
Summary
Background
In today’s society, sleep disturbances and back pain are both common problems which threaten health. Although some studies have focused on the effects of sleep disturbances on back pain, no meta-analysis has been done. The purpose of this study is to systematically review and perform a meta-analysis on the effects of sleep disturbances on back pain.
Methods
A literature search in PubMed, Scopus and EMBASE with keywords until June 2019 was performed. The eligible articles were evaluated qualitatively and the results were pooled using random effects. The publication bias and the degree of heterogeneity were examined.
Results
In all, 21 studies were included in the meta-analysis. Sleep disturbances were associated with back pain (odds ratio 1.52; confidence interval [CI] 1.37–1.68; P < 0.001). In men, the odds ratio was 1.49 (CI 1.34–1.65; P < 0.001). In women, the odds ratio was 1.56 (CI 1.33–1.81; P < 0.001). Begg’s test (P = 0.856) and Egger test (P = 0.188) did not show any publication bias. A funnel plot and trim-and-fill method showed publication bias, and heterogeneity was also high.
Conclusions
Sleep disturbance is associated with risk of back pain. Improving sleep can be a deterrent against back pain. Therefore, interventions to reduce sleep disturbances can help to improve health. On the other hand, the relationship between sleep disturbances and back pain can be two-sided, and back pain can also lead to sleep disturbances. Not only in view of the lifetime prevalence and the multifactorial impairments of those affected, but also in consideration of social and economic burdens, this issue will remain of considerable importance.
Zusammenfassung
Hintergrund
In der heutigen Gesellschaft sind sowohl Schlafstörungen als auch Rückenschmerzen häufige gesundheitsgefährdende Probleme. Zwar haben einige Studien auf die Auswirkungen von Schlafstörungen auf Rückenschmerzen fokussiert, doch bislang gibt noch keine Metaanalyse zu dieser Thematik. Ziel der vorliegenden Studie ist es, die Auswirkungen von Schlafstörungen auf Rückenschmerzen systematisch zu überprüfen und eine Metaanalyse durchzuführen.
Methodik
In PubMed, Scopus und EMBASE wurde mit Stichworten bis Juni 2019 nach Literatur gesucht. Die infrage kommenden Artikel wurden qualitativ bewertet und die Ergebnisse unter Verwendung von Zufallseffekten gepoolt. Untersucht wurden ein möglicher Publikationsbias und der Grad der Heterogenität.
Ergebnisse
Insgesamt wurden 21 Studien in die Metaanalyse einbezogen. Schlafstörungen waren mit Rückenschmerzen assoziiert (Odds Ratio [OR] 1,52; Konfidenzintervall [KI] 1,37‑1,68; p < 0,001). Bei den Männern betrug die OR 1,49 (KI 1,34‑1,65; p < 0,001). Bei Frauen betrug die OR 1,56 (KI 1,33‑1,81; p < 0,001). Der Begg-Test (p = 0,856) und der Egger-Test (p = 0,188) zeigten keinen Publikationsbias, wohl dagegen ein Funnel-Plot und die „trim-and-fill method“. Die Heterogenität war ebenfalls hoch.
Schlussfolgerungen
Schlafstörungen sind mit dem Risiko von Rückenschmerzen verbunden. Verbesserter Schlaf kann Rückenschmerzen abhalten. Daher können Interventionen zur Verringerung von Schlafstörungen einen Beitrag zur Verbesserung der Gesundheit leisten. Andererseits kann der Zusammenhang zwischen Schlafstörungen und Rückenschmerzen umgekehrt sein sein: Rückenschmerzen können auch zu Schlafstörungen führen. Nicht nur angesichts der Lebenszeitprävalenz und der multifaktoriellen Beeinträchtigungen der Betroffenen, sondern auch im Hinblick auf die sozialen und ökonomischen Belastungen wird diese Thematik von erheblicher Bedeutung bleiben.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Low back pain is considered as a type of pain that is characterized by pain between costal margins and the inferior gluteal folds, which is usually followed by restriction of movement. The pain is drawn to the legs; a pain that is not associated with any fracture, injury or illness [1,2,3]. Low back pain is a common problem in health care and it imposes a significant social and economic burden on society [4,5,6,7].
In a study published in 2002, the point prevalence of low back pain in the adult population was 12–33% and 1‑year prevalence was between 22–65% [8]. A study on the prevalence of back pain and spinal pain in an adolescent population also indicated that lifetime prevalence was between 4.7–74.4%, and lifetime prevalence of low back pain was 7–72% [9]. A systematic review study of children and adolescents showed that the mean point prevalence of low back pain was 15.25%, with a lifetime prevalence of 38.98% [10]. A recent study of the global prevalence of low back pain, which included published studies between 1980 and 2009, indicated a high prevalence of low back pain [1]. This study showed that lifetime prevalence of low back pain ranges between 60 and 80% and this prevalence was higher in women than in men and also in the age range of 40–80 years [1].
Many review and meta-analysis studies have examined the risk factors for back pain, which include individual factors, physical and psychological work-related factors, physical risk factors, psychological factors and lifestyle factors [11,12,13,14,15,16,17,18,19,20,21,22]. It has been shown that sleep quality can predict pain [23]. Sleep disturbances are prevalent with between 6 and 15% of the general population being diagnosed with insomnia; excessive sleepiness prevalence is 4–26%, narcolepsy which is a rare disorder has an average prevalence of 0.04%, and the prevalence of obstructive sleep apnea syndrome is 2–4% [24]. Sleep disturbances are associated with a variety of health problems; long sleep duration is a risk factor for mortality, diabetes, cardiovascular disease, stroke, coronary heart disease and obesity [25], risk of dementia [26] and sleep changes and pain-related outcomes [27].
Sleep disturbances are commonly found among people who experience chronic pain [28, 29]. Poor sleep plays an important role in predicting the growth and intensification of pain over time [30]. Almost 50% of people with chronic low back pain have sleeping disturbances and are more likely to experience other psychological disturbances [31,32,33]. One of comorbid problems with back pain is insomnia [34]. Though studies have already been conducted to examine the relationship between sleep disturbances and pain types such as chronic pain [23] and musculoskeletal pain [35], reviewing the studies on the effects of sleep on pain, points out a few facts. Studies on the effect of sleep disturbances on pain have not specifically addressed back pain. The studies have examined the prevalence of sleep disturbances in people with chronic and multiskeletal pain, but they have not determined how much sleep disturbances can lead to back pain. Although sleep disturbances have been reported as risk factors for back pain, a meta-analysis has become necessary.
The study of the effects of sleep disturbances on low back pain, requires a review study to clarify the findings of this field; it also requires a meta-analysis to produce statistical results. The purpose of this study is to investigate sleep disturbances and back pain. On the other hand, the role of gender differences, type of sleep disturbances, and study design in relation between sleep disturbances and back pain are specifically evaluated.
Methods
Search strategy
The PRISMA [36] protocol, which is used in systematic review and meta-analysis studies, was used as a guide in this study. After developing the subject, the researchers performed a search of scientific databases, including PubMed, Scopus, and EMBASE. To search in these databases, keywords were used and searching period was limited to the articles published before June 2019, and only articles in English were reviewed.
Eligibility criteria
The cohort studies and cross-sectional studies were eligible for inclusion. Independent variable in this research was conceptualized as sleep disturbances. The following sleep disturbances were included: insomnia, sleep quality, sleep quantity and sleep disorders. Sleep disturbance scales or self-reported items were applied for measuring sleep dimensions. Participants who had sleep disturbances at baseline and were from the general population and the working population were considered eligible. Participants were considered healthy if they were without health problems. The dependent variable was included as back pain. Valid scales, interview, and self-reporting items were considered as the criteria for measuring back pain. Back pain was described as the following: low back pain, sciatic, chronic low back pain, acute low back pain, recurrent low back pain, local low back pain and disabling low back pain. Studies that were found eligible reported odd ratios. Randomized controlled trials, nonobservational studies and review studies were not eligible. Studies with mixed outcome were not eligible either. The studies in which participants had adjusted for physical or psychological comorbidity were also eligible. In most studies the results were controlled for confounders; therefore, some comorbidities were adjusted.
Extraction
The researchers extracted the data from qualified articles, which include the following: the authors and the year of publication of the study, country and continent where studies took place, the type of population which studies were conducted on, follow-up period in cohort studies, age, gender composition of the studies, sample size, types of sleep disturbances and how they were measured, the type of back pain and its results. Extractions were performed by S. Amiri and S. Behnezhad independently. When each of the researchers prepared the extracted information, they finally came together by consensus. Cases of disagreement were resolved through explanation and discussion.
Quality assessment
For qualitative evaluation, four dimensions of the EPHPPC (Effective Public Health Practice Project Quality Assessment) tool [37] were used.
Meta-analysis
The results of the studies are listed in online Table 1 (in the Electronic Supplementary Material). The effect size in this study is the odds ratio. To calculate this index, the researchers referred to eligible articles. For calculating the odd ratio, sample and event of the exposure and nonexposure groups are required. The results of the odds ratio for each study are listed in online Table 1. When the hazard ratio was reported (two studies), they were pooled with the odds ratio. In cases where the prevalence is less than 10%, the odds ratio and risk ratio have relatively similar results. To perform the meta-analysis, the results of each study were converted into a single index, and the result was calculated for each study. Pooling the results was done using random effects method. In total, a number of subgroup analyses were conducted, including continents, study designs, adjusted quality, type of sleep disturbances, and gender. To test the heterogeneity and bias of publication, the χ2 and I2 tests were used [38, 39] and yield two indicators. Other visual (funnel plots) and statistical tests (Begg, Egger, trim-fill) were also performed to estimate the probability of propagation bias [40,41,42].
Result
Study selection
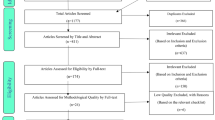
The diagram for study selection is shown in Fig. 1. A total of 9334 articles were found inside the databases. Repetitive and overlapping articles were dropped and the number of the articles decreased to 7345. Articles were reviewed based on abstracts and titles, and 605 articles were reviewed in full-text. Thus, 98 articles remained for evaluating the eligibility. In the qualitative synthesis, 51 articles remained, 30 of which were omitted for the following reasons: three articles due to inadequate results, 2 articles because of adequate results not provided after contacting authors, 3 articles due to the usage of the same databases, and one study because of its low sample size. Furthermore, 21 studies in which the exposure was back pain were also excluded. In all, 21 studies [43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63] including 10 cross-sectional studies, 9 prospective cohort and 1 retrospective cohort were presented for meta-analysis (Table 1 available online). The total population in the meta-analysis consisted of 1,505,124 participants.

Selection flow diagram (From Moher et al. [36]. Open-access article. For more information, visit www.prisma-statement.org)
Quality assessment
Qualitative assessment of the studies was done in four dimensions. Fourteen studies with low selection bias, three studies with moderate selection bias, and four studies with high selection bias were found. Ten articles had low bias, four of the studies had moderate bias and seven studies had high bias regarding the confounder’s bias. Two-way studies showed moderate performance bias and nine studies showed high performance bias. Twelve studies showed low withdrawals/dropouts bias, seven studies had moderate bias, and two studies had high bias.
Sleep disturbances and back pain
Studying the association between sleep disturbances and back pain in Fig. 2 revealed that sleep disturbances, with odds ratio of 1.52 and confidence interval of 1.37–1.68, were associated with back pain (P < 0.001; I2 96.2%).

Sleep disturbances and back pain. OR odd ratio, CI confidence interval
The evaluation of the association between sleep disturbances and back pain based on the type of sleep disturbances are presented in Fig. 3. In insomnia, the results showed that this sleep disturbance was associated with back pain, and odds ratio (OR) was 1.57 and confidence interval (CI) = 1.29–1.90 (P < 0.001; I2 35.3%). Sleeping less than 7 h was associated with back pain, and OR was 1.49 and CI = 1.34–1.65 (P < 0.001; I2 63.0%). Low sleep quality had a nonsignificant association with back pain, and OR was 1.55 and CI = 0.96–2.50 (P = 0.073; I2 88.8%). Other sleep disturbances were associated with back pain, and OR was 1.58 and CI = 1.33–1.89 (P < 0.001; I2 96.9%).

Sleep disturbances and back pain according to sleep disturbances types
The association between sleep disturbances and back pain based on gender is presented in Fig. 4. In men, the OR was 1.49 with CI = 1.34–1.65 (P < 0.001; I2 65.9%). In women, the OR was 1.56 with CI = 1.33–1.81 (P < 0.001; I2 87.6%).

Sleep disturbances and back pain according to gender
The association between sleep disturbances and back pain based on the study design is presented in Fig. 5. In prospective cohort studies, the OR was 1.50 with CI = 1.35–1.67 (P < 0.001; I2 53.2%). In cross-sectional studies, the OR was 1.60 with a confidence interval of 1.28–2.01 (P < 0.001; I2 97.8%).

Sleep disturbances and back pain according to study design
The association between sleep disturbances and back pain based on the adjust quality is presented in Fig. 6. In well adjusted studies, the OR was 1.35 with CI = 1.15–1.59 (P < 0.001; I2 92.8%). In poorly adjusted studies, OR was 1.75 with a CI = 1.49–2.05 (P < 0.001; I2 97.1%).

Sleep disturbances and back pain according to adjust quality
The association between sleep disturbances and back pain based on the continent is displayed in Fig. 7. In European studies, the OR was 1.47 with CI = 1.32–1.64 (P < 0.001; I2 58.2%). In Asian studies, the OR was 1.49 with a confidence interval of 1.23–1.80 (P < 0.001; I2 47.8%). In American studies, OR was 1.41 with CI = 1.20–1.66 (P < 0.001; I2 98.3%).

Sleep disturbances and back pain according to the continent
Publication bias
Evaluation of publication bias using Begg’s test (P = 0.856) and Egger test (P = 0.188) did not show any bias. The funnel plot in Fig. 8 indicates asymmetry. Nine studies were needed to symmetry the graph (trim-and-fill method [42]), the OR was 1.31 with CI = 1.19–1.43 (p < 0.001). The I2 index in 21 studies was 92.6% which indicates a high heterogeneity [64]. χ2 was examined along with the degree of freedom, which was equal to 530.32 (df 20; P < 0.001).

Funnel plot of publication bias
Discussion
The effects of sleep disturbances on back pain were pooled and to this end, 21 cohort and cross-sectional studies were introduced into the systematic review and meta-analysis. After the meta-analysis of the 21 studies, the main result of this study was that sleep disturbance increases the likelihood of back pain by 52%; therefore, people with sleep disturbances are more likely to experience back pain. A study examines the possible mechanism of insomnia effects on back pain [43]. One explanation offered is that both insomnia and back pain may be due to a third factor. The second explanation is that insomnia causes nonspecific back pain. Accordingly, the study suggests a dopaminergic abnormality in both insomnia and back pain [65]. Dopamine is a neurobiological agent that is associated with both insomnia and chronic pain symptoms although the exact nature of this relationship is still unclear. In this regard, a meta-analysis study has shown that depressive symptoms are associated with a higher risk of low back pain and increase the risk by up to 59% [18]. The relationship between dopamine and depression is also expressed [65], and dopamine seems to play an important role in this regard. The relationship between sleep disturbances and back pain problems can also be explained through other mediating factors. Several variables which mediate the relationship between sleep disturbances and back pain can be considered. Insomnia as a sleep disturbance is associated with an increased risk of depression up to 2.27 [66] and as it has been said, an increase in depression is associated with low back pain [18]. Insomnia is associated with low physical activity [67] and it has been found that physical activity can also be a deterrent against the risk of back pain [21].
Another finding of this study was that there was a significant relationship between sleep disturbances and back pain in both men and women, i.e., the rate of back pain was higher in women than in men. Studies have reported a higher prevalence of back pain in women than in men [68]. Given that men are more likely to have unhealthy lifestyles including smoking, alcohol use and eating compared with women [69,70,71,72], an explanation regarding these differences and contradictions is related to somatization of pain which appears to be higher in women [73, 74]. In cross-sectional studies, the relationship between sleep disturbances and back pain was higher than the prospective cohort studies. In studying causal relationships, prospective cohort studies can investigate this issue, but cross-sectional studies cannot investigate this. In addition, the study of the relationship between a variety of sleep disturbances and back pain showed that there was a risk of back pain in insomnia and sleeping fewer than 7 h a day. In studies in which the mixed variables were well adjusted, the risk of back pain was also significant due to sleep disturbances.
The present study which was conducted by systematic review and meta-analysis has limitations and strengths. This is the first study of this type that examines the effects of sleep disturbances on back pain by performing a systematic review and meta-analysis. Both eligible cohort studies and cross-sectional studies were reviewed. These studies were controlled for confounding variables, which could be a strong point in explaining the relationship. Subgroups of analysis were also performed based on adjust quality, which again showed a significant relationship between sleep disturbances and back pain. The relationship between sleep disturbances and back pain based on gender, types of sleep disturbances, study design, adjusted quality and continents were checked. But there are limitations which need to be mentioned. Although this study distinguishes between cross-sectional studies and cohort studies, it should be noted that cross-sectional studies cannot determine causal relationships and this should be considered in the interpretation of the results. Heterogeneity was a subject for this study. The population of the studies varied, which could be one of the causes of high heterogeneity in the current research and should be considered in the interpretation [64]. It should be borne in mind that there are methodological and clinical variations in research. This is inevitable [64] and also increases heterogeneity. But in the analysis of subgroups, this heterogeneity was reduced to a moderate level based on cohort studies. In insomnia, heterogeneity was reduced to a low level. In the study of men, this heterogeneity also decreased to a moderate level. The present studies included different cultures and age groups, so in generalizing the results, these limitations should be considered.
References
Hoy D, Bain C, Williams G, et al. A systematic review of the global prevalence of low back pain. Arthritis Rheum. 2012;64(6):2028–37.
Dagenais S, Caro J, Haldeman S. A systematic review of low back pain cost of illness studies in the United States and internationally. Spine J. 2008;8(1):8–20.
Vos T, Flaxman AD, Naghavi M, et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2163–96.
Andersson GB. Epidemiology of low back pain. Acta Orthop Scand. 1998;281:28–31.
Dionne CE, Dunn KM, Croft PR. Does back pain prevalence really decrease with increasing age? A systematic review. Age Ageing. 2006;35(3):229–34.
Rapoport J, Jacobs P, Bell NR, Klarenbach S. Refining the measurement of the economic burden of chronic diseases in Canada. Chronic Dis Can. 2004;25(1):13–21.
Deyo RA, Cherkin D, Conrad D, Volinn E. Cost, controversy, crisis: low back pain and the health of the public. Annu Rev Public Health. 1991;12:141–56.
Walker BF. The prevalence of low back pain: a systematic review of the literature from 1966 to 1998. J Spinal Disord. 2000;13(3):205–17.
Jeffries LJ, Milanese SF, Grimmer-Somers KA. Epidemiology of adolescent spinal pain: a systematic overview of the research literature. Spine. 2007;32(23):2630–7.
Calvo-Munoz I, Kovacs FM, Roque M, Gago Fernandez I, Seco Calvo J. Risk factors for low back pain in childhood and adolescence: a systematic review. Clin J Pain. 2018;34(5):468–84.
Janwantanakul P, Sitthipornvorakul E, Paksaichol A. Risk factors for the onset of nonspecific low back pain in office workers: a systematic review of prospective cohort studies. J Manipulative Physiol Ther. 2012;35(7):568–77.
Wai EK, Roffey DM, Bishop P, Kwon BK, Dagenais S. Causal assessment of occupational carrying and low back pain: results of a systematic review. Spine J. 2010;10(7):628–38.
Campbell P, Wynne-Jones G, Muller S, Dunn KM. The influence of employment social support for risk and prognosis in nonspecific back pain: a systematic review and critical synthesis. Int Arch Occup Environ Health. 2013;86(2):119–37.
Pinheiro MB, Ferreira ML, Refshauge K, et al. Symptoms of depression as a prognostic factor for low back pain: a systematic review. Spine J. 2016;16(1):105–16.
Taylor JB, Goode AP, George SZ, Cook CE. Incidence and risk factors for first-time incident low back pain: a systematic review and meta-analysis. Spine J. 2014;14(10):2299–319.
Zhang TT, Liu Z, Liu YL, Zhao JJ, Liu DW, Tian QB. Obesity as a risk factor for low back pain: a meta-analysis. Clin Spine Surg. 2018;31(1):22–7.
Shiri R, Karppinen J, Leino-Arjas P, Solovieva S, Viikari-Juntura E. The association between obesity and low back pain: a meta-analysis. Epidemiol Rev. 2010;171(2):135–54.
Pinheiro MB, Ferreira ML, Refshauge K, et al. Symptoms of depression and risk of new episodes of low back pain: a systematic review and meta-analysis. Arthritis Care Res. 2015;67(11):1591–603.
Shiri R, Falah-Hassani K. The effect of smoking on the risk of sciatica: a meta-analysis. Am J Med. 2016;129(1):64–73.e2.
Shiri R, Karppinen J, Leino-Arjas P, Solovieva S, Viikari-Juntura E. The association between smoking and low back pain: a meta-analysis. Am J Med. 2010;123(1):87.e7–87.e35.
Shiri R, Falah-Hassani K. Does leisure time physical activity protect against low back pain? Systematic review and meta-analysis of 36 prospective cohort studies. Br J Sports Med. 2017;51(19):1410–8.
Parreira P, Maher CG, Steffens D, Hancock MJ, Ferreira ML. Risk factors for low back pain and sciatica: an umbrella review. Spine J. 2018;18(9):1715–21.
Bonvanie IJ, Oldehinkel AJ, Rosmalen JG, Janssens KA. Sleep problems and pain: a longitudinal cohort study in emerging adults. Pain. 2016;157(4):957–63.
Ohayon MM. Epidemiological overview of sleep disorders in the general population. Sleep Med Res. 2011;2(1):1–9.
Jike M, Itani O, Watanabe N, Buysse DJ, Kaneita Y. Long sleep duration and health outcomes: a systematic review, meta-analysis and meta-regression. Sleep Med Rev. 2018;39:25–36.
Shi L, Chen SJ, Ma MY, et al. Sleep disturbances increase the risk of dementia: a systematic review and meta-analysis. Sleep Med Rev. 2018;40:4–16.
Afolalu EF, Ramlee F, Tang NKY. Effects of sleep changes on pain-related health outcomes in the general population: a systematic review of longitudinal studies with exploratory meta-analysis. Sleep Med Rev. 2018;39:82–97.
Nalajala N, Walls K, Hili E. Insomnia in chronic lower back pain: Non-pharmacological physiotherapy interventions. Int J Ther Rehabil. 2013;20(10):510–6.
Mathias JL, Cant ML, Burke ALJ. Sleep disturbances and sleep disorders in adults living with chronic pain: a meta-analysis. Sleep Med. 2018;52:198–210.
Finan PH, Goodin BR, Smith MT. The association of sleep and pain: an update and a path forward. J Pain. 2013;14(12):1539–52.
Morin CM, Gibson D, Wade J. Self-reported sleep and mood disturbance in chronic pain patients. Clin J Pain. 1998;14(4):311–4.
Tang NK, Wright KJ, Salkovskis PM. Prevalence and correlates of clinical insomnia co-occurring with chronic back pain. J Sleep Res. 2007;16(1):85–95.
Marty M, Rozenberg S, Duplan B, Thomas P, Duquesnoy B, Allaert F. Quality of sleep in patients with chronic low back pain: a case-control study. Eur Spine J. 2008;17(6):839–44.
Alsaadi SM, McAuley JH, Hush JM, Maher CG. Prevalence of sleep disturbance in patients with low back pain. Eur Spine J. 2011;20(5):737–43.
Andreucci MA, Campbell P, Dunn KM. Are sleep problems a risk factor for the onset of musculoskeletal pain in children and adolescents? A systematic review. Sleep. 2017; https://doi.org/10.1093/sleep/zsx093.
Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Plos Med. 2009;6(7):e1000097.
Armijo-Olivo S, Stiles CR, Hagen NA, Biondo PD, Cummings GG. Assessment of study quality for systematic reviews: a comparison of the Cochrane collaboration risk of bias tool and the effective public health practice project quality assessment tool: Methodological research. J Eval Clin Pract. 2012;18(1):12–8.
Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002;21(11):1539–58.
Ioannidis JP, Patsopoulos NA, Evangelou E. Uncertainty in heterogeneity estimates in meta-analyses. BMJ. 2007;335(7626):914–6.
Begg CB, Mazumdar M. Operating characteristics of a rank correlation test for publication bias. Biometrics. 1994;50(4):1088–101.
Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315(7109):629–34.
Duval S, Tweedie R. Trim and fill: a simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics. 2000;56(2):455–63.
Agmon M, Armon G. Increased insomnia symptoms predict the onset of back pain among employed adults. Plos One. 2014;9(8):e103591–e103591.
Auvinen JP, Tammelin TH, Taimela SP, et al. Is insufficient quantity and quality of sleep a risk factor for neck, shoulder and low back pain? A longitudinal study among adolescents. Eur Spine J. 2010;19(4):641–9.
Benyamina Douma N, Cote C, Lacasse A. Occupational and ergonomic factors associated with low back pain among car-patrol police officers: findings from the quebec serve and protect low back pain study. Clin J Pain. 2018;34(10):960–6.
Chun MY, Cho B‑J, Yoo SH, Oh B, Kang J‑S, Yeon C. Association between sleep duration and musculoskeletal pain: the Korea National Health and Nutrition Examination Survey 2010–2015. Medicine. 2018;97(50):e13656–e13656.
Kaila-Kangas L, Kivimaki M, Harma M, et al. Sleep disturbances as predictors of hospitalization for back disorders—a 28-year follow-up of industrial employees. Spine. 2006;31(1):51–6.
Kardouni JR, Shing TL, Rhon DI. Risk factors for low back pain and spine surgery: a retrospective cohort study in soldiers. Am J Prev Med. 2016;51(5):e129–e38.
Kawaguchi M, Matsudaira K, Sawada T, et al. Assessment of potential risk factors for new onset disabling low back pain in Japanese workers: findings from the CUPID (cultural and psychosocial influences on disability) study. BMC Musculoskelet Disord. 2017;18(1):334–332.
Kim MG, Ahn YS. Associations between lower back pain and job types in south Korean Male Firefighters. Int J Occup Saf Ergon. 2019;15:1–19.
Lusa S, Miranda H, Luukkonen R, Punakallio A. Sleep disturbances predict long-term changes in low back pain among Finnish firefighters: 13-year follow-up study. Int Arch Occup Environ Health. 2015;88(3):369–79.
Miranda H, Viikari-Juntura E, Punnett L, Riihimaki H. Occupational loading, health behavior and sleep disturbance as predictors of low-back pain. Scand J Work Environ Health. 2008;34(6):411–9.
Mork PJ, Vik KL, Moe B, Lier R, Bardal EM, Nilsen TI. Sleep problems, exercise and obesity and risk of chronic musculoskeletal pain: the Norwegian HUNT study. Eur J Public Health. 2014;24(6):924–9.
Rasmussen-Barr E, Grooten WJA, Hallqvist J, Holm LW, Skillgate E. Are job strain and sleep disturbances prognostic factors for low-back pain?A cohort study of a general population of working age in Sweden. J Rehabil Med. 2017;49(7):591–7.
Soe KT, Laosee O, Limsatchapanich S, Rattanapan C. Prevalence and risk factors of musculoskeletal disorders among Myanmar migrant workers in Thai seafood industries. Int J Occup Saf Ergon. 2015;21(4):539–46.
Stubbs B, Koyanagi A, Thompson T, et al. The epidemiology of back pain and its relationship with depression, psychosis, anxiety, sleep disturbances, and stress sensitivity: Data from 43 low- and middle-income countries. Gen Hosp Psychiatry. 2016;43:63–70.
Suri P, Boyko EJ, Smith NL, et al. Modifiable risk factors for chronic back pain: insights using the co-twin control design. Spine J. 2017;17(1):4–14.
Taylor DJ, Pruiksma KE, Hale WJ, et al. Prevalence, correlates, and predictors of insomnia in the US army prior to deployment. Sleep. 2016;39(10):1795–806.
Wei G, Li H, Wang B, Wu J, Wu F, Lin Z. A retrospective cross-sectional survey of non-specific lower back pain among a cohort of Chinese army soldiers. Int J Surg. 2018;56:288–93.
Yabe Y, Hagiwara Y, Sekiguchi T, et al. Sleep disturbance is associated with new onset and continuation of lower back pain: a longitudinal study among survivors of the great east Japan earthquake. Tohoku J Exp Med. 2018;246(1):9–14.
Yang H, Haldeman S. Behavior-related factors associated with low back pain in the US adult population. Spine. 2018;43(1):28–34.
Yoshimoto T, Oka H, Fujii T, et al. Survey on chronic disabling low back pain among care workers at nursing care facilities: a multicenter collaborative cross-sectional study. J Pain Res. 2019;12:1025–32.
Zanuto EA, Codogno JS, Christofaro DG, Vanderlei LC, Cardoso JR, Fernandes RA. Prevalence of low back pain and associated factors in adults from a middle-size Brazilian city. Cien Saude Colet. 2015;20(5):1575–82.
Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557–60.
Finan PH, Smith MT. The comorbidity of insomnia, chronic pain, and depression: dopamine as a putative mechanism. Sleep Med Rev. 2013;17(3):173–83.
Li L, Wu C, Gan Y, Qu X, Lu Z. Insomnia and the risk of depression: a meta-analysis of prospective cohort studies. BMC Psychiatry. 2016;16(1):375–375.
Sherrill DL, Kotchou K, Quan SF. Association of physical activity and human sleep disorders. Arch Intern Med. 1998;158(17):1894–8.
Schneider S, Randoll D, Buchner M. Why do women have back pain more than men? A representative prevalence study in the federal republic of Germany. Clin J Pain. 2006;22(8):738–47.
Ezzati M, Lopez AD, Rodgers A, Vander Hoorn S, Murray CJ. Selected major risk factors and global and regional burden of disease. Lancet. 2002;360(9343):1347–60.
Jha P, Ranson MK, Nguyen SN, Yach D. Estimates of global and regional smoking prevalence in 1995, by age and sex. Am J Public Health. 2002;92(6):1002–6.
Europe WHOROf. The European report on tobacco control policy: progress report on the European strategy for tobacco control 2002–2005. 2006.
Bundesamt S. Gesundheitsbericht für Deutschland: Gesundheitsberichtserstattung des Bundes. Wiesbaden: Metzler Poeschel; 1998.
Nakao M, Fricchione G, Zuttermeister PC, Myers P, Barsky AJ, Benson H. Effects of gender and marital status on somatic symptoms of patients attending a mind/body medicine clinic. Behav Med. 2001;26(4):159–68.
Von Korff M, Dworkin SF, Le Resche L, Kruger A. An epidemiologic comparison of pain complaints. Pain. 1988;32(2):173–83.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
S. Amiri and S. Behnezhad declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Caption Electronic Supplementary Material
Table 1:
Studies included in the meta-analysis
Rights and permissions
About this article

Cite this article
Amiri, S., Behnezhad, S. Sleep disturbances and back pain. Neuropsychiatr 34, 74–84 (2020). https://doi.org/10.1007/s40211-020-00339-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40211-020-00339-9