
Abstract
Purpose
Data on the systemic dissemination in Staphylococcus aureus bloodstream infection (SAB) remain sparse. We investigated the timing and the sequence of clinical symptoms, diagnostic confirmation, and occurrence of multiple infective foci in relation to three major infective foci.
Methods
From 2006 to 2011, all adult patients with first-time SAB in Cologne and Freiburg, Germany were followed prospectively. The study was restricted to patients with short-term central venous catheter (CVC)-related SAB, vertebral osteomyelitis (VO), and infective endocarditis (IE). The collection date of the first positive blood culture was used as reference point for determining time to onset of clinical symptoms, microbiological findings, imaging results compatible with focal infection, and occurrence of additional infective foci.
Results
We included 266 patients with first-time SAB. Among patients with CVC-related SAB, clinical onset, collection of the first positive blood culture, and microbiological confirmation almost coincided. In contrast, among patients with VO or IE, the onset of clinical symptoms most often preceded the collection of the first positive blood culture, and imaging and microbiological confirmation were most frequently obtained subsequent to the SAB diagnosis. CVC-related SAB was infrequently associated with further foci (n = 15/15.5%). Conversely, more than one infective focus was observed in 44 (56.4%) patient with VO and 68 (64.8%) patients with IE.
Conclusions
The sequence of clinical symptoms, diagnostic confirmation, and occurrence of multiple infective foci varied considerably with different infective foci in SAB. Based on these results, we propose a pragmatic and evidence-based terminology for the clinical course of SAB and suggest the terms “portal of entry”, “infective focus”, “multiple infective foci”, and “dominant infective focus”.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Staphylococcus aureus bloodstream infection (SAB) is a serious disease associated with osteoarticular infection, infective endocarditis, and a 30-day mortality of 20–30% in the Western world [1, 2]. Early identification and control of the infective focus remain the mainstays of clinical management in patients with SAB [3, 4]. Indeed, the prognosis of SAB has been demonstrated to vary considerably according to the infective focus, viz respiratory focus, endocarditis and an unidentified focus are associated with high mortality, whereas SAB due to the infection of intravascular access devices is associated with a better outcome [2, 5, 6]. Nevertheless, rather different and inconsistent definitions of the infective focus have been employed in prior studies of SAB and terms such as source of infection, portal of entry, primary and secondary infective foci and primary and secondary SAB have been used interchangeably [7,8,9,10,11,12,13,14,15,16]. Consequently, several aspects of the systemic dissemination of S. aureus infection remain unclear and there is a lack of detailed data elucidating the onset of clinical symptoms, blood culture draw, microbiological confirmation, imaging results, occurrence of multiple infective foci, and whether the chronology of these events differs according to the infective focus.
Such data are important to extend our knowledge of the clinical course of patients with SAB and might help to reduce the interval from onset of infection to initiation of appropriate antimicrobial treatment, thereby potentially contributing to improved clinical outcomes. Therefore, using a prospective cohort of patients with SAB, we elucidated the clinical course of SAB with special attention to the timing and order of events concerning onset of clinical symptoms, diagnostic confirmation, and the presence of multiple infective foci in relation to the infective focus. Furthermore, we briefly introduce the terms used to describe the clinical course of SAB and discuss their usefulness in clinical settings.
Patients and methods
Setting
The present study uses prospectively collected patient data from the Invasive S. aureus Infection Cohort (INSTINCT) which was conducted in two German tertiary care university hospitals in Cologne and Freiburg between 1 January 2006 and 31 December 2011. Details of the INSTINCT study have been described previously [17, 18]. Clinical variables were prospectively recorded by a study group led by infectious diseases physicians and clinical microbiologists during the patients´ hospital stay.
Patients with S. aureus bloodstream infection
Eligible cases were defined as patients ≥ 18 years of age with at least one blood culture positive for S. aureus and accompanying clinical symptoms and signs of infection. We restricted the study population to patients with first-time SAB. Furthermore, patients were excluded if an additional clinically significant bacterial pathogen was isolated from the blood culture. We classified all SAB patients as either community-acquired SAB (CA-SAB) or hospital-acquired SAB (HA-SAB) based on the interval between time of admission and sampling of the first positive blood culture (≤ 2 vs. >2 days, respectively) [19]. The subset of patients with CA-SAB and recent healthcare contacts predating the current hospitalization were further classified as healthcare-associated SAB (HCA-SAB) if one or more of the following criteria were met: (1) intravenous therapy, wound care, or specialized nursing care in the 30 days before SAB onset, (2) contact to a hospital or hemodialysis clinic or intravenous chemotherapy within 30 days of the onset of SAB, (3) > 2 days of hospitalization during the three months before the onset of SAB, or (4) admission from a nursing home [19].
Demographics and comorbidity
We noted the patients´ age at the time of blood culture draw and obtained information on gender. Next, information of all preexisting comorbidities included in the Charlson Comorbidity Index (CCI) was collected. The CCI is a validated comorbidity scoring system assigning between 1 and 6 points to a range of major disease categories [20]. The aggregate score was computed for each patient and three levels of comorbidity were defined: low (score = 0), intermediate (score = 1–2), or high (score > 2). In addition, we collected information on a history of chronic alcohol abuse and active intravenous drug use which are not included in the CCI.
Onset of clinical symptoms, microbiological confirmation, and imaging results
For each patient, we obtained a detailed medical history to gain information on the time of onset of clinical symptoms, defined as systemic signs of infection (fever and/or chills) with or without accompanying local signs of infection. We collected data on all available non-blood culture microbiological findings serving as diagnostic confirmation of S. aureus infection, e.g., cultures of catheter tips, bone biopsies, and heart valve biopsies. Furthermore, data on reports from ultrasonography, magnetic resonance imaging, computed tomography scans, and echocardiographic investigations were obtained.
Portal of entry and infective focus
Information on the portal of entry and the infective focus was individually reviewed post-hoc taking into account the patient history, clinical signs, microbiological findings, and imaging results. We defined the portal of entry as the site where the infection had most likely been initiated, i.e., where S. aureus due to either infection or procedure had initially breached the physical barrier and entered the bloodstream. Accordingly, the portals of entry were categorized into (1) skin (a) skin and soft tissue infections, (b) intravenous drug abuse, or (c) other injections, (2) vascular device, (3) other, and (4) unknown. The infective focus was defined as the site of infection considered most likely to be responsible for seeding S. aureus into the bloodstream. To elucidate a wide and still clearly defined clinical spectrum of SAB, we chose to restrict the study population to patients with the presence of one (or more) of the following three infective foci: (1) central venous catheter (CVC)-related infection, (2) vertebral osteomyelitis (VO), and (3) infective endocarditis (IE). Within these three groups, we further obtained data on any additional infective foci identified during the course of infection.
Statistical analysis
First, the study population was characterized in a contingency table according to the three different infective foci; CVC-related infection, VO, and IE. Next, using the date the first positive blood culture was drawn as reference point, we computed the median time with interquartile ranges (IQRs) to onset of clinical symptoms, microbiological findings, imaging results, and diagnosis of additional infective foci for each patient, and graphically displayed the results stratified by the infective focus. The time of diagnosis of any additional infective foci was established by clinical signs, microbiological findings, or imaging results, whichever came first. To examine whether the chronology of clinical and diagnostic events differed in subsets of SAB patients, we repeated the analyses stratifying by (1) mode of acquisition (CA-SAB, HA-SAB, and HCA-SAB) and (2) oxacillin susceptibility (MSSA and MRSA). All statistical analyses were performed using R software (R Foundation for Statistical Computing, Vienna Austria) and STATA software version 11.2 (STATA, College Station, TX, USA).
Results
Descriptive data
During the study period, we identified 266 patients with first-time SAB and one of the three predefined infective foci. A CVC was an infective focus in 97 (36.5%) of patients, 78 (29.3%) patients were diagnosed with VO and 105 (39.5%) patients had IE. A total of 14 (5.3%) patients had overlapping infective foci (a brief description of these patients´ clinical course and infective foci is given in Online Resource 1).
The proportion of male patients did not differ notably across the three groups. However, patients with a CVC as an infective focus were slightly younger than patients with VO and patients with IE (Table 1). All patients with a CVC as an infective focus were either classified as HA-SAB (96.9%) or HCA-SAB (3.1%), whereas 43.6% of patients with VO and 48.6% of patients with IE were classified as CA-SAB, respectively (Table 1). A substantial difference between the three groups was neither found with MRSA nor with the median CCI scores. As expected, the vascular device was considered the most likely portal of entry among all patients with a CVC as the infective focus. The portal of entry was microbiologically confirmed in 74 (76.3%) of these patients and determined based on clinical signs of infection alone in 23 (23.7%) cases. Among patients with VO, the skin was the most likely portal of entry in 27 (34.6%) of patients [microbiologically confirmed in 9 (11.5%) cases], whereas no portal of entry was identified in 45 (57.7%) of patients. Among patients with IE, the most frequent portals of entry were the skin [34 (32.3%) patients, microbiologically confirmed in 10 (9.5%) cases], vascular devices [27 (25.7%) patients, microbiologically confirmed in 18 (17.1%) cases], and in 43 (41.0%) of patients the portal of entry remained unknown (Table 1).
Sequence of clinical and diagnostic events according to the infective focus
Among patients with CVC-related SAB, the time the first positive blood culture was drawn, onset of clinical symptoms, and microbiological confirmation (cultures of catheter tips positive for S. aureus) were close (Fig. 1a). In contrast, among patients with IE, the onset of clinical symptoms most often preceded the time of blood culture draw (median time = − 1.5 days, interquartile range (IQR) − 4; 0), and imaging confirmation was most frequently obtained subsequent to the SAB diagnosis [median time = 3 days (IQR 1; 8)]. Among patients with VO, the median time from onset of clinical symptoms to the time the first positive blood culture was drawn was − 4 days (IQR − 11; − 1), and median time to microbiological and imaging confirmation was 2 days (IQR 0; 7.5) and 1 day (− 1; 8.5), respectively.

Time to onset of clinical signs of infection, microbiological findings, and imaging results according to each of the three foci (a) and occurrence of additional infective foci (b)
CVC-related infection was infrequently associated with further foci (n = 15/15.5%). Conversely, in 68 (64.8%) patients with IE and 44 (56.4%) patient with VO more than one infective focus was observed within a median of 0 days (IQR − 4; 0) and 0 days (IQR − 2; 2), respectively (Fig. 1b). We observed no consistent pattern or major differences in analyses stratified according to the mode of acquisition (hospital-acquired SAB versus community-acquired SAB) or according to oxacillin resistance (MSSA and MRSA) (shown in Online Resource 2).
Discussion
In this prospective cohort study, we observed notable variation in the clinical course of patients with SAB. In patients with CVC-related SAB, the time the first blood culture was drawn, onset of clinical symptoms, and microbiological confirmation were close. In contrast, among patients with IE and VO, the onset of clinical symptoms most often preceded the time the first positive blood culture was drawn and imaging confirmation was most frequently obtained subsequent to the SAB diagnosis. Patients with CVC-related infection rarely developed further infective foci, whereas this was observed in more than half of patients with IE and VO, respectively.
The time from blood culture positivity to final diagnostic confirmation of the infective focus was considerably shorter for patients with CVC-related infection, as compared with patients with VO and IE. Moreover, while additional infective foci were frequently observed in patients with VO and patients with IE, this was rarely seen in patients with CVC-related infection. Early identification and control of the portal of entry and/or infective focus are strongly associated with decreased risk of developing further infective foci in patients with SAB [2, 5, 6]. As focus identification and control most frequently is more accessible and straightforward among patients with manifest CVC-related infection, this most likely explains part of our findings. In contrast, the portal of entry was only identified in roughly half of the patients with IE and patients with VO in our study population. This may be due to unsuccessful identification despite extensive clinical efforts or, in some cases, it could be that the portal of entry had resolved spontaneously or due to antibiotic treatment at the time of the SAB diagnosis. In addition, it cannot be precluded that in some cases of SAB the portal of entry does not always constitute an actual infective focus (e.g., intravenous drug abuse without local infection leading to IE or hemodialysis and subsequent VO).
In previous studies of SAB, the terms used in the description of the clinical course have been defined with considerable inconsistency [7,8,9,10,11,12,13,14,15,16]. In SAB, the bacteria access the blood by breaching the body´s protective barriers at a specific site, which has most frequently been described as the portal of entry [7,8,9,10]. Nevertheless, the same and other studies have employed different terms for the portal of entry, including the primary site of infection [7], the initial staphylococcal lesion [8], the source of infection [13,14,15], and the primary infective focus [9]. Furthermore, assuming that the portal of entry always constitutes an infective focus, the term the primary infective focus has also been used in a number of previous studies to denote the initial staphylococcal infection leading to bacteraemia while any additional foci were thought to be the result of the SAB and designated secondary infective foci [7, 9, 13, 14]. In contrast, other prior studies have used the prefixes primary and secondary only to discern between primary SAB where no portal of entry or associated infection site was identified and secondary SAB in which the bacteraemia is assumed to stem from an identified portal of entry and/or infective focus [8, 11, 12, 16]. Finally, the occurrence of infective foci in multiple organ systems has often been referred to as metastatic infection. However, the concept remains inconsistently defined [10, 11, 21,22,23] and other terms such as metastatic complications [24], complicating infectious foci [10], and complicated SAB [13, 14, 25] have been used interchangeably.
As suggested by our data, the full extent of S. aureus infection may not be obvious at the time of the SAB diagnosis. Thus, several infective foci may be present and the sequence of occurrence is not always clear. Indeed, as the pathophysiological events are most frequently putative and unobserved, distinguishing between the aforementioned primary and secondary infective foci or primary or secondary SAB may prove very difficult in everyday clinical practice. Although the time elapsed from onset of clinical symptoms to the diagnosis of SAB was less than 2 weeks in the majority of cases it should, nevertheless, be noted that some patients demonstrated a notably insidious clinical course with onset of clinical symptoms as early as 7 weeks before the SAB diagnosis. Furthermore, additional infective foci were frequently observed in patients with VO and IE and occurred as late as 9 weeks after the first positive blood culture was drawn, which emphasizes the importance of continuous monitoring for additional infective foci to attain optimal focus control and adequate treatment duration. Therefore, it may possibly prove more clinically useful to describe the clinical course of SAB simply in terms of (1) the portal of entry and (2) the infective focus/foci and omit theoretical assumptions of sequence. In patients with multiple infective foci, the clinical presentation and the existing evidence on the ranked prognostic impact of the different infective foci (e.g., IE > VO > CVC-related infection) [1, 3, 5, 6] could possibly help the clinician determine a so-called dominant infective focus1 which could guide clinical management including adequate treatment duration (Table 2).
The main strenghts of our study include the restriction of the study population to patients with first-time, monomicrobial SAB and the use of comprehensive prospectively recorded data. Nevertheless, some potential limitations of the study should be addressed. We only included patients from tertiary care medical centers, thus our results may not be directly applicable to other settings. Even so, it seems reasonable to assume that these results may apply to other settings and countries with similar demographics and equal access to healthcare. In addition, information on the onset of clinical symptoms were obtained subsequent to the SAB diagnosis, therefore, we cannot rule out that these particular data have been affected by some degree of recall bias and thus inaccuracy. Still, the clinical data were meticoulously obtained by infectious diseases physicians and clinical microbiologists during the hospitalization, and we consider it unlikely that misclassification of onset of clinical symptoms has influenced our results notably. We chose only to include SAB patients with CVC-related infection, IE, or VO. However, we cannot entirely rule out that some patients may have died before an infective focus was identified or that some patients with one of the three predefined foci were falsely classified as another or unknown infective focus. If such misclassification was particularly pronounced for one type of the three predefined foci, it might have influenced our findings.
In conclusion, the order of events concerning onset of clinical symptoms, diagnostic confirmation, and presence of multiple infective foci varied considerably with different infective foci in patients with SAB. In patients with VO and IE, additional foci were diagnosed as late as 9 weeks after the SAB diagnosis which underlines the importance of continuous search for additional infective foci to attain optimal focus control and adequate treatment duration. To ensure a consistent, pragmatic, and evidence-based terminology for the clinical course of SAB, we suggest the terms portal of entry, the infective focus, multiple infective foci, and dominant infective focus, as defined above, yet further clinical studies addressing this important issue are indeed warranted.
References
Kaasch A, Barlow G, Edgeworth JD, Fowler VG Jr, Hellmich M, Hopkins S, et al. Staphylococcus aureus bloodstream infection: a pooled analysis of five prospective, observational studies. J Infect. 2014;68:242–51.
van Hal SJ, Jensen SO, Vaska VL, Espedido BA, Paterson DL, Gosbell IB. Predictors or mortality in Staphylococcus aureus bacteremia. Clin Microbiol Rev. 2012;25:362 – 86.
Gudiol F, Aguado JM, Almirante B, Bouza E, Cercenado E, Domínguez M, et al. Diagnosis and treatment of bacteremia and endocarditis due to Staphylococcus aureus. A clinical guideline from the Spanish Society of Clinical Microbiology and Infectious Diseases (SEIMC). Enferm Infecc Microbiol Clin. 2015;33:625.e1–625.e23
Holland TL, Arnold C, Fowler VG Jr. Clinical management of Staphylococcus aureus bacteremia. JAMA. 2014;312:1330–41.
Tong SYC, Davis JS, Eichenberger E, Holland TL, Fowler VG Jr. Staphylococcus aureus infections: epidemiology, pathophysiology, clinical manifestations, and management. Clin Microbiol Rev. 2015;28:603–61.
Soriano A, Martinez JA, Mensa J, Marco F, Almela M, Moreno-Martínez A, et al. Pathogenic significance of methicillin resistance for patients with Staphylococcus aureus bacteremia. Clin Infect Dis. 2000;30:368–73.
Nolan CM, Beaty HN. Staphylococcus aureus bacteremia. Current clinical patterns. Am J Med. 1976;60:495–500.
Lautenschlager S, Herzog C, Zimmerli W. Course and outcome of bacteremia due to Staphylococcus aureus: Evaluation of different clinical case definitions. Clin Infect Dis. 1993;16:567–73.
Mylotte JM, Tayara A. Staphylococcus aureus bacteremia: predictors of 30-day mortality in a large cohort. Clin Infect Dis. 2000;31:1170–4.
Cuijpers ML, Vos FJ, Bleeker-Rovers CP, Krabbe PF, Pickkers P, van Dijk AP, et al. Complicating infectious foci in patients with Staphylococcus aureus or Streptococcus species bacteraemia. Eur J Clin Microbiol Infect Dis. 2007;26:105–13.
Saginur R, Suh KN. Staphylococcus aureus bacteraemia of unknown primary source: Where do we stand? Int J Antimicrob Agents. 2008;32:S21-25.
del Rio A, Cervera C. Moreno A, Moreillon P, Miró JM. Patients at risk of complications of Staphylococcus aureus bloodstream infection. Clin Infect Dis. 2009;48:S246-253.
Price J, Baker G, Heath I, Walker-Bone K, Cubbon M, Curtis S, et al. Clinical and microbiological determinants of outcome in Staphylococcus aureus bacteraemia. Int J Microbiol 2010;2010:654858.
Asgeirsson H, Kristjansson M, Kristinsson KG, Gudlaugsson O. Clinical significance of Staphylococcus aureus bacteriuria in a nationwide study of adults with S. aureus bacteremia. J Infect. 2012;64:41–6.
Paulsen J, Mehl A, Askim Å, Solligård E, Åsvold BO, Damås JK. Epidemiology and outcome of Staphylococcus aureus bloodstream infection and sepsis in a Norwegian county 1996–2011: an observational study. BMC Infect Dis. 2015;15:116. https://doi.org/10.1186/s12879-015-0849-4.
https://www.cdc.gov/nhsn/pdfs/pscmanual/4psc_clabscurrent.pdf. 2018. Accessed 22 Feb 2018
Seifert H, Wisplinghoff H, Kaasch A, Achilles K, Langhorst A, Peyerl-Hoffmann G, et al. Epidemiology, course and prognosis of Staphylococcus aureus bacteremia - Preliminary results from the INSTINCT (INvasive STaphylococcus aureus INfection CohorT) cohort. Dtsch Med Wochenschr. 2008;133:340–5.
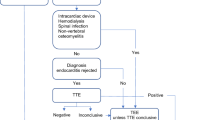
Kaasch AJ, Fowler VG Jr, Rieg S, Peyerl-Hoffmann G, Birkholz H, Hellmich M, et al. Use of a simple criteria set for guiding echocardiography in nosocomial Staphylococcus aureus bacteremia. Clin Infect Dis. 2011;53:1–9.
Friedman ND, Kaye KS, Stout JE, McGarry SA, Trivette SL, Briggs JP, et al. Healthcare-associated infections in adults: a reason to the change the accepted definition if community-acquired infections. Ann Intern Med. 2002;137:791–7.
Charlson M, Pompei P, Ales KL. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J Chron Dis. 1987;40:373 – 83.
Horino T, Sato F, Hosaka Y, Hoshina T, Tamura K, Nakahrai K, et al. Predictive factors for metastatic infection in patients with bacteremia caused by methicillin-sensitive Staphylococcus aureus. Am J Med Sci. 2015;349:24–8.
Kim SH, Park WB, Lee KD, Kang CI, Kim HB, Oh MD, et al. Outcome of Staphylococcus aureus bacteremia in patients with eradicable foci versus noneradicable foci. Clin Infect Dis. 2003;37:794–9.
Vos FJ, Kullberg BJ, Sturm PD, Krabbe PF, van Dijk AP, Wanten GJ, et al. Metastatic infectious disease and clinical outcome in Staphylococcus aureus and Streptococcus species bacteremia. Medicine (Baltimore). 2012;91:86–94.
Ringberg H, Thorén A, Lilja B. Metastatic complications of Staphylococcus aureus septicemia. To seek is to find. Infection. 2000;28:132–6.
Fowler VG Jr, Olsen MK, Corey GR, Woods CW, Cabell CH, Reller LB, et al. Clinical identifiers of complicated Staphylococcus aureus bacteremia. Arch Intern Med. 2003;163:2066–72.
Acknowledgements
The authors thank Christian Bernasch (Institute for Medical Microbiology, Immunology and Hygiene, University of Cologne, Germany), Hanna Birkholz (Clinical Trials Center, University of Cologne, Germany), and Gabriele Peyerl-Hoffmann (Department of Medicine II, University Medical Center Freiburg, Germany) for providing administrative support and collecting patient data.
Funding
This work was supported by the Deutsche Forschungsgemeinschaft (DFG; grant number KA 3104/1–1 to A.J.K.), the Paul-Ehrlich Gesellschaft für Chemotherapie (to HS and WVK), and the Bundesministerium für Bildung und Forschung (BMBF 01KI1017 to AJK/01KN1106 to the Clinical Trial Center Cologne). The funding organizations had no role in the design of the study, data collection, and data analysis.
Author information
Authors and Affiliations
Contributions
JS: study design, data management, analysis and interpretation, and manuscript preparation. AJK: data collection, study concept and design, data management, analysis and interpretation, and manuscript review. SRR, WVK, HS, AFW: data collection, study design, interpretation of the data, manuscript review. HCS: study design, interpretation of the data, manuscript review. All the authors have read and approved the final draft submitted.
Corresponding author
Ethics declarations
Ethical approval
The study and data collection were approved by the institutional review boards of the University Medical Centers Freiburg and Cologne. We followed the ethical standards set by the Helsinki Declaration of 1975, as revised in 2004, and the research guidelines of the Universities of Freiburg and Cologne. Written informed consent was obtained from the patients at the University Medical Center Cologne. The institutional review board of the University Medical Center Freiburg considered the investigation as evaluation of service within a quality assurance program and waived the need for written informed consent. The study is registered in the German Clinical Trials Registry (DRKS00005045).
Conflict of interest
A.J.K. has received payments for lectures from BD Biosciences, bioMérieux, MSD Sharp & Dohme, Limbach Gruppe SE, and ViiV Healthcare and travel support from Janssen-Cilag. H.S. has received grants or research support from the Bundesministerium für Bildung und Forschung (BMBF), Germany, the German Centre for Infection Research (DZIF), Basilea, Novartis and Pfizer, has been a consultant for Astellas, AstraZeneca, Basilea, Cubist, Novartis, Pfizer, Tetraphase, and The Medicines Company, and has received payments for lectures from MSD, Novartis and Pfizer. S.R. has received payments for lectures from Pfizer and MSD Sharp & Dohme, as well as travel support from Astellas and MSD Sharp & Dohme. W.V.K., A.F.W., J.S and H.C.S report no conflicts.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Smit, J., Rieg, S.R., Wendel, A.F. et al. Onset of symptoms, diagnostic confirmation, and occurrence of multiple infective foci in patients with Staphylococcus aureus bloodstream infection: a look into the order of events and potential clinical implications. Infection 46, 651–658 (2018). https://doi.org/10.1007/s15010-018-1165-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s15010-018-1165-x