
Summary
Ambulatory assessment studies may provide important insights in the etiology of suicidal behaviors, because suicidal behaviors and their risk factors fluctuate over time.
The review aims at (1) evaluating the current state of research and (2) summarizing main findings in this field. Reviewed studies (N = 4) were heterogeneous. Up to 74 % of participants reported suicidal ideation during ambulatory assessment sampling. Suicidal ideation was predicted by intensity and instability of negative affective states (e.g., worry, sadness). Ambulatory assessment studies seem a promising approach to uncover the dynamic course of suicidal ideation and its risk factors in clinically relevant time frames (i.e., real-time).
Zusammenfassung
Studien mit ambulanten Assessments können wichtige Einblicke in die Ätiologie suizidaler Verhaltensweisen ermöglichen, da Suizidalität und assoziierte Risikofaktoren zeitlich fluktuierend auftreten.
Der Übersichtsartikel soll 1) die aktuelle Studienlage bewerten und 2) relevante Befunde aus vorhandenen Studien zusammenfassen. Die eingeschlossenen Studien (N = 4) waren heterogen. Bis zu 74 % der Studienteilnehmer berichteten Suizidgedanken während des ambulanten Assessments. Suizidgedanken wurden durch die Intensität und Instabilität negativer affektiver Zustände (z. B. Sorge, Traurigkeit) vorhergesagt. Studien, die diese vielversprechende Methode anwenden, könnten den dynamischen Verlauf von Suizidgedanken und seiner Risikofaktoren in klinisch relevanten Zeitfenstern (d. h. in Echtzeit) abbilden.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Because of their prevalence and drastic outcomes, suicide and suicidal behaviors (ranging from suicidal ideation to suicide attempts) represent a major public health problem [1]. Epidemiological research has empirically established various socio-demographic and psychiatric/psychological risk factors for suicidal behaviors (e.g., male sex, presence of a mental disorder, impulsivity, or critical life events) [2–4]. Most of these risk factors are associated with an increased risk for suicide or suicidal behavior in the long term, but their ability to predict imminent suicide risk is limited [5, 6]. Yet factors increasing the risk in clinically relevant time frames of hours and days are of great importance for clinicians to assess and predict individual suicide risk [6]. For example, observable behaviors and self-reported symptoms such as self-harm, sudden changes in sleeping pattern or intensive and excessive thoughts about death serve as warning signs for an imminent suicidal crisis [6]. In addition, acute risk factors such as hopelessness, agitation, intense anxiety, loneliness, sleep disturbances, and intense negative affect (e.g., rage, self-hatred, guilt) indicate an increased risk for the emergence of suicidal behavior in the short term [2, 7, 8]. Despite their relevance, empirical knowledge regarding short-term risk factors is still limited due to their episodic and transient nature that makes them difficult to study [2, 6]. Suicidal behavior and related risk factors fluctuate over time. However, only few studies so far addressed this issue [2, 9]. Studies using ambulatory assessment (i.e., multiple self-assessments per individual over time) adequately address these needs and may provide important insights in the etiology of suicidal behaviors and their treatment [10, 11]. Beyond that, ambulatory assessment overcomes shortcomings of traditional self-report data (e.g., retrospective bias in self-report questionnaires) and offers additional advantages (e.g., high ecological validity, simultaneous capture of context variables) [12]. The present paper reviews available studies in this field in order to (1) evaluate the current state of research and to (2) summarize main findings with regards to the assumed fluctuation of suicidal behaviors and its risk factors.
Methods
To find relevant ambulatory assessment studies on suicidal behaviors, we conducted a literature search (Web of Science, PubMed). Keywords were ambulatory assessment, experience sampling method, ecological momentary assessment, real-time assessment, diary, suicidal behavior, suicidality, suicidal ideation and suicidal desire. Additionally, reference lists of identified studies were screened. Abstracts were screened and studies employing ambulatory assessment to assess suicidal behaviors were included. All studies were published in English up to June 2014.
Results
Only four studies were identified that used ambulatory assessment to assess suicidal behaviors [13–16]. Table 1 displays characteristics and main results of these studies.
Current state of research and methodology of reviewed studies
Suicidal ideation was either the main outcome or among the main variables under study in the reviewed studies. No study investigated the occurrence of other suicidal behaviors (e.g., suicide attempts or suicide). In terms of sample and methodology, the reviewed studies were very heterogeneous, complicating comparisons between them (see Table 1). Ambulatory assessment was realized in different settings such as everyday life or in a psychiatric hospital. The majority of studies (N = 3) investigated variables predicting the occurrence or intensity of suicidal ideation during the observation period [13, 15]. One study explicitly focused on the feasibility and potential iatrogenic effects of ambulatory assessment in research on suicidal ideation.
Samples were different with regards to age, diagnosis and setting in all four studies included in the review. Yet the majority of participants had a history of suicidal or self-injurious behavior to increase the likelihood for the occurrence of suicidal ideation during the observation period. If reported, compliance rates (i.e., percentage of valid observations) ranged from 58.1 [13] up to 85.7 % in healthy controls [16]. In patients at high-risk (i.e., patients with recent or past suicide attempts) compliance rates of 73.8 and 81.6 %, respectively were achieved [16]. It is noteworthy that two studies employing personal digital assistant and palm to realize ambulatory assessments (i.e., electronic devices minimizing the possibility of delayed responding) demonstrated good compliance rates ranging from 73.8 to 83 % [15, 16]. All studies applied a single-item measure asking about the presence of suicidal ideation. In one study, participants had to answer a gate question about the experience of negative thoughts. If they had positively answered this question they were asked about the presence of thoughts about suicide.
Main findings
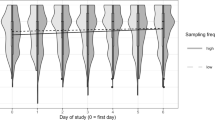
Prevalence of suicidal ideation during the observation period varied from 7.7 % in a low-risk population (i.e., healthy controls) [16] up to 74.2 % in psychiatric inpatients with major depression [14]. In participants with a current psychiatric diagnosis and/or a history of past suicide attempts, the prevalence of suicidal ideation was higher. Predictors for suicidal ideation were identified by three studies (i.e., negative affective states such as worry, sadness or boredom, mean negative mood intensity) [13–15]. Most importantly, the study by Husky et al. demonstrated that repeated assessments of suicidal ideation did not lead to a reactive effect (i.e., day of study or time of day did not predict the occurrence of suicidal ideation) [16].
Discussion
So far, ambulatory assessment research related to suicidal behaviors is still in its infancy, and only four studies have been identified following such an approach. Because of the great heterogeneity of those studies, comparing and summarizing results is somewhat difficult. However, findings underline that suicidal ideation fluctuates over time (i.e., occurs and disappears within hours or days) and negative affective states play a significant role in the prediction of suicidal ideation (i.e., momentary ratings of affective states predict suicidal ideation). The assumption that suicidal ideation and its predictors show a dynamic course is supported. This is in line with current debates suggesting that suicidality is a fluctuating phenomenon [17, 18]. For clinicians, these findings underline the importance of repeated assessments of current mood or presence of suicidal ideation of their patients. Yet the available evidence is not sufficient to give clear recommendations for clinical routine care with regards to the assessment of suicidal behaviors or its short-term risk factors.
Most importantly, the few available studies indicate that assessing suicidal ideation by ambulatory assessment might be a theoretically as well as practically useful approach. To date, the research in this field is, however, inconclusive and future studies need to give further evidence for this claim. Good compliance rates and the absence of reactive effects further demonstrate that the repeated assessment of suicidal ideation does not lead to an increased burden or danger for participating patients [16]. This is in line with other studies investigating the potential iatrogenic effect of repeated questions about suicidal behavior [19]. However, the role that therapeutic relationships may play for suicidal behavior was not addressed by any of the studies.
These results appear promising and further support the use of ambulatory assessment in the investigation of suicidal behavior. Yet it is among the limitations of this review that the search strategy did not include databases such as PsycINFO or PSYNDEX. Moreover, only few and highly heterogeneous studies are available and on this basis it is difficult to derive clear guidelines for the development of studies in this field. Designing such studies remains challenging and some aspects causing specific difficulties need to be mentioned.
First of all, general limitations and methodological challenges related to ambulatory assessment methods (e.g., intrusiveness and participant burden, data security and privacy issues [12], data analysis [20], or item development [21]) apply to ambulatory assessment research on suicidal behavior as well. Discussing these aspects in detail is beyond the scope of the present paper. The investigation of suicide behavior using ambulatory assessment provides specific challenges that will be briefly described in the following section. The relatively low prevalence of suicidal behavior leads to specific demands in the selection of an appropriate study sample and sample size. In populations with low base rates of suicidal behavior (e.g., general population [22, 23], large samples need to be examined to perform statistical analysis and identify risk factors predicting the occurrence of suicidal behavior [16]. However, in samples at high risk for suicide (i.e., persons with a history of suicide attempts or current psychiatric condition (e.g., major depression [24]) a relevant proportion of participants reported suicidal ideation in the reviewed studies. Moreover, it is not clear if the repeated assessments (i.e., asking about mood, affect, etc.) include an interventional effect on the frequency of suicidal ideation (i.e., increase or decrease the experience of suicidal behavior). This eventually leads to serious confounding of results and somewhat limits their ecological validity. Besides, it is possible that participants at risk receive psychotherapeutic or pharmaceutic interventions from their environment (e.g., if psychiatric inpatients are assessed). Because of ethical considerations, suicidal behavior needs to be closely monitored in patients at high risk, and in case of increased suicidality, interventions need to be administered.
Conclusion
Ambulatory assessment research about suicidal behaviors does not currently allow general conclusions about the temporal dynamics and predictors of suicidal behaviors in different populations. While the importance of real-time studies identifying acute risk factors has already been acknowledged for clinical settings, several aspects need to be further investigated. Future studies should address suicidal behavior and its predictors in real-time, extending the assessment to suicidal behaviors beyond suicidal ideation (i.e., including suicidal desire, suicide plans, suicide attempts) [2]. Additionally, analyzing context and setting factors (e.g., interpersonal events, daytime) influencing the occurrence and disappearance of suicidal behavior in detail, is of great interest for research and practice. In conclusion, findings from ambulatory assessment studies targeting suicidal behaviors might play a significant role in the development of intervention and monitoring concepts and, consequently help to understand and prevent suicidal behaviors [25].
Conflict of interest
L. Spangenberg, T. Forkmann, and H. Glaesmer declare that there are no actual or potential conflicts of interest in relation to this article.
References
World Health Organization. Suicide. 2014. http://www.who.int/mental_health/prevention/suicide/suicideprevent/en. Accessed 1 July 2014.
Chesin M, Stanley B. Risk assessment and psychosocial interventions for suicidal patients. Bipol Dis. 2013;15(5):584–93.
Fassberg MM, Van Orden KA, Duberstein P, Erlangsen A, Lapierre S, Bodner E, et al. A systematic review of social factors and suicidal behavior in older adulthood. Int J Environ Res Public Health. 2012;9(3):722–45.
Nock MK, Borges G, Bromet EJ, Cha CB, Kessler RC, Lee S. Suicide and suicidal behavior. Epidemiol Rev. 2008;30(1):133–54.
Hawton K, Comabella C, Haw C, Saunders K. Risk factors for suicide in individuals with depression: a systematic review. J Affect Dis. 2013;147(1–3):17–28.
Rudd MD, Berman AL, Joiner TE, Nock MK, Silverman MM, Mandrusiak M, et al. Warning signs for suicide: theory, research, and clinical applications. Suicide Life Threat Behav. 2006;36(3):255–62.
Hendin H, Al Jurdi RK, Houck PR, Hughes S, Turner J. Role of intense affects in predicting short-term risk for suicidal behavior a prospective study. J Nerv Ment Dis. 2010;198(3):220–5.
Hendin H, Maltsberger JT, Szanto K. The role of intense affective states in signaling a suicide crisis. J Nerv Ment Dis. 2007;195(5):363–8.
Witte TK, Fitzpatrick KK, Joiner TE, Schmidt NB. Variability in suicidal ideation: a better predictor of suicide attempts than intensity or duration of ideation? J Affect Dis. 2005;88(2):131–6.
Trull TJ, Ebner-Priemer UW. Using experience sampling methods/ecological momentary assessment (ESM/EMA) in clinical assessment and clinical research: introduction to the special section. Psychol Assess. 2009;21(4):457–62.
Myin-Germeys I, Oorschot M, Collip D, Lataster J, Delespaul P, van Os J. Experience sampling research in psychopathology: opening the black box of daily life. Psychol Med. 2009;39(9):1533–47.
Trull TJ, Ebner-Priemer U. Ambulatory assessment. Annu Rev Clin Psychol. 2013;9:151–76.
Links PS, Eynan R, Heisel MJ, Barr A, Korzekwa M, McMain S, et al. Affective instability and suicidal ideation amd behavior in patients with borderline personality disorder. J Personal Dis. 2007;21(1):72–86.
Ben-Zeev D, Young MA, Depp CA. Real-time predictors of suicidal ideation: mobile assessment of hospitalized depressed patients. Psychiatr Res. 2012;197(1–2):55–9.
Nock MK, Prinstein MJ, Sterba SK. Revealing the form and function of self-injurious thoughts and behaviors: a real-time ecological assessment study among adolescents and young adults. J Abnorm Psychol. 2009;118(4):816–27.
Husky M, Olie E, Guillaume S, Genty C, Swendsen J, Courtet P. Feasibility and validity of ecological momentary assessment in the investigation of suicide risk. Psychiatr Res. 2014;220:564–70.
Joiner T. Why people die by suicide. Cambridge: Harvard University Press; 2005.
Leboyer M, Slama F, Siever L, Bellivier F. Suicidal disorders: a nosological entity per se? Am J Med Gens Part C Sem Med Gen. 2005;133C(1):3–7.
Gould MS, Marrocco FA, Kleinman M, Thomas JG, Mostkoff K, Cote J, et al. Evaluating iatrogenic risk of youth suicide screening programs—a randomized controlled trial. J Am Med Assoc. 2005;293(13):1635–43.
Ebner-Priemer UW, Eid M, Kleindienst N, Stabenow S, Trull TJ. Analytic strategies for understanding affective (In)stability and other dynamic processes in psychopathology. J Abnorm Psychol. 2009;118(1):195–202.
Palmier-Claus J, Myin-Germeys I, Barkus E, Bentley L, Udachina A, Delespaul P, et al. Experience sampling research in individuals with mental illness: reflections and guidance. Acta Psychiatr Scand. 2011;123(1):12–20.
Ladwig KH, Klupsch D, Ruf E, Meisinger C, Baumert J, Erazo N, et al. Sex- and age-related increase in prevalence rates of death wishes and suicidal ideation in the community: results from the KORA-F3 Augsburg study with 3154 men and women, 35 to 84 years of age. Psychiatr Res. 2008;161(2):248–52.
Forkmann T, Braehler E, Gauggel S, Glaesmer H. Prevalence of suicidal ideation and related risk factors in the german general population. J Nerv Ment Dis. 2012;200(5):401–5.
Sokero TP, Melartin TK, Rytsala HJ, Leskela US, Lestela-Mielonen PS, Isometsa ET. Suicidal ideation and attempts among psychiatric patients with major depressive disorder. J Clin Psychiatr. 2003;64(9):1094–100.
Wichers M, Simons C, Kramer I, Hartmann J, Lothmann C, Myin-Germeys I, et al. Momentary assessment technology as a tool to help patients with depression help themselves. Acta Psychiatr Scand. 2011;124(4):262–72.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Spangenberg, L., Forkmann, T. & Glaesmer, H. Investigating dynamics and predictors of suicidal behaviors using ambulatory assessment. Neuropsychiatr 29, 139–143 (2015). https://doi.org/10.1007/s40211-015-0142-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40211-015-0142-1