
Abstract
Purpose
In 2016, the number of refugees worldwide reached 65.6 million. So far, only limited data are available on the health status of refugees and asylum seekers (RAs). Especially, notifiable infectious diseases (NIDs) carry the risk of outbreaks in communal accommodations hosting RAs.
Methods
We conducted a monocentric retrolective cross-sectional study including 15,137 RAs treated in a special health care unit for RAs located in the major reception center in Munich from November 2014 to October 2016. Altogether 811 RAs with NIDs according to sections 6 and 7 of the German Infection Protection Act or with other infections relevant in the setting of a communal accommodation (RIDs) could be identified.
Results
The gender and age distribution was generally comparable to that of refugees in Germany. However, patients from East Africa and Nigeria were significantly overrepresented. NIDs/RIDs were dominated by cases of tuberculosis, hepatitis B, and vaccine-preventable and parasitic diseases. Significant risk factors included country of origin (COI) and age for hepatitis B, age for hepatitis C, gender and age for HIV, and COI, gender and age for tuberculosis and ectoparasitosis. Calculated prevalences of hepatitis B, hepatitis C, and HIV were mostly below those of the COI. Incidences of tuberculosis were mostly strongly elevated.
Conclusions
COI, gender, and age have an impact on the occurrence of NIDs/RIDs. Early vaccinations and improved hygiene could be effective in preventing NIDs/RIDs in communal accommodations. Screening, prompt therapy, and infection protection measures are necessary to prevent the transmission of diseases.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The Global Trends Report of the United Nations High Commissioner for Refugees shows a number of 65.6 million forcibly displaced persons worldwide by the end of 2016 [1]. In 2015, the number of newly registered asylum seekers in Germany amounted to a total of 890,000 people [2]. Representative data on the health status of refugees and asylum seekers (RAs) are not available up to now [3, 4]. In this study, the occurrence of notifiable infectious diseases (NIDs) in accordance with section 6 as well as infections with a pathogen according to section 7 of the German Infection Protection Act (IfSG) or any other infectious disease relevant in the setting of a communal accommodation (RIDs) is examined using the example of the “Bayernkaserne”, the major reception center located in Munich, Germany.
In 2015, 476,649 asylum applications were submitted to the Federal Office for Migration and Refugees (BAMF), followed by further 745,545 applications in 2016 [5, 6]. Syria, Afghanistan, and Iraq were among the most relevant nationalities of RAs in 2016. In general, 65.7% of the RAs are male and 73.8% are under the age of 30 [6]. Due to the sharp rise in involuntary migration, considerable challenges for the health systems of the hosting countries arise [7]. Previous studies showed that refugees are often suffering from the same diseases as the resident population and thus do not represent an increased risk of infection for the general population [8,9,10]. In particular, illnesses well known in general medicine, such as respiratory infections, neuropsychiatric diseases, gastrointestinal infections, diseases of the musculoskeletal system, and skin diseases, have been diagnosed [11, 12] Also, partly due to the screening procedures, the reported infectious diseases of RAs as of October 2017 reveal a comparatively higher number of cases of tuberculosis, hepatitis B, and hepatitis C as well as vaccine-preventable diseases and gastrointestinal infections [8]. As RAs are a heterogeneous population, they could differ concerning risk factors for acquiring infectious diseases. The countries of origin (COIs), countries crossed in transit, and the conditions during the flight could be of importance [9, 13]. Other relevant issues concern the lack of knowledge about sexually transmitted diseases, provision of barrier contraceptives, and sexual violence [14].
Research question and hypotheses
The primary goal of this study was to identify and statistically confirm possible risk factors for NIDs and RIDs to improve detection and prevention of these diseases in RAs.
Methods
The population under investigation consists of RAs who were treated from November 1, 2014 to October 10, 2016, at a special health care unit for RAs run by REFUDOCS, an association for the medical care of refugees, asylum seekers, and their children, in the reception center “Bayernkaserne” in Munich. Medical data were collected by REFUDOCS using a commercially available database (x.isynet version 15.1 of medatixx GmbH & Co. KG, Regensburg, Germany). REFUDOCS provided irreversibly anonymized data concerning patients suffering from an NID/RID. The following data were collected: gender, date of birth, nationality, and diagnosis.
Concerning the classification of the hepatitis B serology, all cases in which the HBs antigen, anti-HBc, and anti-HBe were positive were considered to be chronic, whereas cases in which the HBs antigen, anti-HBc, and the HBe antigen were positive were additionally regarded as highly infective. All cases with both positive anti-HBs and anti-HBc, and cases in which only anti-HBc was positive in the serology and hepatitis B virus DNA was not detectable were regarded as past infections [15]. Cases with a past infection remain part of the hepatitis B number of cases to obtain a larger comparison population. NIDs/RIDs were additionally classified into disease groups: skin diseases (impetigo contagiosa, pediculosis, scabies, and varicella zoster), vaccine-preventable diseases (hepatitis B, influenza, measles, pertussis, post-polio syndrome, and varicella), sexually transmittable diseases (hepatitis B, hepatitis C, HIV, lues, and scabies), and systemic and gastrointestinal diseases (giardiasis, hepatitis B, hepatitis C, HIV, influenza, louse-borne relapsing fever, lues, malaria, measles, post-polio syndrome, and tuberculosis). As several diseases were included into more than one group, percentages can add to more than 100%. Statistical analysis and graphics were done with IBM SPSS Statistics 24 (IBM, Armonk, USA). Risk factors for the occurrence of the infectious diseases hepatitis B, hepatitis C, HIV, pediculosis, scabies, and tuberculosis were explored by logistic regression analysis. The risk factors such as gender, age, and regions according to the geographic division of the United Nations were used [16]. The reference category for the variable regions consisted of regions which could not been included in the logistic regression analysis due to the small number of patients and those patients with unknown nationalities. A p < 0.05 was considered to be significant. The study was approved by the ethics committee of the Ludwig-Maximilians University, Munich.
Results
Demographic data
The population under investigation consisted of 15,137 RAs. The nationality of only 8130 patients was known and included 66 different nationalities. Out of 15,137 RAs, the study population of 811 patients with an NID/RID was identified. Altogether, 882 NIDs/RIDs were diagnosed. The study population consisted of 197 (24.3%) women and 614 (75.7%) men. Concerning the gender distribution according to COI, male patients were mostly predominant, except for individuals with Nigerian origin showing almost 50% female patients (Fig. 1).

Gender distribution by nationality
Regarding the age structure, the large number of young adults is noticeable compared to the decrease in the number of patients over the age of 40. 116 (14.3%) minors and 695 (85.7%) adults were treated. In 738 out of 811 patients (91.0%) the nationality was known. These came from 33 COIs. Predominantly, patients from Somalia (17.8%), Nigeria (13.4%), Afghanistan (13.3%), Eritrea (9.7%), and Syria (7.4%) were treated for an NID/RID.
Notifiable and other relevant infectious diseases
Hepatitis B, hepatitis C, HIV, pediculosis, scabies, and tuberculosis represented the NIDs/RIDs with the highest number of cases accounting for 798 (90.5%) out of the 882 cases (Fig. 2). Concerning hepatitis B virus infections, 17 (10.6%) cases had an unclear serostatus, 100 (62.5%) had chronic infections, 6 (3.8%) had chronic infections and were highly infectious, and 37 (23.1%) had past infections. Cases of tuberculosis could be divided into 142 (65.4%) pulmonary, 18 (8.3%) extrapulmonary, 17 (7.8%) both pulmonary and extrapulmonary, and 40 (18.4%) with no further differentiation. Notably, 194 (22.0%) out of the 882 cases were vaccine-preventable diseases and 407 (46.1%) were caused by skin diseases. 382 (43.3%) cases were caused solely by scabies and pediculosis. In addition, 513 (58.2%) of the cases were sexually transmittable. Systemic and gastrointestinal diseases together amounted to 457 (51.8%) cases.

Overview of NIDs/RIDs
NIDs/RIDs according to gender
213 cases (24.1%) occurred in female patients and 669 (75.9%) in male patients. This was mostly consistent with the general gender distribution. Notably, concerning HIV and pediculosis, the female sex was significantly overrepresented (65.4 and 68.0%, respectively).
NIDs/RIDs according to age
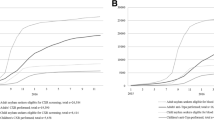
RAs in our study were a young population (range 2–76 years, median 23 years). Skin diseases and vaccine-preventable diseases were more prevalent from childhood to young adulthood (Fig. 3). Chronic infectious diseases and sexually transmitted diseases were predominant in adults older than 25 years. Concerning cases of varicella zoster, the low age median is noticeable.

Overview of NIDs/RIDs by age
NIDs/RIDs according to country
Concerning hepatitis B, 55.2% of the patients with NIDs/RIDs from Mali, 50.0% from Senegal, 48.1% from Sierra Leone, 29.4% from Nigeria, 13.9% from Afghanistan, and 11.1% from Somalia were infected or had past infections. Hepatitis C infections were found in 6.7% of patients from Syria and 2.8% from Nigeria. HIV infections were predominantly diagnosed in patients of Nigerian origin (14.7%). The highest percentage shares for pediculosis were found in patients from Syria (28.3%), Nigeria (11.0%), Afghanistan (7.4%), and Somalia (6.3%). Scabies was most often seen in patients from Eritrea (65.8%), Somalia (47.9%), Afghanistan (39.8%), and Nigeria (26.6%). COIs with the highest percentage shares for tuberculosis were Pakistan (58.5%), Somalia (45.1%), and Afghanistan (30.6%). The two patients with louse-borne relapsing fever stemmed from Somalia, had condition after infection and presented for follow-up. One had experienced a mild course of disease, the other a severe form with multi-organ failure requiring invasive ventilation and intensive care therapy.
Due to the high number of patients, incidences and prevalences in RAs could be calculated for the countries Afghanistan, Eritrea, Nigeria, Sierra Leone, Somalia, and Syria and compared with those in the respective COI (Table 1).
The prevalences of hepatitis B, hepatitis C, and HIV, except for the prevalence of hepatitis B in Sierra Leone, were below those in the respective COIs. The same applies to the incidences of malaria except for Somalia. In contrast, the incidences of tuberculosis show on average 23 times higher values in the “Bayernkaserne”. Especially, the high incidences of tuberculosis for the nationalities Sierra Leone and Somalia have to be mentioned.
Concerning the results of the logistic regression analysis, rising age and the COI were significant risk factors for hepatitis B, rising age for hepatitis C, gender and rising age for HIV, COI, gender and rising age for tuberculosis, and COI, gender and falling age for scabies and pediculosis (Table 2).
Discussion
The composition of the study population concerning gender and age distribution corresponds to that of refugees in general [6, 23,24,25]. Syria, Afghanistan, Iraq, Albania, and Kosovo were the most important COIs in 2015 and 2016 [26, 27]. The RKI numbers Syria, Afghanistan, Iraq, Eritrea and Somalia among the most frequently mentioned COIs related to NIDs [28, 29]. In our study population, in descending order, Somalia, Nigeria, Afghanistan, Eritrea, and Syria were the most relevant COIs. Patients from East Africa and Nigeria were, therefore, overrepresented. Traditionally, more African asylum seekers can be found in Munich, resulting also from the specialization and competence of the regional offices of the BAMF [30, 31]. Whereas RAs from Syria and Iraq used the Balkan route until March 2016, RAs from sub-Saharan Africa had to cross the Mediterranean Sea. This flight route includes possibly more health risks (e.g., desolate hygienic and social conditions in refugee camps in Northern Africa). In addition, the countries of sub-Saharan Africa have higher prevalences of hepatitis B and HIV compared to West Asia [32, 33]. In accordance with that, a Swiss study also showed a higher number of infectious diseases in refugees from the African region and in particular in Eritrean refugees [24].
Due to screening, tuberculosis, hepatitis B, and hepatitis C cases are found more often among RAs. In addition, vaccine-preventable diseases and gastrointestinal infections have been reported frequently [8]. According to an article reviewing studies from 2003 to 2016 at points of care in Europe, respiratory, gastrointestinal, and dermatological infections are among the most frequent communicable diseases in refugees and migrants as well as vaccine-preventable diseases [12]. This is largely in accordance with the NIDs/RIDs diagnosed in this study. The high proportion of vaccine-preventable and sexually transmitted diseases is of interest, as these cases could be significantly reduced by vaccination, sex education, and the provision of barrier contraceptives [14]. The share of pediculosis and scabies could also be reduced by improved hygienic measures. Other European studies confirm the high number of infections with scabies and skin infections in general [23, 24].
Concerning gender distribution, the relatively high percentage of female patients with HIV and pediculosis is interesting. Female Nigerians with an NID/RID were clearly overrepresented in our population, particularly regarding HIV infections. In general, women not only in Nigeria (3.3 vs. 2.6%) but also in all of Africa show higher prevalences of HIV [34]. Furthermore, HIV infections are important in the medical care for pregnant women, leading to more documented cases. The female predominance for pediculosis can be explained by hair length and frequent contact with children.
Concerning age distribution, skin diseases and vaccine-preventable diseases play a major role in childhood and young adulthood. Especially in the view of low immunization rates in underaged RAs (68.9%) for complete positive serostatus for measles, mumps, rubella, and varicella, prompt vaccination is recommended [35]. In Greece, 91.3% of refugee children presented with an unknown vaccination status [36]. Outbreaks of measles can affect the population of the host countries as seen in the measles outbreak in Berlin in 2014/2015 [37]. Regarding varicella zoster, the comparatively low median age of the patients could be explained by the small number of only three persons affected and the physical and psychological stress caused by the flight as further infectious diseases could be excluded.
Lower prevalences of hepatitis B, hepatitis C, and HIV and lower incidences of malaria were found in the reception center compared to the COIs. As in the reception center, the documentation of NIDs depends on the medical consultation, possibly not all cases are captured. This is confirmed by the higher percentage shares in the data from the Bavarian Office for Health and Food Safety which has access to the complete screening data from all RAs arriving in Bavaria which are, for example, in accordance with the HIV prevalences in the COIs, e.g., 3.58% in Nigerian RAs [38]. An Italian study also reported higher prevalences of hepatitis B, hepatitis C, and HIV (9, 4 and 1%, respectively), and identified in RAs from sub-Saharan Africa an HBsAg-positivity rate of 14% [33]. The results of a meta-analysis validated the prevalences of hepatitis B and hepatitis C (10.5, 3.4%) among RAs of African origin [39].
Concerning the lower incidences of malaria, especially for malaria tropica, the stay in malaria-endemic regions within the previous 3 months after arrival is crucial [40]. Only those RAs with persisting low-grade parasitaemia acquired in their home countries or malarious areas crossed during the flight could get symptomatic as no further relevant risk of infection exists in the areas of Northern Africa and Europe. In contrast to this, tertian malaria can still show relapses even after years. In several European countries, a rise of Plasmodium vivax malaria, predominantly in RAs from Eritrea, has been observed [25, 41]. Unfortunately, in our study, malaria cases could not be further differentiated.
The incidences of tuberculosis show highly elevated rates, up to a factor of 23. An up to tenfold increase in incidences in asylum screenings compared to country-specific incidences could also be confirmed by other studies [30, 42]. In addition, almost half of the asylum seekers who presented at the Emergency Department of a Dutch university hospital had an infectious disease of which 34% suffered from pulmonary tuberculosis [25]. In our study, the COIs, the division into pulmonary and extrapulmonary cases, and the age median are in accordance with the data of the RKI [43]. Physical and psychosocial stress can lead to a reduced general condition of health as well as to a progression and reactivation of a latent tuberculosis infection [44]. On the other hand, the incidences and prevalences calculated in this study should also be considered cautiously, since they are based on the system-stored nationality of only 8130 patients limiting the value of these data, and the nationality was known for only 738 out of 811 patients with NIDs/RIDs. In addition, the population is suffering from at least one NID/RID and thus does not correspond to a large healthy group. The exposure for tuberculosis can take place in the COI or during the flight. In our study, particularly, RAs arriving from regions of East Africa, South Asia, Eastern Europe, and Southern Europe are at risk. On the other hand, published data up to now do not suggest a significantly elevated risk of transmission to the population of the hosting countries. Risk group for infection are the RAs themselves either by reactivation or infection by close contact to other RAs [45].
Origin from the regions Middle and West Africa was a significant risk of infection with hepatitis B. Other publications also suggest that countries in sub-Saharan Africa and the Western Pacific region have the highest prevalences of hepatitis B [32]. Screening for hepatitis B and vaccination are, therefore, relevant for RAs stemming from these regions [14].
Primarily children would take advantage of prevention against pediculosis. The protective effect the risk factor “regions” has on scabies can be explained by the reference category used, which consisted of patients from other regions not specially mentioned or of unknown nationality of which a large proportion was suffering from scabies.
Regarding the limitations of the study, it has to be pointed out that the nationality was unfortunately not known for all RAs, therefore, resulting in imprecision concerning the calculations of the country-specific incidences and prevalences. In addition, the study was conducted as a single-center analysis, which includes the risk of bias concerning nationality and typology of the RAs, making a generalization of the results difficult. As the time of permanence of the RAs in Europe could not be determined, the site of infection acquisition is difficult to ascertain.
Although the high rates of tuberculosis are of concern, the prevalence of other NIDs/RIDs with relevant risk of spreading in the hosting country like hepatitis B or HIV in our study was low. However, the vulnerability of RAs regarding, especially, vaccine-preventable diseases should be of utmost importance in the prevention of infectious diseases and cases of NIDs/RIDs should be monitored across Europe [46]. Treating physicians should be aware of the possibility of tuberculosis reactivation in RAs so that cases can be detected and treated early on. Laboratory tests identifying those persons that are at elevated risk of reactivation of tuberculosis are especially warranted. Furthermore, collection of medical data should also focus on the medical presentations of RAs in the regular medical system, i.e., at the offices of general practitioners, pediatricians, or gynecologists to investigate, in the future, the scope of the burden of illness in RAs concerning especially tuberculosis and also psychiatric sequelae of the flight such as post-traumatic stress disorders.
References
United Nations High Commissioner for Refugees. Global Trends 2016. 2017. http://www.unhcr.org/5943e8a34.pdf. Accessed 17 Dec 2017.
Federal Office for Migration and Refugees (BAMF). Migration report of the Federal Office for Migration and Refugees (BAMF) on behalf of the Federal Government 2015. Federal Ministry of the Interior (BMI), Berlin. 2016. https://www.bmi.bund.de/SharedDocs/downloads/DE/publikationen/2016/migrationsbericht-2015.pdf?__blob=publicationFile&v=4. Accessed 24 Mar 2018.
Schneider C, Mohsenpour A, Joos S, Bozorgmehr K. Health status of and health-care provision to asylum seekers in Germany: protocol for a systematic review and evidence mapping of empirical studies. Syst Rev. 2014;3:139. https://doi.org/10.1186/2046-4053-3-139.
Bradby H, Humphris R, Newall D, Phillimore J. WHO Health Evidence Network Synthesis Reports. Public Health Aspects of Migrant Health: A Review of the Evidence on Health Status for Refugees and Asylum Seekers in the European Region. Copenhagen: WHO Regional Office for Europe Copyright (c) World Health Organization 2015; 2015.
Federal Office for Migration and Refugees (BAMF). Current figures on asylum. Issue: December 2015. 2016. http://www.bamf.de/SharedDocs/Anlagen/DE/Downloads/Infothek/Statistik/Asyl/aktuelle-zahlen-zu-asyl-dezember-2015.pdf?__blob=publicationFile. Accessed 30 May 2017.
Federal Office for Migration and Refugees (BAMF). Current figures on asylum. Issue: December 2016. 2017. https://www.bamf.de/SharedDocs/Anlagen/DE/Downloads/Infothek/Statistik/Asyl/aktuelle-zahlen-zu-asyl-dezember-2016.pdf?__blob=publicationFile. Accessed 30 May 2017.
Khan MS, Osei-Kofi A, Omar A, Kirkbride H, Kessel A, Abbara A, et al. Pathogens, prejudice, and politics: the role of the global health community in the European refugee crisis. Lancet Infect Dis. 2016;16:e173–7. https://doi.org/10.1016/S1473-3099(16)30134-7.
Robert Koch Institute. Notifiable infectious diseases in asylum seekers in Germany submitted to the Robert Koch Institute—October 2017. 2017. https://www.rki.de/DE/Content/Gesundheitsmonitoring/Gesundheitsberichterstattung/GesundAZ/Content/A/Asylsuchende/Inhalt/meldepflichtige_Infektionskrankheiten_bei_Asylsuchenden.pdf?__blob=publicationFile. Accessed 17 Dec 2017.
Razum O, Wenner J. Social and health epidemiology of immigrants in Germany: past, present and future. Public Health Rev. 2016;37:4. https://doi.org/10.1186/s40985-016-0019-2.
World Health Organization. Refugees and migrants: common health problems. n.d. http://www.euro.who.int/__data/assets/pdf_file/0005/293270/Migration-Health-Key-Issues-.pdf?ua=1&ua=1. Accessed 25 Mar 2018.
Alberer M, Wendeborn M, Löscher T, Seilmaier M. Spectrum of diseases occurring in refugees and asylum seekers: data from three different medical institutions in the Munich area from 2014 and 2015. Dtsch Med Wochenschr. 2016;141:e8–15. https://doi.org/10.1055/s-0041-106907.
Pavli A, Maltezou H. Health problems of newly arrived migrants and refugees in Europe. J Travel Med. 2017;24:1–8. https://doi.org/10.1093/jtm/tax016.
European Centre for Disease Prevention and Control. Infectious diseases of specific relevance to newly-arrived migrants in the EU/EEA, p. 2. 2015b. http://ecdc.europa.eu/en/publications/Publications/Infectious-diseases-of-specific-relevance-to-newly-arrived-migrants-in-EU-EEA.pdf. Accessed 30 May 2017.
Schulz TR, Paxton G, Biggs B-A. Infectious Diseases. In: Loue S, Sajatovic M, editors. Encyclopedia of Immigrant Health. 1st ed. New York: Springer; 2012. p. 902–10.
Song JE, Kim DY. Diagnosis of hepatitis B. Ann Transl Med. 2016;4:338. https://doi.org/10.21037/atm.2016.09.11.
United Nations. Methodology: Standard country or area codes for statistical use (M49). Countries or areas/geographical regions. n.d. https://unstats.un.org/unsd/methodology/m49/. Accessed 25 Mar 2018.
Ott JJ, Stevens GA, Groeger J, Wiersma ST. Global epidemiology of hepatitis B virus infection: new estimates of age-specific HBsAg seroprevalence and endemicity. Vaccine. 2012;30:2212–9. https://doi.org/10.1016/j.vaccine.2011.12.116.
Gower E, Estes C, Blach S, Razavi-Shearer K, Razavi H. Global epidemiology and genotype distribution of the hepatitis C virus infection. J Hepatol. 2014;61(1 Suppl):S45–57. https://doi.org/10.1016/j.jhep.2014.07.027.
World Health Organization. Prevalence of HIV among adults aged 15 to 49. 2017. http://apps.who.int/gho/data/node.main.622?lang=en. Accessed 21 June 2017.
Joint United Nations Programme on HIV/AIDS (UNAIDS). Nigeria: HIV and AIDS estimates 2015. n.d. http://www.unaids.org/en/regionscountries/countries/nigeria/. Accessed 21 June 2017.
World Health Organization. Malaria: Reported indigenous confirmed cases. 2015. http://apps.who.int/gho/data/node.main.A1364?lang=en. Accessed 21 June 2017.
World Health Organization. Tuberculosis Incidence: Data by country. 2017. http://apps.who.int/gho/data/view.main.57040ALL?lang=en. Accessed 21 June 2017.
van Berlaer G, Bohle Carbonell F, Manantsoa S, de Béthune X, Buyl R, Debacker M, Hubloue I. A refugee camp in the centre of Europe: clinical characteristics of asylum seekers arriving in Brussels. BMJ Open. 2016;6:e013963. https://doi.org/10.1136/bmjopen-2016-013963.
Bloch-Infanger C, Bättig V, Kremo J, Widmer AF, Egli A, Bingisser R, et al. Increasing prevalence of infectious diseases in asylum seekers at a tertiary care hospital in Switzerland. PLoS One. 2017;12:e0179537. https://doi.org/10.1371/journal.pone.0179537.
Ravensbergen SJ, Lokate M, Cornish D, Kloeze E, Ott A, Friedrich AW, et al. High prevalence of infectious diseases and drug-resistant microorganisms in asylum seekers admitted to hospital; no carbapenemase producing enterobacteriaceae until september 2015. PLoS One. 2016;11:e0154791. https://doi.org/10.1371/journal.pone.0154791.
Federal Office for Migration and Refugees (BAMF). Asylum statistics of 2015. 2016. https://www.proasyl.de/wp-content/uploads/2015/12/2015_HKL_AntragsEntscheidungsstatistik.pdf. Accessed 13 June 2017.
Federal Office for Migration and Refugees (BAMF). Asylum statistics of 2016. 2017. https://www.proasyl.de/wp-content/uploads/2015/12/Asylantrage-und-Entscheidungen-2016.pdf. Accessed 13 June 2017.
Robert Koch Institute. Notifiable infectious diseases in asylum seekers in Germany submitted to the Robert Koch Institute—2015. 2016. https://www.landtag.nrw.de/Dokumentenservice/portal/WWW/dokumentenarchiv/Dokument/MMV16-3729.pdf;jsessionid=33DF2BEE1BA1FB429AC4BA7CE41F813D.ifxworker. Accessed 15 June 2017.
Robert Koch Institute. Notifiable infectious diseases in asylum seekers in Germany submitted to the Robert Koch Institute—2016. 2017. http://docplayer.org/40443138-Dem-robert-koch-institut-uebermittelte-meldepflichtige-infektionskrankheiten-bei-asylsuchenden-in-deutschland.html. Accessed 25 Mar 2018.
Halder G, Kerschel J. Tuberculosis in asylum seekers—data from Munich 2015. Hyg Med. 2016;41:D179–82.
Organisation for Economic Co-operation and Development (OECD). Finding their Way—The Labour Market Integration of Refugees in Germany. 2017. https://www.oecd.org/berlin/publikationen/Arbeitsmarktintegration-von-Fluechtlingen-in-Deutschland-2017.pdf. Accessed 1 June 2017.
Schweitzer A, Horn J, Mikolajczyk RT, Krause G, Ott JJ. Estimations of worldwide prevalence of chronic hepatitis B virus infection: a systematic review of data published between 1965 and 2013. Lancet. 2015;386:1546–55. https://doi.org/10.1016/s0140-6736(15)61412-x.
Coppola N, Alessio L, Gualdieri L, Pisaturo M, Sagnelli C, Caprio N, et al. Hepatitis B virus, hepatitis C virus and human immunodeficiency virus infection in undocumented migrants and refugees in southern Italy, January 2012 to June 2013. Euro Surveill. 2015;20:30009. https://doi.org/10.2807/1560-7917.ES.2015.20.35.30009.
Joint United Nations Programme on HIV/AIDS (UNAIDS). Country factsheets Nigeria 2016: HIV and AIDS Estimates. n.d. http://aidsinfo.unaids.org/?did=5581277ae9beccab3bd5a44e&r=world&t=2016&tb=q&bt=undefined&ts=0,0&qla=C&qls=NGA. Accessed 3 Aug 2017.
Jablonka A, Happle C, Grote U, Schleenvoigt BT, Hampel A, Dopfer C, et al. Measles, mumps, rubella, and varicella seroprevalence in refugees in Germany in 2015. Infection. 2016;44:781–7. https://doi.org/10.1007/s15010-016-0926-7.
Pavlopoulou ID, Tanaka M, Dikalioti S, Samoli E, Nisianakis P, Boleti OD, et al. Clinical and laboratory evaluation of new immigrant and refugee children arriving in Greece. BMC Pediatr. 2017;17:132. https://doi.org/10.1186/s12887-017-0888-7.
Werber D, Hoffmann A, Santibanez S, Mankertz A, Sagebiel D. Large measles outbreak introduced by asylum seekers and spread among the insufficiently vaccinated resident population, Berlin, October 2014 to August 2015. Euro Surveill. 2017;22:30599. https://doi.org/10.2807/1560-7917.ES.2017.22.34.30599.
Hörmansdorfer S, Ackermann N, Berger A, Bischoff H, Bengs K, Rieder G, et al. Infectiological status of asylum seekers and refugees in Bavaria. Hyg Med. 2016;41:D160–4.
Chernet A, Utzinger J, Sydow V, Probst-Hensch N, Paris DH, Labhardt ND, et al. Prevalence rates of six selected infectious diseases among African migrants and refugees: a systematic review and meta-analysis. Eur J Clin Microbiol Infect Dis. 2017;37:605-19. https://doi.org/10.1007/s10096-017-3126-1.
Pottie K, Greenaway C, Feightner J, Welch V, Swinkels H, Rashid M, et al. Evidence-based clinical guidelines for immigrants and refugees. CMAJ. 2011;183:E824–925. https://doi.org/10.1503/cmaj.090313.
Eperon G, Durieux-Paillard S, Mauris A, Chappuis F, Gysin N. Malaria cases in Switzerland from 2005 to 2015 and recent rise of imported Plasmodium vivax malaria. Swiss Med Wkly. 2017;147:w14510. https://doi.org/10.4414/smw.2017.14510.
Herzmann C, Golakov M, Malekzada F, Lonnroth K, Kranzer K. Radiological screening of refugees in Germany. Eur Respir J. 2017;49:1602487. https://doi.org/10.1183/13993003.02487-2016.
Brodhun B, Altmann D, Hauer B, Fiebig L, Haas W. Nationwide analysis in detail. In: Robert Koch Institute, editor. Report on the Epidemiology of Tuberculosis in Germany—2015. Berlin: Robert Koch Institute; 2016. p. 19–63.
Matteelli A, Sulis G, Capone S, D’Ambrosio L, Migliori GB, Getahun H. Tuberculosis elimination and the challenge of latent tuberculosis. La Presse Médicale. 2017;46:e13–21. https://doi.org/10.1016/j.lpm.2017.01.015.
Sandgren A, Schepisi MS, Sotgiu G, Huitric E, Migliori GB, Manissero D, et al. Tuberculosis transmission between foreign- and native-born populations in the EU/EEA: a systematic review. Eur Respir J. 2014;43:1159–71. https://doi.org/10.1183/09031936.00117213.
European Centre for Disease Prevention and Control. Communicable disease risks associated with the movement of refugees in Europe during the winter season. 2015a. http://ecdc.europa.eu/en/publications/Publications/refugee-migrant-health-in-european-winter-rapid-risk-assessment.pdf. Accessed 23 May 2017.
Acknowledgements
The authors thank REFUDOCS-Verein zur medizinischen Versorgung von Flüchtlingen, Asylsuchenden und deren Kindern e.V. for providing the data. This paper is the result of the doctoral thesis of S.M. The authors have no support or funding to report.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest.
Ethical standards
This study has been approved by the ethics committee of the Ludwig-Maximilians-University (LMU), Munich, Germany and has, therefore, been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Additional information
M.A. and S.M. contributed equally to this work.
Rights and permissions
About this article

Cite this article
Alberer, M., Malinowski, S., Sanftenberg, L. et al. Notifiable infectious diseases in refugees and asylum seekers: experience from a major reception center in Munich, Germany. Infection 46, 375–383 (2018). https://doi.org/10.1007/s15010-018-1134-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s15010-018-1134-4