
Abstract
Background
Diabetes is a chronic, metabolic disorder characterized by elevated level of blood glucose. In order to delay and prevent diabetes related complications, healthy meal planning and leading active life are very crucial. However, appropriate feeding practice among type 2 diabetic patients is low in many developing countries including Ethiopia. Therefore, the aim of this study was to assess dietary practice and associated factors among type 2 diabetic patients.
Methods
Institution based cross sectional study was conducted from July to December 2019. A total of 422 type 2 diabetic patients who had follow up at the diabetes clinic of the University of Gondar Comprehensive Specialized hospital were include in the study. Logistic regression was used to see the strength of the association between dependent and independent variables. In the logistic regression, both bivariable and multivariable logistic regression analysis were computed to identify factors associated with dietary practice.
Results
The overall prevalence of good dietary practice among type 2 diabetic patients was 46.7 % [95 % CI: 41.7, 51.4]. In the multivariable logistic regression analysis attending secondary and above education [AOR = 4.08, 95 % CI: 1.76, 9.46], high wealth status [AOR = 5.34, 95 % CI: 2.72, 10.50], presence of family support [AOR = 2.54, 95 % CI: 1.40, 4.63], and absence of difficulty of choosing food [AOR = 2.27, 95 % CI: 1.47, 3.53] were significantly associated with good dietary practice.
Conclusions
Less than half of the patients with type 2 diabetes had good dietary practice. Dietary practice was good among high economic status, presence of family support, high educational level and no difficulty of choosing food. Therefore, strengthening income generating activities, improving literacy rate of nations, developing family engagement and food choosing strategies by the health care providers, policy makers and the Government are very crucial to improve good dietary practice among type 2 diabetic patients.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Background
Diabetes mellitus (DM) is a chronic metabolic disorder characterized by high blood glucose level due to problems in insulin secretion, its action, or both [1, 2].
Based on World Health Organization (WHO) 2016 Global report on diabetes indicates that the number of people with diabetes has risen from 108 million to 422 million and specific to adults over 18 years of age the prevalence has increased from 4.7 to 8.5 % between 1980 and 2014 [3].
Diabetes is expected to affect 642 million people by the year 2040, among all diabetic cases two-thirds of it is expected to be occurred in low to middle-income countries [4]. In Africa, more than 14 million people have diabetes, and this prevalence is expected to rise to more than double by 2040 [5]. In Ethiopia there were over 1.33 million cases of diabetes in the year 2015.[6].
Type 2 DM most commonly affects adults and accounts for the vast majority (90–95 %) of people with diabetes around the world. The number of type 2 DM cases in 2011 were 366 million and is anticipated to rise beyond 552 million in 2030 [7, 8].
Evidences showed that diabetes is the 4th or 5th leading cause of death in most high-income countries and it is epidemic in many low- and middle-income countries [4]. Complications from diabetes are resulting in reduced life expectancy, increasing disability and enormous health costs for virtually every society [4, 9]. Each year, 3.2 million people around the world die from complications associated with it [9, 10].
In order to prevent and delay complications related to DM, dietary management is one of the most important modalities of diabetes care [11]. Patients with DM should make a balance between healthy eating, exercise and medication in order to manage diabetes properly [12]. Related to this, most diabetic patients have difficulty of choosing both the quality and the amount of food they have to eat as recommended in order to control the level of glucose in their blood [13]. Dietary practice refers to patients’ choices in food consumption based on diabetes nutrition education that gives emphasis to intake of food with lower fat, higher fiber, and lower sodium [14]. Studies showed that a two servings per day increment in whole-grain intake was associated with a 21 % lower risk of diabetes [15]. A healthy meal plan and being active can keep blood glucose level, blood pressure, and cholesterol level at normal. Continues patient self-management education and support are critical to prevent acute complications, reduce the risk of long-term complications, and early death [16].
To address this problem one of the Ethiopian National Nutrition Program (NNP) initiative is promoting public awareness of healthy life style, increased outdoor activities, increased consumption of fruit and vegetables, reduced consumption of soda beverage and unhealthy behaviour [17].
Previous findings reported in Ethiopia revealed that more than half of type 2 DM patients had poor dietary practice. A study done at Yekatit 12 Medical College Hospital, Addis Ababa, Ethiopia, showed that 51.4 % of the participants had poor dietary practice [18]. Another study conducted at Felege Hiwot referral hospital, Bahir Dar, Ethiopia, among type 2 diabetic patients found out that only 36 % of the patients had good dietary practice [19].
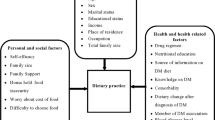
Various previous studies indicated that diabetic patients’ dietary practices are influenced by psycho-socioeconomic factors, such as perceived barriers and personal challenges from family and friends, health care team, work site, organizational and community barriers [20, 21]. Not getting nutrition education in hospitals, having despondency, non-availability of fruits and vegetables and thinking about high cost of foods were identified for having significant associations with poor dietary practice [18].
There is a limited evidence on dietary practice among type 2 diabetic patients in the study area. Therefore, this study aimed at assessing the level of dietary practice and associated factors among type 2 diabetic patients having followed up at the University of Gondar Comprehensive Specialized hospital, northwest Ethiopia.
Methods
Study setting
The study was conducted at the Outpatient department (OPD) diabetic clinic of University of Gondar Comprehensive Specialized hospital from July to December 2019. Gondar City is located 727 km away from Addis Ababa, the capital City of Ethiopia. The hospital is a public hospital and provides preventive, curative and rehabilitative services to the catchment population. In the Outpatient chronic follow up department approximately 200 diabetes mellitus patients visited the clinic every week.
Study design and population
An institution based cross sectional quantitative study design was used to assess dietary practice and associated factors among type 2 diabetic patients who had follow up at the Outpatient department diabetic clinic of University of Gondar Comprehensive Specialized hospital, northwest Ethiopia. All type 2 DM patients attending the clinic were the source population. All adult type 2 diabetic patients aged 18 years and older, having follow up in the diabetic clinic, and randomly selected were participants of this study. Those patients who were critically ill, unable to communicate, pregnant women and who had less than one year of diabetes duration since confirmed diagnosis were excluded from the study.
Sample size determination and sampling procedure
Sample size was estimated using a single population proportion formula by considering the following assumptions; 51.4 % of prevalence of good dietary practice (p) [18], 95 % confidence level and 5 % margin of error (d), yielding 384 samples. Finally, by considering a 10 % non-response rate, the minimum sample size required for this study become 422.
Systematic random sampling technique was used to select study participants. Based up on the information obtained from registration book, every month about 800 DM patients were visiting the clinic. Accordingly, the estimated sample size and the number of patients visiting the clinic were used to determine the sampling interval (K) and was found to be 2. The first participant who was identified by lottery method was 2 and thus, study subjects were recruited at every 4th interval.
Data collection procedures
Data were collected by using structured and pretested questionnaire. The questionnaire was composed of sociodemographic characteristics, ownership of assets, duration of diabetes, lifestyle, behavioural and social factors, health service related factors and diabetic risk factors. Dietary practice of type 2 DM patients was assessed using the general dietary advice of South Africa diabetes association which is used by the Ethiopian diabetes association which contains 11 components. Consequently, in order to classify the dietary practice of participants as good and poor, their responses were computed and the mean value of their responses was taken as a cut-off point. Hence, participants were classified as having good or poor dietary practice if they scored above or below the mean value respectively. A value of 1 was assigned for good dietary practice and a value of 0 (zero) was assigned for poor dietary practice. Relevant patient information was picked up from their medical records. The questionnaire was initially prepared in English and then translated into the local language, Amharic and then translated back to English by language expertise. Laboratory technicians, nurses, and supervisors were participated in the data collection process.
Data quality control
To obtain quality data, maximum efforts were attempted. The data collection tool was pre-tested on 5 % of similar study subjects and setting prior to the commencement of the actual data collection period. As a result, necessary modifications were done on it. Caution was taken while selecting data collectors and supervisors, those who had previous data collection experience were selected. Four diploma and two-degree holder nurse professionals were recruited as data collectors and supervisors, respectively. All of them have received two days training regarding the objectives of the study, interview techniques, ways of approaching the study participants and ethical issues. Furthermore, on spot site check and close supervision were done and completeness of the questionnaire was also checked by the principal investigator on daily basis.
Data management and analysis
After data was coded, cleaned and checked for its completeness, it was entered into EPI data software version 7 and exported in to the Statistical Package for Social Science (SPSS) software version 20 for further analysis. Principal component analysis (PCA) method was used to calculate wealth index score. Individuals monthly income, agricultural productivity, land size, durable household assets, and utility were used to compute it. Descriptive statistics including; frequency, percentage, mean and standard deviation were used to describe variables. In addition, results were presented by using tables, figures, and texts. Both bivariable and multivariable logistic regression analysis were computed to identify variables associated with dietary practice. Independent variables with a p-value of 0.2 and less during the bivariable analysis were fitted in to the multivariable logistic regression analysis to control the effects of confounders. Statistically significant association between independent variables and dietary practice was declared at a p-value of less than 0.05 at 95 % CI in the multivariate analysis.
Ethical considerations
Ethical clearance was obtained from the Ethical Review Board of the University of Gondar. Permission and supportive letter were also obtained from University of Gondar Comprehensive Specialized hospital. Informed written consent was obtained from each respondent by assuring confidentiality throughout data collection period. Participants were clearly informed about the objectives of the study and their rights to refuse, stop or withdraw at any time of data collection.
Results
All (422) study participants have participated and provided a response rate of 100 %. Among those participants, 238 (56.4 %) and 184 (43.6 %) of them were females and males, respectively. The mean (± SD) age of study participants was 51.71 (± 11.40) years. About less than half (41.9 %) of the respondents completed college and above schooling. More than three fourths (78.4 %) of the participants were married and Orthodox Christian followers (79.9 %). More than half (59.0 %) of them had less than five family members (Table 1).
Health status, available health services and behavioral related characteristics
Duration of diabetes mellitus was less than five years for 53.6 % of the respondents. Nearly one thirds (31.5 %) of them had other types of chronic diseases. About 31 % of the participants didn’t get diabetes related nutrition education and 28.9 % of them had reported family history of diabetes.
Regarding to respondents’ behavioural characteristics, a very few (1.9 %) of the patients had responded that they have a habit of smoking. About 10.9 %, 19.9 % and 3.1 % of the participants had a habit of drinking alcohol, physical exercise and did checked their glucose level (Table 2).
Dietary practice among type 2 diabetic patients
The prevalence of good dietary practice in this study was 46.7 % (95 % CI: 41.7–51.4). About more than half (57 %) and 43 % of type 2 DM patients who had good dietary practice were males and females, respectively. The proportion with good dietary practice was 48.7 % and 51.3 % among the age groups of 25–60 and 61 and older (Table 3).
Factors associated with dietary practice
Among thirteen variables fitted in to the multivariate logistic regression analysis, only five of them were remained significantly associated with the outcome variable. Accordingly, in multivariate analysis among those who completed secondary education were 4 times more likely to have good dietary practice thon those who were illiterate (AOR = 4.08, 95 %CI:1.76–9.46). Similarly, the odds: of having good practice were higher among those who were employed than their counterparts (AOR = 3.17, 95 %CI:1.39–7.24). Patients with high economic status were 5 times more likely to have good dietary practice than patients with low economic status (AOR = 5.34, 95 %CI:2.72–10.50). Patients who had family support had higher odds of dietary practice than who hadn’t (AOR = 2.54, 95 %CI:1.40–4.63). Those with had no difficulty to choose food items were nearly twofold to have good dietary practice as compared to those who had difficulty (AOR = 2.27, 95 %CI :1.47–3.53) (Table 4).
Discussion
Diabetes Mellitus is a chronic disease requiring pharmacological and non-pharmacological lifestyle adjustments, of which nutritional intervention is an integral component in management plan. Dietary intake appears to be one of the most important factors related to diabetes care. Cooking and eating practices are related to deeply rooted cultural beliefs and values, which may pose difficulty for patients’ adherence to dietary guidelines [22].
This study tried to address the prevalence of dietary practice and influencing factors among type 2 diabetic patients at University of Gondar Comprehensive Specialized hospital. In the current study the overall prevalence of good dietary practice among type 2 diabetic patients was found to be 46.7 %. This finding is in line with the study conducted in Addis Ababa, Ethiopia (51.4 %) [19].
On the other hand, this figure was lower compared to study findings reported from Brazil (73.0 %) and Nekemet, Ethiopia (55.0 %) [23, 24].The difference in the study period, setting, methodology, and socio cultural characteristics of study participants might be attributable for the variations observed between studies. Studies done in United Arab Emirates, Nepalese, and Felege Hiwot hospital, Bahir Dar, Ethiopia [19, 25,26,27] revealed that lower rates of dietary practice compared to our present study finding. The discrepancy could probably be due to the difference in socio-cultural, economic, diet habit, and time gap between the studies. Again, the variation could also be explained by diabetes and other chronic non-communicable diseases is emerging in Ethiopia and thus, dietary practice of diabetic patients is getting more attention by the Government, health sectors and other stakeholders to enhance the patients’ awareness than so far.
Respondents’ educational status was one of the predictors of dietary practice. It was significantly associated with good dietary practice. The association between being literate and appropriate dietary practice could be partially explained by patients with higher education might be able to access diet and other related information from different medias better than illiterate patients. In addition, educated once might have a good understanding on the diabetes nutrition education received from health care providers and other sources than uneducated once. This, in turn helps them to change those health messages received in to practice. This finding suggested that the paramount importance of education to improve dietary practice and other diabetes related cares. Studies from Nepalese, Pakistan, and Bahir Dar, Ethiopia had reported similar findings [19, 26, 27].
Being employed was another factor identified for good dietary practice. This might be due to people who is employed will not be economically dependent on others and financially secured which, in turn, helps them to access information and buy different food items. Most probably an employed people are more educated and thus, they might have better awareness than unemployed once. A study done at Felege Hiwote hospital, Bahir Dar, Ethiopia was in line with our finding [19].
Respondents who were in the better economic status category were over two times more likely to have good dietary practice compared to those with low economic status. This might be related to rich patients have a better purchasing power than the poor patients. A better economic status enables them to purchase different food items from the market which, in turn, contributes to have good dietary practice. In other words, patients who have economic constraints will not be able to buy different types of foods to ensure their daily nutrition security. Therefore, they will be forced to depend only on some types of specific foods without food preference and thus are at higher risk of getting poor self-dietary management. This evidence was supported by the study conducted in Nepalese [26].
Presence of family support was another factor contributed to diabetic patients’ good dietary practice. Encouraging family support is a means to assist patients by reminding and/or restricting to consume or to avoid some food items and providing psychological support which helps them to adhere with diet recommendations. This evidence suggests that family involvement positively influences DM patients to have a good dietary practice. Similar evidence was reported from a study conducted in Felege Hiwot hospital, Bahir Dar, Ethiopia [19].
Absence of difficulty to choose foods was also identified as a factor for good dietary practice. This may be related to overcome cultural influences and managing their food choice, improving their income, and have clear understanding of the diet-disease relationship. This is supported by the study conducted in Addis Ababa, Ethiopia which showed that those with difficulty of choosing food items for diabetic care were poor in their dietary practice [18].
Limitations of the study
Due to the cross sectional nature of the study design, the current study may not be able to show the temporal relationships between independent variables and good dietary practice. Social desirability bias may also be the other limitation of this study due to self-reported dietary practice was used to measure the prevalence of their dietary practice. In addition, using a quantitative questionnaire; the general dietary advice of South Africa diabetes association which is used by the Ethiopian diabetes association which consists of 11 components to assess the data on the quality of meals, dietary practice of type 2 DM patients instead of using a qualitative tool which could possibly offer a more accurate view of these data, since through this, foods consumed with low frequency can also be reported by patients could also be another limitation of this study. Furthermore, some important variables such as; nutritional status of the patients, frequency of consumption of fruits and vegetables were not included. Finally, as the study was based on samples from a single hospital/health institution, thus, it is impossible to give generalization about the general community.
Conclusions
The findings of this study showed that less than half of the patients with type 2 diabetes mellitus had good dietary practice. As it implies, dietary practice is a major public health concern. Higher level of education, being employed, being wealthy, presence of family support and no difficulty of choosing food items were factors associated with dietary practices of type 2 diabetic patients. Therefore, the government and other concerned bodies should improve the literacy rate, employment status and income of diabetic patients. Health care providers should also provide due attention and strengthen nutrition education and other health messages by involving patients’ families in the hospitals.
Data availability
Data will be available upon request from the corresponding author.
Abbreviations
- ADA:
-
American Diabetes Association
- AOR:
-
Adjusted Odds Ratio
- CI:
-
Confidence Interval
- COR:
-
Crude Odds Ratio
- DM:
-
Diabetes Mellitus
- EDA:
-
Ethiopian Diabetes Association
- FBG:
-
Fasting Blood Glucose
- IDF:
-
International Diabetes Federation
- PCA:
-
Principal Component Analysis
- SADA:
-
South African Diabetes Association
- SD:
-
Standard Deviation
- SPSS:
-
Statistical Package for Social Sciences
- WHO:
-
World Health Organization
References
Alberti KG, Zimmet PF. Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: diagnosis and classification of diabetes mellitus. Provisional report of a WHO consultation. Diab Med. 1998;15(7):539–53.
American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diab Care. 2015;38(Supplement 1):8–16.
World Health Organization. Global report on diabetes. World Health Organization. 2016. https://apps.who.int/iris/handle/10665/204871.
International Diabetes Federation (IDF). Diabetes Atlas. 7th Edition, International Diabetes Federation, Brussels, Belgium. 2015. http://www.diabetesatlas.org.
International Diabetes Federation African Region, (2015) Diabetes Atlas. 7th Edition, International Diabetes Federation, Brussels, Belgium. http://www.diabetesatlas.org.
Ethiopian Diabetes Association. 2014. Available from: http://www.diabetesethiopia.org.et/. Accessed June 17, 2014
Kharroubi AT, Darwish HM. Diabetes mellitus: the epidemic of the century. World J Diab. 2015;6(6):850.
Sami W, Ansari T, Butt NS, Hamid MRA. Effect of diet on type 2 diabetes mellitus: a review. Int J Health Sci. 2017;11(2):65–71.
SShaw JE, Sicree RA, Zimmet PZ. Global estimates of the prevalence of diabetes for 2010 and 2030. Diabetes Res Clin Pract. 2010;87(1):4–14. https://doi.org/10.1016/j.diabres.2009.10.007.
Alberti KG, Zimmet P, Shaw J. Metabolic syndrome-a new world-wide definition. A Consensus Statement from the International Diabetes Federation. Diabet Med. 2006;23(5):469-80. https://doi.org/10.1111/j.1464-5491.2006.01858.x.
Ekore RI, Ajayi IO, Ekore JO. Dietary management of diabetes: a practical approach for primary care physicians in Nigeria. Diabetes. 2008;16:13–4.
Centers for Disease Control and Prevention. National diabetes fact sheet: national estimates and general information on diabetes and prediabetes in the United States, 2011. Atlanta, G.A: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, 2011.
Association SAd. South african diabetes association. In South africa diabetes association; 2001.
N Shamsi, Z Shehab, Z AlNahash - 2013 - King Hamad University Hospital. Factors Influencing Dietary Practice Among Type 2 Diabetics\Bahrain Medical Bulletin. 2013;35(3):130–135.
De Munter JS.L, Hu FB, Spiegelman D, Franz M, Van Dam RM. Whole grain, bran, and germ intake and risk of type 2 diabetes: A prospective cohort study and systematic review. PLoS Medicine 2007;4(8):1385–1395. https://doi.org/10.1371/journal.pmed.0040261
Nutrition Recommendations and Interventions for Diabetes-2008 American Diabetes Association Diabetes Care 2008 31 Suppl 1 S61 S78. 10.2337/dc08-S061 18165339. February 2008 Diabetes Care 31 Suppl 1(Suppl 1):S61–78. https://doi.org/10.2337/dc08-S06
National Nutrition Programme - June 2013 – June 2015. Government of the Federal Democratic Republic of Ethiopia. 2013;C1
Worku A, Mekonnen Abebe S, Wassie MM. Dietary practice and associated factors among type 2 diabetic patients: a cross sectional hospital based study, Addis Ababa, Ethiopia. Springerplus. 2015;4:15. https://doi.org/10.1186/s40064-015-0785-1.
Mulugeta DY, Tefera AA, Aragaw EA. Dietary practice and associated factors among type 2 diabetic patients in Felege Hiwot Regional Referral Hospital, Bahir Dar, Ethiopia. BMC Res Notes. 2018;11(1):434.
Najla, Shamsi; Zainab, Shehab; Zahra, Al Nahash; Shawq, Al Muhanadi; Faisal, Al Nasir. Bahrain Medical Bulletin. 2013;35(3):130–135
Nti CA, David A, Clara O-O. Relationship between dietary practices, physical activity and body mass indices of type 2 diabetics attending a clinic in Accra, Ghana. J Public Health Epidemiol. 2016;8(4):60–6.
Shaw JE, Sicree RA, Zimmet PZ. Global estimates of the prevalence of diabetes for 2010 and 2030. Diabetes Res Clin Pract. 2010;87(1):4–14. https://doi.org/10.1016/j.diabres.2009.10.007.
do Nascimento de Oliveira V, Neto ABL, de Souza APS, Façanha TC, Montenegro RM Jr, Guedes MIF. Demographics factors and food consumption of diabetic patients type 1 in outpatient care of a Federal University Hospital. Diabetol Metab Syndr 2015;7(Suppl 1):A238. https://doi.org/10.1186/1758-5996-7-S1-A238.
Amente T, Belachew T, Hailu E, Berhanu N. Self care practice and its predictors among adults with diabetes mellitus on follow up at Nekemte hospital diabetic clinic, West Ethiopia. World J Med Med Sci [Internet]. 2014.
Al-Kaabi J, Al-Maskari F, Saadi H, Afandi B, Parkar H, Nagelkerke N. Assessment of dietary practice among diabetic patients in the United Arab Emirates. Rev Diabet Stud. 2008;5(2):110.
Parajuli J, Saleh F, Thapa N, Ali L. Factors associated with nonadherence to diet and physical activity among Nepalese type 2 diabetes patients; a cross sectional study. BMC Res Notes. 2014;7(1):758.
Ralineba T, Netshikweta M, Shilubane N. Knowledge and practices associated with diabetes among patients with chronic diabetes mellitus in rural areas of Vhembe District, Limpopo Province, South Africa. J Hum Ecol. 2015;51(1–2):193–201.
Acknowledgements
We would like to thank all study participants for providing their genuine response and valuable time. We would like also to extend our gratitude to University of Gondar Comprehensive specialized hospital, data collectors and supervisors for their valuable time.
Author information
Authors and Affiliations
Contributions
BB conceived the idea of the study, developed the tool, managed data collection, analyses, interpretation, and report writing. TD assisted with tool development, data analysis and interpretation and critically reviewed the manuscript. MS conceptualized and assisted with design of the study, tool development, data interpretation and drafted the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical clearance was obtained from the Ethical Review Board of the University of Gondar. Permission and supportive letter were also obtained from University of Gondar Comprehensive specialized hospital. Informed written consent was obtained from each respondent by assuring confidentiality throughout data collection period. Participants were clearly informed about the objective of the study and their rights to refuse, stop or withdraw at any time of data collection.
Confidentiality of their response were kept using codes instead of any personal identifiers.
Consent for publication
Not applicable.
Conflict of interest
Authors declare that, there is no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Belay, B., Derso, T. & Sisay, M. Dietary practice and associated factors among type 2 diabetic patients having followed up at the University of Gondar Comprehensive specialized hospital, northwest Ethiopia, 2019. J Diabetes Metab Disord 20, 1103–1110 (2021). https://doi.org/10.1007/s40200-021-00752-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40200-021-00752-z