
Summary
A group effect is generally assumed regarding the prolongation of the QT interval through butyrophenone antipsychotics like haloperidol. Consequently intravenous administration of benperidol is seen critically notwithstanding sparse evidence; thus benperidol and haloperidol were compared regarding their cardiac risk of prolonging the QT interval when administered intravenously for acute sedation of psychotic patients. The QT interval was measured by a 12-lead ECG. For the correction of QT values Bazett’s formula was used. The resulting QTc intervals of the benperidol and the haloperidol group were compared using Mann–Whitney U-test. Our data provide statistical evidence for benperidol being less prone to cause QTc prolongation than haloperidol (p = 0.049). The results of our study indicate a more favourable risk profile of benperidol compared to haloperidol regarding QTc prolongation when administered intravenously.
Zusammenfassung
Ziel dieser Anwendungsbeobachtung ist ein Vergleich der beiden Butyrophenon-Antipsychotika Benperidol und Haloperidol hinsichtlich ihrer Auswirkung auf das QT-Intervall im Zuge einer Akutsedierung mittels i.v.-Injektion. Die QT-Zeiten wurden mit einem 12-Kanal-EKG gemessen und mittels Bazett-Formel korrigiert (QTc). Die ermittelten Zeiten der Benperidol- und der Haloperidol-Gruppe wurden mittels nichtparametrischer Tests verglichen. In der erhobenen Stichprobe zeigt sich, dass Benperidol gegenüber Haloperidol das QT-Intervall statistisch signifikant geringer beeinflusst. Da man bei Butyrophenonen einen Gruppeneffekt bezüglich der EKG-Veränderungen annimmt, wird die i.v.-Applikation von Benperidol ebenso kritisch gesehen wie jene von Haloperidol, obwohl es für Benperidol bis dato nur vereinzelte Fallberichte gibt. Die Ergebnisse dieser Untersuchung deuten darauf hin, dass Benperidol ein günstigeres Nebenwirkungsprofil in Bezug auf kardiale Nebenwirkungen zu haben scheint als Haloperidol (p = 0,049).
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
Due to the occurrence of QT prolongations leading to Torsade de pointes (TdP) and cardiac death, the intravenous administration of the typical antipsychotic haloperidol has no longer been recommended since 2007 [1,2,3].
The department of psychiatry at the Donauspital Vienna decided to continue intravenous (IV) administration as a means of acute sedation. The decision was made due to the assumption that IV medication is less traumatizing for both the patient and the team compared to intramuscular (IM) medication. This might result in a higher acceptance of treatment while safety is warranted by monitoring of vital signs. The treatment was delivered with the recommended safety precautions such as ECG monitoring as well as predefined clinical standards. Data from 2010–2013 were collected, assessed and published in 2014 [4]. Partly due to the adverse outcome of the study regarding QT prolongation, haloperidol has been replaced by benperidol registered for IV use in Germany [5]. Assuming all butyrophenones are capable of causing QT prolongation [6], we evaluated the assumptive QT prolongation during IV administration of benperidol in a clinical setting. The results were compared with the outcomes of the study of Scharfetter and Fischer [4].
To date only a few case studies have analysed the potential of benperidol to lengthen the QT interval [7]. An in vitro study proved that benperidol interacts with the hERG channel [8].
Methods
This case–control study was designed both retrospectively and prospectively. One part of the retrospectively gathered data stems from Scharfetter and Fischer published in 2014 (haloperidol group).
Under consideration of their relevance for the QT value the following parameters were collected: age, sex, blood potassium level, time interval between the single ECG recordings, dose of IV administered medication and dose of oral medication with a potential to lengthen the QT interval.
The following exclusion criteria have been defined for this study:
-
Simultaneous IV administration of a QT-prolonging drug
-
Intervals being too long between the respective ECG recordings in relation to the half-life periods of benperidol and haloperidol (7.65 h for benperidol and 21 h for haloperidol)
-
Incomplete ECG recordings
-
QT value > 500 ms before first administration
A 12-lead ECG was used for the recordings. The ECG was recorded immediately before and after each IV administration of the respective drug. If this procedure could not be applied correctly, the ECG was recorded within the specific half-life period of each drug.
The QT intervals of at least three ECG recordings were measured manually and corrected with Bazett’s formula given below [9].
Because the data within the haloperidol group were not distributed normally, the Mann–Whitney test was used to compare the differences of the QTc values.
Additionally oral administered and potentially QT lengthening medication was not analysed in more detail because the ECG leads were recorded shortly after and before IV administration of either haloperidol or benperidol.
For the statistical analysis, ‘Minitab 16’ was used.
Results
Data were collected from 107 patients. Data from 102 of 107 have been included in the evaluation. Three of 5 patients received benperidol more than 7.65 h after the first ECG recording, 2 patients also received potentially QT-prolonging drugs IM (zuclopenthixol and risperidone). During our study, only one patient did not qualify for IV benperidol treatment and was excluded due to meeting the exclusion criterion according to our clinical standards of more than 500 ms QTc prior to treatment. Characteristics of the two groups are given in Table 1.

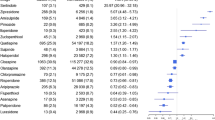
Boxplot comparing QTc difference of benperidol and haloperidol
The average patients’ age was 36.8 (benperidol) or 38.1 (haloperidol) years. The mean potassium level in the blood is 3.6 mmol/l, which already constitutes a mild form of hypokalaemia. Each patient received one vial of either benperidol or haloperidol, which equals a dose of 2 mg or 5 mg.
This study shows that QTc is statistically less prolonged by benperidol than by haloperidol (arithmetic mean 8 vs 16 ms; median: 10 vs. 20 ms; p = 0.049; confidence interval = 95%, see Fig. 1).
Discussion
The risk profile of IV administered antipsychotics concerning cardiac complications such as TdP caused by extension of the QT interval has been discussed intensely and controversially in recent years [10,11,12]. For haloperidol there is some contradictory clinical data regarding its potential to extend the QT range [4, 13, 14], whereas for benperidol there is only one case report [7]. In literature the opinion prevails that all antipsychotics of the butyrophenone type are capable of prolonging the QT range, which appears to be confirmed by in vitro studies with the cardiac hERG channel. Blocking this potassium channel is considered the main reason for QT prolongation [10, 11]. If a drug or substance is able to block more than 50% of the hERG channel in a concentration lower than 100 nm, it is classified as a so-called high potency blocker [15]. Haloperidol as well as benperidol and other butyrophenones meet this definition [8, 15].
The neuroleptic efficacy of benperidol is assumed to be superior over that of haloperidol [16]. This is indicated by the different standard doses (5 mg per vial for haloperidol and 2 mg for benperidol) and by the recommended plasma level (5–17 ng/ml for haloperidol and 2–10 ng/ml for benperidol) [17].
Consequently, having on average administered one standard dose of each substance, respectively, to each of our patients, we feel confident to assume that patients in the benperidol group developed half the effective plasma levels of medication than patients in the haloperidol group (we did not measure plasma level though). We further feel confident to assume that our finding of half the QTc prolongation in the benperidol group is a consequence of the assumably lower plasma levels of benperidol. After all, QTc prologation is known to be dose dependent. Consequently we assume that the lower plasma levels of benperidol required for antipsychotic efficacy are advantageous regarding the risk of adverse cardiac side effects.
So far it is not clear whether the incidence of the occurrence of extrapyramidal motoric adverse effects (e. g. akathisia) and the neuroleptic malignant syndrome vary between the two butyrophenones. Clinical observations and theoretic considerations may suggest a rather unfavourable profile of benperidol regarding the described adverse reactions [18]. For this reason, the applicability of this butyrophenone may be limited to its use in the specific setting of acute sedation.
References
Fachinformation Haldol® Injektionslösung. Janssen-Cilag Pharma GmbH. 2013.
FDA. Information for Healthcare Professionals: Haloperidol (marketed as Haldol, Haldol Decanoate and Haldol Lactate). http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsand Providers/DrugSafetyInformationforHeathcare Professionals/ucm085203.htm. Accessed 07/05/2017.
Mayer-Massetti C, Cheng CM, Sharpe BA, Meier CR, Guglielmo BJ. The FDA extended warning for intravenous Haloperidol and Torsades de pointes: how should institutions respond? J Hosp Med. 2010;5(4):8–16.
Scharfetter J, Fischer P. QTc Veränderungen bei intravenöser Akutsedierung mit Haloperidol, Prothipendyl und Lorazepam. Neuropsychiatrie. 2014;28:1–5.
Fachinformation Glianimon® Injektionslösung. Destin GmbH. 2014.
Messer T, Pajonk FG, Müller MJ. Pharmakotherapie von psychiatrischen Akut- und Notfallsituationen. Nervenarzt. 2015;86:1097–110.
Anonym. Amisulpride/benperidol/olanzapine: QT Interval Prolongation: Case Report. React Wkly. 2014;1497:6.
Silvestre J, Prous J. Comparative evaluation of hERG potassium channel blockade by antipsychotics. Methods Find Exp Clin Pharmacol. 2007;7:457–65.
Bazett HC. An analysis of time relations of electrocardiograms. Heart. 1920;7:353–67.
Nachimuthu S, Assar MD, Schussler JM. Drug-induced QT interval prolongation: mechanism and clinical management. Ther Adv Drug Saf. 2012;3(5):241–53.
DeBruin ML, Pettersson M, Meyboom RHB, Hoes AW, Leufkens HGM. Anti-HERG activity and the risk of drug-induced arrhythmias and sudden death. Eur Heart J. 2005;26:590–7.
Straus SM, Bleumink GS, Dieleman JP, et al. Antipsychotics and the risk of sudden cardiac death. Arch Intern Med. 2004;164(12):1293–7.
Duprey MS, Al-Qadheeb N, Roberts R, Skrobik Y, Schumaker G, Devlin JW. The use of low-dose IV haloperidol is not associated mith Qtc prolongation: post hoc analysis of a randomized, placebo-controlled trial. Intensive Care Med. 2016;42:1818–9.
Gaffigan ME, Bruner DI, Wason C, Pritchard A, Frumkin K. A randomized controlled trial of intravenous Haloperidol vs. intravenous Metoclopramide for acute migraine therapy in the emergency department. J Emerg Med. 2015;49(3):326–34.
Katchman AN, Koerner J, Tosaka T, Woosley RL, Ebert SN. Comparative evaluation of HERG currents and QT intervals following challenge with suspected Torsadogenic and Nontorsadogenic drugs. J Pharmacol Exp Ther. 2006;316:1098–106.
Gardner DM, Murphy AL, O’Donnell H, Centorrino F, Baldessarini RJ. International consensus study of antipsychotic dosing. Am J Psychiatry. 2010;167:686–93.
Baumann P, Hiemke C, Ulrich S, et al. The AGNP-TDM expert group consensus guidelines: therapeutic drug monitoring in psychiatry. Pharmacopsychiatry. 2004;37:243–65.
Leucht S. Therapie der Schizophrenie. München: Urban&Fischer; 2007.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
A. Schmidt, P. Fischer, B. Wally, and J. Scharfetter declare that they have no competing interests.
Rights and permissions
About this article

Cite this article
Schmidt, A., Fischer, P., Wally, B. et al. Influence of intravenous administration of the antipsychotic drug benperidol on the QT interval. Neuropsychiatr 31, 172–175 (2017). https://doi.org/10.1007/s40211-017-0230-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40211-017-0230-5