physicians’ Judgement
Doctors make decisions on behalf of their clients. In doing so, they need to safeguard the interests of their patients. The objective is maximum benefit for the affected individuals. This implies that doctors – regardless of discipline and belief—must act and decide in the sense of the best overall benefit to their patients. In addition to impact on mortality and morbidity (evaluated patient benefit), the perceived benefit for patients must play an important role in healthcare decision making. Healthcare services and products can be evaluated in three dimensions: perceived health, evaluated health and satisfaction [28]. Perceived benefit for patients (patient subjective evaluation) and evaluated patient benefit (doctor judgement) will be identical only in rare cases. It can rather be assumed that different assessment criteria are applied, depending on who assesses. Further, it is likely that doctors and patients show diverse assessment results because of information asymmetries. In comparing the opinion of patients and healthcare professionals, the latter are asked to decide for patients, not for themselves. In other words, they are making decisions for other people. Evaluations doctors make (an expert decides what is best for a patient or a group of patients) should not be called preferences but judgements. While differences between doctor judgements and patient preferences are inherent in the system, patient experience and satisfaction should not be ignored [29].
In general, decision making in healthcare takes place on three different levels and consequently may impact three different groups of stakeholders.
-
Micro-level decision making (shared decision making) The micro-level includes the treatment decisions for individual patients. Decisions on this level are built on relevance of the therapy for the disease or illness and the subsequent impact on patients’ quality of life. In most cases, these decisions are influenced by the individual circumstances and the patient’s life conditions [30] and directly impact care [31].
-
Meso-level decision making (evidence-based medicine) The meso-level describes the treatment decisions for specific patient populations. The main focus of decision making on this level is defining evidence-based medicine/nursing through evidence-based (clinical) guidelines. Here, it is important to consider patient or public preferences as well as doctor judgements [17, 22].
-
Macro-level decision making (public preferences and regulatory decisions) In evidence-based healthcare, the principles of evidence-based medicine are communicated to the organizational or institutional levels. This means that treatment decisions are not made for a single patient or a group of patients, but for a whole population [31]. The main objectives on this level are risk-benefit or cost-benefit assessments.
3 Literature Review
This article reviews studies that have elicited patient preferences and physician judgements. A literature search was conducted by the research team between October and December 2011 in the databases of PubMed/Medline and the Cochrane Library. Within the search, the following keywords and combinations led to useful hits: ‘provider preferences’, ‘experts preferences’, ‘doctors preferences’, ‘patient preferences’, ‘priorities’, ‘perspective’. Concerning the methods used for eliciting preferences, the literature research was narrowed by using the keywords ‘Discrete Choice Experiment’ or ‘DCE’, ‘Conjoint Analysis’, ‘Rating’, ‘Ranking’, ‘Time Trade Off’, ‘Visual Analog Scale’ as well as ‘Standard Gamble’. The keyword ‘preference’ or ‘preferences’ was also included as an unaccompanied search term. However, given the high number of hits in both databases, the focus was laid on the combined search terms. Moreover, an ‘all fields’ search in PubMed was applied which ensures that all key words of the combined search terms are displayed in the results.
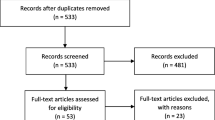
Finally, 1284 articles were found. After exclusion of duplicates, 836 were transferred to an abstract and title analysis. All studies reviewed were published between 1985 and 2011. This date range was set to encompass a full period of 25 years.
When combined with desk research (e.g., studies out of reference lists of already included articles), 102 articles met the inclusion criteria (language: German or English, elicitation and comparison of preferences and/or judgements). They reported on patient or public preferences as well as stakeholder judgements concerning a certain topic of healthcare intervention, treatment or general decision making and physician attitude. These studies underwent full text analysis. In conducting this analysis, it became clear that 22 studies had to be excluded again as the full text revealed that there was no comparison of patient/public and physician preferences.
4 Findings
The literature review shows that the methodology employed to compare preferences was diverse. Numerous methods are used to elicit preferences for a given healthcare condition, treatment procedure or for the design of a healthcare system or policy reform. The conducted literature research shows that the most common methods used in preferences studies are conjoint analyses (CA), discrete choice experiments (DCEs), standard gamble (SG), time trade-offs (TTO), and paired comparisons. In addition to these, several other quantitative and qualitative techniques are also available, including rankings, ratings, visual analogue scales as well as interviews, focus groups and card sorts. Although all of these instruments can measure needs or relevance in a certain way, researchers have concluded that preferences are best ascertained with studies that require the respondents to make decisions among different options [32].
For this reason, this review was focused on the methods of DCE, CA, SG, TTO and paired comparisons, which accounted for 46 studies. All provided a comparison of patient preferences and physicians’ judgement (see Table 1).
In the studies reviewed, the groups of stakeholders involved varied. Along with a comparison of patient and physician preferences, there were also studies comparing the views of other interest groups, including family caregivers, policy makers and representatives of the general public. Since we were focusing on the congruence of preferences and expert judgement, we included only studies that made quantifiable and comparable estimates of preferences and judgements for at least two of the stakeholder groups of interest: patients, physicians, family caregivers, policy makers or the general public.
4.1 Conjoint Analyses
CA, a form of stated preferences, is a decompositional method for estimating the structure of consumer preferences based on an evaluation of a set of alternatives defined by levels and attributes [7]. CA is a broad term covering various stated-preference methods. Stated-preference methods are specifically designed to provide information about individuals’ willingness to accept trade-offs among attributes of multi-attribute products or services. It is based on the principle that products are composed of a set of various characteristics and that the value of a product to an individual is a function of these characteristics. Patients’ relative preferences among treatments attributes and levels vary, and thus, they are willing to accept trade-offs among them. Preferences can be elicited through ranking, rating and choice between alternatives [14]. In this review, the literature research has shown 13 studies that facilitated a CA for the assessment of patient and doctor preferences [33–45]. The studies were all published between 1985 and 2010. To elicit preferences, the authors of the reviewed studies used between three and twelve attributes each. One adaptive CA was web-based (see Appendix I, Online Resource 1).
4.2 Discrete Choice Experiments
While the previous category focused generally on rating and ranking of different alternatives (covering various CA methods), this category limits its attention specifically to choice-based conjoint analysis (CBCA), also commonly referred to as discrete-choice experiments (DCEs). The DCE is a commonly used method for eliciting preferences of citizens, the insured or patients [46–51]. It is a choice-based variant of CA and a method for surveying preferences for tangible or intangible goods. The method is based on the theoretic work of McFadden [52]. The random utility theory assumes that the benefits of a good or service consist of a systematic or observable component and a random, unobservable, component [52–54]. DCEs are also based on the demand theory of Lancaster, which states that the overall benefits of a product or service can be viewed as the aggregate of the partial utility of the various properties or characteristics [55]. The respondent is asked to choose one of at least two presented alternatives (choice sets) by making trade-offs between the characteristics. Based on this discrete information, preferences (utility weights) can be estimated [56]. The theoretical foundation of DCEs in welfare economics, demand theory and utility theory has led to the increasing popularity of this method [47].
Overall, ten studies that used DCEs to elicit preferences were analysed in this review [18, 46, 57–64]. These studies were published between 2005 and 2011 and included four to seven attributes each. DCEs were used to elicit patient preferences and physician judgements in diverse conditions including psoriasis, osteoporosis, pap tests (cervical screening), Crohn’s disease, chemotherapy-related anaemia, haemophilia, multiple myeloma, relapsed follicular lymphoma and surgery for oesophagogastric cancer. One DCE was conducted exclusively online. Most other studies used a mix of online as well as paper-based questionnaires. In terms of triplet versus pairs, most studies used choice sets based on pairs of alternatives (see Appendix II, Online Resource 1).
4.3 Paired Comparisons
The method of paired comparisons was first introduced by Thurstone [65]. In a paired comparison, objects or conditions are presented in pairs. The respondents are asked to state which one they prefer. The method of paired comparisons is mostly used when the objects to be compared can only be judged subjectively [66]. Paired comparisons were the chosen methods of preference elicitation in four studies that analysed preferences and judgement for urinary incontinence [67], schizophrenia [68], T3-laryngeal cancer [69] and diabetes mellitus [70]. These studies were published between 1995 and 2008 (see Appendix III, Online Resource 1).
4.4 Time Trade-Offs, Probability Trade-Offs
The use of the TTO method in healthcare is based on the work by Torrance et al [71]. TTOs are used to value health states and determine the quality of life of a patient. Like the SG, the TTO has generally a theoretical foundation in utility theory. Both ask people to trade one thing they value in order to gain another thing they place a higher value on. TTO and SG offer an estimation of quality-adjusted life years (QALYs) [8].
Eight studies, published between 1995 and 2010, elicited preferences using the TTO as well as resource or probability trade-offs [69, 72–78]. Conditions of interest included T3-laryngeal cancer, arthritis, physical disabilities, surgery for colorectal cancer, laryngectomy, hypertension, breast cancer chemotherapy and head and neck cancer (see Appendix IV, Online Resource 1).
4.5 Standard Gamble
The SG method was developed by von Neumann and Morgenstern in 1944 [79] and is based directly on their expected utility theory. It is a classical model of measuring preferences under uncertainty and cardinal utility [79]. In an SG, quality weights for health states are generated by comparing a certain number of years in a given health state with a treatment (gamble) that can lead to two outcomes: either full health or immediate death [15].
Conditions studied to elicit preferences of patients and judgements of doctors using an SG included chorionic villus sampling (CVS) to amniocentesis, open tibial fracture, chronic bronchitis, schizophrenia, hepatitis C, surgery for colorectal cancer, arthritis, musculoskeletal diseases, T3-laryngeal cancer and valuation of birth outcomes. Together, ten studies published between 1989 and 2011 [68, 69, 76, 78, 80–85] were found (see Appendix V, Online Resource 1).
4.6 Controlled Preference Scale and Prospective Preference Measure
Next to the five classical methods of preference elicitation, the literature research revealed two studies using the controlled preference scale. The controlled preference scale encompasses five cards that each portray a different role in treatment decision making, from which the patient has to choose [86]. The analysed studies included paired comparisons and they assessed patient involvement in breast cancer treatment decisions [87] as well as rectal cancer treatment [88]. The method of prospective measure of preference (PMP) presents a modification of the TTO and the SG methods [89]. The PMP includes willingness to gamble/willingness to trade as well as a prospective measure of preferences (standard) gamble. This method was used for Crohn’s disease [89] and colorectal cancer [90] (Appendix VI, Online Resource 1).
We also considered two reviews by Stein [16] and Montgomery and Fahey [30] to evaluate our findings. Both provided a review of studies comparing patient preferences and physician judgements using different methodological approaches.
Montgomery and Fahey [30] provided a review of scientific articles published between 1994 and 2001, analysing concordance between patients and physicians. They concluded that there are clear differences in treatment preferences between patients and health professionals. However, magnitude and direction may vary with the clinical condition of interest. Similarly, Stein [16] concluded in his review of ten studies using the TTO method that there are significant differences between patients and physicians.
5 Does Congruence of Preferences and Judgements Depend on Elicitation Techniques?
The review of the studies in terms of the elicitation technique was based on the research question of whether different techniques can lead to different results concerning the consistency between patients and doctors, or not. However, it cannot be concluded that one certain method or technique always results in a disagreement while another method always results in agreement.
5.1 Discrete Choice Experiment
Looking at the DCE studies, it is obvious that the research question cannot be clearly answered. The DCE does not always result in a higher degree of agreement or disagreement than other techniques used. However, it can be stated that out of the ten studies involving a DCE, eight resulted in a high degree of commonality among patients, healthcare professionals and other stakeholder groups [18, 57, 60–62, 64]. The rankings by the diverse groups are quite similar. One study resulted in disagreement between patients and physicians about how much risk is tolerable for improvement in efficacy. However, this study also showed that there are no statistically significant differences in physician judgements for different patient profiles/situations [59].
Finally, two studies using the DCE resulted in a high degree of disagreement [46, 58]. Both studies revealed that doctors tend to overestimate effectiveness/efficacy and underestimate side effects. Physicians often underestimated the importance of the preferences of those affected, especially in terms of quality of life.
5.2 Conjoint Analyses
Similar to DCEs, studies employing CA do not show a common result. As with DCEs, there are several studies supporting the assumption that patient preferences and doctors’ judgement differ constantly. Contrary to DCEs, CAs more often support the assumption of differences. Out of the 13 studies, we found nine that resulted in a certain rate of disagreement, while only four resulted in similar rankings [34, 37, 38, 45]. As with all other techniques, some studies resulted in similar rankings, but different strengths of preferences [37].
5.3 Time Trade-Off, Probability Trade-Off, Resource Trade-Off
The group of studies that used the TTO or any other trade-off showed differences in preferences and judgements between patients and physicians. All studies that were included in the review showed statistically significant differences between the two groups [72, 74, 75, 77, 78]. Patients tended to place higher value on effectiveness/efficacy [72], while physicians seemed to overestimate (health-related) quality of life [75, 77] and underestimated time of survival [75].
5.4 Standard Gamble
We found one study that facilitated a comparison of different elicitation techniques. Suarez-Almazor and Conner-Spady compared TTO and SG [78]. They found statistically significant differences among patients, the public and physicians. Moreover, their results showed significant differences in both TTO and SG and among all three groups. The SG method resulted in higher valuations of health states by doctors compared with the public’s ratings. Patient ratings fell in between.
Studies that used only the SG method to elicit preferences and judgements all resulted in significant differences between the assessed stakeholder groups (patients, physicians, general public). Like the TTO before, this group strengthens the idea of a non-existing concordance among the groups. All eight studies showed different ratings and different utility values placed on the attributes [69, 76, 80, 81, 83–85]. While patients focus on quality of life [81], doctors place higher value on outcome quality [81] and underestimate survival rates [76]. However, another study concluded that physicians overestimated survival and rated their patients’ health status higher than the patients themselves did [84]. Surprisingly, the SG studies also showed that the general public assessments are consistent with clinician assessments [85].
5.5 Paired Comparison
The literature review also included one study that compared SG and paired comparison as means of eliciting preferences and judgements of patients, caregivers and physicians. It found that correlations between physician-rated, patient-rated and caregiver-rated health states were uniformly high, regardless of the technique used [68]. Out of the other three studies using paired comparison, all resulted in reasonable agreement between patients, physicians and public or family caregiver [67, 68, 70]. Overall, patient preferences were mostly comparable with clinician and caregiver preferences. When comparing the preferences and judgement of patients and their relatives, Pfisterer et al. [67] found that next-of-kin showed almost perfect agreement with patient preferences.
5.6 Control Preference Scale
Two studies used the control preference scale to elicit patient preferences and attending physician judgements concerning their role in the process of decision-making during the treatment. Pieterse et al. [88] showed that there is a certain consistency in that both patients and physicians preferred treatment decisions to be a shared process. To the contrary, Janz et al. [87] concluded that there are differences and robust disagreement between both groups.
5.7 Prospective Measure of Preferences
Two studies used the technique of PMP to elicit preferences and judgements [89, 90]. Both studies revealed consistently different results. Patients’ preferences often do not correspond with the preferences of attending physicians.
6 Does Congruence of Preferences and Judgements Depend on Conditions?
6.1 Chronic Conditions
Respondents tended to give similar statements whenever the conditions or services of interest were not directly linked to a potentially life-threatening condition or to severe side effects. There is a higher concordance between patients and experts (physicians, nurses, other healthcare professionals) when the condition is a chronic disease or the service is preventative. Accordingly, the analysed studies revealed a high degree of consistency in conditions like psoriasis, diabetes, anaemia, haemophilia or services including screenings during pregnancy (for Down’s Syndrome, Chorionic Villius Sampling/CVS), Pap tests, wound dressing, supply of hearing aids and decision making during treatment (see Table 2).
6.2 Acute Conditions
However, it became clear that patients and doctors tended to show different preferences whenever the analysed condition was more acute, potentially life threatening, or at least connected with severe side effects or limitations to daily life. Consequently, significant differences were found, among others, for spinal surgery, open tibial fracture, cardiovascular diseases, cardiac risk assessment, cancer (colorectal cancer, rectal cancer, and laryngeal cancer), acute respiratory illness, multiple myeloma, cataract surgery, hepatitis C, physical disabilities or musculoskeletal diseases.
6.3 Construal Level Theory
The initial research question was whether agreement between patients and experts depends on the psychological distance of the decision maker, influenced by the time to utilization of healthcare services or interventions. Following the findings on acute and chronic conditions, the construal level theory and especially the psychological and (inter-)personal distances can be supported. The theory states that the more abstract and further away a disease is, the easier it is for a patient to make decisions rationally and reasonably [1, 4–6]. This said, a patient confronted with a chronic disease does not act as emotionally and irrationally as a patient diagnosed with a life-threatening condition (psychological distance). The (inter-)personal distance may explain the differences concerning acute conditions. While the physician always decided rationally, the patient is in a ‘hot state’. This indicates that he or she is making a decision on a more emotional and less rational basis.
7 Does Congruence of Preferences and Judgements Depend on the Attributes?
To structure the several attributes used in the studies, we decided to follow Donabedian [91]. He proposed the differentiation based on structures, processes and outcomes of healthcare. Figure 1 (see Appendix VII, Online Resource 1) displays the attributes and assessment criteria that were used in the reviewed studies.
7.1 Attributes Focusing on Outcomes
Most of the reviewed studies focussed on outcome quality. They included attributes such as pain, time to improvement, risk of morbidity and mortality or overall effectiveness/efficacy of treatment. Given the initial research question on differences in terms of attributes, it has to be stated that this cannot be supported in terms of outcome quality. All analysed studies showed varying results. There were several studies indicating that patients and physicians value the same attributes when making a decision. However, there were as many studies showing huge differences with regard to treatment outcomes. In between, there were studies that indicated that the groups value the same attributes when choosing a treatment and make the same rankings, but with slightly different preferences strengths [63].
Byrne et al. showed gastroenterologists were more likely to be willing to gamble avoiding radical treatment compared with surgeons and patients [89]. Additionally, Johnson et al. concluded that physicians and patients disagreed about how much risk is tolerable for improvements in efficacy. Patients were less tolerant in trading risk than were physicians who also placed high value on effectiveness/efficacy [59].
Overall, experts tended to place higher value on clinical outcomes than patients did [81]. The patients tended to place much higher values on long-term side effects [76] as well as on quality of life than doctors did [16, 33, 77]. One study revealed that 88 % of patients and even 87 % of healthcare professionals doubted that clinicians could properly weigh the quality value of individual patient rights when comparing that to length of life [87]. The only study in which both respondent groups valued quality of life in similar ways was Gregorian et al. [36]. This study assessed pain relief and opioid side effects.
Two other studies revealed that physicians underestimated time of survival [75, 76]. Suarez-Almazor et al. [78, 84] stated that physicians rated their patients’ health status higher than the patients themselves did and overestimated survival [84].
7.2 Attributes Focusing on Process and Outcomes
In 16 of 44 studies (reviews not included), the authors decided to apply a mix of attributes focussing on both process and outcome quality. All the studies analysed revealed varying results. Casparie and van der Waal [70] stated that patients valued attributes focussing on process quality higher, while doctors paid higher attention to outcomes.
Patients generally placed higher values than physicians on side effects occurring during the treatment process [85]. Healthcare professionals placed more importance on treatment outcomes [37] and effectiveness/efficacy of procedure during the treatment process [58] than patients did. However, physicians as well as patients valued effectiveness/efficacy higher than any other attribute when selecting an erythropoietic agent to treat chemotherapy-related anaemia [60]. With respect to wound dressing, preferences related to time for procedure, pain, frequency and required duration of hospitalization were similar for doctors, nurses and patients. In this study, patients and physicians also valued effectiveness/efficacy very highly [45]. Hypertension patients were less likely to accept antihypertensive therapy than physicians; they wanted greater benefits prior to accepting treatment. Therefore, the authors of the study concluded that patients place higher value on effectiveness/efficacy [74].
As already shown with outcome quality, studies focusing on process and outcomes additionally show that experts overestimate clinical outcomes [41] and side effects [39]. Moreover, patients tended to prefer testing safety, while physicians rated timeliness higher when asked to choose a preventive screening [38].
On the other hand, Meister et al. [39] documented that clinicians overestimated the importance of all process and outcome quality-related attributes in terms of supply of hearing aids (handling, cost, comfort, speech perception). Complementary to these findings, Mühlbacher and Nübling [46] concluded that there are different estimates between patients and physicians. According to this study, physicians underestimated the importance of aspects of medical effectiveness/efficacy, side effects and quality of life from the perspective of those affected. As shown before, the analysis of outcome and process parameters also revealed studies that indicated that patients and physicians value the same attributes when choosing a treatment and make similar rankings, but with slightly different strengths of preferences [61].
7.3 Attributes Focusing on Process
We found six studies that focused solely on attributes or assessment criteria for process quality. Two of these studies showed either a slight agreement between patients and other groups or nearly perfect agreement. In the latter, the authors concluded that patients and attending physicians placed the same preferences or judgements on the role they want to play in decision making for the treatment process [88]. In terms of process quality, it becomes clear that patients’ preferences often do not correspond with the preferences of physicians. While patients seem to deny most forms of radical treatment in cancer therapy, experts favour it [90]. Moreover, physicians underestimated side effects that might occur during the treatment process [83]. In terms of organizing aftercare, patients had a higher preference value for process quality than did physicians [35]. Mantonavi et al. [61] concluded that preferences and judgements diverged most on attributes related to the process of care.
7.4 Attributes Focusing on Structure
In the literature review we found only one study that applied attributes referring to structure quality. Thrumurthy et al. [64] included the attribute ‘hospital type’ in their DCE. Results showed similar ratings for patients and physicians, with both groups placing the hospital type as their lowest preference.
Overall, it can be stated that several common attributes are used to elicit preferences and judgements, resulting in diverse assessments by the two groups. Physicians generally overestimated the value that patients place on clinical outcomes, safety and effectiveness/efficacy. On the other hand, patients put much more importance on quality of life and social values than physicians believed.
8 Does Congruence Vary Within Different Groups of Respondents?
In addition to the three initial questions, we found certain insights in concordance or disconcordance between patients and family caregivers or between different medical specialties [40, 89]. Four studies compared patients’ preferences with the preferences of the general public.
Jalukar et al. [72] found that there are very similar perspectives between healthcare professionals and patients, but significant differences between patients and medical students. This implies the need to incorporate patient preferences and knowledge about diverging patient needs and priorities into the medical training of future doctors. Sampietro-Colom et al. [42] found a high consistency between the general public and patients/relatives. In another CA, the same authors reinforced these findings [43].
In terms of cardiac risk assessment, Sassi et al. [44] found that the public attached at least three times more importance to prognostic value than did general practitioners. In contrast to this, van der Donk et al. [69] found higher Quality-Adjusted Life Expectancy (QALE) scores in clinicians and for the general public than in patients in the assessment of T3-Laryngeal cancer. Moreover, the general public was consistent with clinicians.
When comparing the preferences and judgements of patients and their relatives, Pfisterer et al. [67] found that next-of-kin showed almost perfect agreement with patients. This indicates that it might be possible to involve relatives speaking on behalf of patients in preference studies if the patients are too ill or unable to answer properly.
9 Discussion
There has been a lot of discussion about which preferences should be crucial for health policy decisions [92]. A major argument for the consideration of patient preferences is the fact that the patients are affected by the consequences of a disease and know the possible impact on their quality of life through their own experience. According to Article IV of the Declaration of Alma Ata (1978), the right, and even the duty, to participate in the planning and implementation of health services lies with the people [93]. Following this, the public should be involved in healthcare decision making, particularly when decision makers in politics and self-government are faced with the difficult task of setting priorities [94].
As the review has shown, preferences and judgements by different stakeholders are not always congruent. Therefore, a decision has to be made on when to consider patients and when to take public preferences into account. To our understanding this can be done based on two levels. On a lower level, when concrete measures and procedures have to be assessed, the assessment can only be done by persons who are experienced in the particular disease. Hence, patient’s preferences should be considered. When decisions are made on a higher level, for example, in terms of discussions of values and norms, the preferences of the public should be considered.
While analysing the studies and the conclusions of the authors, it became obvious that studies can be defined with three different distinctions:
-
A study that concludes that preferences and judgements show no meaningful or significant difference.
-
A study that concludes that preferences and judgements show no meaningful or significant difference in the ranking of attributes, but meaningful differences of strengths.
-
A study that concludes that preferences and judgements show meaningful or significant differences.
Overall, we found 11 studies that stated a reasonable agreement between patients and physicians [18, 34, 36, 38, 57, 60, 62, 68, 80, 82, 88] as well as 11 studies supporting the second distinction [35, 37, 39, 45, 46, 59, 61, 63, 64, 70, 72]. In addition, there are 23 studies that show poor concordance between actual patient preferences and physician judgement. This implies that many experts do not know their patients’ preferences, and so cannot give recommendations based on patients’ needs and values. One study, Leu et al. [82], could not be included in this analysis because the authors did not provide a conclusion on agreement between patients and physicians.
Because differences exist between physician judgement and patient preferences, it is important to integrate the needs and wants of the patient into treatment decisions. Also, patient perceptions and experiences related to quality (structure, process, outcome quality) during past treatments might influence patient preferences or choices. This should be considered in future research.
As these studies show, the preferences of physicians and patients relating to diverse disease states or treatment options can differ substantially. This observation reinforces the importance of considering patient as well as public perspectives and values when making significant healthcare decisions. Patient-centred outcomes will provide objective information about the impact of patient involvement—the experiences, as well as the needs and wants of patients. Patient preference data will help insurers, policy makers and others promote patient-centred coordinated care as the new standard of primary care.
Evidence-based decisions on the macro level encompass all fields of healthcare delivery, from disease management, quality improvement and performance measurement to medical necessity, regulations and public policy [31]. This is important for two reasons. First is the lack of information, meaning that preferences can only be taken into account when the required information is available. Second is a lack of physician sensibility to the needs and preferences of their patients. Even if information on patient and public preferences is available, doctors still need to be aware of it to make lasting changes to the delivery system.
9.1 Future Research
As this review has shown, there are noticeable differences between patient preferences and physician judgement. As seen, there is a higher concordance with DCE and paired comparisons than with CA. Our results indicate that there is a higher concordance with chronic rather than with acute conditions. Future research should evaluate whether results are influenced by the type of treatment, certain lifestyle changes or management options. Moreover, patient perception and quality experience (structure, process, and outcome) during past treatments may influence patient preferences or choices. This should be considered in future healthcare research. Finally, the influence of a particular design of the preference study (e.g. presentation of tasks, information given to respondents) could be addressed in future studies.
9.2 Limitations
This review has several potential limitations. The greatest limitation lies in the diversity of methods and techniques used to elicit preferences. As each study uses different scales and measures for statistical analysis, the comparability of the results is limited. A universal statement is hardly possible. Similarly, the means of assessing the quality of the reviewed studies are rather limited. The review had to rely on the data and description of the study design given in the publication. A conclusion on differences based on different designs or ways of elicitation is difficult to draw. Additionally, the possibility of comparing patient preferences and expert judgement within one study is partly methodically limited. Sassi et al. [44] and Fiebig et al. [18] used different questionnaires for the patient and the expert population. So, a conclusion on the congruence or disagreement between patients and experts is difficult to make.
Moreover, it is not clear whether all the studies used the same paradigm or context for the questions. The method of introducing choices and the information the respondents had (e.g., the personal situation or consequences of their choices) is not always replicable. This problem was inherent in all studies. Another important point to address is the fact that differences between patient preferences and expert judgement may also be due to the characteristics of respondents as well as the methods themselves. Some methods are seen to be more cognitively demanding than others. The same might be true for attributes that can easily be too complex or misleading, especially in the patient population.
Special interest in this review was paid to CA and DCEs. However, these methods have limitations as well. The primary critique is that DCE studies provide information about hypothetical choices, which may differ from real-world choices. Studies that have compared DCE preferences to actual choices, such as the physical activity studies and field experiments conducted by Brown et al. [95] and Finkelstein et al. [96] found good agreement. However, ‘revealed’ data on actual choices have numerous limitations, and they provide no information about new or emerging testing options; that is, DCEs provide the ability to study objectives that would be infeasible or impossible to actually observe. Further, DCEs are efficient tools for exploratory research, since a wide range of policy options can be considered without the expense of RCTs.
10 Conclusion
The role of patients has changed significantly in recent years. Patients are encouraged to get involved in healthcare decision making and patient preferences are increasingly given weight. Patient or public preferences should also be considered on the macro level and should help support decisions on the design of healthcare systems and the allocation of limited resources. Aligning clinical practice and health policy with patient preferences will improve the effectiveness/efficacy of health interventions.
This article has summarized the results of various studies; most of them demonstrate a disparity between the preferences of actual patients and the judgement of physicians. For most conditions, physicians overestimated effectiveness/efficacy and underestimated the impact of side effects or treatment effects on patients as well as their quality of life. Differences in perceptions may be due, in part, to ineffective communication between the provider and the patient. This could be keeping physicians from fully appreciating the impact of certain medical conditions on patient preferences [16].
References
Trope Y, Liberman N. Construal-level theory of psychological distance. Psychol Rev. 2010;117(2):440.
Liberman N, Trope Y, Wakslak C. Construal level theory and consumer behavior. J Consumer Psychol. 2007;17(2):113–7.
Trope Y, Liberman N. Temporal construal. Psychol Rev. 2003;110(3):403–21.
Bar-Anan Y, Liberman N, Trope Y. The association between psychological distance and construal level: evidence from an implicit association test. J Exp Psychol Gen. 2006;135(4):609–22.
Nan X. Social distance, framing, and judgment: a construal level perspective. Human Commun Res. 2007;33(4):489–514.
Ariely D. The upside of irrationality: the unexpected benefits of defying logic at work and at home. Harper, 2011.
Green PE, Srinivasan V. Conjoint analysis in marketing: new developments with implications for research and practice. J Market. 1990;54(4):3–19.
Dolan P, Gudex C, Kind P, Williams A. The time trade-off method: results from a general population study. Health Econ. 1996;5(2):141–54.
Mühlbacher A, Juhnke C, Bethge S. Experts’ judgement on patient-centered coordinated care. Value Health. 2010;13(7):A337.
Australian Research Council. Summary of Successful Linkage: Projects Proposals for Funding to Commence in 2010 by State and Organisation. Canberra: Australian Government; 2010.
Stafinski T, Menon D, Philippon DJ, McCabe C. Health technology funding decision-making processes around the world: the same, yet different. PharmacoEconomics. 2011;29(6):475–95.
National Institute for Health and Clinical Excellence. Patient and public involvement policy [online]. http://www.nice.org.uk/getinvolved/patientandpublicinvolvement/patient_and_public_involvement.jsp. Accessed 25 Feb 2013.
Billings JA, Krakauer EL. On patient autonomy and physician responsibility in end-of-life care. Arch Intern Med. 2011;171(9):849–53.
Telser H, Becker K, Zweifel P. Validity and reliability of willingness-to-pay estimates: evidence from two overlapping discrete-choice experiments. Patient. 2008;1(4):283–98.
Bleichrodt H, Johannesson M. Standard gamble, time trade-off and rating scale: experimental results on the ranking properties of QALYs. J Health Econ. 1997;16(2):155–75.
Stein JD. Disparities between ophthalmologists and their patients in estimating quality of life. Curr Opin Ophthalmol. 2004;15(3):238.
Haynes RB, Devereaux P, Guyatt GH. Physicians’ and patients’ choices in evidence based practice. BMJ. 2002;324(7350):1350.
Fiebig DG, Haas M, Hossain I, Street DJ, Viney R. Decisions about Pap tests: what influences women and providers? Soc Sci Med. 2009;68(10):1766–74.
Charles C, Gafni A, Whelan T. Shared decision-making in the medical encounter: what does it mean? (or it takes at least two to tango). Soc Sci Med. 1997;44(5):681–92.
Robinson A, Thomson R. Variability in patient preferences for participating in medical decision making: implication for the use of decision support tools. Qual Health Care. 2001;10(Suppl. 1):i34–8.
Sackett DL, Rosenberg W, Gray J, Haynes RB, Richardson WS. Evidence based medicine: what it is and what it isn’t. BMJ. 1996;312(7023):71–2.
van Til JA. Integrating preferences into decision making: the treatment of ankle-foot impairment in stroke [dissertation]. Enschede: University of Twente; 2009.
Ford S, Schofield T, Hope T. What are the ingredients for a successful evidence-based patient choice consultation? A qualitative study. Soc Sci Med. 2003;56(3):589–602.
Edwards A, Elwyn G, Wood F, Atwell C, Prior L, Houston H. Shared decision making and risk communication in practice: a qualitative study of GPs’ experiences. Br J Gen Pract. 2005;55(510):6–13.
Edwards A, Elwyn G. Inside the black box of shared decision making: distinguishing between the process of involvement and who makes the decision. Health Expect. 2006;9(4):307–20.
Speedling EJ, Rose DN. Building an effective doctor–patient relationship: from patient satisfaction to patient participation. Soc Sci Med. 1985;21(2):115–20.
Holmes-Rovner M, Valade D, Orlowski C, Draus C, Nabozny-Valerio B, Keiser S. Implementing shared decision-making in routine practice: barriers and opportunities. Health Expect. 2000;3(3):182–91.
Andersen RM. Revisiting the behavioral model and access to medical care: does it matter? J Health Soc Behav. 1995;36(1):1–10.
Mühlbacher AC, Bethge S, Ekert S, Tockhorn A, Nübling M. Der Wert von Innovationen im Gesundheitswesen: Spielen die Patientenpräferenzen eine Rolle. RPG Recht und Politik im Gesundheitswesen. 2008;14(2):53–62.
Montgomery A, Fahey T. How do patients’ treatment preferences compare with those of clinicians? Qual Health Care. 2001;10(Suppl. 1):i39–43.
Eddy DM. Evidence-based medicine: a unified approach. Health Aff. 2005;24(1):9–17.
Amaya-Amaya M, Gerard K, Ryan M. Discrete choice experiments in a nutshell. In: Ryan M, Gerard K, Amaya-Amaya M, editors. Using discrete choice experiments to value health and health care. Dordrecht: Springer; 2008. pp. 13–46.
Bederman SS, Mahomed NN, Kreder HJ, McIsaac WJ, Coyte PC, Wright JG. In the eye of the beholder: preferences of patients, family physicians, and surgeons for lumbar spinal surgery. Spine (Phila Pa 1976). 2010;35(1):108–15.
Bishop AJ, Marteau TM, Armstrong D, Chitty LS, Longworth L, Buxton MJ, Berlin C. Women and health care professionals’ preferences for Down’s syndrome screening tests: a conjoint analysis study. BJOG. 2004;111(8):775–9.
Bunch WH, Chapman RG. Patient preferences in surgery for scoliosis. J Bone Joint Surg Am. 1985;67(5):794–9.
Gregorian RS Jr, Gasik A, Kwong WJ, Voeller S, Kavanagh S. Importance of side effects in opioid treatment: a trade-off analysis with patients and physicians. J Pain. 2010;11(11):1095–108.
Lee A, Gin T, Lau AS, Ng FF. A comparison of patients’ and health care professionals’ preferences for symptoms during immediate postoperative recovery and the management of postoperative nausea and vomiting. Anesth Analg. 2005;100(1):87–93.
Lewis SM, Cullinane FM, Carlin JB, Halliday JL. Women’s and health professionals’ preferences for prenatal testing for Down syndrome in Australia. Aust N Z J Obstet Gynaecol. 2006;46(3):205–11.
Meister H, Lausberg I, Kiessling J, Walger M, von Wedel H. Determining the importance of fundamental hearing aid attributes. Otol Neurotol. 2002;23(4):457–62.
Pieterse AH, Stiggelbout AM, Baas-Thijssen MC, van de Velde CJ, Marijnen CA. Benefit from preoperative radiotherapy in rectal cancer treatment: disease-free patients’ and oncologists’ preferences. Br J Cancer. 2007;97(6):717–24.
Porzsolt F, Clouth J, Deutschmann M, Hippler HJ. Preferences of diabetes patients and physicians: a feasibility study to identify the key indicators for appraisal of health care values. Health Qual Life Outcomes. 2010;8:125.
Sampietro-Colom L, Espallargues M, Comas M, Rodriguez E, Castells X, Pinto JL. Prioritizing patients on waiting list for cataract surgery: preference differences among citizens. Gac Sanit. 2006;20(5):342–51.
Sampietro-Colom L, Espallargues M, Rodriguez E, Comas M, Alonso J, Castells X, Pinto JL. Wide social participation in prioritizing patients on waiting lists for joint replacement: a conjoint analysis. Med Decis Making. 2008;28(4):554–66.
Sassi F, McDaid D, Ricciardi W. Conjoint analysis of preferences for cardiac risk assessment in primary care. Int J Technol Assess Health Care. 2005;21(2):211–8.
Vermeulen H, Ubbink DT, de Zwart F, Goossens A, de Vos R. Preferences of patients, doctors, and nurses regarding wound dressing characteristics: a conjoint analysis. Wound Repair Regen. 2007;15(3):302–7.
Mühlbacher AC, Nübling M. Analysis of physicians’ perspectives versus patients’ preferences: direct assessment and discrete choice experiments in the therapy of multiple myeloma. Eur J Health Econ. 2011;12(3):193–203.
de Bekker Grob EW, Ryan M, Gerard K. Discrete choice experiments in health economics: a review of the literature. Health Econ. 2012;21(2):145–72.
Mühlbacher AC, Rudolph I, Lincke HJ, Nübling M. Preferences for treatment of attention-deficit/hyperactivity disorder (ADHD): a discrete choice experiment. BMC Health Serv Res. 2009;9:149.
Dolan P, Olsen JA, Menzel P, Richardson J. An inquiry into the different perspectives that can be used when eliciting preferences in health. Health Econ. 2003;12(7):545–51.
Marshall D, Bridges JFP, Hauber B, Cameron R, Donnalley L, Fyie K, Johnson FR. Conjoint analysis applications in health how are studies being designed and reported? An update on current practice in the published literature between 2005 and 2008. Patient. 2010;3(4):249–56.
Ryan M, Bate A, Eastmond CJ, Ludbrook A. Use of discrete choice experiments to elicit preferences. Qual Health Care. 2001;10(Suppl. 1):i55–60.
McFadden D. Conditional logit analysis of qualitative choice behavior. Zarembka. 1974;1:105–42.
Thurstone LL. A law of comparative judgment. Psychol Rev. 1927;34:273–86.
Manski CF. The structure of random utility models. Theory Decis. 1977;8(3):229–54.
Lancaster KJ. A new approach to consumer theory. J Polit Econ. 1966;74(2):132–57.
Ryan M, Gerard K, Amaya-Amaya M. Using discrete choice experiments to value health and health care. Dordrecht: Springer; 2008.
Ashcroft DM, Seston E, Griffiths CE. Trade-offs between the benefits and risks of drug treatment for psoriasis: a discrete choice experiment with U.K. dermatologists. Br J Dermatol. 2006;155(6):1236–41.
de Bekker-Grob EW, Essink-Bot ML, Meerding WJ, Koes BW, Steyerberg EW. Preferences of GPs and patients for preventive osteoporosis drug treatment: a discrete-choice experiment. Pharmacoeconomics. 2009;27(3):211–9.
Johnson FR, Hauber B, Ozdemir S, Siegel CA, Hass S, Sands BE. Are gastroenterologists less tolerant of treatment risks than patients? Benefit-risk preferences in Crohn’s disease management. J Manag Care Pharm. 2010;16(8):616–28.
Langer CJ, Fastenau JM, Forlenza JB, Tak Piech C, Bolge SC, Gano Allen J, Zilberberg MD. Effectiveness versus convenience: patient preferences for an erythropoietic agent to treat cancer-related anemia. Curr Med Res Opin. 2007;23(1):85–92.
Mantovani LG, Monzini MS, Mannucci PM, Scalone L, Villa M, Gringeri A. Differences between patients’, physicians’ and pharmacists’ preferences for treatment products in haemophilia: a discrete choice experiment. Haemophilia. 2005;11(6):589–97.
Seston EM, Ashcroft DM, Griffiths CE. Balancing the benefits and risks of drug treatment: a stated-preference, discrete choice experiment with patients with psoriasis. Arch Dermatol. 2007;143(9):1175–9.
Shafey M, Lupichuk SM, Do T, Owen C, Stewart DA. Preferences of patients and physicians concerning treatment options for relapsed follicular lymphoma: a discrete choice experiment. Bone Marrow Transpl. 2011;46(7):962–9.
Thrumurthy SG, Morris JJ, Mughal MM, Ward JB. Discrete-choice preference comparison between patients and doctors for the surgical management of oesophagogastric cancer. Br J Surg. 2011;98(8):1124–31.
Thurstone LL. The method of paired comparisons for social values. J Abnorm Soc Psychol. 1927;21(4):384.
David HA. The method of paired comparisons. In: Proceedings of The Fifth Conference on the Design Of Experiments In Army Research Developments and Testing, Durham, 1960.
Pfisterer MH, Johnson TM 2nd, Jenetzky E, Hauer K, Oster P. Geriatric patients’ preferences for treatment of urinary incontinence: a study of hospitalized, cognitively competent adults aged 80 and older. J Am Geriatr Soc. 2007;55(12):2016–22.
Revicki DA, Shakespeare A, Kind P. Preferences for schizophrenia-related health states: a comparison of patients, caregivers and psychiatrists. Int Clin Psychopharmacol. 1996;11(2):101–8.
van der Donk J, Levendag PC, Kuijpers AJ, Roest FH, Habbema JD, Meeuwis CA, Schmitz PI. Patient participation in clinical decision-making for treatment of T3 laryngeal cancer: a comparison of state and process utilities. J Clin Oncol. 1995;13(9):2369–78.
Casparie AF, van der Waal MA. Differences in preferences between diabetic patients and diabetologists regarding quality of care: a matter of continuity and efficiency of care? Diabet Med. 1995;12(9):828–32.
Torrance GW. Utility approach to measuring health-related quality of life. J Chronic Dis. 1987;40(6):593–600.
Jalukar V, Funk GF, Christensen AJ, Karnell LH, Moran PJ. Health states following head and neck cancer treatment: patient, health-care professional, and public perspectives. Head Neck. 1998;20(7):600–8.
Mandelblatt JS, Sheppard VB, Hurria A, Kimmick G, Isaacs C, Taylor KL, et al. Breast cancer adjuvant chemotherapy decisions in older women: the role of patient preference and interactions with physicians. J Clin Oncol. 2010;28(19):3146–53.
McAlister FA, O’Connor AM, Wells G, Grover SA, Laupacis A. When should hypertension be treated? The different perspectives of Canadian family physicians and patients. CMAJ. 2000;163(4):403–8.
Otto RA, Dobie RA, Lawrence V, Sakai C. Impact of a laryngectomy on quality of life: perspective of the patient versus that of the health care provider. Ann Otol Rhinol Laryngol. 1997;106:693–99.
Solomon MJ, Pager CK, Keshava A, Findlay M, Butow P, Salkeld GP, Roberts R. What do patients want? Patient preferences and surrogate decision making in the treatment of colorectal cancer. Dis Colon Rectum. 2003;46(10):1351–7.
Stineman MG, Maislin G, Nosek M, Fiedler R, Granger CV. Comparing consumer and clinician values for alternative functional states: application of a new feature trade-off consensus building tool. Arch Phys Med Rehabil. 1998;79(12):1522–9.
Suarez-Almazor ME, Conner-Spady B. Rating of arthritis health states by patients, physicians, and the general public. Implications for cost-utility analyses. J Rheumatol. 2001;28(3):648–56.
Von Neumann J, Morgenstern O. Theory of games and economic behavior. Princeton: Princeton University Press; 1944.
Bryce RL, Bradley MT, McCormick SM. To what extent would women prefer chorionic villus sampling to amniocentesis for prenatal diagnosis? Paediatr Perinat Epidemiol. 1989;3(2):137–45.
Chung KC, Shauver MJ, Saddawi-Konefka D, Haase SC. A decision analysis of amputation versus reconstruction for severe open tibial fracture from the physician and patient perspectives. Ann Plast Surg. 2011;66(2):185–91.
Leu RE, Gerfin M, Spycher S. The validity of the MIMIC (Multiple Indicators/MultIple Causes) health index: some empirical evidence. Dev Health Econ Public Policy. 1992;1:109–42.
Schackman BR, Teixeira PA, Weitzman G, Mushlin AI, Jacobson IM. Quality-of-life tradeoffs for hepatitis C treatment: do patients and providers agree? Med Decis Making. 2008;28(2):233–42.
Suarez-Almazor ME, Conner-Spady B, Kendall CJ, Russell AS, Skeith K. Lack of congruence in the ratings of patients’ health status by patients and their physicians. Med Decis Making. 2001;21(2):113–21.
Vandenbussche FP, De Jong-Potjer LC, Stiggelbout AM, Le Cessie S, Keirse MJ. Differences in the valuation of birth outcomes among pregnant women, mothers, and obstetricians. Birth. 1999;26(3):178–83.
Degner LF, Sloan JA, Venkatesh P. The control preferences scale. Can J Nurs Res. 1997;29(3):21–43.
Janz NK, Wren PA, Copeland LA, Lowery JC, Goldfarb SL, Wilkins EG. Patient–physician concordance: preferences, perceptions, and factors influencing the breast cancer surgical decision. J Clin Oncol. 2004;22(15):3091–8.
Pieterse AH, Baas-Thijssen MC, Marijnen CA, Stiggelbout AM. Clinician and cancer patient views on patient participation in treatment decision-making: a quantitative and qualitative exploration. Br J Cancer. 2008;99(6):875–82.
Byrne CM, Solomon MJ, Young JM, Selby W, Harrison JD. Patient preferences between surgical and medical treatment in Crohn’s disease. Dis Colon Rectum. 2007;50(5):586–97.
Harrison JD, Solomon MJ, Young JM, Meagher A, Butow P, Salkeld G, Hruby G, Clarke S. Patient and physician preferences for surgical and adjuvant treatment options for rectal cancer. Arch Surg. 2008;143(4):389.
Donabedian A. Evaluating the quality of medical care. Milbank Mem Fund Q. 1966;44(3):166–206.
Gandjour A. Theoretical foundation of patient v. population preferences in calculating QALYs. Med Decis Mak. 2010;30(4):E57–63.
World Health Organization. Declaration of Alma-Ata: International Conference on Primary Health Care. Alma-Ata: USSR; 1978.
Caddy J, Vergez C. Citizens as partners: information, consultation and public participation in policy-making. Paris: Organisation for Economic Cooperation and Development (OECD); 2001.
Brown DS, Finkelstein EA, Brown DR, Buchner DM, Johnson FR. Estimating older adults’ preferences for walking programs via conjoint analysis. Am J Prev Med. 2009;36(3):201–7, e4.
Finkelstein EA, Brown DS, Brown DR, Buchner DM. A randomized study of financial incentives to increase physical activity among sedentary older adults. Prev Med. 2008;47(2):182–7.
Bederman SS, McIsaac WJ, Coyte PC, Kreder HJ, Mahomed NN, Wright JG. Referral practices for spinal surgery are poorly predicted by clinical guidelines and opinions of primary care physicians. Med Care. 2010;48(9):852–8.
Acknowledgments
Funding: Axel Mühlbacher received a Harkness Fellowship in Health Care Policy and Practice from the Commonwealth Fund, New York. The authors received no additional funding for this paper.
Conflict of interest
The authors declare that they have no conflicts of interest.
Author contributions
ACM designed the study and is the guarantor for the overall content. CJ extracted the relevant data from the databases, and assisted with the interpretation of the results. Both authors contributed equally to writing and revision of the paper and have given final approval of the version to be published.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article
Cite this article
Mühlbacher, A.C., Juhnke, C. Patient Preferences Versus Physicians’ Judgement: Does it Make a Difference in Healthcare Decision Making?. Appl Health Econ Health Policy 11, 163–180 (2013). https://doi.org/10.1007/s40258-013-0023-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40258-013-0023-3