
Abstract
The use of fixed dose combination (FDC) drug therapies has been world-widely accepted for long years due to providing better disease treatment with enhanced therapeutic efficacy and safety as well as improved patient compliance and adherence, and reduced cost to patients than single drug therapies. From many different perspectives, the development of FDC products is likely a promising approach to achieving clinical benefits and business advantages in many classes of drugs. The rationale for drug combinations can be well established only when the potential benefits are based on valid therapeutic principles and substantiated by clinical evidences. Herein, how combination products can be rationalized, individually or combinedly, with respect to category of therapeutic benefits, class of pharmacokinetic and pharmacodynamics interactions, and type of combination effects is first discussed. Potential limitations of FDC products are to be minimized through a careful assessment of benefits to risks by selecting rational component drugs and their doses as well as by either taking their efficacious interactions and/or avoiding their non-efficacious interactions. A series of step-wise product development strategies are necessary to attain target product profiles of prospective oral FDC products set based on their intended clinical use. This review gives an overview of strategies for formulation development of oral FDC products to be optimized differently depending upon prior knowledge of single products and designated dosage regimens of the FDC products, along with highlighting the current issues and challenges arising in formulation development and evaluation on the performance of FDC products.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Fixed dose combination (FDC) drug products, in which two or more active pharmaceutical ingredients with different modes of pharmacological action are formulated in a fixed proportional manner into a single dosage form, are prevalent for the disease prevention and treatment in almost all therapeutic areas (Desai et al. 2013; Kararli et al. 2014a; Pourkavoos 2012). The use of FDC drug therapies has been widely accepted for long years due to providing enhanced clinical effectiveness and safeness, improved patient compliance and convenience, and reduced treatment cost to patients over single drug therapies, which can lead to increased patient adherence to the combination therapy and eventually improved disease treatment and management (Bangalore et al. 2007; Kararli et al. 2014b; Mitra and Wu 2012; Pan et al. 2008). These benefits of combination therapies may come out of only taking appropriate, multiple target, fixed-ratio drug combinations, and collectively reducing multiple risk factors of the relevant diseases without increasing the risk of adverse effects (Mitra and Wu 2012). FDC drug products have been playing important roles in treating human immunodeficiency virus/acquired immune deficiency syndrome (HIV/AIDS), malaria, tuberculosis and cardiovascular (CV) diseases as well as have made significant contributions to improving public health through enhanced patient care and compliance with lower costs, as recognized by the World Health Organization (WHO) and regulatory authorities in many countries (EMA 2015; FDA 2015; Orloff 2005; WHO 2005). As such, FDC products have been increasingly licensed for the medical treatment areas of communicable and life-threatening diseases over the world (Kararli et al. 2014b, Pourkavoos 2012; WHO 2003). From a clinical (physician) perspective, FDCs can offer enhanced therapeutic efficacy and safety profiles with improved patient adherence and reduced development of drug resistance (Bangalore et al. 2007; Desai et al. 2013; Pan et al. 2008). Also, FDCs can benefit patients through improved convenience and compliance, reduced dosing unit burden, and cost savings. Especially, elderly patients usually need multiple medications to treat age related chronic complex diseases and their co-morbidities. FDCs are more cost-effective than individual drugs administered separately (Newman et al. 2008; Pourkavoos 2012). The manufacturing and distribution costs of FDC products are generally low compared with separate products (Desai et al. 2013). From an industrial perspective, pharmaceutical companies may have opportunities to maximize the value of their own single drug products, to sustain their product’s life, and ultimately to extend market exclusivity with a resultant increase in sales and profits (Hiremath et al. 2011).
Likewise, the number of FDC products has increased over the past two decades and the trend is likely to continue on account of offering various clinical benefits and business advantages in many drug classes (Hiremath et al. 2011; Kararli et al. 2014b). Most combinations of established drugs generally bring about low risk due to less development activities and burdensome regulatory process to approval because the safety and efficacy evidences of individual drugs have already been secured (Desai et al. 2013; Pourkavoos 2012). To this date, FDC products have been developed mainly for substituting for free combinations being frequently used, treating two closely related diseases and resolving unmet needs of patients insufficiently controlled by monotherapies (Pourkavoos 2012). Recently, FDC drug products actually hold a considerable portion (>25%) of the new drug products approved by the Unite States (US) Food and Drug Administration (FDA) (Desai et al. 2013; Kararli et al. 2014a, b). A significant amount of world-widely, newly approved drug products are FDC products which keep most of the recent blockbusters in the global pharmaceutical market. Accordingly, the market size of FDC products has been growing (Hiremath et al. 2011; Pourkavoos 2012). Oral route of administration is most commonly used for FDC products, although parenteral, inhalation, transdermal and transmucosal types of FDC formulations are available. The oral FDC drug products have been proven to be highly advantageous and technologically advanced in the treatment of various diseases such as cancer, tuberculosis, HIV/AIDS, hepatitis B and C virus infection (HBV/HCV), hypertension, dyslipidemia, diabetes, pain and other CV diseases (Borghi and Cicero 2010; Farnier 2011; Sanz and Fuster 2009; Sica 2002). Some selected examples of oral FDC drug products recently approved in the US and worldwide market are listed in Table 1. Predominant CV FDC products are for hypertension and dyslipidemia, major infectious FDC products are for HIV/AIDS and HCV, and diabetes is most in metabolic FDC products (Desai et al. 2013; Farnier 2011). Long-term concurrent therapies employing oral FDC drugs are recognized to be more effective for the patient populations with multiple chronic diseases that are readily affecting to each other (Desai et al. 2013). As the high risk patient population continues to grow, the use of early combination therapy will likely increase by proactively reducing the multi-morbidity, mortality and organ damage (Liu et al. 2014; Kumar et al. 2008). To maximize some potential of combination therapy to slow down disease progression, more aggressive treatment with earlier drug combinations has been investigated (Woodcock et al. 2011). Development strategies of rational FDC drug products for the better treatment of complex and refractory diseases are currently being explored within global pharmaceutical industry (Kararli et al. 2014c).
Nevertheless, FDC products may bring about suboptimal effectiveness, unexpected adverse effects and safety issues, inclusion of unneeded drugs, reduced dosing flexibility and unacceptable dosage (WHO 2005; FDA 2015). These limitations are to be minimized through a careful assessment of benefits to risks by selecting rational multiple target component drugs and their doses as well as by using the most optimized product development strategies (WHO 2003; Woodcock et al. 2011). Theoretical rationale for drug combinations should be established prior to FDC drug development and later substantiated by clinical evidences. Besides establishing the rationale and target populations for proposed combinations and accumulating the development information of component drug products, there exist substantial hurdles in fulfilling regulatory requirements for approval during FDC product development (Orloff 2005; Pourkavoos 2012). The formulation and manufacturing development for acceptable FDC products are certainly more complicated and require more activities than those of the individual single products, which undoubtedly carry various kinds of issues and challenges (Siew 2015; Desai et al. 2013). Combination drug delivery and formulation technologies available currently or being developed need to be applicable to achievement of the drug release and pharmacokinetic (PK) profiles of component drugs inside FDC products realizing their designated dosage regimens. Overall, a series of step-wise product development strategies are necessary to attain target product profiles of prospective FDC products set based on their intended clinical use. In this review, a comprehensive discussion is first presented on the rationale for developing drug combinations, selection of component drugs and its rationality. Focusing on oral FDC products, this review also gives an overview of the strategies and technologies of combination formulation development along with the product performance evaluation.
Rationale for developing drug combinations
Unmet treatment needs
Treatment with single drugs acting on specific targets is often evaluated to be suboptimal in the treatment and management of complex and refractory diseases (Liu et al. 2014; Pourkavoos 2012). The existing drugs used for the diseases may have some limitations, including suboptimal efficacy and safety, serious side or adverse effects, short duration of action, drug resistance, and/or anything else that causes insufficient therapeutic effects. Although single target drugs have distinct regulatory activities on their designated targets, they cannot always exhibit desired therapeutic effects on all the respective pathophysiological characteristics (Liu et al. 2014). Any single targets can rarely produce satisfactory therapeutics for the treatment of many complex diseases. Also, any active compounds with lack of perfect selectivity can interact with off-targets other than their primary targets and all the targets can have other physiological functions in addition to their roles in principal actions, which may cause unexpected side effects. As such, novel or better therapeutic outcomes can hardly be achieved with even larger doses of single target drugs. CV diseases and their complications have multiple pathogenesis and are the end result of complex pathophysiology from metabolic diseases, which require multiple target drug therapies (Kumar et al. 2008; Sanz and Fuster 2009). Combination drug therapies for CV disease treatment and prevention become highly recommended options to prevent or delay the multiple morbidity and mortality pertinent to CV diseases and their risk factors (Orloff 2005; Sanz and Fuster 2009). A particular patient group has unique characteristics in terms of age, physical state of functions, pathophysiological conditions, co-existing diseases, differentiated drug response and resistance, pharmacogenetics and genetic polymorphism affecting PK and pharmacodynamics (PD). This may need appropriate selection of drugs with different pharmacological mechanisms suitable for the patient groups, and reasonable determination of their doses and dosing frequency (Pourkavoos 2012).
Rationale for drug combinations
A potential combination of drugs would be therapeutically effective for the treatment and risk reduction of a target disease if the combination drug therapy could demonstrate better clinical outcomes than any of the single drug therapies (Mitra and Wu 2012; Pourkavoos 2012). The rationale for drug combinations can be well established only when the potential benefits are based on valid therapeutic principles and substantiated by clinical evidences (Orloff 2005; Pourkavoos 2012), as summarized in Table 2. The combination of drugs with different modes of action from which each drug shows principal effects to treat same pathophysiological signs or symptoms are generally rationalized according to the following categories of therapeutic benefits or advantages:
-
1.
There is an addition or potentiation of the therapeutic activities of individual drugs resulting in an enhanced efficacy with a similar safety or tolerability profile, or a similar efficacy with an improved safety or tolerability profile. A FDC product can be more effective than the higher doses of component drugs with similar side or adverse effects, or as effective as the higher doses of component drugs with lower side or adverse effects. This rationale basically comes from potential additive or synergistic effects involving PD and PK interactions of individual component drugs, and/or their reduced doses when combined. A number of marketed FDC drug products have been developed on the basis of enhanced efficacy and/or tolerability, including an antihypertensive with another antihypertensive (e.g., lercanidipine with enalapril), an antihypertensive with a diuretic (e.g., telmisartan with hydrochlorothiazide) and an antidiabetic with another antidiabetic (e.g., glipizide with metformin) (Borghi and Cicero 2010; Mandal and Pal 2008; Rosenthal and Gavras 2006; Sica 2002) The lower dose combination of the calcium channel blocker (CCB), lercanidipine and the angiotensin converting enzyme (ACE) inhibitor, enalapril has greater blood pressure lowering efficacy than the higher dose of either component alone as well as is well tolerated with similar adverse effect rates to the single drug therapies (Borghi and Cicero 2010; Wald et al. 2009).
-
2.
This category of clinical benefits is improvement in symptomatic and PK profile using at least one component not previously approved for a relevant indication. The pharmacological intensity and duration of one component drug can be increased through changes in its PK behaviors caused by other components. Alternatively, the improved safety profile of one drug can be achieved by diminishing its dose-related side or adverse effects on the basis of some interactions with other components. The addition of booster agents (e.g., cobicistat) is for enhancing the antiretroviral effect of protease and integrase inhibitors (e.g., ritonavir and darunavir) (Marzolini et al. 2016; Putcharoen et al. 2015; Shah et al. 2013). A combination of buprenorphine, a partial opioid agonist and naloxone, an opioid antagonist is used to minimize the opioid addiction of buprenorphine.
-
3.
Better clinical outcomes without benefits of enhanced efficacy and safety may be reasonably anticipated by the improved patient compliance derived from the simplified therapies with drug combinations. A combination drug product has a single dosage form and is supposed to provide a dosing regimen unified for the component drugs that are contained in separate dosage units and administered on different dosing schedules in single drug therapies, which can reduce dosage unit burden, simplify disease medication and management, and improve patient adherence to the combination therapy. The improved patient compliance and adherence can lead to better patient care and clinical outcomes particularly for patients taking several medicines at the same time as well as for complex and refractory diseases to be treated in a long-term with heavy schedules of relevant multiple drugs (Bangalore et al. 2007; Pan et al. 2008). Novel combination drug products should have at least one or more clinical benefits or advantages.
The enhanced efficacy and safety profiles shown in rational combination drug products are substantially associated with drug interactions, PD interactions in which the effects of one drug are modified at its action site by another drug, and PK interactions in which the absorption, distribution, metabolism and excretion behaviors of one drug are altered by the other drug (Jia et al. 2009; Liu et al. 2014). The enhanced efficacy and safety can be the results from the sum of independent actions of individual components and/or their beneficial PD and PK interactions. The PD interactions can be grouped, based on the action sites (targets) of active ingredients, into acting on same targets and acting on different targets in the same or different biological pathway. The PK interactions can also be classified into four groups, which are regulation of drug transport (or permeation) and distribution, and interaction of drug metabolism and elimination. The PD and PK interactions are mutually related and multiply involved in the therapeutic effects of drug combinations at the same time. There are examples of efficacious PD interactions: Emodin complements the inactivation of protein kinase B by celecoxib and the combination has synergistic effect of enhanced growth repression (Lai et al. 2003), and exenatide decreases rosiglitazone-associated myocardial infarction and the combination can increase the antidiabetic efficacy (Zhao et al. 2013). There are examples of efficacious PK interactions: probenecid inhibits the renal tubular secretion of ciprofloxacin to prolong the plasma retaining time of ciprofloxacin, and anamorelin (ghrelin mimetic) elevates the absorption rate of zolmitriptan (antimigraine drug) to improve the migraine treatment (Hiremath et al. 2011; Liu et al. 2014).
Further, the four types of combination effect can be individually or combinedly used to establish the therapeutic rationale for combination drugs (Liu et al. 2014; Orloff 2005; Pourkavoos 2012):
-
1.
The first type is additive or synergistic effect. The individual component drugs in combination drugs affect the same primary PD end-point (marker or surrogate) with different pharmacological mechanisms and can make contributions to additive or synergistic effects of the combinations on the reduction of disease severity and risk. This type of additive effect is common in antihypertensive, antiviral and antidiabetic combinations. Another example is a combination of a statin and ezetimibe which lower both plasma cholesterol levels. A statin inhibiting endogenous cholesterol synthesis as a HMG-CoA reductase inhibitor and ezetimibe inhibiting intestinal cholesterol absorption are combined to work additively, as clinically found, to lower CV and cerebrovascular risks and events pertinent to elevated low density lipoprotein cholesterol. The coverage of prolonged period in allergy relief is a result of additive effect from the combination of short-acting pseudoephedrine and long-acting loratadine. Additionally, synergistic effects from combination drugs may potentially bring about enhanced efficacy and tolerability by reducing their doses or developing new formulations and administration methods. The combination of two antiplatelet drugs, aspirin and extended-release dipyridamole, was found to have synergistic effects, showing significantly better efficacy of reduced risk of stroke than the co-administration of the two drugs (Serebruany et al. 2004).
-
2.
The second type is complementary combination effect. The individual component drugs in combination drugs address different primary PD end-points and can make contributions to additive or synergistic effects of the combinations on the reduction of disease risk and complications. This complementary effect often appears in the combinations of an antihypertensive or antidiabetic with a statin (e.g., amlodipine with atorvastatin, olmesartan with rosuvastatin, sitagliptin with simvastatin and metformin with rosuvastatin). The coexistence of hypertension and dyslipidemia or type 2 diabetes and dyslipidemia has been reported to be prevalent and cause the increase in CV risk factors and their interactions (Karim et al. 2013; Park et al. 2016a, b). These combination therapies can be effective for comprehensive control of complex coronary heart diseases and their complications.
-
3.
The third type is cooperative combination effect. One of component drugs with different pharmacological mechanisms can affect the activity of the other to provide the combination with an optimized balance of therapeutic efficacy and safety, which may lead to enhancement of effectiveness, reduction of adverse effects, drug resistance and/or abuse potential of the component drug(s). In the cooperative drug combinations, examples include amoxicillin plus clavulanic acid (effectiveness of amoxicillin enhanced by clavulanic acid, an inhibitor of β lactamases), aspirin plus omeprazole (adverse effect of aspirin alleviated by omeprazole, a proton pump inhibitor), rifampicin plus isoniazid (drug resistance of rifampicin reduced by isoniazid, an antituberculosis agent), and diphenoxylate plus atropine (decreased abuse potential from the opioid-like effect of diphenoxylate counteracted by the anticholinergic effects of atropine).
-
4.
The last type of combination effect is convenience and improved patient compliance by reducing dosage unit burden. The combination drugs, usually so called “polypill”, containing several component drugs with different pharmacological mechanisms address complex and refractory coexisting diseases and/or their multiple risk factors. For example, this type of drug combinations of convenience, i.e., multiple combinations of antihypertensive, anticholesterol, antidiabetic and antiplatelet drugs, can collectively regulate a number of risk factors caused by the coexistence of hypertension, dyslipidemia, diabetes and/or obesity. Many combinations of several antiretroviral agents are cocktail therapies in HIV/AIDS, with reduced dosing burden and cost, to raise the genetic barriers to HIV replication and to lower the probability of drug resistance.
However, drug combinations may have toxicities, additive or synergistic adverse effects coming from combination of active components itself and increased chances of their multiple unbeneficial interactions. Any irrational selection of active components and their doses may also cause undesired therapeutic effects, serious side or adverse effects and exposure of patients to unnecessary drugs (Gautam and Saha 2008). Additional disadvantages deriving from fixed dose formulations include lack of dosing flexibility, misidentification of causes for undesirable effects and instability of FDC products (WHO 2003; Desai et al. 2013). The ratio of benefit to risk for a FDC product should be at least as good as that of its individual component drugs. A careful assessment of potential benefits to possible risks should be conducted based on unmet treatment needs and characteristics of a defined patient population to obtain solutions giving a reasonable balance between of therapeutic benefits and risks. These limitations could be minimized by selecting rational multiple target component drugs and their doses, taking their efficacious interactions and/or avoiding their non-efficacious interactions as well as by using optimized product development strategies (Liu et al. 2014; Pourkavoos 2012).
Selection of component drugs and its rationality
In order to justify the potential rationale for a combination drug with intended therapeutic indications, the foremost mission is to select the most appropriate active components therapeutically contributing to its desired combination effects and efficacious drug interactions (Pourkavoos 2012). A combination of therapeutic targets necessary for the combination drug is first selected based on the pathogenesis and pathophysiological characteristics of targeted diseases. Following proposed selection of combination components, theoretical potential of the drug combination effects is later evaluated using the pharmacological and biopharmaceutical properties of the component drugs and the previously accumulated information of their single drug products. Careful considerations must be given to the mechanisms and targets of action, and PK properties of the component drugs (Mitra and Wu 2012). The theoretical rationale for the combination effects and benefits (i.e., improved efficacy and safety to the patient population) is established through PK and PD characterization of the combination drug. When accepted PD biomarkers for clinical effectiveness are available, the effects of the individual components and the combination drug on the PD end points can be studied and may be sufficient for evidencing the contributions of the component drugs as well as establishing the therapeutic efficacy and safety of the combination drug (Orloff 2005). Previously approved single-target and multi-target drugs are mostly chosen as active ingredients of most FDC products for multiple target treatment. The well-documented development data and information of established drugs often prescribed concomitantly may minimize the number of new studies needed to establish efficacy and safety of the proposed combination drug (Pourkavoos 2012). The component drugs having similar PK behaviors are favorable. Their different PK requires particular formulation strategies and technologies to resolve the issues of their inconsistent dosage and dosing frequency.
The examples of rational selection of component drugs include a progestin with a validated estradiol analog, an antihypertensive with hydrochlorothiazide, an antihypertensive with a statin, an antidiabetic with metformin, an antihistamine with pseudoephedrine and so forth. There are many cases of irrational selection of component drugs. The addition of niacin and laropiprant to a statin did not reduce the risk of major vascular events but elevated the serious adverse effects (The HPS2-THRIVE collaborative group 2014). The combinations of aliskiren (renin inhibitor) with ACE inhibitors or angiotensin receptor blockers (ARB) are not recommended for hypertensive patients with diabetes because they cause the risk of renal impairment, hypotension and hyperkalemia. The addition of acetaminophen to nimesulide did not enhance the therapeutic efficacy but increased hepatotoxic effects. The FDC products of quinolones and nitroimidazoles can increase antibiotics resistant strains of microorganisms rapidly. Rationale for the selection of component drugs should consider their reasonable doses and dosing frequency. Their doses can be increased or decreased but their ratio is fixed in FDC products, which is particularly problematic if both component drugs require dose titration. The dose strengths of the individual components need to be considered to be able to allow flexibility of dosing. Low dose combination drug therapy has the chance of reducing dose-related adverse effects and improving efficacy (Wald et al. 2009). FDC products should contain the appropriate drug ratios and minimal doses that are safe and effective in a significant proportion of the defined patient populations. The number of FDC dose strengths should be finalized through development needs and regulatory guidelines because it impacts the key clinical study designs. Developing too many dose FDC products could nullify the object of creating a simplified combination therapy (Pourkavoos 2012).
Regulatory considerations on oral FDC drug products
The WHO guidelines to assure safe and effective use of FDCs require that “New FDC drugs are regarded as new drugs in their own right. They are acceptable only when the dosage of each ingredient meets the requirements of a defined population group, and the combination has a proven advantage over single compounds administered separately in terms of therapeutic effect, safety or compliance. They should not be treated as generic versions of single-component products.” (WHO 2003, 2005). The US FDA’s policy on the approval of FDC products for humans states that “Two or more drugs may be combined in a single dosage form when each component makes a contribution to the claimed effects and the dosage of each component (amount, frequency, duration) is such that the combination is safe and effective for a significant patient population requiring such concurrent therapy as defined in the labeling for the drug.” (FDA 2006, 2015). European Medicines Agency (EMA) also guides the similar rule for FDC products (EMA 2015).
In summary, for the global approval of a FDC product, there should be unequivocal evidences for the following requirements but not limited to: (1) there are its demonstrable medical needs; (2) its rationale and patient population are established; (3) it contains the appropriate ratios and minimal doses of its component drugs; (4) all the classes of information of its component drugs are documented; (5) it has clinical safety and efficacy for its patient population; (6) the ratio of its benefits to risks is at least as good as that of its component drugs; (7) the contribution of each of its individual components to its claimed effects is established; (8) its PD and PD studies in healthy subjects, patients, and high-risk subgroups are performed; (9) its beneficial and unbeneficial PK and PD interactions are analyzed; (10) all the categories of information of its chemistry, manufacturing and control, and quality are documented; and (11) all the levels of information of its stability are documented.
Formulation development of oral FDC drug products
Formulation development challenges and strategies
Formulation development and manufacturing of acceptable FDC products are certainly more complicated and require more activities than those of the individual single products, which undoubtedly carry various kinds of issues and challenges (Siew 2015; Desai et al. 2013). The high complexity arises from formulation processes for putting together two or more component drugs with different physicochemical and biopharmaceutical properties into a single dosage form from which is designed to exhibit new drug performance, differently from their single formulations. New issues and challenges usually unhappened before the combination may include the followings: (1) dose proportionality and dose ratios of active components: (2) number of dose strengths of active components; (3) physicochemical incompatibility between active components or active components and excipients used in the FDC formulation; (4) drug–drug interactions; (5) changes in drug release (or dissolution) and PK profiles of active components; (6) development needs of various simultaneous analytical and testing methods for active components; (7) development needs of new combination formulation and drug delivery technologies: (8) increase in dosage bulk volume (or weight); (9) undesirable processing and manufacturing characteristics; (10) increase in quality attributes; and (11) increase in stability testing items.
Multiple dose strengths are common in FDC products. The number of dose strength combinations may have a profound impact on the technical complexity of formulation design, manufacturability, productivity, and bioequivalence (BE) studies. To cope with this issue, alterative dosage forms and formulation options need to be proactively prepared. For FDC products with dose proportionality which can accommodate the formulation development, it is possible to obtain bio-waivers for the lower dose strength combinations after establishing the BE for the highest dose strength combination. However, disproportionate drug dose combinations are challenging in achieving good content uniformity and process optimization. The different physicochemical properties in solid and solution state as well as processing characteristics of individual component drugs should be carefully considered for the formulation design and process development of FDC drug products. Also, the component drugs need to be classified according to biopharmaceutics classification system (BCS) to identify what formulation design and technologies are to be used for controlling drug release, absorption and BE. Solubilization and absorption enhancement technologies are used to secure BE and to improve bioavailability (BA). Simultaneous analytical and testing methods for active components should be developed in advance, where there exists difficulty. The active components composing a FDC product should be assessed for physicochemical compatibility, along with their excipients, to ensure that either their impurities are not generated or unfavorable drug–drug interactions are prevented. Incompatibility among active components can lead to physicochemical instability of the FDC product, loss of BA and safety issues which are challenging in developing a viable FDC product. Compatibility test in FDCs are always the first step in formulation design and process development. In drug–drug and drug–excipients incompatibility cases, it is critical to formulate FDC products to mitigate such interactions by keeping the active components separated.
A FDC product is supposed to provide a dosing regimen unified for the component drugs that are contained in separate dosage units and administered on different dosing schedules in single drug therapies. The FDC product requires a formulation platform for managing two or more drugs in a single unit to be separately released at proper rate and duration at different action sites. Each drug needs a release unit exhibiting its own drug delivery program, assembly of two or more systems stuck together to form a single dosage form. Although there are several ways to assess the equivalency between a FDC and co-administered individual single products, establishing BE is a very favorable approach compared to therapeutic equivalence as a clinical strategy for FDC development due to shorter development timeline and less resource intensive (Mitra and Wu 2012). In general, achieving BE between FDC product and individual single products is much more difficult than demonstrating BE of different formulations of a single drug. In addition to the increase in failure possibility due to multiple PK end-points, there are other challenges in achieving BE that are unique to FDC products. Drug–drug interactions in FDC products and possible food effects on the drug components need to be evaluated carefully. Some drugs may have positive or negative food effects. In case of positive food effects, the drug BA is increased significantly in a fed state compared to in a fasted state. The BE failure risk is high for BCS Class IV drugs (drugs with low solubility and low permeability) compared to other BCS classes of drugs. The potential BE failure risk also needs to be considered in selecting the FDC formulation option.
Dosage form design and formulation technologies
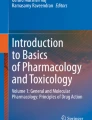
The selection of FDC drug formulations is mainly based on (1) the physicochemical compatibility among the active pharmaceutical ingredients (APIs) as well as their excipients, (2) the similarity of drug release profiles, and (3) the drug loading of APIs. An example decision tree for the formulation design of a FDC product is shown in Fig. 1. These challengeable hurdles make the FDC delivery systems more complex than single API product.

Decision tree for the formulation design of a FDC
Monolithic systems
The drugs which are compatible with each other and require the similar dissolution profiles can be combined in a single homogeneous system. The monolithic FDC tablet consists of mixed two or more APIs in single layer tablet. Since it is easily prepared using conventional single-layer tablet presses, the monolithic system is the first choice to develop FDC tablets. Although it is simple in developing formulation and manufacturing process, the suitability of the drugs in monolithic systems should be thoroughly investigated. In case of FDC drugs combined the drugs of which absorption mechanisms are different such as the combination of BCS Class II and BCS Class III drugs, the dissolution rate of poor soluble drug, i.e. the BCS Class II drug, may be decreased in FDC formulation, thereby changing its BA (Desai et al. 2013). Although telmisartan and hydrochlorothiazide require the similar immediate release profiles, an alkaline excipient which can degrade hydrochlorothiazide is required for telmisartan formulation, which is not recommended in monolithic system (Nakatani et al. 2014).
Non-monolithic systems
Since the close contact between drug–drug or drug–excipients can facilitate incompatible drug interactions in monolithic systems, APIs unacceptable in monolithic system in FDC have to be separated. API-separation technologies in FDC include bilayer/multi-layer tablets, multiparticulate systems, active coating and hot melt co-extrusion approach.
Bilayer/multi-layer tablets
Bilayer/multi-layer tablets composed of two or more compressed layers can be one of the best options to circumvent physicochemical incompatibilities of APIs or to achieve the different drug release profiles of each drug in a single dosage unit by physical separation. Several advantages over the conventional tablets were reported in literature as listed below:
-
1.
Bilayer tablets are designed to deliver two or more APIs, which can reduce the pill burden thereby improving patient compliance (Bangalore et al. 2007; Bergmann 2008; LaForce et al. 2008).
-
2.
Physicochemical incompatible two APIs can be in one bilayer tablet (Efentakis and Peponaki 2008; Vaithiyalingam and Sayeed 2010).
-
3.
Different release profile requiring APIs can be combined in a single bilayer tablets (Nirmal et al. 2008; Shiyani et al. 2008).
-
4.
Bilayer tablets can be developed to extend the life cycle of drug product (Abebe et al. 2014).
-
5.
Bilayer tablets may enhance the efficacy of APIs due to their synergistic or additive effects (Serebruany et al. 2004).
For example, the bilayer tablet of extended-release metoprolol succinate, a beta-1 (cardio-selective) adrenoceptor-blocking agent, and immediate-release hydrochlorothiazide, a well-established diuretics is more effective than monotherapy with the individual components to lower elevated blood pressure (Hainer et al. 2007). Although bilayer tablet approach is a common, economic and reliable FDC technology, there are some challenges attributed to the mechanical and compression of bilayer tablet for formulation design, manufacturing process, controls and product performance requirements. Some of the key challenges are accuracy in weight control of individual layers (Abebe et al. 2014), delamination at the non-planer interface between the adjacent compacted layers during manufacturing and storage (Abdul and Poddar 2004), insufficient tablet hardness and friability (Abdul and Poddar 2004), cross-contamination between the layers (especially for incompatible APIs) (Akseli et al. 2010), and reduced yield (Abdul and Poddar 2004). To overcome these challenges it is critical to understand the mechanical properties of the materials and bilayer processing parameters for the characterization of bilayer tablets.
Elastic mismatch between the layers in a bilayer tablet caused from the differences of material properties (plasticity and brittleness) in each layer induces delamination. It was reported that the nature of materials played a critical role on the strength of the interface and individual compacts and also on their mode of fracture (Akseli et al. 2010; Kottala et al. 2012b). In general, the decrease of the surface roughness of the first layer increases the propensity of delamination due to the low mechanical interlinkage. Therefore, the compression force for the first layer which can affect the tensile strength of the first layer and surface roughness plays a critical role in delamination (Desai et al. 2013). Since brittle materials in the first layer can produce the large surface area effectively to enhance interlocking the adjacent layers, it is preferable to select brittle materials with higher fragmentation tendency as the first layer (Desai et al. 2013). The lubricant used for reducing the friction between the blends with dies and punches during the compression may affect the interfacial interaction between the adjacent layers. Therefore, the level of lubricant also has to be assessed in formulation and process development for bilayer tablets (Abebe et al. 2014).
There are some benefits of physical integrity evaluation of bilayer tablets in early formulation development such as measurement of the interfacial strength in bilayer tablets, detection of unusual or extreme properties of compacted layers, building rationale strategy to guide formulation and manufacturing processes, understanding the mechanism of material failure and so on (Abebe et al. 2014). Physical integrity including fracture and delamination of bilayer tablets is evaluated by conventional hardness and friability test. X-ray micro-computed tomography is a three-dimensional imaging technique, which can be used as a non-invasive determination of the density of a material, visualization of the delamination and fracture patterns inside the tablets (Akseli et al. 2010). Inman et al. characterized the topographic profiles and quantitative roughness and fracture of surfaces at the interface of the bilayer tablets using non-contact laser profilometry (Inman et al. 2008). As the process analytical technology (PAT) has been developed, terahertz pulsed imaging using interface index (Niwa et al. 2013) and near infrared (NIR) transmittance spectroscopy (Ito et al. 2010) were introduced in determination the interfacial strength of bilayer tablets. Ito et al. demonstrated the control of API contents in two separate layers of intact bilayer tablets using calibration models for nondestructive NIR (Ito et al. 2010).
As aforementioned, bilayer tablet approach is a convenient approach to formulate incompatible drugs or to enable an immediate release loading dose and another sustained release dose in a single dosage unit. In severe incompatible cases, the buffer layer can be inserted between the two layers to prevent direct contact of two APIs. To prevent the chemical reactions between aspirin and pravastatin which is unstable under acidic condition, an alkaline buffering layer can be added between each drug layer (Desai et al. 2013). Since the drug release profiles in a layer can be affected by the API or excipients in the other layer by changing the microenvironment, the impact of another drug’s in vitro dissolution profile should be evaluated.
In general, similar level of formulation in each layer is preferred to mitigate the challenges in bilayer tablet development. Composition similarity of the two layers subsequently lead to similarities of the physical and mechanical properties of the granular/powder materials for tablet compression and swelling capacity may lead to layer separation at the interface under highly humid condition. Practically, the layer ratio is 1:1 or 1:2 weight ratio between the two layers. Although a layer ratio of up to 1:6 can be encountered in bilayer tablet formulation, it will be a greater challenge to maintain the consistency as the disproportionate ratio increases (Kottala et al. 2012a). To assure the content uniformity of the APIs in bilayer tablets, the weight in each layer has to be controlled with accuracy. Commercially-available bilayer tablet machines provide their own weight control system to monitor the first layer weight and the second bilayer weight.
Multiparticulate systems
Most multiparticulate systems for FDC contain pellets prepared by extrusion/spheronization or layering the drug solution or suspension onto sugar pellets and/or granules compressed into tablets or encapsulated into capsules. The pellets processed by extrusion/spheronization give some advantages in process development such as narrow particle size distribution of the pellets with low friability (Desai et al. 2013). Coated pellets are commonly applied in oral modified release. Pellets loaded with different drugs as FDC can be combined in a single dosage form, which allows each drug to achieve desirable drug release profile irrelevant to drug compatibility. In addition, the pellets can be applied to improve stability for chemically unstable and moisture sensitive drugs such as dipeptidyl peptidase IV (DPP-IV) inhibitors by coating with various seal coats and moisture barriers (Burke et al. 2013).
Multiparticulates offer therapeutic advantages over single-unit dosage form such as capsules or tablets; the pellets are distributed evenly throughout the gastrointestinal tract, thereby reducing the risk of toxicity caused by high local drug concentration and improving BA with low inter- or intra-individual variations (Zeeshan and Bukhari 2010). Furthermore, drug release profiles can be easily modified by simply mixing pellets with different release characteristics. For the treatment of drug–resistant tuberculosis, FDC of tablet is recommended. A first-line anti-tubercular drug, rifampicin is easily degraded in the presence of isoniazid and interacts with other drugs. The formulation of pellet form for each API in FDCs can eliminate the drug interaction and drug degradation (Sapte 2004). However, there are some challenges with compression of coated pellets including rupturing of coated film for controlled-release characteristics particularly for water-soluble drugs, thereby to date, only a few pellet- containing tablet products are commercially available (Dashevsky et al. 2004). Highly compressible microcrystalline cellulose, Ceolus KG-801, is one of the suitable compression excipients to protect coated pellets containing a freely water-soluble drug during the compression (Zeeshan et al. 2009). The technical complexities of unique pellet manufacturing equipment and process including palletization by extrusion-spheronization are still major challenges to application of multiparticulates for commercialization (McConnell et al. 2009).
Active film-coating approach
Tablet coating is a common drug manufacturing process for protection for the tablet core or modification of drug release. Active film-coating, API integration into the coating layer, enables the development of FDCs which maintain two different drug release profiles with minimizing chemical interactions of an extended release dose in the tablet core and an immediate release dose in the coating layer (Rege et al. 2002). Environment-sensitive drugs such as compression sensitive drugs or acid-/base-labile drugs can be protected by incorporating into active coating layer in FDC formulation. Relatively high drug to excipient ratio in the film coat of non-reactive coating material improves the its chemical stability (Desai et al. 2012). In addition, active coated tablets are easy-to-swallow with reduced dosage size comparable to bilayer tablets. Furthermore, active film coating technology allows the effective delivery platform for disproportionate FDC containing a low-dose API and a high-dose API (e.g. 2 mg of glimepiride-coated 500 mg of metformin extended-release tablet) without other specialized equipment or process in palletization (Kim et al. 2012).
The major challenges for active film coating are end-point determination, content uniformity, efficiency, and stability which are affected by process parameters and drug properties. The end point of the coating process is estimated by the gain in tablet weight or quantity of coating suspension sprayed. During the coating process, weight gain and the amount of API deposited are periodically determined in tablet samples. Kim et al. suggested NIR spectroscopy as an analytical tool for determining the end-point (Kim et al. 2012). The coating uniformity can be divided into the intra-tablet coating uniformity and the inter-tablet coating uniformity (Tobiska and Kleinebudde 2003). The intra-tablet coating uniformity can be characterized by terahertz pulsed imaging (TPI) which can provide the information on tablet film coating layer thickness and variations in coating density as an analytical tool for monitoring a film coating unit operation (Ho et al. 2009). Optical coherence tomography (OCT), a non-invasive analysis technique allowing fast and high-quality cross-sectional imaging of scattering media, can also applied for the characterization of coating by providing the information of layer thickness and homogeneity, tablet weight gain and tablet diameters (Koller et al. 2011). The inter-tablet coating uniformity can be determined by TPI, mass uniformity, content uniformity or computational simulation tools like the discrete element method (DEM) (Just et al. 2013).
Hot-melt co-extrusion approach
Hot-melt extrusion (HME) is a technology to reduce polymer viscosities at higher temperature and increasing its surface area, thereby improving compression characteristics of the homogeneous granules containing drug and polymer. It offers unique advantages over conventional pharmaceutical technologies such as continuous manufacturing process with fewer processing steps, cost-effectiveness, ease of processing scale-up, good content uniformity, decreased environmental implications and the possibility of improving drug solubility (Tiwari et al. 2016). HME technology is particularly suitable for high drug-loading formulation, thus, beneficial for FDC formulation.
Hot-melt co-extrusion is a technology to produce a multi-layered extrudate by extruding simultaneous hot-melt of two or more materials through the same die (Quintavalle et al. 2008). Although it is only applied to prepare implants and vaginal rings and has not been used for market oral products yet, co-extrusion technology in FDC offers the similar advantages to bilayer tablet technology such as combination of different release profile-requiring APIs or of simultaneous administration of non-compatible drugs (Dierickx et al. 2013). The combination of available polymers in terms of extrusion temperature and dissolution rate enables to obtain the desired drug release profile in each layer. However, selecting polymer combinations is a big challenge in formulation as technical requirement should be satisfied such as similar extrusion temperature, melt viscosity, adhesion between layers, and prevention of interfacial interaction and delamination (Vynckier et al. 2014b). In addition, it requires specific equipments such as extruders and specific dies, and complex simultaneous extrusion process which should be carefully controlled. The thermal behavior and crystallinity of the individual APIs, physical mixtures and co-extrudate can be evaluated by differential scanning calorimetry (DSC). The distribution of the different components in the coat and core of the co-extrudates was evaluated with Raman microscopic mapping (Dierickx et al. 2014; Vynckier et al. 2014a).
Performance evaluation of FDC drug products
Characterization of FDC drug products
The drugs in FDCs are selected based on PK profiles and manufacturability as well as clinical unmet needs. Various formulation designs for FDC have been suggested. In addition to the clinical performance, the physicochemical integrity of the FDC should be demonstrated. In bilayer/multilayer tablet formulations, several physicochemical problems which can significantly impact the quality and efficacy of the product including layer separation, insufficient hardness, inaccurate individual layer weight control, and cross-contamination between the layers should be evaluated (Choi and Jeong 2011). Layer separation commonly occurs during the compression or the dissolution process due to the insufficient bonding between the adjacent layers during the tablet compression. The radial lamination of the tablet with the butterfly-shaped hydrated matrix developed under the influence of swelling pressure and the differential extent of hydration in bilayer tablet may affect the undesirable release properties of the hydrophilic matrix tablet (Cahyadi et al. 2011).
Physicomechanical properties in FDCs can be evaluated by various analytical instruments: Interfacial topography is determined by optical microscopy, scanning electrical microscopy (SEM), laser profilometry, and stylus based perthometer. Molecular dispersion of the drug in carriers can be detected by DSC and X-ray diffraction (XRD) (Dierickx et al. 2014). In addition to technical challenges in FDC formulations, new impurities generated by chemical interaction between combined APIs in one formulation have to be considered. Therefore, the stability issue is critical in development of FDCs. The instability of combination drugs is categorized into three groups: physical instability such as color change, precipitation, and hardness; chemical instability such as variation in drug content and impurities; and functional instability such as changes in the drug release pattern. Generated new impurities should be qualified to be safe in accordance with the ICH guideline Q3A. The approval of Truvada, an FDC product containing tenofovir and emtricitabine, developed by Gilead had been refused by FDA due to failure of providing sufficient information on the analytical methodology to establish acceptable levels of recently identified degradants related to emtricitabine (Caspi 2011).
PK studies in FDC drug products
During the development of FDC formulations, in vitro dissolution studies are performed routinely to test product performance for quality control and to understand the critical parameters affecting drug biopharmaceutics (Dokoumetzidis and Macheras 2006). However, the compendial dissolution methodologies do not always have sufficient predictability for in vivo performance including PK properties as per the formulation change. Therefore, it is necessary to the development of discriminating dissolution method using new biorelevant dissolution systems with physiologically relevant conditions (Panchagnula et al. 2006). The development of FDC dissolution method is more challenging than that of single dosage units due to the different release mechanisms or significant difference in dose or physicochemical properties of the APIs. The PK profiles and in vitro–in vivo correlation (IVIVC) can be estimated by in silico tools based on the advanced compartmental absorption and transit model to reduce the cost and time in development of FDC drugs by providing viable formulation options that are intended to improve oral BA (Heikkinen et al. 2012; Honorio Tda et al. 2013; Kuentz 2008). Once discriminating dissolution method and IVIVC are established, formulation can be corrected to alter the in vitro drug release that would result into the desired PK profiles (Dubey 2012). Prior to human clinical study, preclinical in vivo studies are performed in animals, usually using dogs. As there may be significant differences among human and the animal models in GI physiology and the fraction of dose absorbed (Chiou et al. 2000; Kararli 1995), there are limitations to predict formulation performance in human based on preclinical animal data.
Since the synergistic effects in FDCs is hard to be determined, the BE comparison between drugs in FDC and drugs co-administered as each single dosage form is a typical clinical approach for FDC development (Desai et al. 2013). It is of note that in vivo disposition of the APIs in FDC products can be changed, when administered together. If there are PK interactions between the APIs, possible impact of such interaction on clinical performance has to be investigated carefully (Dubey 2012). Since limited dose strengths of FDC products are available, it is of importance to determine the number and dose strength combinations in FDC development. In general, the number of FDC dose strengths to be developed depends on the medical rationale and/or the number of doses available for each API. During the FDC formulation development, PK profile of co-administering two individual single entity tablets can be evaluated for BE references for the comparison of optimized FDC formulation. Food effects on the APIs in the FDC may be changed. The evaluation of the effect of food on the absorption of the APIs in FDC is also recommended by the EMA (EMA, 2006). Food can affect oral drug absorption by physiological changes of gastric pH, GI motility, and presystemic metabolism, thereby changing bioavailability. For example, metformin dosed after the meal for better GI tolerance, is recommended to be administered with meals in FDC formulations. Moreover, this bioavailability change is more complicated by the influence of physicochemical properties of APIs. The oral absorption of poorly water soluble BCS Class II drugs is generally enhanced in fed state (Mitra and Wu 2012). Typically food effect bioavailability studies are designed as an open label, 2-way, crossover study between fed and fasting conditions.
BE in FDC drug products
For approval of a FDC product, BE study designed as randomized, single-dose, two-way crossover in which one arm receives the FDC, and the other arm receives the same dose of the APIs, with an adequate washout (generally at least five half-lives of the API with the longest half-life in duration) between treatments is generally used. The BE between sitagliptin/metformin FDC tablets (Janumet®) and co-administration of corresponding doses of mono-product was demonstrated in this approach (Migoya et al. 2010). However, achieving BE can be very challenging since the predicted biopharmaceutical and PK behaviors could be changed due to combining multiple APIs and excipients in a single drug product such as drug–drug interaction or formulation interaction. One API can upregulate or down regulate the metabolic enzyme for the other API, thereby changing their PK parameters. Excipients in FDC formulation may lead to drug degradation under in vivo condition. If the properties of individual reference drugs are different, i.e. reference drugs are an immediate release BCS Class II API and the other extended release BCS Class II API or a tablet and the other capsule containing micronized drug, the more sophisticated formulation design is required to achieve BE (Dubey 2012).
Prior to pivotal BE studies, pilot BA studies can be performed to screen prototype FDC formulation and to understand the oral BA of APIs of the FDC product. The pilot BA study is generally designed as open-label, single dose, crossover in fasted healthy subjects of which size is smaller than pivotal BE studies. The prototype formulation of which PK parameters is similar to those of the reference treatment can be generally considered for scale-up and be performed pivotal PK study. In typical FDC development, BE is achieved if the confidence interval (CI) of ratio (test product:reference product) of geometric mean of log-transformed Cmax as well as AUC for each API in FDC and the respective reference listed drugs using two way one-sided analysis of variance (ANOVA) are within the 80 to 125% boundaries (FDA 2006). Replicate study designs are recommended in case of highly variable drugs with the within-subject variability of 30%. In spite of their high intra-subject variability, highly variable drugs generally have a wide therapeutic window. Therefore, adjustment of the conventional BE criteria for these drugs and products may be required to reduce the number of subject in BE trials. FDA proposed the BE study with three-period, reference-replicated, crossover design with sequences of test/reference/reference (TRR), RTR, and RRT (Haidar et al. 2008).
The number of BE studies for the registration of FDC product consisting of multiple dose strengths should be determined. In case the APIs show dose-PK linearity across the dose ranges tested and material attributes such as the ratio among API and excipients, the manufacturing process and equipment are similar across all dose ranges, limited number of BE studies with the highest dose strengths and demonstration of the similarity of in vitro dissolution profiles can be enough to register all dose strengths. For example, BE studies in a randomized, open label, two way cross over study design at the highest (10/80 mg; n = 62) and lowest (5/10 mg; n = 64) dose strengths for amlodipine/atorvastatin FDC were applied for the registration of 11 different dose proportions including 2.5/10, 2.5/20, 2.5/40, 5/10, 5/20, 5/40, 5/80, 10/10, 10/20, 10/40, and 10/80 mg (Chung et al. 2006).
Clinical studies in FDC drug products
Although there are no harmonized clinical development guidance for FDCs, completion of the full phases of clinical trials was not always required for approval by the FDA (Kwon and Lee 2016). According to the guideline for clinical development of FDCs by EMA, for the FDC approval applicants should demonstrate the combination of APIs enhances the benefit/risk by improving efficacy and/or safety, compared to the use of single API (EMA 2006). The FDA suggested required data and information to demonstrate the contribution of each API to the effect of a combination in recent published proposed rule, which are summarized in Table 3 (FDA 2015). According to this proposed rule, FDCs in which the APIs are directed at the same sign, symptom or condition should demonstrated positive risk–benefit greater than the use of single API at its therapeutic dose. To support the additive or synergic pharmacological effects of the FDCs over the use of individual APIs, a factorial design study is generally applied. The efficacy and tolerability of the combination of an ARB (e.g. olmesartan medoxomil) with a CCB (e.g. amlodipine besylate) in fully additive blood pressure reduction can be demonstrated by a randomized, double-blind, placebo-controlled, factorial study (Chrysant et al. 2008; Gradman et al. 2010). In case of combinations in which one API is intended to provide a direct effect to improve the efficacy or safety of another API by making more tolerable another API, or minimizing an adverse effect or abuse potential associated with another API, clinical trial should demonstrate improved safety or effectiveness of the FDC over the single use of disease- active ingredient. FDCs of cobicistat, a booster of CYP3A, and protease inhibitors have been investigated with FDCs of ritonavir-boosted protease inhibitor (Marzolini et al. 2016; Shah et al. 2013). The combination in which each API is directed at different signs or symptoms of a disease or condition may not need the factorial study if an API does not affect the safety or effectiveness of another API. Instead the individual effectiveness of API and no interference with each other should be demonstrated. With the clinical supportive data, the BE also should be suggested. However, if all clinical data support the rationale of FDCs, the BE study may be waived (EMA 2015).
Conclusions and future perspectives
Combination drug therapies have become prevalent for the prevention and treatment of chronic and complex diseases, and their necessity and usefulness would be increasingly continued with advances in pathophysiological, pharmacological and pharmacogenomic approaches as well as existence of unmet medical needs. The regulatory authorities already recognize the therapeutic potential of rational combination therapies and encourage the development of combination products effective for serious diseases (EMA 2015; WHO 2005; Woodcock et al. 2011). In reality, there is still a lot of room for the needs of combination therapies providing improved efficacy, safety and patient compliance in the management of multiple dreadful and refractory diseases. Current trend of great increase in elderly patient population who in most cases need long-term concurrent therapies may be a great driving force for the more active development of potential FDC drug products. These current status and prospects could bring more opportunities to develop new oral FDC products for better systematic disease management from numerous combination possibilities over different drug classes, which can give an alignment with promising strategies for lifecycle extension of established single drugs in pharmaceutical industry.
In spite of the continuous use of FDC products for better pharmacotherapies, they often produce no intended therapeutic improvement or their benefits cannot often be understood. In the development of FDC products, the rationale for drug combination should be established based on valid therapeutic principles and proven by clinical outcomes (FDA 2015; Orloff 2005). The selection and screening of new drug combinations can be based on predictions from both action mechanisms and targets of the active components as well as their PK behaviors (Pourkavoos 2012; Foucquier and Guedj 2015). However, the mechanisms and principles that underlie therapeutic benefits of drug combinations are still elusive (Liu et al. 2014). Notable progresses of computational prediction and high-throughput screening methodologies using target network analysis and genomics/bioinformatics systems have contributed to reliable screening and prediction of effective drug combinations (Chou 2010; Foucquier and Guedj 2015; Huang et al. 2014; Park et al. 2013; Pritchard et al. 2013). Physiologically based absorption and PK modeling and simulations have become a creditable tool for screening of potential drug combinations and development of combination formulations by providing quantitative assessment on PK interactions and IVIVC of FDC products and the active components (Min et al. 2016; Mitra and Wu 2012; Sperry et al. 2010). To improve the development process for FDC products, it is important to establish clear strategies for both formulation development and performance evaluation (Mitra and Wu 2012). The dosage form design, formulation and process development, and performance testing for prospective oral FDC products should be performed using appropriate strategies for addressing the defined dose ratios and strengths of active components, their drug–drug and drug–excipients compatibility, a dosing regimen unified with their separate drug release and PK profiles, their efficacious PD and PK interactions, patient-acceptable volume of dosage form and their long-term stability thorough consideration of their physicochemical properties, and using combination formulation and drug delivery technologies eligible for all of the strategies. With the continuous growth of oral FDC products, innovative formulation approaches and technologies need to be invented to optimally develop the FDC formulations suitable for a variety of novel drug combinations to be proposed through new therapeutic insights.
References
Abdul S, Poddar SS (2004) A flexible technology for modified release of drugs: multi layered tablets. J Control Release 97:393–405
Abebe A, Akseli I, Sprockel O, Kottala N, Cuitino AM (2014) Review of bilayer tablet technology. Int J Pharm 461:549–558
Akseli I, Dey D, Cetinkaya C (2010) Mechanical property characterization of bilayered tablets using nondestructive air-coupled acoustics. AAPS PharmSciTech 11:90–102
Bangalore S, Kamalakkannan G, Parkar S, Messerli FH (2007) Fixed-dose combinations improve medication compliance: a meta-analysis. Am J Med 120:713–719
Bergmann JF (2008) Review: fixed-dose drug combinations improve medication compliance compared with free-drug regimens. Evid.-Based Med 13:18
Borghi C, Cicero AFG (2010) Rationale for the use of a fixed-dose combination in the management of hypertension. Clin Drug Investig 30:843–854
Burke MD, He X, Cook C, Petrov GA, Long S, Coffin MD (2013) Stability enhancement of drug layered pellets in a fixed dose combination tablet. AAPS PharmSciTech 14:312–320
Cahyadi C, Chan L, Colombo P, Heng P (2011) The butterfly effect: a physical phenomenon of hypromellose matrices during dissolution and the factors affecting its occurrence. Int J Pharm 406:31–40
Caspi A (2011) Clinical trials, research, and FDA findings. Biotechnol Healthc 8:10–11
Chiou WL, Jeong HY, Chung SM, Wu TC (2000) Evaluation of using dog as an animal model to study the fraction of oral dose absorbed of 43 drugs in humans. Pharm Res 17:135–140
Choi D-H, Jeong S-H (2011) Multi-layered matrix tablets with various tablet designs and release profiles. J Pharm Investig 41:263–272
Chou TC (2010) Drug combination studies and their synergy quantification using the Chou-Talalay method. Cancer Res 70:440–446
Chrysant SG, Melino M, Karki S, Lee J, Heyrman R (2008) The combination of olmesartan medoxomil and amlodipine besylate in controlling high blood pressure: COACH, a randomized, double-blind, placebo-controlled, 8-week factorial efficacy and safety study. Clin Ther 30:587–604
Chung M, Calcagni A, Glue P, Bramson C (2006) Bioavailability of amlodipine besylate/atorvastatin calcium combination tablet. J Clin Pharmacol 46:1030–1037
Dashevsky A, Kolter K, Bodmeier R (2004) Compression of pellets coated with various aqueous polymer dispersions. Int J Pharm 279:19–26
Desai D, Rao V, Guo H, Li D, Stein D, Hu FY, Kiesnowski C (2012) An active film-coating approach to enhance chemical stability of a potent drug molecule. Pharm Dev Technol 17:227–235
Desai D, Wang J, Wen H, Li X, Timmins P (2013) Formulation design, challenges, and development considerations for fixed dose combination (FDC) of oral solid dosage forms. Pharm Dev Technol 18:1265–1276
Dierickx L, Remon JP, Vervaet C (2013) Co-extrusion as manufacturing technique for multilayer mini-matrices with dual drug release. Eur J Pharm Biopharm 85:1157–1163
Dierickx L, Van Snick B, Monteyne T, De Beer T, Remon JP, Vervaet C (2014) Co-extruded solid solutions as immediate release fixed-dose combinations. Eur J Pharm Biopharm 88:502–509
Dokoumetzidis A, Macheras P (2006) A century of dissolution research: from Noyes and Whitney to the biopharmaceutics classification system. Int J Pharm 321:1–11
Dubey R (2012) Bioequivalence challenges in development of fixed-dose combination products: looking beyond reformulation. Expert Opin Drug Deliv 9:325–332
Efentakis M, Peponaki C (2008) Formulation study and evaluation of matrix and three-layer tablet sustained drug delivery systems based on Carbopols with isosorbite mononitrate. AAPS PharmSciTech 9:917–923
EMA (2006) Guideline on pharmaceutical fixed combination products. European Medicines Agency, London
EMA (2015) Guideline on clinical development of fixed combination medicinal products. European Medicines Agency, London
Farnier M (2011) Safety review of combination drugs for hyperdemia. Expert Opin Drug Saf 10:363–371
FDA (2006) Guidance for industry fixed dose combinations, co-packaged drug products, and single entity versions of previously approved antiretrovirals for the treatment of HIV. Food and Drug Administration (FDA), Rockville
FDA (2015) Fixed-combination and co-packaged drugs: applications for approval and combinations of active ingredients under consideration for inclusion in an over-the-counter monograph. Proposed rule, Federal Register, 12/23/2015
Foucquier J, Guedj M (2015) Analysis of drug combinations: current methodological landscape. Pharmacol Res Perspect 3(e00149):1–11
Gautam CS, Saha L (2008) Fixed dose drug combinations (FDCs): rational or irrational: a view point. Br J Clin Pharmacol 65:795–796
Gradman AH, Basile JN, Carter BL, Bakris GL, Group ASoHW (2010) Combination therapy in hypertension. J Am Soc Hypertens 4:42–50
Haidar SH, Davit B, Chen M-L, Conner D, Lee L, Li QH, Lionberger R, Makhlouf F, Patel D, Schuirmann DJ (2008) Bioequivalence approaches for highly variable drugs and drug products. Pharm Res 25:237–241
Hainer JW, Sugg J, Vasc J (2007) Metoprolol succinate extended release/hydrochlorothiazide combination tablets. Vasc Health Risk Manag 3:279–288
Heikkinen AT, Baneyx G, Caruso A, Parrott N (2012) Application of PBPK modeling to predict human intestinal metabolism of CYP3A substrates—an evaluation and case study using GastroPlus. Eur J Pharm Sci 47:375–386
Hiremath PS, Bhonsle SA, Thumma S, Vemulapalli V (2011) Recent patents on oral combination drug delivery and formulations. Recent Pat Drug Deliv Formul 5:52–60
Ho L, Muller R, Gordon KC, Kleinebudde P, Pepper M, Rades T, Shen Y, Taday PF, Zeitler JA (2009) Terahertz pulsed imaging as an analytical tool for sustained-release tablet film coating. Eur J Pharm Biopharm 71:117–123
Honorio Tda S, Pinto EC, Rocha HV, Esteves VS, dos Santos TC, Castro HC, Rodrigues CR, de Sousa VP, Cabral LM (2013) In vitro-in vivo correlation of efavirenz tablets using GastroPlus(R). AAPS PharmSciTech 14:1244–1254
Huang L, Li F, Sheng J et al (2014) DrugComboRanker: drug combination discovery based on target network analysis. Bioinformatics 30:i228–i236
Inman SJ, Briscoe BJ, Pitt KG, Shiu C (2008) Axial tensile fracture of microcrystalline cellulose compacts. Int J Pharm 349:172–179
Ito M, Suzuki T, Yada S, Nakagami H, Teramoto H, Yonemochi E, Terada K (2010) Development of a method for nondestructive NIR transmittance spectroscopic analysis of acetaminophen and caffeine anhydrate in intact bilayer tablets. J Pharm Biomed Anal 53:396–402
Jia J, Zhu F, Ma X, Cao ZW, Li YX, Chen YZ (2009) Mechanisms of drug combinations: interaction and network perspectives. Nat Rev Drug Discov 8:111–128
Just S, Toschkoff G, Funke A, Djuric D, Scharrer G, Khinast J, Knop K, Kleinebudde P (2013) Optimization of the inter-tablet coating uniformity for an active coating process at lab and pilot scale. Int J Pharm 457:1–8
Kararli TT (1995) Comparison of the gastrointestinal anatomy, physiology, and biochemistry of humans and commonly used laboratory animals. Biopharm Drug Dispos 16:351–380
Kararli TT, Sedo K, Bossart J (2014a) Fixed-dose combination products-A review (Part 1-introduction). Drug Dev Deliv 14(2):32–35
Kararli TT, Sedo K, Bossart J (2014b) Fixed-dose combination products-A review (Part 2-analysis). Drug Dev Deliv 14(3):28–32
Kararli TT, Sedo K, Bossart J (2014c) Fixed-dose combination products-A review (Part 3-pipeline). Drug Dev Deliv 14(4):36–39
Karim MN, Ahmed KR, Bukht MS, Akter J, Chowdhury HA, Hossain S, Anwar N, Selim S, Chowdhury SH, Hossain F, Ali L (2013) Pattern and predictors of dyslipidemia in patients with type 2 diabetes mellitus. Diabetes Metab Syndr Clin Res Rev 7(2):95–100
Kim JY, Kim DW, Kuk YM, Park CW, Rhee YS, Oh TO, Weon KY, Park ES (2012) Investigation of an active film coating to prepare new fixed-dose combination tablets for treatment of diabetes. Int J Pharm 427:201–208
Koller DM, Hannesschlager G, Leitner M, Khinast JG (2011) Non-destructive analysis of tablet coatings with optical coherence tomography. Eur J Pharm Sci 44:142–148
Kottala N, Abebe A, Sprockel O, Akseli I, Nikfar F, Cuitino AM (2012a) Influence of compaction properties and interfacial topography on the performance of bilayer tablets. Int J Pharm 436:171–178
Kottala N, Abebe A, Sprockel O, Bergum J, Nikfar F, Cuitino AM (2012b) Evaluation of the performance characteristics of bilayer tablets: Part I. Impact of material properties and process parameters on the strength of bilayer tablets. AAPS PharmSciTech 13:1236–1242
Kuentz M (2008) Drug absorption modeling as a tool to define the strategy in clinical formulation development. AAPS J 10:473–479
Kumar V, Prasad B, Singh S (2008) Pharmaceutical issues in the development of a polypill for the treatment of cardiovascular diseases. Drug Discov Today Ther Strateg 5:63–71
Kwon KC, Lee C (2016) Analysis of fixed-dose combination products approved by the US food and drug administration, 2010-2015 implications for designing a regulatory shortcut to new drug application. Ther Innov Regul Sci 2168479016663263
LaForce C, Gentile DA, Skoner DP (2008) A randomized, double-blind, parallel-group, multicenter, placebo-controlled study of the safety and efficacy of extended-release guaifenesin/pseudoephedrine hydrochloride for symptom relief as an adjunctive therapy to antibiotic treatment of acute respiratory infections. Postgrad Med 120:53–59
Lai GH, Zhang Z, Sirica AE (2003) Celecoxib acts in a cyclooxygenase-2-independent manner and in synergy with emodin to suppress rat cholangiocarcinoma growth in vitro through a mechanism involving enhanced akt inactivation and increased activation of caspases-9 and -3. Mol Cancer Ther 2:265–271
Liu Y, Wei Q, Yu G, Gai W, Li Y, Chen X (2014) DCDB 2.0: a major update of the drug combination database. Database bau124:1–6
Mandal U, Pal TK (2008) Formulation and in vitro studies of a fixed-dose combination of a bilayer matrix tablet containing metformin HCl as sustained release and glipizide as immediate release. Drug Dev Ind Pharm 34:305–313
Marzolini C, Gibbons S, Khoo S, Back D (2016) Cobicistat versus ritonavir boosting and differences in the drug–drug interaction profiles with co-medications. J Antimicrob Chemother 71:1755–1758
McConnell EL, Macfarlane CB, Basit AW (2009) An observational study on the influence of solvent composition on the architecture of drug-layered pellets. Int J Pharm 380:67–71
Migoya EM, Miller JL, Gutierrez M, Zheng W, Johnson-Levonas AO, Liu Q, Matthews CZ, Wagner JA, Gottesdiener KM (2010) Bioequivalence of sitagliptin/metformin fixed-dose combination tablets and concomitant administration of sitagliptin and metformin in healthy adult subjects. Clin Drug Investig 30:855–866
Min JS, Kim D, Park JB et al (2016) Application of physiologically based pharmacokinetic modeling in predicting drug–drug interactions for sarpogrelate hydrochloride in humans. Drug Des Dev Ther 10:2959–2972
Mitra A, Wu Y (2012) Challenges and opportunities in achieving bioequivalence for fixed-dose combination products. AAPS J 14:646–655
Nakatani M, Yokoyama K, Sawada T (2014) Bilayer tablet comprising telmisartan and diuretic. US Patents. 8637078
Newman J, Grobman WA, Greenland P (2008) Disease prevention in men: a decision analysis and cost-effectiveness model. Prev Cardiol 11:36–412
Nirmal J, Saisivam S, Peddanna C, Muralidharan S, Godwinkumar S, Nagarajan M (2008) Bilayer tablets of atorvastatin calcium and nicotinic acid: formulation and evaluation. Chem Pharm Bull 56:1455–1458
Niwa M, Hiraishi Y, Iwasaki N, Terada K (2013) Quantitative analysis of the layer separation risk in bilayer tablets using terahertz pulsed imaging. Int J Pharm 452:249–256
Orloff DG (2005) Fixed combination drugs for cardiovascular disease risk reduction: regulatory approach. Am J Cardiol 96:28K–33K
Pan F, Chernew ME, Fendrick AM (2008) Impact of fixed-dose combination drugs on adherence to prescription medications. J Gen Intern Med 23:611–614
Panchagnula R, Kumar Bajpai A, Agrawal S, Ashokraj Y (2006) Dissolution testing of marketed rifampicin containing fixed dose combination formulations using a new discriminative media: a post marketing retrospective study. Pharmazie 61:851–854
Park J, Lee S, Kim K, Lee D (2013) Systematic approach for analyzing drug combination by using target-enzyme distance. IBC 5(3):1–7
Park HS, Han JH, Jung SH, Jo EJ, Myung CS (2016a) The combination of valsartan and ramipril protects against blood vessel injury and lowers blood pressure. J Pharm Investig 46:265–272
Park JS, Shin JH, Hong TJ et al (2016b) Efficacy and safety of fixed-dose combination therapy with olmesartan medoxomil and rosuvastatin in Korean patients with mild to moderate hypertension and dyslipidemia: an 8-week, multicenter, randomized, double-blind, factorial-design study (OLSTA-D RCT: OLmesartan rosuvaSTAtin from Daewoong). Drug Des Dev Ther 10:2599–2609
Pourkavoos N (2012) Unique risks, benefits, and challenges of developing drug–drug combination products in a pharmaceutical industrial setting. Comb Prod Ther 2:2–31
Pritchard JR, Bruno PM, Gilbert LA et al (2013) Defining principles of combination drug mechanisms of action. Proc Natl Acad Sci USA 110:E170–E179
Putcharoen O, Do T, Avihingsanon A, Ruxrungtham K (2015) Rationale and clinical utility of the darunavir–cobicistat combination in the treatment of HIV/AIDS. Drug Des Devel Ther 9:5763–5769
Quintavalle U, Voinovich D, Perissutti B, Serdoz F, Grassi G, Dal Col A, Grassi M (2008) Preparation of sustained release co-extrudates by hot-melt extrusion and mathematical modelling of in vitro/in vivo drug release profiles. Eur J Pharm Sci 33:282–293
Rege BD, Gawel J, Kou JH (2002) Identification of critical process variables for coating actives onto tablets via statistically designed experiments. Int J Pharm 237:87–94
Rosenthal T, Gavras I (2006) Fixed-drug combinations as first-line treatment for hypertension. Prog Cardiovasc Dis 48:416–425
Sanz G, Fuster V (2009) Fixed-dose combination therapy and secondarycardiovascular prevention: rationale, selection of drugs and target population. Nat Rev Cardiol 6:101–110. doi:10.1038/ncpcardio1435
Sapte V (2004) Stabilized short-course chemotherapy (SCC) anti-tuberculosis drug compositions. US Patents 200502498
Serebruany VL, Malinin AI, Sane DC, Jilma B, Takserman A, Atar D, Hennekens CH (2004) Magnitude and time course of platelet inhibition with Aggrenox and Aspirin in patients after ischemic stroke: the AGgrenox versus Aspirin Therapy Evaluation (AGATE) trial. Eur J Pharmacol 499:315–324
Shah BM, Schafer JJ, Priano J, Squires KE (2013) Cobicistat: a new boost for the treatment of human immunodeficiency virus infection. Pharmacotherapy 33:1107–1116
Shiyani B, Gattani S, Surana S (2008) Formulation and evaluation of bi-layer tablet of metoclopramide hydrochloride and ibuprofen. AAPS PharmSciTech 9:818–827
Sica DA (2002) Rationale for fixed-dose combinations in the treatment of hypertension. Drugs 62:443–462
Siew A (2015) Fixed-dose combinations. Pharm Technol 39(4):36–39
Sperry DC, Thomas SJ, Lobo E (2010) Dissolution modeling of bead formulations and predictions of bioequivalence for a highly soluble, highly permeable drug. Mol Pharm 7:1450–1457
The HPS2-THRIVE Collaborative Group (2014) Effects of extended-release niacin with laropiprant in high-risk patients. N Engl J Med 371:203–212
Tiwari RV, Patil H, Repka MA (2016) Contribution of hot-melt extrusion technology to advance drug delivery in the 21st century. Expert Opin Drug Deliv 13:451–464
Tobiska S, Kleinebudde P (2003) Coating uniformity and coating efficiency in a Bohle Lab-Coater using oval tablets. Eur J Pharm Biopharm 56:3–9
Vaithiyalingam SR, Sayeed VA (2010) Critical factors in manufacturing multi-layer tablets–assessing material attributes, in-process controls, manufacturing process and product performance. Int J Pharm 398:9–13
Vynckier AK, Dierickx L, Saerens L, Voorspoels J, Gonnissen Y, De Beer T, Vervaet C, Remon JP (2014a) Hot-melt co-extrusion for the production of fixed-dose combination products with a controlled release ethylcellulose matrix core. Int J Pharm 464:65–74
Vynckier AK, Dierickx L, Voorspoels J, Gonnissen Y, Remon JP, Vervaet C (2014b) Hot-melt co-extrusion: requirements, challenges and opportunities for pharmaceutical applications. J Pharm Pharmacol 66:167–179
Wald DS, Law M, Morris JK, Bestwick JP, Wald NJ (2009) Combination therapy versus monotherapy in reducing blood pressure: meta-analysis on 11,000 participants from 42 trials. Am J Med 122:290–300
WHO (2003) WHO drug information 17(3):143–227
WHO (2005) WHO expert committee on specifications for pharmaceutical preparations. WHO Tech Rep Ser No. 929
Woodcock J, Griffin JP, Behrman RE (2011) Development of novel combination therapies. N Engl J Med 364:985–987
Zeeshan F, Bukhari NI (2010) Development and evaluation of a novel modified-release pellet-based tablet system for the delivery of loratadine and pseudoephedrine hydrochloride as model drugs. AAPS PharmSciTech 11:910–916
Zeeshan F, Peh KK, Tan YT (2009) Exploring the potential of a highly compressible microcrystalline cellulose as novel tabletting excipient in the compaction of extended-release coated pellets containing an extremely water-soluble model drug. AAPS PharmSciTech 10:850–857
Zhao S, Nishimura T, Chen Y et al (2013) Systems pharmacology of adverse event mitigation by drug combinations. Sci Transl Med 5:206ra140
Acknowledgements
This research was supported by the Bio & Medical Technology Development Program of the National Research Foundation funded by the Ministry of Science, ICT & Future Planning (2013M3A9B5075840) and in part by Sunchon National University Research Fund in 2015.
Conflict of interest
All authors (C. Moon and E. Oh) declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Moon, C., Oh, E. Rationale and strategies for formulation development of oral fixed dose combination drug products. Journal of Pharmaceutical Investigation 46, 615–631 (2016). https://doi.org/10.1007/s40005-016-0286-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40005-016-0286-4