
Abstract
Skin of color, also known as ethnic skin, is described as skin of individuals of African, Asian, Hispanic, Native-American, Middle Eastern, and Pacific Island backgrounds. Differences in hair morphology, hair grooming, cultural practices, and susceptibility to keloid scarring exist within these populations and have been implicated in hair, scalp, and skin disorders. Acne keloidalis (AK), central centrifugal cicatricial alopecia (CCCA), dissecting cellulitis of the scalp (DCS), pseudofolliculitis barbae (PFB), traction alopecia (TA), and keloids are the most prevalent follicular and scarring disorders in skin of color. They have been associated with disfigurement, permanent hair loss, emotional distress, and decreased quality of life. Hair grooming practices, such as the use of chemical relaxers, heat straightening, and tight braiding and weaving can cause scalp irritation and follicular damage and are linked to the pathogenesis of some of these conditions. Consequently, patient education and behavior modifications are integral to the prevention and management of these disorders. Scarring disorders are also of concern in ethnic populations. Keloid scarring is more prevalent in individuals of African, Asian, and Hispanic descent. The scarring alopecia CCCA is almost exclusively seen in patients of African descent. Therapeutic regimens such as intralesional corticosteroids, surgical excision, and laser therapy can be effective for these follicular and scarring disorders, but carry a risk of dyspigmentation and keloid scarring. Ethnic skin and hair may present unique challenges to the clinician, and knowledge of these differences is essential to providing quality care.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Acne keloidalis, central centrifugal cicatricial alopecia, dissecting cellulitis of the scalp, pseudofolliculitis barbae, traction alopecia, and keloids are the most common follicular and scarring disorders in skin of color |
Hair grooming practices, such as the use of chemical relaxing, heat straightening, tight braiding and weaving, and close shaving of tightly coiled hair, are linked to the pathogenesis of these conditions |
Patient education and behavior modifications can help prevent the progression of these conditions |
1 Introduction
Skin of color, also known as ethnic skin, is described as skin of individuals of African, Asian, Hispanic, Native-American, Middle Eastern, and Pacific Island backgrounds. Differences in hair morphology, hair grooming, cultural practices, and susceptibility to keloid scarring exist within these populations and require special consideration by the clinician.
Studies of hair in the Black population have shown differences such as flat elliptical-shaped hair strands, curved hair follicles [1], and fewer elastic fibers anchoring hair follicles to the dermis [2]. Hair strands of Asians are round with the largest cross-sectional area [3]. The structure and texture of ethnic hair has influenced hair-grooming practices, including the use of chemical relaxers, heat styling, and tight braiding and weaving [4]. Cultural practices also influence hair styling [5]. Differences in hair morphology and hair-grooming practices have been implicated in the pathogenesis of hair and scalp disorders in ethnic populations.
In addition to follicular disorders, scarring disorders are of particular concern in ethnic populations. Keloid scarring is more prevalent in those of African, Asian, and Hispanic descent [6]. Central centrifugal cicatricial alopecia (CCCA) is a scarring alopecia almost exclusively seen in patients of African descent [4].
The most prevalent follicular and scarring disorders in skin of color include acne keloidalis (AK), CCCA, dissecting cellulitis of the scalp (DCS), pseudofolliculitis barbae (PFB), traction alopecia (TA), and keloids (Table 1).
In considering therapeutic regimens for ethnic skin, the potential for side effects, such as dyspigmentation and keloid scarring, must be considered. The distinct features of ethnic skin and hair may present unique challenges to the clinician, and knowledge of these differences is essential to providing adequate care.
For our review of literature, we consulted PubMed, EMBASE, Cochrane Library, MD Consult, Web of Science, and Google Scholar with specific search terms (Table 2). Bibliographies of relevant articles were evaluated for further sources. We included cohort and cross-sectional studies, review articles, case reports, and randomized controlled studies with research participants primarily of color from January 1950 to January 2014. Publications not pertaining to pathogenesis, presentation, or management, and publications without objective methods were excluded.
2 Acne Keloidalis
AK is a chronic scarring folliculitis characterized by papules, pustules, and keloidal plaques on the occipital scalp. It was first described by Bazin in 1869 as “dermatitis papillaris capillitii” and later renamed “acne keloidalis” by Kaposi [7]. AK has been described in all races but predominantly affects Black men under the age of 50 years, followed by Hispanic, Asian, and White men [8]. AK also occurs in women [9, 10], with a ratio of occurrence in men to women of 20:1 [11]. Though benign, AK can negatively affect quality of life [12].
2.1 Pathogenesis
The etiology of AK is unclear, but many theories exist. Sperling et al. [13] suggested that AK is a primary cicatricial alopecia, with similar pathogenesis to CCCA. The proposed pathogenesis involves antigens on the follicular epithelium or intrafollicular canal that incite an inflammatory response, damaging follicular components. This damage leaves residual hair shaft and follicular epithelial fragments that can cause hypertrophic scarring and keloid formation. Possible antigens include “demodex, normal skin flora (fungal spores and bacteria) and their metabolic by-products, cosmetics, sebum, and desquamated keratinocytes” [13]. Herzberg et al. [14] described a similar mechanism. Through histopathological evidence, both Sperling et al. [13] and Goette and Berger [15] claim that there is no pathogenic relationship between AK and PFB.
In contrast to the theory that AK is a primary cicatricial alopecia, it has been proposed that AK is induced by mechanical irritation. Trauma from razors and electric clippers along the occipital hairline has been implicated. Salami et al. [12] found that 90 % of 30 cases of AK had the precipitating event of a haircut by a barber. Khumalo et al. [16] also found this association. Burkhart and Burkhart [17] claim that AK is a form of lichen simplex chronicus and that manual scratching induces a follicular foreign body response and can lead to bacterial infection.
It has been suggested that in football players, nuchal acne mechanica (AM) may progress to AK as a result of irritation and secondary infection from helmet use [18]. However, a study of 453 American football players by Knable et al. [19] found that nuchal AM and mechanical irritation from helmet use was not sufficient as a primary cause of AK.
2.2 Presentation
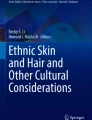
Clinically, AK presents as 2–4 mm papules and pustules along the occipital hairline, which may coalesce to form keloid plaques in a band-like distribution [11] or large keloid nodules [20] (Fig. 1). Subcutaneous abscesses with sinus drainage may form, and scarring alopecia may develop in the involved region. Unlike acne, AK is not comedonal in nature [11]. AK may be associated with pruritus or pain and can cause great cosmetic concern to patients [8].

Acne keloidalis. Cluster of 1–2 mm dome-shaped perifollicular papules on the occipital scalp of an African-American man
Histopathologically, AK lesions show perifollicular inflammation at the isthmus and lower infundibulum with a neutrophilic, lymphocytic, or plasmacytic infiltrate [13, 14]. Other reported features include the absence of sebaceous glands, thinning or destruction of the follicular epithelium, granulomatous inflammation, and scarring at the deep isthmus of the hair follicles [14]. Residual hair fragments may be trapped within the inferior portion of the follicle [13, 14].
2.3 Management
Strategies to prevent exacerbation or future development of AK should be discussed with patients. Avoidance of apparel such as hats or shirts with high collars is recommended [11]. Hairstyles cut close to the scalp and the use of razors/hair clippers along the occipital hairline should be discontinued [11, 21].
Mild to moderate cases of AK may respond to treatment with class I or II corticosteroids, sometimes in combination with topical antibiotics or retinoic acid [11]. In an open-label study by Callender et al. [22], clobetasol propionate 0.05 % and betamethasone valerate 0.12 % foams improved AK. A small-scale study found a regimen of imiquimod 5 % cream for 5 consecutive days per week for 8 weeks effective [11]. Other therapies include intralesional steroid injections and cryotherapy, which both carry the risk of hypopigmentation of the treated area for 12–18 months [11]. Long-pulse neodymium-doped yttrium aluminum garnet (Nd:YAG) lasers and long-pulse diode lasers have been shown effective in improving and successfully treating AK [23, 24].
Severe cases may require surgical excision. Options include excision with skin grafting, excision with primary closure, and excision with secondary intention healing [20]. Excision with skin grafting is associated with a less desirable cosmetic outcome due to atrophic shiny grafts that may not match the patient’s skin color [25]. Excision with primary closure has been reported as effective [25], but complications such as stretching of the scar and limited movement of the neck have been reported [26]. These complications may be avoided by performing the closure in multiple stages [25]. Excision with secondary-intention healing was found effective and more cosmetically desirable than primary closure [26] but may require more involved wound care [25].
3 Central Centrifugal Cicatricial Alopecia
CCCA is a chronic progressive scarring alopecia that originates at the vertex or crown of the scalp and spreads outward centrifugally. This condition primarily presents in middle-aged Black women, but has also been reported in young women and in men [27]. The condition was first described in 1968 by LoPresti et al. [28] with the name “hot comb alopecia,” as its cause was thought to be hot comb use. It was later renamed “follicular degeneration syndrome (FDS)” by Sperling et al. [29] to incorporate its histopathological features and “central centrifugal scarring alopecia” by Sperling et al. to include it in a group of closely related scarring alopecias [29]. Most recently, the name ‘central centrifugal cicatricial alopecia’ was adopted by the National Hair Research Society to distinguish it from other forms of scarring alopecia [30].
Though Halder et al. [31] described CCCA as the fifth most common dermatosis in African-Americans, its prevalence has not been well defined. A recent study performed by Olsen et al. [32] reported an incidence of 5.6 % in a group of 233 participants of similar composition to the general population, but a large-scale epidemiological study has not been performed.
3.1 Pathogenesis
The etiology of CCCA is not completely understood. An existing theory is that CCCA is caused by traumatic hairstyling practices, such as tight braids, weaves, or cornrows and the use of chemical relaxers, texturizers, or heat. Headington [33] postulated that CCCA (known as FDS at the time) was caused by the repeated injury of follicular stem cells from chemical and physical trauma. This aligned with a theory previously proposed by Nicholson et al. [34] in their publication, Cosmetically Induced Alopecia, that CCCA was caused by external insults. Ackerman hypothesized that FDS was a form of TA [4]. In a recent cross-sectional survey of 326 black women, Kyei et al. [35] found a significant association between severe CCCA and traction caused by hairstyles (e.g. braids and weaves), but not with heat or chemical relaxers. This finding supports previous theories implicating traction. This is in contrast to previous studies by Khumalo and Gumedze [36] and Olsen et al. [37] that found no association between traumatic styling and CCCA. Kyei et al. [35] also reported a positive correlation between CCCA, bacterial scalp infections, and type 2 diabetes mellitus, but potential mechanisms have not been suggested.
Genetics may play a role in the pathogenesis of CCCA. Dlova and Forder [38] reported a possible genetic etiology in two South African families. Members of both families presented with clinical and histological features of CCCA, with no history of chemical relaxers or traumatic hairstyling [38]. Dlova et al. [39] reported an autosomal dominant pattern of inheritance of CCCA in 14 Black South African families. Of the 31 participants with CCCA, six (19.4 %) did not have a history of chemical processing or traction hairstyling, suggesting a potential genetic etiology. Olsen et al. [32] found that 27 % of women with pattern 3–5 hair loss on the Central Hair Loss Photographic Scale had mothers with the same pattern, but whether the association is genetic or due to similar hair styling practices is unclear.
3.2 Presentation
Clinically, CCCA presents as scarring at the vertex or crown of the scalp and spreads centrifugally (Fig. 2). Patients may report scalp tenderness or pruritus, and short brittle hair strands may be seen at the affected region [40]. Callender et al. [41] proposed that early stages of CCCA may present as hair breakage at the vertex of the scalp, with or without scalp symptoms.

Central centrifugal cicatricial alopecia. Smooth patch of alopecia with complete loss of follicular orifices on the crown of an African-American woman
Histopathologically, CCCA shares features with other scarring alopecias such as perifollicular lymphocytic infiltrate, perifollicular fibroplasia and loss of sebaceous epithelium [42]. Desquamation of the inner root sheath and eccentric thinning of follicular epithelium are distinctive features of CCCA [43]. Miteva and Tosti [44] proposed that “goggles,” or “compound follicular structures formed by the fusion of their outer root sheaths and surrounded by concentric fibrosis with or without inflammation,” are diagnostic, especially when found at the level of the lower follicle. End-stage histopathological changes are noted to be indistinguishable from other forms of cicatricial alopecia [43].
The differential diagnosis of CCCA includes lichen planopilaris (LPP), frontal fibrosing alopecia (FFA), folliculitis decalvans (FD), discoid lupus erythematous (DLE), female pattern hair loss (FPHL), and TA. LPP can originate at the vertex of the scalp and spread centrifugally, but can occur on all areas of the scalp [4]. FFA is localized to the frontal temporal hairline and may involve eyebrow or body hair loss [45]. FD most commonly involves the vertex and occipital area of the scalp and presents as follicular pustules within or surrounding areas of alopecia [42]. Patients with FD may experience spontaneous bleeding, pruritus, or pain [46]. TA commonly occurs in the frontotemporal region and presents as alopecia surrounded by retained hairs [47], perifollicular hyperkeratosis, and folliculitis. Histopathologically, and in contrast to CCCA, sebaceous glands are retained [44]. In FPHL, there is a decrease in hair density that can occur centrally, but FPHL is a non-scarring alopecia characterized by a miniaturization of terminal hair follicles [48] and not follicular epithelial destruction. Lesions of DLE are characterized by follicular plugging, telangiectasias and scale [42].
3.3 Management
Though the etiology of CCCA has not been fully elucidated, it has been recommended that patients eliminate or reduce potentially traumatic haircare practices. Styles such as tight braids, twists, weaves, and cornrows should be avoided, as well as heavy hair grease and hardening gels or sprays. The application of excessive heat from pressing combs, flat irons, and hooded or blow dryers should be discontinued, especially on chemically processed hair [42]. The adoption of a ‘natural’ hairstyle (free of chemical relaxers, texturizers, or dyes) has been recommended, but if this is not possible, relaxers should be applied by a professional, and the frequency decreased to once every 8–12 weeks [40, 42]. Patients should ask their stylist to use a mild formulation, apply a protective base to the scalp, and neutralize after no more than 20 min [4, 40]. It has also been recommended that chemical treatments, such as dyes, should not be applied to relaxed hair [4].
Currently, there are no clinical trials showing the effectiveness of medical therapies for CCCA, but clinicians have advocated symptomatic treatment. Early intervention is key, as hair loss is often permanent once scarring has occurred.
Mid- to high-potency topical steroids can control local inflammation [4] but may not extend to deep areas of inflammation seen in CCCA [42]. Intralesional steroids such as triamcinolone acetonide can be injected monthly around the margins of active areas as well as surrounding areas of normal-appearing scalp to prevent the spread of inflammation. Dosing up to 10 mg/ml has been suggested [4], but potential side effects include hypopigmentation and atrophy. Oral antibiotics such as tetracyclines have been suggested for their anti-inflammatory and anti-bacterial properties [42]. A seborrheic dermatitis regimen may be used to reduce pruritus and scaling, and hair should be washed once weekly [40]. After inflammation has been controlled, topical minoxidil 2 or 5 % solution or 5 % foam may be used to stimulate hair growth in viable areas of scalp [42]. Once inflammation has been controlled for 12 months, hair replacement options may be considered [42].
4 Dissecting Cellulitis of the Scalp
DCS, also known as perifolliculitis capitis abscedens et suffodiens or Hoffman’s Disease, is a chronic inflammatory condition of the follicles of the scalp, characterized by fluctuant nodules and cysts, draining sinus tracts, and secondary scarring alopecia [49]. The lesions of DCS can be both painful and disfiguring [50]. It was first described by Spitzer [51] and most commonly affects Black males in their third to fifth decade of life [52]. However, DCS has been reported in other races [53–55] and in male and female pediatric patients [56, 57]. DCS has been linked to osteomyelitis of the skull [58], sternocostoclavicular hyperostosis [59], squamous cell carcinoma [60], and spondyloarthritis [61].
4.1 Pathogenesis
The pathogenesis of DCS is thought to involve follicular occlusion. The pilosebaceous unit can become occluded with keratin, followed by follicular expansion and inflammation [57]. Follicular dilatation occurs, followed by secondary bacterial infection, resulting in a folliculitis or perifolliculitis [62]. Dilated follicles can then rupture, releasing keratin and bacteria and precipitating a neutrophilic and granulomatous response [63]. Abscesses form and eventually become connected by sinus tracts [62]. The pathology of DCS is similar to that of hidradenitis suppurativa, acne conglobata, and pilonidal cysts, and all are considered part of the ‘follicular occlusion triad’ or tetrad [50]. A genetic connection has not been made, but familial cases of DCS have been reported [64].
4.2 Presentation
DCS initially presents as folliculitis at the vertex and occipital scalp [49]. It can then spread and form inflammatory pustules, fluctuant cysts and abscesses, suppurative nodules, and draining sinus tracts [65]. The chronic inflammation in DCS may cause hypertrophic scarring, keloids, and cicatricial alopecia [49] (Fig. 3). As DCS is considered a part of the follicular occlusion tetrad, hidradenitis suppurativa, acne conglobata, and pilonidal cysts may also be present [50].

Dissecting cellulitis. Residual scattered patches of alopecia on the scalp of an African-American man treated with isotretinoin
The differential diagnosis of DCS includes AK, tinea capitis, and FD. AK does not present with sinus tracts, suppurative nodules, or extensive scarring alopecia [63]. Though tinea capitis has been reported to mimic DCS in presentation [66], KOH preparation or a positive fungal culture can differentiate the two processes. Folliculotropic mycosis fungoides can also mimic DCS, and treatment-resistant cases of DCS should be evaluated for lymphoma [67]. Both FD and tufted folliculitis can cause a scarring alopecia, but do not present with sinus tracts or nodules [63, 68].
The histopathological appearance of DCS includes distension of the follicular infundibula with perifollicular, mixed, neutrophilic, and lymphoplasmacytic inflammation [69]. This inflammatory infiltrate is located at the dermis or subcutaneous level and leads to the destruction of follicular units [69, 70]. Abscesses, granulomas, and giant cells can accompany the follicular destruction [70]. Left untreated, abscesses can form sinus tracts. Following destruction of the follicle, fibrosis of both the dermis and superficial fat occurs [69]. On trichoscopy, a potential defining characteristic of DCS are three-dimensional yellow ‘dots’ imposed over dystrophic hairs [71].
4.3 Management
Available treatment methods for DCS are medical, destructive, and surgical. Medical therapy is considered first-line treatment [72] and includes intralesional steroids, oral tetracyclines, antibiotic soaps [63], isotretinoin as monotherapy or in combination with rifampin [73–75], oral zinc [76], prednisone [77], and ciprofloxacin [78]. The tumor necrosis factor (TNF) inhibitors adalimumab [79, 80] and infliximab [81] have also been reported as treatment, but DCS may return upon discontinuation [79].
Destructive therapies for DCS include laser and radiation beam epilation and provide another option for patients who have failed medical therapy. Boyd and Binhlam reported the successful use of an 800 nm pulsed diode laser in treating resistant DCS [82]. Chinnaiyan et al. [83] suggested that radiation beam therapy can be a safe and effective treatment method for recalcitrant DCS; no long-term toxicity was noted. Treatment with a 1,064 nm long-pulse Nd:YAG laser was associated with less pus formation, less dependence on systemic medications, and an attenuated or terminated disease process without dyspigmentation. Terminal hair regrowth was reported in some patients [84].
Surgical options exist for the treatment of DCS. Initially, incision and drainage can treat the lesions [85]. For very resistant DCS, the scalp and diseased tissue is completely removed and replaced with a split-thickness skin graft [62]. This method was first reported by Williams et al. [62] in 1986, and successful results have been reported in subsequent case reports [56, 86, 87].
5 Pseudofolliculitis Barbae
PFB is an inflammatory condition affecting men and women with tightly coiled hair. It presents as perifollicular papules and pustules, primarily affecting the neck and face [88]. It was first described by Fox [89] and called “pseudofolliculitis of the beard” by Kligman and Strauss [90] in 1956. Other names include pili incarnati, folliculitis barbae traumatica, sycosis barbae, ingrown hairs, or razor bumps [91]. The pathogenesis of PFB is complex but is associated with shaving and other forms of hair removal. Though PFB can occur in all races, it primarily affects men of African descent, with a reported prevalence of 45–83 % [92]. Latinos are the next most affected group [93]. PFB can also occur in women [94] and mostly affects the axillae and pubic area [95]. Women of African or Hispanic descent who have hirsutism or hypertrichosis have a similar incidence of PFB as men [95]. PFB can present a significant obstacle for people employed in industries/sectors with strict requirements for grooming, most notably the US military, where servicemen are expected to be cleanly shaven [95].
5.1 Pathogenesis
PFB is most commonly precipitated by shaving. When tightly coiled hair is shaved, sharp tapered edges can remain and can enter the skin through extrafollicular or transfollicular penetration [11]. In extrafollicular penetration, hair that has exited the follicle grows toward the scalp and penetrates the epidermis and dermis [95]. Transfollicular penetration is usually caused by shaving against the grain while the skin is pulled taut. When the skin is released, hair retracts back into the follicle and penetrates the epidermis and dermis [95]. Hair plucking can also precipitate transfollicular penetration [93]. Penetration causes an invagination of the epidermis and forms a ‘pseudofollicle’. The epidermis can rupture, inciting a foreign body response that manifests as inflamed perifollicular papules or pustules [91]. Post-inflammatory hyperpigmentation can follow [93]. The lesions of PFB are usually sterile but can become secondarily infected. When the hair grows to 10 mm in length, the embedded hair can release naturally through spring-like action [96].
In addition to shaving practices, genetics may also play a role in the pathogenesis of PFB. In a study of 200 men and women, Winter et al. [97] found that that 36 % of affected individuals had a disruptive Ala12Thr polymorphism of keratin K6hf compared with 9 % of unaffected individuals. It is believed that this mutation is partially responsible for the phenotypic expression of PFB, but the mechanism is not clear [97, 98].
5.2 Presentation
PFB presents as 2–4 mm inflammatory papules or pustules, located primarily in the beard distribution. The most common site of presentation in men is the neck and in women is the chin [95] (Fig. 4). These follicular-based lesions may be flesh-colored, erythematous or hyperpigmented, and accompanied by pruritus and pain [95]. Secondary bacterial infection, hypertrophic scarring, or keloid formation may also occur [88]. Trapped hairs can grow in a parallel fashion and appear as grooves or depressions in the skin [11]. Other areas subject to shaving, such as the axillae, legs, pubic area, and scalp, are susceptible to PFB [11].

Pseudofolliculitis barbae. Discrete perifollicular papules over the chin and extending to the neck in an African-American woman
The differential diagnosis for PFB includes acne vulgaris, bacterial folliculitis, traumatic folliculitis, tinea barbae, and sarcoidal papules [11, 95]. Acne vulgaris is comedonal in nature and can present in non-hair-bearing areas. Cultures of bacterial folliculitis will be positive, whereas PFB can be sterile, unless infected secondarily [95]. Traumatic folliculitis will regress a few days after shaving has been discontinued unlike PFB, which will remain for at least a week [11]. Tinea barbae presents as erythematous annular plaques with overlying scale that are unilateral and confluent and fungal cultures will be positive. Sarcoidal papules have a similar presentation to PFB [11].
Histopathologically, PFB is characterized by a foreign body inflammatory response to an invading trapped hair [72]. Epidermal penetration will show invagination with an inflammatory infiltrate, often with intraepidermal microabcesses [11]. Dermal penetration will incite a more intense inflammatory reaction and is accompanied by a downgrowth of the epidermis in an attempt to release the entrapped hair [90]. Giant cells and fibrosis may also be present [95].
5.3 Management
Patient education is important for the management of PFB. As shaving is implicated, it is recommended that patients discontinue the practice [11]. For patients who wish to continue shaving, there are suggested techniques that may decrease the activity of PFB. For each shave, patients should use a new sharp blade razor [91] or an electric razor that leaves hair 2–3 mm long [93]. It is recommended that they shave in the direction of hair growth without holding the skin taut and avoid shaving close to the skin [91]. Though it has been suggested that blade razors have single [93] or no more than two blades [91], Daniel et al. [99] found that an increased number of blades (three or five) was associated with a reduction in the number of ingrown hairs and improvement in severity of PFB. An alternative to shaving is the use of a depilatory cream. In a randomized trial, Kindred et al. [100] found that depilatory creams were associated with fewer papules and a smoother appearance than manual razors but were also associated with more irritation.
Topical therapies have been suggested but there are limited studies evaluating their use. One recommendation is the alternation of a topical steroid and a topical retinoid [93]. Topical antibiotics such as clindamycin have also been suggested [93] as well as glycolic acid [101]. A randomized controlled trial by Cook-Bolden et al. [102] demonstrated the efficacy of a regimen of benzoyl peroxide 5 %/clindamycin 1 % gel over a 10-week period. They reported a 32.8 % reduction in pustules and papules at week 2 and a 63.9 % decrease at week 10. These therapies may improve severity of PFB but do not offer a cure.
Laser therapy is considered the treatment modality closest to a cure [72]. Laser hair reduction has been associated with a significant decrease in papule/pustule formation in PFB [103, 104], with reported improvement for up to 3 months [104]. A previous concern with laser therapy on skin of color has been the potential for epidermal damage of the skin. The use of long-pulse diode and Nd:YAG lasers has allowed for improved safety of hair removal in darker skin types [105]. Weaver and Sagaral [104] found that treatment with a 1,064 nm long-pulse Nd:YAG laser significantly reduced the number of papules/pustules in patients with type V or VI skin. Smith et al. [106] found that the use of a modified 810 nm super long-pulse diode laser is effective in treating PFB in type V skin, with a reduced safety profile in type VI skin [107]. In a two-phase observational study, Ross et al. [103] found that the use of a long-pulse Nd:YAG laser was associated with decreased pustule/papule formation in skin types IV, V, and VI. The addition of eflornithine hydrochloride 13.9 % cream to laser therapy was found to expedite hair reduction and decrease the number of inflammatory pustules [108]. Though laser therapy may prove effective in some patients, it can be a painful procedure requiring local anesthetics. Potential side effects include dyspigmentation, blistering, crusting, and scarring [11].
6 Traction Alopecia
TA is hair loss caused by repetitive or prolonged tension on the hair due to tight hairstyling. While usually located on the frontal hairline and temporal region, TA can occur anywhere on the scalp [49]. While TA is most common in women of African descent [109], a high prevalence has also been reported in Hispanic women [47]. TA also occurs in men [110] and in the pediatric population [111]. It has also been reported in patients of other races and groups who wear their hair in tight ponytails or buns, such as ballerinas [112], Japanese and European women [113], and Sikh men and boys. In the Sikh religion, males are not permitted to cut their hair; they twist their hair tightly on their scalp and cover it with a turban. This constant tension has been implicated in cases of TA within this group [110, 114, 115]. The hair loss in TA can be reversed if the traction is released, but continued tension can lead to permanent hair loss [115].
6.1 Pathogenesis
The precipitating factor in TA is thought to be hairstyling that causes tension and stress on the scalp. Hair practices such as tight braiding [116], hair extensions that are sewed or glued onto the scalp, tight ponytails [115], and the use of hair rollers [117], hard gels, or hairsprays around the hairline have been implicated. The use of chemical relaxers concomitantly with tight hairstyles has also been associated with TA [118, 119]. The pathogenesis involves mechanical loosening of hair strands from the follicle, resulting in perifollicular inflammation [52]. Continued inflammation from tension can lead to permanent alopecia [115].
6.2 Presentation
Clinically, TA presents as hair loss or thinning around the frontal hairline or temple region, but can occur anywhere on the scalp [49]. An early sign of traction is perifollicular erythema, accompanied by follicular-based papules or pustules [72]. Clinical manifestations of early- and late-stage TA include the loss of follicular ostia and the presence of retained hair along the frontal or temporal rim, known as the ‘fringe sign’ [47]. Folliculitis and perifollicular hyperkeratosis may be present [49].
The differential diagnosis for TA includes ophiasis pattern alopecia areata (AA) and FFA [72]. In AA, follicular ostia are retained, there is no perifollicular hyperkeratosis, and eyebrow involvement can occur [47]. In FFA, follicular ostia are absent, there is no retention of hair along the frontal or temporal rim (fringe sign), and eyebrows can be affected [47]. For hair loss that occurs elsewhere on the scalp without a clear history of tight hairstyles, androgenic alopecia, telogen effluvium, CCCA, and trichotillomania should also be considered.
Histopathologically, the characteristic appearance of early TA is the preservation of sebaceous glands with decreased follicular number. Follicular scarring may or may not be present, and vellus follicles outnumber the terminal follicles [44]. In end-stage TA, follicular scarring is present and the number of sebaceous glands may be reduced. Residual terminal hair follicles are surrounded by fibrosis and a lymphoplasmacytic infiltrate can be seen at the level of the infundibulum [120].
6.3 Management
The first step in managing TA is the removal of hairstyles that are causing traction [121]. Without removal of the tension, TA may progress and render medical therapies less effective [115]. Patients should temporarily discontinue the use of heat or chemical treatments that can cause further damage to the scalp [121]. Sikh patients can be advised to tie their hair loosely at the scalp and to not wear their turban at night [114, 115].
Medical therapies may decrease inflammation and slow, if not prevent, the progression of TA. Oral and topical antibiotics can be used for their anti-inflammatory properties [122]. Topical or intralesional corticosteroids can also control inflammation at the periphery of the hair loss [122]. Khumalo and Ngwanya [123] reported the effective use of 2 % topical minoxidil in recovering hair loss caused by TA [124].
7 Keloids
Keloids are fibroproliferative scars that develop following dermal trauma. The scar extends past the border of the original wound and can be disfiguring. Without intervention, keloid scars will not regress, and recurrence is common even with treatment [125]. Keloids can occur in any race but are more prevalent in people of African, Asian, and Hispanic descent [6] and have a slight female predominance [126]. In Black and Latino populations, the incidence has been reported as 16 %, which increases during puberty and pregnancy [127]. Patients between the ages of 10 and 30 years are most at risk [128]. In addition to cosmetic issues, keloids can be associated with pruritus and pain and can cause emotional distress [125].
7.1 Pathogenesis
The pathogenesis of keloids has not been fully elucidated. It is thought that keloid formation occurs in part due to aberrant fibroblast activity. Fibroblasts derived from keloids were found to overexpress the pro-fibrotic cytokines transforming growth factor (TGF)-β1/2 and their receptors [129]. Expression of platelet-derived growth factor (PDGF), a factor that stimulates extracellular matrix (ECM) production and collagenase activity, is also increased in keloid fibroblasts. Increased levels of vascular endothelial growth factor (VEGF), connective tissue growth factor (CTGF), and procollagen I were also found [130]. In addition to the overexpression of growth factors, it has been shown that keloids have a slower rate of apoptosis [125]. The role of apoptosis in inhibiting cell proliferation and degradation of the ECM is important in wound healing. Mutations in the tumor suppressor gene p53 have been reported in keloids and may play a role in the altered apoptosis [131]. In addition to fibroblasts, melanocytes may contribute with their ability to stimulate fibroblast growth and proliferation, increase collagen synthesis and ECM deposition, and activate the TGF-β signaling pathway [132].
The prevalence of keloids in certain ethnic populations and in twins has suggested a possible genetic cause [128, 133]. Marneros et al. [133] performed a study of the clinical and genetic characteristics of 14 pedigrees with familial keloids and found an autosomal dominant pattern of inheritance with incomplete penetrance and variable expression. A genome-wide linkage search by the same authors found susceptibility loci on chromosome 2p23 in a Japanese family and on chromosome 7p11 in an African-American family [134]. Yan et al. [135] suggested two susceptibility loci on chromosome 15q22.31–q23 and chromosome 18q21.1.
7.2 Presentation
Clinically, keloids present as firm, raised scars. In patients with fair complexions, keloids can be erythematous and telangiectatic (Fig. 5). In patients with darker complexions, the lesions can be hyperpigmented [125] (Fig. 6). The most common locations for keloid formation are the sternum, earlobes, shoulders, posterior neck, and upper back [136]. The lesions can be pruritic and painful and are associated with areas of dermal trauma, though the traumatic or inflammatory event may be unknown [137]. Keloids usually appear within 1 year of trauma, but a delay of 24 years has been reported [138]. The differential diagnosis for keloids includes hypertrophic scars. While hypertrophic scars remain confined to the area of the original wound, keloids expand beyond the border of the wound [139]. Hypertrophic scars appear soon after the injury and regress over time, while keloid scars can have a delayed presentation and do not spontaneously resolve [140]. Histological features of keloids include hyalinized collagen, a tongue-like advancing edge under normal appearing epidermis and papillary dermis, horizontal cellular fibrous bands in the upper reticular dermis, and prominent fascia-like bands [141].

Keloid scar. Erythematous firm bow-tie-shaped firm plaque on the chest of an East Asian man

Keloid scar. Hyperpigmented firm plaque over the shoulder of an African-American man
7.3 Management
The first line of management is prevention. Wounds should be kept clean and free of debris [139, 140]. Predisposed individuals should avoid elective procedures that require penetration of the skin such as piercings or tattoos. If ear piercing is desired, it should be performed prior to age 11, as ear piercing after age 11 is associated with a greater incidence of keloids [142]. For surgical wounds, intralesional corticosteroids can be injected prophylactically [139], and mechanical stretching should be avoided [140]. Fixable materials such as silicone gel sheets, tape, and bandages have been recommended to keep the wound in place and prevent stretching [140]. A randomized controlled trial performed by Gold et al. [143] showed that silicone gel sheets prevented the formation of keloid and hypertrophic scarring. A systematic review by O’Brien and Jones [144] concluded that there is weak evidence supporting the efficacy of silicone gel sheets in keloid prevention due to poor quality of studies. Therefore, uncertainty remains regarding the effectiveness of this material in preventing keloids.
Intralesional corticosteroids (triamcinolone acetonide 10–40 mg/ml) are considered the first-line treatment [8, 145]. Keloid shrinkage has been reported as 50–100 % with a recurrence rate of 9–50 % [125, 146]. Side effects include pain, atrophy, telangiectasias, and hypopigmentation [139]. Other therapies include cryotherapy, surgical excision, radiotherapy, laser therapy, and intralesional adjuvant therapies [137].
Cryotherapy can be effective for keloids, especially smaller [147, 148] and more recent lesions [108, 149, 150]. Success rates have been reported as 50–75 % and require multiple sessions. Possible side effects include pain, atrophy of the skin, and hypopigmentation [137]. The cryoneedle has been reported to improve side effects, improve results, and decrease healing time as compared with open spray or cryoprobe mechanisms [151].
Surgical excision can be used as a monotherapy or with an adjuvant intralesional therapy or radiotherapy. Improved recurrence rates are seen with combination therapy and thus adjuvant intralesional corticosteroids and immunomodulators are recommended [6, 125]. When used in conjunction with excision, imiquimod decreases recurrence rates, but the effect is reversed upon removal of therapy [152]. Radiotherapy in combination with excision has been shown effective in the treatment of keloids [153, 154]. However, it is associated with various side effects, including malignancy [6, 137]. Recurrence has been associated with excessive tension used when closing surgical wounds. Surgeons can minimize tension by making incisions along relaxed skin tension lines and everting the wound during closure [155]. Suture materials known to cause inflammatory responses should be avoided [6].
Ablative and non-ablative laser therapy is another treatment option. The use of CO2 lasers as a monotherapy has been associated with recurrence rates as high as 95.7 % [156, 157]. CO2 lasers combined with intralesional steroids may be more effective [157, 158]. In a pilot study, erbium-doped YAG (Er:YAG) lasers reduced erythema, height, and hardness of keloids [156]. Alster and Williams [159] found that the 585-nm pulsed dye laser improved erythema, height, and pliability of keloid scars and reported a 57–83 % success rate. In a single-blinded randomized controlled trial, pulsed dye laser therapy was more effective when used in combination with intralesional steroids and intralesional 5-fluorouracil (5-FU) [160]. Pulsed dye lasers are best used on Fitzpatrick types I–III [137]. Nd:YAG lasers can flatten and improve the cosmetic appearance of keloid scarring and treat thicker keloids better than pulsed dye lasers, through deeper penetration of the skin [156]. Nd:YAG lasers are considered safe to use on Fitzpatrick types IV–VI [105].
Intralesional adjuvant treatments include interferon alpha-2b, botulinum toxin, 5-FU, and bleomycin. Interferon alpha-2b can reduce keloid size, but is associated with high recurrence and resistance to treatment [161]. Uyesugi et al. [162] found that botulinum toxin significantly reduced pain associated with keloids. 5-FU has been shown effective in flattening keloids, including resistant lesions and may have similar efficacy as intralesional steroids [163–166]. Side effects include pain, hyperpigmentation, and tissue sloughing [163]. Bleomycin has been shown to improve keloidal pruritus [167] and flatten keloids with an 86–100 % success rate [168–170].
8 Conclusion
Follicular and scarring disorders can significantly affect the lives of people of color. They can cause disfigurement, permanent hair loss, dysesthesias, and psychological distress and can affect overall quality of life. There is a great need for research on the pathogenesis and management of these conditions, as current treatments are limited and lack support of randomized controlled trials. In addition to providing treatment, the clinician can play an important role in the management of these conditions through patient education. Knowledge of differences in hair structure, hair grooming, and cultural practices as well as the presentation and management of these disorders is paramount to providing quality care to this population.
References
Lindelof B, Forslind B, Hedblad MA, Kaveus U. Human hair form. Morphology revealed by light and scanning electron microscopy and computer aided three-dimensional reconstruction. Arch Dermatol. 1988;124(9):1359–63.
Montagna W, Carlisle K. The architecture of black and white facial skin. J Am Acad Dermatol. 1991;24(6 Pt 1):929–37.
Vernall DG. A study of the size and shape of cross sections of hair from four races of men. Am J Phys Anthropol. 1961;19:345–50.
Ackerman AB, Walton NW, Jones RE, Charissi C. Hot comb alopecia/follicular degeneration syndrome in African-American women is traction alopecia. Dermatopathol Prac Concept. 2000:6–21
Taylor SC. Skin of color: biology, structure, function, and implications for dermatologic disease. J Am Acad Dermatol. 2002;46(2 Suppl Understanding):S41–62.
Chike-Obi CJ, Cole PD, Brissett AE. Keloids: pathogenesis, clinical features, and management. Semin Plast Surg. 2009;23(3):178–84. doi:10.1055/s-0029-1224797.
Kaposi M. Pathology and treatment of diseases of the skin for practitioners and students. New York: William Wood and Co; 1895.
Kundu RV, Patterson S. Dermatologic conditions in skin of color: part II. Disorders occurring predominately in skin of color. Am Fam Physician. 2013;87(12):859–65.
Dinehart SM, Tanner L, Mallory SB, Herzberg AJ. Acne keloidalis in women. Cutis. 1989;44(3):250–2.
Ogunbiyi A, George A. Acne keloidalis in females: case report and review of literature. J Natl Med Assoc. 2005;97(5):736–8.
Kelly AP. Pseudofolliculitis barbae and acne keloidalis nuchae. Dermatol Clin. 2003;21(4):645–53.
Salami T, Omeife H, Samuel S. Prevalence of acne keloidalis nuchae in Nigerians. Int J Dermatol. 2007;46(5):482–4. doi:10.1111/j.1365-4632.2007.03069.x.
Sperling LC, Homoky C, Pratt L, Sau P. Acne keloidalis is a form of primary scarring alopecia. Arch Dermatol. 2000;136(4):479–84.
Herzberg AJ, Dinehart SM, Kerns BJ, Pollack SV. Acne keloidalis. Transverse microscopy, immunohistochemistry, and electron microscopy. Am J Dermatopathol. 1990;12(2):109–21.
Goette DK, Berger TG. Acne keloidalis nuchae. A transepithelial elimination disorder. Int J Dermatol. 1987;26(7):442–4.
Khumalo NP, Gumedze F, Lehloenya R. Folliculitis keloidalis nuchae is associated with the risk for bleeding from haircuts. Int J Dermatol. 2011;50(10):1212–6. doi:10.1111/j.1365-4632.2010.04655.x.
Burkhart CG, Burkhart CN. Acne keloidalis is lichen simplex chronicus with fibrotic keloidal scarring. J Am Acad Dermatol. 1998;39(4 Pt 1):661.
Koehn GG. Skin injuries in sports medicine. J Am Acad Dermatol. 1991;24(1):152.
Knable AL Jr, Hanke CW, Gonin R. Prevalence of acne keloidalis nuchae in football players. J Am Acad Dermatol. 1997;37(4):570–4.
Beckett N, Lawson C, Cohen G. Electrosurgical excision of acne keloidalis nuchae with secondary intention healing. J Clin Aesthet Dermatol. 2011;4(1):36–9.
Quarles FN, Brody H, Badreshia S, Vause SE, Brauner G, Breadon JY, et al. Acne keloidalis nuchae. Dermatol Ther. 2007;20(3):128–32. doi:10.1111/j.1529-8019.2007.00123.x.
Callender VD, Young CM, Haverstock CL, Carroll CL, Feldman SR. An open label study of clobetasol propionate 0.05% and betamethasone valerate 0.12% foams in the treatment of mild to moderate acne keloidalis. Cutis. 2005;75(6):317–21.
Esmat SM, Abdel Hay RM, Abu Zeid OM, Hosni HN. The efficacy of laser-assisted hair removal in the treatment of acne keloidalis nuchae; a pilot study. Eur J Dermatol. 2012;22(5):645–50. doi:10.1684/ejd.2012.1830.
Dragoni F, Bassi A, Cannarozzo G, Bonan P, Moretti S, Campolmi P. Successful treatment of acne keloidalis nuchae resistant to conventional therapy with 1064-nm ND:YAG laser. G Ital Dermatol Venereol. 2013;148(2):231–2.
Gloster HM Jr. The surgical management of extensive cases of acne keloidalis nuchae. Arch Dermatol. 2000;136(11):1376–9.
Glenn MJ, Bennett RG, Kelly AP. Acne keloidalis nuchae: treatment with excision and second-intention healing. J Am Acad Dermatol. 1995;33(2 Pt 1):243–6.
Sperling LC, Skelton HG 3rd, Smith KJ, Sau P, Friedman K. Follicular degeneration syndrome in men. Arch Dermatol. 1994;130(6):763–9.
LoPresti P, Papa CM, Kligman AM. Hot comb alopecia. Arch Dermatol. 1968;98(3):234–8.
Sperling LC, Solomon AR, Whiting DA. A new look at scarring alopecia. Arch Dermatol. 2000;136(2):235–42.
Olsen EA, Bergfeld WF, Cotsarelis G, Price VH, Shapiro J, Sinclair R, et al. Summary of North American Hair Research Society (NAHRS)-sponsored Workshop on Cicatricial Alopecia, Duke University Medical Center, February 10 and 11, 2001. J Am Acad Dermatol. 2003;48(1):103–10. doi:10.1067/mjd.2003.68.
Halder RM, Grimes PE, McLaurin CI, Kress MA, Kenney JA, Jr. Incidence of common dermatoses in a predominantly black dermatologic practice. Cutis. 1983;32(4):388, 390.
Olsen EA, Callender V, McMichael A, Sperling L, Anstrom KJ, Shapiro J, et al. Central hair loss in African American women: incidence and potential risk factors. J Am Acad Dermatol. 2011;64(2):245–52. doi:10.1016/j.jaad.2009.11.693.
Headington JT. Cicatricial alopecia. Dermatol Clin. 1996;14(4):773–82.
Nicholson AG, Harland CC, Bull RH, Mortimer PS, Cook MG. Chemically induced cosmetic alopecia. Br J Dermatol. 1993;128(5):537–41.
Kyei A, Bergfeld WF, Piliang M, Summers P. Medical and environmental risk factors for the development of central centrifugal cicatricial alopecia: a population study. Arch Dermatol. 2011;147(8):909–14. doi:10.1001/archdermatol.2011.66.
Khumalo NP, Gumedze F. Traction: risk factor or coincidence in central centrifugal cicatricial alopecia? Br J Dermatol. 2012;167(5):1191–3
Olsen EA, Callender V, McMichael A, Sperling L, Anstrom KJ, Shapiro J, et al. Central hair loss in African American women: incidence and potential risk factors. J Am Acad Dermatol. 2011;64(2):245–52. doi:10.1016/j.jaad.2009.11.693.
Dlova NC, Forder M. Central centrifugal cicatricial alopecia: possible familial aetiology in two African families from South Africa. Int J Dermatol. 2012;51(Suppl 1):17–20, 23. doi:10.1111/j.1365-4632.2012.05557.x.
Dlova NC, Jordaan FH, Sarig O, Sprecher E. Autosomal dominant inheritance of central centrifugal cicatricial alopecia in black South Africans. J Am Acad Dermatol. 2014;. doi:10.1016/j.jaad.2013.11.035.
Callender VD, McMichael AJ, Cohen GF. Medical and surgical therapies for alopecias in black women. Dermatol Ther. 2004;17(2):164–76. doi:10.1111/j.1396-0296.2004.04017.x.
Callender VD, Wright DR, Davis EC, Sperling LC. Hair breakage as a presenting sign of early or occult central centrifugal cicatricial alopecia: clinicopathologic findings in 9 patients. Arch Dermatol. 2012;148(9):1047–52. doi:10.1001/archdermatol.2011.3428.
Whiting DA, Olsen EA. Central centrifugal cicatricial alopecia. Dermatol Ther. 2008;21(4):268–78. doi:10.1111/j.1529-8019.2008.00209.x.
Stefanato CM. Histopathology of alopecia: a clinicopathological approach to diagnosis. Histopathology. 2010;56(1):24–38. doi:10.1111/j.1365-2559.2009.03439.x.
Miteva M, Tosti A. ‘A detective look’ at hair biopsies from African-American patients. Br J Dermatol. 2012;166(6):1289–94. doi:10.1111/j.1365-2133.2012.10892.x.
Racz E, Gho C, Moorman PW, Noordhoek Hegt V, Neumann HA. Treatment of frontal fibrosing alopecia and lichen planopilaris: a systematic review. J Eur Acad Dermatol Venereol. 2013;27(12):1461–70. doi:10.1111/jdv.12139.
Otberg N, Kang H, Alzolibani AA, Shapiro J. Folliculitis decalvans. Dermatol Ther. 2008;21(4):238–44. doi:10.1111/j.1529-8019.2008.00204.x.
Samrao A, Price VH, Zedek D, Mirmirani P. The “Fringe Sign”—a useful clinical finding in traction alopecia of the marginal hair line. Dermatol Online J. 2011;17(11):1.
Olsen EA. Female pattern hair loss and its relationship to permanent/cicatricial alopecia: a new perspective. Journal of Investigative Dermatology Symposium Proceedings/the Society for Investigative Dermatology, Inc [and] European Society for Dermatological Research. 2005;10(3):217-21. doi:10.1111/j.1087-0024.2005.10109.x.
McMichael AJ. Hair and scalp disorders in ethnic populations. Dermatol Clin. 2003;21(4):629–44.
Chicarilli ZN. Follicular occlusion triad: hidradenitis suppurativa, acne conglobata, and dissecting cellulitis of the scalp. Ann Plast Surg. 1987;18(3):230–7.
Spitzer L. Dermatitis follicularis et parifollicularis conglobata. Dermatol Ztschr. 1903;10:109
Scott DA. Disorders of the hair and scalp in blacks. Dermatol Clin. 1988;6(3):387–95.
Stites PC, Boyd AS. Dissecting cellulitis in a white male: a case report and review of the literature. Cutis. 2001;67(1):37–40.
Lally A, Wojnarowska F. Hypertrophic pseudofolliculitis in white renal transplant recipients. Clin Exp Dermatol. 2007;32(3):268–71. doi:10.1111/j.1365-2230.2007.02386.x.
Greenblatt DT, Sheth N, Teixeira F. Dissecting cellulitis of the scalp responding to oral quinolones. Clin Exp Dermatol. 2008;33(1):99–100. doi:10.1111/j.1365-2230.2007.02598.x.
Ramesh V. Dissecting cellulitis of the scalp in 2 girls. Dermatologica. 1990;180(1):48–50.
Arneja JS, Vashi CN, Gursel E, Lelli JL. Management of fulminant dissecting cellulitis of the scalp in the pediatric population: case report and literature review. Can J Plast Surg. 2007;15(4):211–4.
Ramasastry SS, Granick MS, Boyd JB, Futrell JW. Severe perifolliculitis capitis with osteomyelitis. Ann Plast Surg. 1987;18(3):241–4.
Ongchi DR, Fleming MG, Harris CA. Sternocostoclavicular hyperostosis: two cases with differing dermatologic syndromes. J Rheumatol. 1990;17(10):1415–8.
Curry SS, Gaither DH, King LE Jr. Squamous cell carcinoma arising in dissecting perifolliculitis of the scalp. A case report and review of secondary squamous cell carcinomas. J Am Acad Dermatol. 1981;4(6):673–8.
Lim DT, James NM, Hassan S, Khan MA. Spondyloarthritis associated with acne conglobata, hidradenitis suppurativa and dissecting cellulitis of the scalp: a review with illustrative cases. Curr Rheumatol Rep. 2013;15(8). doi:10.1007/s11926-013-0346-y.
Williams CN, Cohen M, Ronan SG, Lewandowski CA. Dissecting cellulitis of the scalp. Plast Reconstr Surg. 1986;77(3):378–82.
Scheinfeld NS. A case of dissecting cellulitis and a review of the literature. Dermatol Online J. 2003;9(1):8.
Bjellerup M, Wallengren J. Familial perifolliculitis capitis abscedens et suffodiens in two brothers successfully treated with isotretinoin. J Am Acad Dermatol. 1990;23(4 Pt 1):752–3.
Jacobs F, Metzler G, Kubiak J, Röcken M, Schaller M. New approach in combined therapy of perifolliculitis capitis abscedens et suffodiens. Acta Derm Venereol. 2011;91(6):726–7. doi:10.2340/00015555-1146.
Stein LL, Adams EG, Holcomb KZ. Inflammatory tinea capitis mimicking dissecting cellulitis in a postpubertal male: a case report and review of the literature. Mycoses. 2013;56(5):596–600. doi:10.1111/myc.12082.
Gerami P, Rosen S, Kuzel T, Boone SL, Guitart J. Folliculotropic mycosis fungoides: an aggressive variant of cutaneous T-cell lymphoma. Arch Dermatol. 2008;144(6):738–46. doi:10.1001/archderm.144.6.738.
Annessi G. Tufted folliculitis of the scalp: a distinctive clinicohistological variant of folliculitis decalvans. Br J Dermatol. 1998;138(5):799–805.
Sperling LC. Scarring alopecia and the dermatopathologist. J Cutan Pathol. 2001;28(7):333–42.
Branisteanu DE, Molodoi A, Ciobanu D, Badescu A, Stoica LE, Branisteanu D, et al. The importance of histopathologic aspects in the diagnosis of dissecting cellulitis of the scalp. Rom J Morphol Embryol. 2009;50(4):719-24.
Rakowska A, Slowinska M, Kowalska-Oledzka E, Warszawik O, Czuwara J, Olszewska M, et al. Trichoscopy of cicatricial alopecia. J Drugs Dermatol. 2012;11(6):753–8.
Rodney IJ, Onwudiwe OC, Callender VD, Halder RM. Hair and scalp disorders in ethnic populations. J Drugs Dermatol. 2013;12(4):420–7.
Khaled A, Zeglaoui F, Zoghlami A, Fazaa B, Kamoun MR. Dissecting cellulitis of the scalp: response to isotretinoin. J Eur Acad Dermatol Venereol. 2007;21(10):1430–1. doi:10.1111/j.1468-3083.2007.02239.x.
Karpouzis A, Giatromanolaki A, Sivridis E, Kouskoukis C. Perifolliculitis capitis abscedens et suffodiens successfully controlled with topical isotretinoin. Eur J Dermatol. 2003;13(2):192–5.
Georgala S, Korfitis C, Ioannidou D, Alestas T, Kylafis G, Georgala C. Dissecting cellulitis of the scalp treated with rifampicin and isotretinoin: case reports. Cutis. 2008;82(3):195–8.
Kobayashi H, Aiba S, Tagami H. Successful treatment of dissecting cellulitis and acne conglobata with oral zinc. Br J Dermatol. 1999;141(6):1137–8.
Adrian RM, Arndt KA. Perifolliculitis capitis: successful control with alternate-day corticosteroids. Ann Plast Surg. 1980;4(2):166–9.
Onderdijk AJ, Boer J. Successful treatment of dissecting cellulitis with ciprofloxacin. Clin Exp Dermatol. 2010;35(4):440. doi:10.1111/j.1365-2230.2009.03514.x.
Navarini AA, Trüeb RM. 3 cases of dissecting cellulitis of the scalp treated with adalimumab: control of inflammation within residual structural disease. Arch Dermatol. 2010;146(5):517–20. doi:10.1001/archdermatol.2010.16.
Sukhatme SV, Lenzy YM, Gottlieb AB. Refractory dissecting cellulitis of the scalp treated with adalimumab. J Drugs Dermatol. 2008;7(10):981–3.
Brandt HRC, Malheiros APR, Teixeira MG, Machado MCR. Perifolliculitis capitis abscedens et suffodiens successfully controlled with infliximab. Br J Dermatol. 2008;159(2):506–7. doi:10.1111/j.1365-2133.2008.08674.x.
Boyd AS, Binhlam JQ. Use of an 800-nm pulsed-diode laser in the treatment of recalcitrant dissecting cellulitis of the scalp. Arch Dermatol. 2002;138(10):1291–3.
Chinnaiyan P, Tena LB, Brenner MJ, Welsh JS. Modern external beam radiation therapy for refractory dissecting cellulitis of the scalp. Br J Dermatol. 2005;152(4):777–9. doi:10.1111/j.1365-2133.2005.06536.x.
Krasner BD, Hamzavi FH, Murakawa GJ, Hamzavi IH. Dissecting cellulitis treated with the long-pulsed Nd:YAG laser. Dermatol Surg. 2006;32(8):1039–44. doi:10.1111/j.1524-4725.2006.32227.x.
Scheinfeld NSMD. A case of dissecting cellulitis and a review of the literature. Dermatol Online J. 2003;9(1):8.
Housewright CD, Rensvold E, Tidwell J, Lynch D, Butler DF. Excisional surgery (scalpectomy) for dissecting cellulitis of the scalp. Dermatol Surg. 2011;37(8):1189–91. doi:10.1111/j.1524-4725.2011.02049.x.
Bellew SG, Nemerofsky R, Schwartz RA, Granick MS. Successful treatment of recalcitrant dissecting cellulitis of the scalp with complete scalp excision and split-thickness skin graft. Dermatol Surg. 2003;29(10):1068–70.
Kundu RV, Patterson S. Dermatologic conditions in skin of color: part II. Disorders occurring predominately in skin of color. Am Fam Physician. 2013;87(12):859–65.
Fox H. Observations on skin diseases in the Negro. J Cutan Dis. 1908;26:67–79
Kligman AM, Strauss JS. Pseudofolliculitis of the beard. AMA Arch Dermatol. 1956;74(5):533–42.
Ribera M, Fernandez-Chico N, Casals M. Pseudofolliculitis barbae. Actas Dermo Sifiliograficas. 2010;101(9):749–57.
Alexander AM, Delph WI. Pseudofolliculitis barbae in the military. A medical, administrative and social problem. J Natl Med Assoc. 1974;66(6):459–64, 79.
Bridgeman S. The medical and surgical therapy of pseudofolliculitis barbae. Dermatol Ther. 2004;17(2):158–63. doi:10.1111/j.1396-0296.2004.04016.x.
Garcia RL, White JW Jr. Pseudofolliculitis barbae in a woman. Arch Dermatol. 1978;114(12):1856.
Perry PK, Cook-Bolden FE, Rahman Z, Jones E, Taylor SC. Defining pseudofolliculitis barbae in 2001: a review of the literature and current trends. J Am Acad Dermatol. 2002;46(2 Suppl Understanding):S113–9.
Dunn JF Jr. Pseudofolliculitis barbae. Am Fam Physician. 1988;38(3):169–74.
Winter H, Schissel D, Parry DAD, Smith TA, Liovic M, Birgitte Lane E et al. An unusual Ala12Thr polymorphism in the 1A alpha-helical segment of the companion layer-specific keratin K6hf: evidence for a risk factor in the etiology of the common hair disorder pseudofolliculitis barbae. J Invest Dermatol. 2004;122(3):652–7. doi:10.1111/j.0022-202X.2004.22309.x.
McLean WHI. Close shave for a keratin disorder-K6hf polymorphism linked to pseudofolliculitis barbae. J Invest Dermatol. 2004;122(3):xi–xiii. doi:10.1111/j.0022-202X.2004.22351.x.
Daniel A, Gustafson CJ, Zupkosky PJ, Candido A, Kemp HR, Russell G, et al. Shave frequency and regimen variation effects on the management of pseudofolliculitis barbae. J Drugs Dermatol. 2013;12(4):410–8.
Kindred C, Oresajo CO, Yatskayer M, Halder RM. Comparative evaluation of men’s depilatory composition versus razor in black men. Cutis. 2011;88(2):98–103.
Perricone NV. Treatment of pseudofolliculitis barbae with topical glycolic acid: a report of two studies. Cutis. 1993;52(4):232–5.
Cook-Bolden FE, Barba A, Halder R, Taylor S. Twice-daily applications of benzoyl peroxide 5%/clindamycin 1% gel versus vehicle in the treatment of pseudofolliculitis barbae. Cutis. 2004;73(6 Suppl):18–24.
Ross EV, Cooke LM, Timko AL, Overstreet KA, Graham BS, Barnette DJ. Treatment of pseudofolliculitis barbae in skin types IV, V, and VI with a long-pulsed neodymium:yttrium aluminum garnet laser. J Am Acad Dermatol. 2002;47(2):263–70.
Weaver SM 3rd, Sagaral EC. Treatment of pseudofolliculitis barbae using the long-pulse Nd:YAG laser on skin types V and VI. Dermatol Surg. 2003;29(12):1187–91.
Battle EF Jr, Hobbs LM. Laser-assisted hair removal for darker skin types. Dermatol Ther. 2004;17(2):177–83. doi:10.1111/j.1396-0296.2004.04018.x.
Smith EP, Winstanley D, Ross EV. Modified superlong pulse 810 nm diode laser in the treatment of pseudofolliculitis barbae in skin types V and VI. Dermatol Surg. 2005;31(3):297–301
Emer JJ. Best practices and evidenced-based use of the 800 nm diode laser for the treatment of pseudofolliculitis barbae in skin of color. J Drugs Dermatol. 2011;10(12 Suppl):s20–2.
Xia Y, Cho S, Howard RS, Maggio KL. Topical eflornithine hydrochloride improves the effectiveness of standard laser hair removal for treating pseudofolliculitis barbae: a randomized, double-blinded, placebo-controlled trial. J Am Acad Dermatol. 2012;67(4):694–9. doi:10.1016/j.jaad.2011.10.029.
Rodney IJ, Onwudiwe OC, Callender VD, Halder RM. Hair and scalp disorders in ethnic populations. J Drugs Dermatol. 2013;12(4):420–7.
Kanwar AJ, Kaur S, Basak P, Sharma R. Traction alopecia in Sikh males. Arch Dermatol. 1989;125(11):1587.
Hantash BM, Schwartz RA. Traction alopecia in children. Cutis. 2003;71(1):18–20.
Samrao A, Chen C, Zedek D, Price VH. Traction alopecia in a ballerina: clinicopathologic features. Arch Dermatol. 2010;146(8):930–1. doi:10.1001/archdermatol.2010.183.
Trüeb RM. “Chignon alopecia”: a distinctive type of nonmarginal traction alopecia. Cutis. 1995;55(3):178–9.
Karimian-Teherani D, El Shabrawi-Caelen L, Tanew A. Traction alopecia in two adolescent Sikh brothers-an underrecognized problem unmasked by migration. Pediatr Dermatol. 2011;28(3):336–8. doi:10.1111/j.1525-1470.2011.01241.x.
James J, Saladi RN, Fox JL. Traction alopecia in Sikh male patients. J Am Board Fam Med. 2007;20(5):497–8. doi:10.3122/jabfm.2007.05.070076.
Rudolph RI, Klein AW, Decherd JW. Corn-row alopecia. Arch Dermatol. 1973;108(1):134.
Lipnik MJ. Traumatic alopecia from brush rollers. Arch Dermatol. 1961;84:493–5.
Rucker Wright D, Gathers R, Kapke A, Johnson D, Joseph CLM. Hair care practices and their association with scalp and hair disorders in African American girls. J Am Acad Dermatol. 2011;64(2):253–62. doi:10.1016/j.jaad.2010.05.037.
Khumalo NP, Jessop S, Gumedze F, Ehrlich R. Determinants of marginal traction alopecia in African girls and women. J Am Acad Dermatol. 2008;59(3):432–8. doi:10.1016/j.jaad.2008.05.036.
Donovan JC, Mirmirani P. Transversely sectioned biopsies in the diagnosis of end-stage traction alopecia. Dermatol Online J. 2013;19(4):11.
Fox GN, Stausmire JM, Mehregan DR. Traction folliculitis: an underreported entity. Cutis. 2007;79(1):26–30.
Callender VD, McMichael AJ, Cohen GF. Medical and surgical therapies for alopecias in black women. Dermatol Ther. 2004;17(2):164–76. doi:10.1111/j.1396-0296.2004.04017.x.
Khumalo NP, Ngwanya RM. Traction alopecia: 2 % topical minoxidil shows promise. Report of two cases. J Eur Acad Dermatol Venereol. 2007;21(3):433–4
Ozçelik D. Extensive traction alopecia attributable to ponytail hairstyle and its treatment with hair transplantation. Aesthetic Plast Surg. 2005;29(4):325–7. doi:10.1007/s00266-005-0004-5.
Naylor MC, Brissett AE. Current concepts in the etiology and treatment of keloids. Facial Plast Surg. 2012;28(5):504–12. doi:10.1055/s-0032-1325644.
Kelly AP. Medical and surgical therapies for keloids. Dermatol Ther. 2004;17(2):212–8. doi:10.1111/j.1396-0296.2004.04022.x.
Alhady SM, Sivanantharajah K. Keloids in various races. A review of 175 cases. Plast Reconstr Surg. 1969;44(6):564–6.
Ramakrishnan KM, Thomas KP, Sundararajan CR. Study of 1,000 patients with keloids in South India. Plast Reconstr Surg. 1974;53(3):276–80.
Lee TY, Chin GS, Kim WJ, Chau D, Gittes GK, Longaker MT. Expression of transforming growth factor beta 1, 2, and 3 proteins in keloids. Ann Plast Surg. 1999;43(2):179–84.
Marneros AG, Krieg T. Keloids—clinical diagnosis, pathogenesis, and treatment options. J Dtsch Dermatol Ges. 2004;2(11):905–13.
Saed GM, Ladin D, Olson J, Han X, Hou Z, Fivenson D. Analysis of p53 gene mutations in keloids using polymerase chain reaction-based single-strand conformational polymorphism and DNA sequencing. Arch Dermatol. 1998;134(8):963–7.
Gao FL, Jin R, Zhang L, Zhang YG. The contribution of melanocytes to pathological scar formation during wound healing. Int J Clin Exp Med. 2013;6(7):609–13.
Marneros AG, Norris JE, Olsen BR, Reichenberger E. Clinical genetics of familial keloids. Arch Dermatol. 2001;137(11):1429–34.
Marneros AG, Norris JE, Watanabe S, Reichenberger E, Olsen BR. Genome scans provide evidence for keloid susceptibility loci on chromosomes 2q23 and 7p11. J Invest Dermatol. 2004;122(5):1126–32. doi:10.1111/j.0022-202X.2004.22327.x.
Yan X, Gao JH, Chen Y, Song M, Liu XJ. [Preliminary linkage analysis and mapping of keloid susceptibility locus in a Chinese pedigree]. Zhonghua zheng xing wai ke za zhi = Zhonghua zhengxing waike zazhi =. Chin J Plast Surg. 2007;23(1):32–5.
Bayat A, Arscott G, Ollier WE, Ferguson MW, Mc Grouther DA. Description of site-specific morphology of keloid phenotypes in an Afrocaribbean population. Br J Plast Surg. 2004;57(2):122–33. doi:10.1016/j.bjps.2003.11.009.
Love PB, Kundu RV. Keloids: an update on medical and surgical treatments. J Drugs Dermatol. 2013;12(4):403–9.
Nemeth AJ. Keloids and hypertrophic scars. J Dermatol Surg Oncol. 1993;19(8):738–46.
Juckett G, Hartman-Adams H. Management of keloids and hypertrophic scars. Am Fam Physician. 2009;80(3):253–60.
Ogawa R. The most current algorithms for the treatment and prevention of hypertrophic scars and keloids. Plast Reconstr Surg. 2010;125(2):557–68. doi:10.1097/PRS.0b013e3181c82dd5.
Lee JY, Yang CC, Chao SC, Wong TW. Histopathological differential diagnosis of keloid and hypertrophic scar. Am J Dermatopathol. 2004;26(5):379–84.
Lane JE, Waller JL, Davis LS. Relationship between age of ear piercing and keloid formation. Pediatrics. 2005;115(5):1312–4. doi:10.1542/peds.2004-1085.
Gold MH, Foster TD, Adair MA, Burlison K, Lewis T. Prevention of hypertrophic scars and keloids by the prophylactic use of topical silicone gel sheets following a surgical procedure in an office setting. Dermatol Surg. 2001;27(7):641–4.
O’Brien L, Jones DJ. Silicone gel sheeting for preventing and treating hypertrophic and keloid scars. Cochrane Database Syst Rev. 2013;9:CD003826. doi:10.1002/14651858.CD003826.pub3.
Mustoe TA, Cooter RD, Gold MH, Hobbs FD, Ramelet AA, Shakespeare PG, et al. International clinical recommendations on scar management. Plast Reconstr Surg. 2002;110(2):560–71.
Niessen FB, Spauwen PH, Schalkwijk J, Kon M. On the nature of hypertrophic scars and keloids: a review. Plast Reconstr Surg. 1999;104(5):1435–58.
Shepherd JP, Dawber RP. The response of keloid scars to cryosurgery. Plast Reconstr Surg. 1982;70(6):677–82.
Careta MF, Fortes AC, Messina MC, Maruta CW. Combined treatment of earlobe keloids with shaving, cryosurgery, and intralesional steroid injection: a 1-year follow-up. Dermatol Surg. 2013;39(5):734–8. doi:10.1111/dsu.12107.
Barara M, Mendiratta V, Chander R. Cryotherapy in treatment of keloids: evaluation of factors affecting treatment outcome. J Cutan Aesthet Surg. 2012;5(3):185–9. doi:10.4103/0974-2077.101376.
Layton AM, Yip J, Cunliffe WJ. A comparison of intralesional triamcinolone and cryosurgery in the treatment of acne keloids. Br J Dermatol. 1994;130(4):498–501.
Weshahy AH. Intralesional cryosurgery. A new technique using cryoneedles. J Dermatol Surg Oncol. 1993;19(2):123–6.
Malhotra AK, Gupta S, Khaitan BK, Sharma VK. Imiquimod 5% cream for the prevention of recurrence after excision of presternal keloids. Dermatology. 2007;215(1):63–5. doi:10.1159/000102036.
Klumpar DI, Murray JC, Anscher M. Keloids treated with excision followed by radiation therapy. J Am Acad Dermatol. 1994;31(2 Pt 1):225–31.
Guix B, Henriquez I, Andres A, Finestres F, Tello JI, Martinez A. Treatment of keloids by high-dose-rate brachytherapy: a seven-year study. Int J Radiat Oncol Biol Phys. 2001;50(1):167–72.
Chen MA, Davidson TM. Scar management: prevention and treatment strategies. Curr Opin Otolaryngol Head Neck Surg. 2005;13(4):242–7.
Mamalis AD, Lev-Tov H, Nguyen DH, Jagdeo JR. Laser and light-based treatment of Keloids—a review. J Eur Acad Dermatol Venereol. 2013;. doi:10.1111/jdv.12253.
Norris JE. The effect of carbon dioxide laser surgery on the recurrence of keloids. Plast Reconstr Surg. 1991;87(1):44–9; discussion 50–3.
Garg GA, Sao PP, Khopkar US. Effect of carbon dioxide laser ablation followed by intralesional steroids on keloids. J Cutan Aesthet Surg. 2011;4(1):2–6. doi:10.4103/0974-2077.79176.
Alster TS, Williams CM. Treatment of keloid sternotomy scars with 585 nm flashlamp-pumped pulsed-dye laser. Lancet. 1995;345(8959):1198–200.
Asilian A, Darougheh A, Shariati F. New combination of triamcinolone, 5-Fluorouracil, and pulsed-dye laser for treatment of keloid and hypertrophic scars. Dermatol Surg. 2006;32(7):907–15. doi:10.1111/j.1524-4725.2006.32195.x.
Shridharani SM, Magarakis M, Manson PN, Singh NK, Basdag B, Rosson GD. The emerging role of antineoplastic agents in the treatment of keloids and hypertrophic scars: a review. Ann Plast Surg. 2010;64(3):355–61. doi:10.1097/SAP.0b013e3181afaab0.
Uyesugi B, Lippincott B, Dave S. Treatment of a painful keloid with botulinum toxin type A. American journal of physical medicine & rehabilitation/Association of Academic Physiatrists. 2010;89(2):153–5.
Kontochristopoulos G, Stefanaki C, Panagiotopoulos A, Stefanaki K, Argyrakos T, Petridis A, et al. Intralesional 5-fluorouracil in the treatment of keloids: an open clinical and histopathologic study. J Am Acad Dermatol. 2005;52(3 Pt 1):474–9. doi:10.1016/j.jaad.2004.09.018.
Nanda S, Reddy BS. Intralesional 5-fluorouracil as a treatment modality of keloids. Dermatol Surg. 2004;30(1):54–6; discussion 6–7.
Gupta S, Kalra A. Efficacy and safety of intralesional 5-fluorouracil in the treatment of keloids. Dermatology. 2002;204(2):130–2 51830.
Manuskiatti W, Fitzpatrick RE. Treatment response of keloidal and hypertrophic sternotomy scars: comparison among intralesional corticosteroid, 5-fluorouracil, and 585-nm flashlamp-pumped pulsed-dye laser treatments. Arch Dermatol. 2002;138(9):1149–55.
Aggarwal H, Saxena A, Lubana PS, Mathur RK, Jain DK. Treatment of keloids and hypertrophic scars using bleom. J Cosmet Dermatol. 2008;7(1):43–9. doi:10.1111/j.1473-2165.2008.00360.x.
Espana A, Solano T, Quintanilla E. Bleomycin in the treatment of keloids and hypertrophic scars by multiple needle punctures. Dermatol Surg. 2001;27(1):23–7.
Bodokh I, Brun P. Treatment of keloid with intralesional bleomycin. Ann Dermatol Venereol. 1996;123(12):791–4.
Naeini FF, Najafian J, Ahmadpour K. Bleomycin tattooing as a promising therapeutic modality in large keloids and hypertrophic scars. Dermatol Surg. 2006;32(8):1023–9; discussion 9–30. doi:10.1111/j.1524-4725.2006.32225.x.
Acknowledgments
No sources of funding were used to prepare this review. Pamela Madu and Roopal Kundu have no conflicts of interest that are directly relevant to the content of this review.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Madu, P., Kundu, R.V. Follicular and Scarring Disorders in Skin of Color: Presentation and Management. Am J Clin Dermatol 15, 307–321 (2014). https://doi.org/10.1007/s40257-014-0072-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40257-014-0072-x