
Abstract
Purpose
Cryptosporidium species is considered to be an important cause of significant morbidity in immunocompromised individuals. A prospective case–control study of sporadic diarrhea due to Cryptosporidium infection was conducted on children with acute lymphoblastic leukemia (ALL).
Methods
Forty children with ALL on maintenance chemotherapy according to the Berlin–Frankfurt–Munster (BFM-90) protocol and 45 sex- and age-matched controls were studied. The ALL group included 25 patients with acute diarrhea and 15 without diarrhea, and the control group included 30 children with acute diarrhea and 15 without. Collected stool specimens were examined using modified Ziehl–Neelsen (MZN) and modified trichrome stains. Serum Cryptosporidium Parvum immunoglobulin G (IgG) antibodies were detected by enzyme-linked immunosorbent assay.
Results
Cryptosporidium oocysts, pathogenic Gram-negative organisms, Giardia lamblia, and Entamoeba histolytica were identified in the stool samples (fecal specimens) of six (24%), eight (32%), four (16%), and two (8%), respectively, of the 25 patients with ALL and actute diarrhea and in one (3%), two (6.5%), six (20%), and five (16.5%), respectively, of the 30 control patients with diarrhea. Serum IgG antibodies were positive in four of the six ALL patients and in one of the control group patients with Cryptosporidium diarrhea who tested positive for oocysts in the stool. Diarrhea duration and severity were greater in ALL patients with stool-positive Cryptosporidium oocysts than in those with non-Cryptosporidium-positive diarrhea (p < 0.000).
Conclusions
Cryptosporidium infection should be considered in children with ALL presenting with prolonged or severe watery diarrhea during chemotherapy, especially those treated with methotrexate and 6-mercaptopurine. Since Cryptosporidium is not routinely tested for in stool examination, a MZN stain is recommended.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
During the past two decades, there has been a progressive improvement in the outcomes for children with acute lymphoblastic leukemia (ALL) in clinical trials, which has resulted in optimized post-induction treatment intensification [1]. Due to the neurotoxicities of cranial irradiation, most ALL protocols are limited to the combination of intrathecal and intravenous methotrexate (MTX) as gold standard for central nervous system (CNS) prophylaxis. High doses of MTX have adverse effects, primarily neutropenia, mucositis, and myelosuppression [2]. The aim of current risk-directed therapy protocols is to improve not only ALL cure rates but also the patients’ quality of life in terms of decreased acute morbidity and long-term sequelae [3]. Treatment-related toxicities represent a major health risk to children with ALL. Bacterial and viral infections, secondary to severe neutropenia and/or immunosuppression, contribute to significant morbidity, hospitalizations, and a 1.7–4.7% incidence of death in remission [4].
Gastroenteritis is common in cancer patients [5]. The diagnosis and treatment of moderate-to-severe diarrhea in patients with cancer is often a challenge because of the variety of infectious and non-infectious causes [6]. Patients with acute leukemia are susceptible to infection at an increased incidence. Neutropenic enterocolitis is an acute, life-threatening inflammation of the small and large bowel and is often seen in children with malignancies during periods of prolonged or severe neutropenia [7]. Patients on immunosuppressive therapy have an increased probability of acquiring parasitic infections, generally with a high degree of severity [8].
Cryptosporidium spp. are a leading cause of diarrhea, particularly persistent diarrhea in children in developing countries [9]. Parasitic infections that cause self-limited diarrhea in immune-competent patients may cause profuse diarrhea in immune-compromised individuals. In such patients, parasites may disseminate to other organs, such as the bronchi, liver, and bile ducts, producing symptomatology specific to the affected organ [10].
Cryptosporidium oocysts are present in 65–97% of surface water (i.e., rivers, lakes, and streams) tested throughout the USA. Transmission of the parasite occurs by the fecal–oral route through the ingestion of oocysts that are shed with the feces of infected hosts [11]. This transmission route together with the resistance of oocysts to environmental conditions and chlorine [12], a large parasite reservoir, and a low infective dose account for the risk of transmission by water [13].
The study reported here was designed to assess the magnitude of Cryptosporidium gastroenteritis in children with ALL who are in remission and on maintenance chemotherapy.
Patients and methods
This study was conducted in the Hematology/Oncology Clinic Children’s Hospital, Ain Shams University. The Pediatrics Ethics Committee of the hospital approved the study and it was performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki. All care-givers of children provided their informed consent prior to the collection of 55 stool specimens from 25 children with ALL and diarrhea and 30 matched controls. Acute diarrhea was defined as three or more loose or watery stools within an 8-h period for <6 days prior to presentation. An episode was considered to have ended when the last day of diarrhea was followed by three consecutive non-diarrheal days. Dysentery was diagnosed when stools mixed with gross blood were observed or reported. Episodes that lasted for >14 days were defined as persistent. Thirty stool specimens were also collected from children without diarrhea: 15 were ALL patients in remission, and 15 were immuno-competent healthy children who were relatives or neighbors of the ALL children and matched for age, sex, social status, and residence. All enrolled children were from rural areas. At the time of specimen collection, families completed questionnaires for each subject in which they provided demographic details and clinical history. Vital signs (temperature, pulse, blood pressure) and the results of a physical examination (including signs of anemia, purpura, mouth ulcers, and signs of dehydration) were recorded. Patients with severe diarrhea and dehydration were treated in-hospital with rehydration measures and, when necessary, appropriate antibiotics were given, based on stool culture results. Children with Cryptosporidium diarrhea were treated for 10 days with azithromycin.
All children with ALL were in remission and on maintenance chemotherapy. None of the enrolled children had neutropenia based on complete blood counts. The Berlin–Frankfurt–Munster (BFM 90) chemotherapy protocol was used to treat ALL. Maintenance therapy was initiated 2 weeks after the end of re-induction. The scheduled dose of 6-mercaptopurine was 50 mg/m2 a day given orally. MTX was given orally at a dose of 20 mg/m2 once a week, with adjustments in dosage made in accordance with the white blood cell (WBC) count (target range 2–3 × 109/L). For all patients, the total duration of therapy was 24 months [14].
Fresh fecal specimens (3 samples from each child, on 3 consecutive days) were collected in clean, labeled, dry disposable plastic cups. All specimens were processed within 2 h of collection for bacterial and parasitological studies. Bacterial isolates were stored for subsequent identification. A direct smear was made for the detection of parasitic infestations [15]; the modified Ziehl–Neelsen (MZN) and modified trichrome stains were used to detect Cryptosporidium spp. [16] and microsporidia [17], respectively. In the active infection, Cryptosporidium oocysts appear as pink entities on a green background following acid-fast staining; during a resolving infection, an increased number of “ghosts” (i.e., non-acid-fast oocysts) are observed (variable staining).
Enteropathogens were investigated by stool cultures. Fecal specimens were inoculated on blood agar, Salmonella–Shigella agar, MacConkey agar (Biofilchem, Roseto, Italy), sorbitol MacConkey agar, and Yersinia selective agar (Oxoid, Basingstoke, UK). Selective and differential media were used for isolating Salmonella, Shigella, Yersinia spp., and Escherichia coli. All plates were examined, and putative colonies of enteropathogenic bacteria were identified by standard biochemical methods (API 20E system; bioMérieux, Marcy-l’Étoile, France) [18]. Stool samples were not examined for viruses.
Serum immunoglobulin G (IgG) antibodies against Cryptosporidium parvum oocysts were detected using an enzyme-linked immunosorbent assay (ELISA) (A8667; Sigma-Aldrich, St. Louis, MO). The cut-off value for the ELISA was determined by estimating the mean optical density of the negative control samples + 3 standard deviations (SD).
Statistical analysis
The Statistical Package for the Social Sciences ver. 9 (SPSS, Chicago, IL) was used for statistical analysis. Differences between groups were tested by analysis of variance (ANOVA), chi-square test (χ2), and the Fisher’s exact two-tailed test was used to detect whether there was a significant association between the different categorical variables. The p value used to indicate the level of significance was set at p < 0.05.
Results
The mean age of the children enrolled in the study was 8.25 ± 3.5 (range 2–15) years. The mean age of the ALL children with Cryptosporidium diarrhea (n = 6) was 8.4 ± 0.66 years, which was comparable to the mean age of 6.9 + 1.79 years of the ALL children with non-Cryptosporidium diarrhea (n = 19) (F = 4.04, p = 0.056). None of the studied ALL children had either neutropenia or eosinophilia at the time of diarrhea.
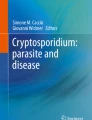
Cryptosporidium oocysts were detected more often in stool specimens of ALL children with diarrhea than in those of the control group with diarrhea [6/25 (24%) vs. 1/30 (3%), respectively; χ2 = 5.24, p = 0.039). Pathogenic Gram-negative organisms were also detected more often in the stool specimens of children with ALL and diarrhea (8/25, 32%; 2 Salmonella typhi, 1 Campylobacter jejuni, 2 Shigella spp., 2 enterotoxigenic Escherichia coli (ETEC), 1 Yersinia enterocolitica] than in the control group with diarrrhea (2/30, 6.5%; 2 with ETEC; χ2 = 5.9, p = 0.032). The prevalence of Giardia lamblia duodenalis/intestinalis (G. lamblia) did not differ between children with ALL and diarrhea (4/25, 16%) and the control group with diarrhea (6/30, 20%) ( χ2 = 0.15, p = 0.74). The Entamoeba histolytica/dispar complex was found in 2/25 (8%) children with ALL and diarrhea and in 5/30 (16.5%) control group children with diarrhea. Cyclospora and microsporidia were not detected in the stool specimens. Serum IgG was positive in 4/6 ALL children whose stool specimen tested positive for Cryptosporidium and in the one control child with Cryptosporidium diarrhea.
No organism were detected in the stool specimens of 5/25 ALL children with diarrhea, 16/30 control children with diarrhea, and in all children without diarrhea whether with ALL or not (healthy control) (Fig. 1).

Organisms detected in stools from children with diarrhea and control groups. ALL Acute lymphoblastic leukemia
The two ALL children whose serum tested negative for Cryptosporidium antibodies but whose stool tested positive for Cryptosporidium oocysts had recurrent attacks of neutropenia, necessitating interruption of the chemotherapy prior the attack of diarrhea. One of these patients had three severe attacks of mouth ulcers and abdominal pains due to MTX therapy (resolved with leucovorin).
When ALL children with diarrhea were compared to the control group with diarrhea, the prevalence of fever was significantly higher in the ALL children with diarrhea (36 vs. 26%, p < 0.001) and the duration of acute diarrhea was significantly longer (20.16 ± 6.3 days vs. 10.8 ± 5.8 days; p < 0.001). Abdominal colic, vomiting, frequency of bowel motions, watery diarrhea, and dehydration were notably higher in ALL children with diarrhea than in the control group with diarrhea. There was no difference in the frequency of fever, vomiting, colic, or stool consistency between ALL children with Cryptosporidium and non-Cryptosporidium diarrhea. ALL children with Cryptosporidium diarrhea had frequent daily diarrheal motions, severe dehydration, and a longer duration of diarrhea compared to children with non-Cryptosporidium diarrhea (Table 1).
Twenty-one ALL children with diarrhea were hospitalized, of whom five had Cryptosporidium diarrhea [1 with persistent diarrhea (>14 days), 2 with persistent high fever, 2 with severe emesis]. All five children with Cryptosporidium diarrhea were treated with nitazoxanide. The two sero-negative children for Cryptosporidium were difficult to treat and responded to azithromycin with stool clearance. Seven ALL children with Gram-negative pathogenic bacteria were hospitalized because of fever, colic, deficient oral intake, and one case of suspected acute appendicitis. Two ALL children with Entamoeba histolytica, three with Giardia lamblia, three with no pathogen detected in their stools, and one with suspected acute appendicitis were hospitalized. All hospitalized children received intravenous fluid therapy and antimicrobial therapy according to the stool culture and sensitivity. Among three of the five ALL children with no detected bacterial pathogen, two improved with ganciclovir treatment. There were two cases of suspected appendicitis among ALL children. One such patient had MTX-induced typhlitis with increased bowel wall thickness based on ultrasonography findings. This was successfully treated with bowel rest (withholding of oral food and fluids) and vancomycin. The second patient had Yersinia enterocolitica enteritis and improved with ceftriaxone treatment. Six ALL children without diarrhea were hospitalized because of fever. The control cases with diarrhea were managed in the rehydration unit as outpatients, except for three who needed hospitalization: one with persistent diarrhea and two with severe dehydration and vomiting. The child with Cryptosporidium diarrhea in the control group did not require hospitalization as the diarrhea resolved spontaneously without antimicrobial treatment after 3 days, as evidenced by clinical improvement and stool clearance.
Discussion
Cryptosporidium oocysts were detected in 6/25 (24%) diarrheal stool specimens from children with ALL. In a previous study, there was a 17.5% incidence of C. parvum oocysts in immune-compromised children with diarrhea, 18.3% incidence in children suffering from protein energy malnutrition, and 7.3% incidence in immune-competent children [19]. Under-notification of infections caused by Cryptosporidium raises the question of whether routine testing should be carried out in all cases of gastroenteritis in children [20].
In our study, diarrhea was more severe in ALL children with Cryptosporidium diarrhea: compared to the controls Cryptosporidium infections in ALL patients were significantly more severe and longer (up to 4 weeks). Similar results have been reported in other studies [21].
Among our patients, stool examination using MZN stain detected detect oocysts in six Cryptosporidium-positive stools of children with diarrhea. However, serum Cryptosporidium IgG tested positive in only four of ALL children with Cryptosporidium-positive stools for oocysts and in the immune-competent control child with Cryptosporidium diarrhea. Other studies have shown the value of stool examination using MZN stain in diagnosing Cryptosporidium (13/35) in immune-deficient cases, with ELISA detecting only 11 cases [22]. Stool examination by MZN stain and PCR was 100% sensitive in both HIV sero-positive and sero-negative patients, with the specificity of antigen detection being 92.2 and 96.3% in human immunodeficiency virus (HIV) sero-positive and sero-negative patients, respectively. Staining techniques have been found to be less sensitive than antigen detection methods and PCR for the detection of Cryptosporidium [23].
In our study, ALL patients were on maintenance chemotherapy. Chemotherapy, especially with MTX and 6-mercaptopurine, has deleterious effects on the gastrointestinal tract. Gwavava et al. [24] noted marked morphological abnormalities in the villus enterocytes by light and electron microscopy examination, with MTX treatment causing striking distention of the lateral basal intercellular spaces, cell vacuolation, and patchy necrosis. These pathological changes were most distinct when the MTX treatment was given 24–72 h before biopsy and may account for the mal-absorption associated with MTX treatment [24]. Toxicity of high-dose methotrexate (HD-MTX) is usually limited to a moderate myelosuppression, reversible mucositis, and moderate hepatic or renal dysfunction. These effects can be substantially reduced via hydration, urinary alkalinization, and the monitoring of renal function and MTX serum concentrations [25]. 6-Mercaptopurine (6 MP) toxicity can also cause neutropenia, diarrhea, and vomiting [26]. Although none of the ALL children in our study had neutropenia during their diarrheal episodes, the two ALL children whose serum tested negative for Cryptosporidium antibodies had recurrent attacks of neutropenia with the interruption of chemotherapy. One of these children had three severe episodes of abdominal pains and mouth ulcers due to MTX therapy (resolved with leucovorin). Studies on impaired MTX elimination, an escalation of the leucovorin rescue, or enzymatic cleavage of the drug by carboxypeptidase in selected cases have succeeded in almost eliminating fatal toxicities [27].
Findings demonstrating specific serum IgG and IgA production in patients infected with Cryptosporidium, both HIV sero-positive and sero-negative, as compared to uninfected subjects [28], suggest the induction of a Cryptosporidium-specific humoral immune response in infected subjects. However, in this study, there was no difference in the number of patients with a positive response in the HIV-seropositive or sero-negative groups, indicating that HIV status may not play a significant role in the modulation of Cryptosporidium-specific antibody responses. The number of patients with positive IgG, IgM and IgA responses was also not significantly different in patients with or without a history of diarrhea, thereby indicating that Cryptosporidium-specific antibody responses may not necessarily be associated with protection from symptomatology [28].
Of the six ALL children with Cryptosporidium diarrhea, five were treated with an antimicrobial agent. The two sero-negative children were difficult to treat. Cryptosporidium diarrhea is self-limiting in immune-competent patients who do not require specific treatment. In immune-compromised patients, however, it is more severe and may be fatal. Various drugs have been tested for the treatment of Cryptosporidium diarrhea in these patients [29]. This severe, prolonged, and difficult-to-treat form of diarrhea was recognized in our study in ALL children with Cryptosporidium diarrhea.
In conclusion, children with ALL are more likely to suffer from severe gastrointestinal manifestations due to the disease itself or infectious and non-infectious complications of chemotherapeutic treatment (especially MTX and 6 MP). Diarrhea in ALL children is difficult to diagnose and treat. Cryptosporidium infection should be considered in cases of severe or prolonged watery diarrhea in ALL children. Since Cryptosporidium is not tested for in a routine stool examination, the laboratory should be notified for diagnostic confirmation using either a MZN stool stain or a more specific diagnostic tool, such as PCR.
References
Schrappe M. Evolution of BFM trials for childhood ALL. Ann Hematol. 2004;83[Suppl 1]:S121–3. doi:10.1007/s00277-004-0850-2.
Moe PJ, Holen A. High-dose methotrexate in childhood all. Pediatr Hematol Oncol. 2000;17(8):615–22. doi:10.1080/08880010050211321.
Pui CH, Robison LL, Look AT. Acute lymphoblastic leukaemia. Lancet. 2008;371(9617):1030–43. doi:10.1016/S0140-6736(08)60457-2.
Hunger SP, Winick NJ, Sather HN, Carroll WL. Therapy of low-risk subsets of childhood acute lymphoblastic leukemia: when do we say enough? Pediatr Blood Cancer. 2005;45(7):876–80. doi:10.1002/pbc.20501.
Bhatti A, Bansal D, Vashishta RK, Lal SB. Isolated gut relapse presenting as chronic diarrhea during maintenance therapy for acute lymphoblastic leukemia. J Pediatr Hematol Oncol. 2010;32(6):504–5. doi:10.1097/MPH.0b013e3181e0159a.
Cherny NI. Evaluation and management of treatment-related diarrhea in patients with advanced cancer: a review. J Pain Symptom Manage. 2008;36(4):413–23. doi:10.1016/j.jpainsymman.2007.10.007.
Rizzatti M, Brandalise SR, de Azevedo AC, Pinheiro VR, Aguiar Sdos S. Neutropenic enterocolitis in children and young adults with cancer: prognostic value of clinical and image findings. Pediatr Hematol Oncol. 2010;27(6):462–70. doi:10.3109/08880018.2010.489934.
Rotterdam H, Tsang P. Gastrointestinal disease in the immunocompromised patient. Hum Pathol. 1994;25(11):1123–40.
Dillingham RA, Lima AA, Guerrant RL. Cryptosporidiosis: epidemiology and impact. Microbes Infect. 2002;4(10):1059–66.
Idris NS, Dwipoerwantoro PG, Kurniawan A, Said M. Intestinal parasitic infection of immunocompromised children with diarrhoea: clinical profile and therapeutic response. J Infect Dev Ctries. 2010;4(5):309–17.
Fayer R, Morgan U, Upton SJ. Epidemiology of Cryptosporidium: transmission, detection and identification. Int J Parasitol. 2000;30(12–13):1305–22.
Bajszar G, Dekonenko A. Stress-induced Hsp70 gene expression and inactivation of Cryptosporidium parvum oocysts by chlorine-based oxidants. Appl Environ Microbiol. 2010;76(6):1732–9. doi:10.1128/AEM.02353-09.
DuPont HL, Chappell CL, Sterling CR, Okhuysen PC, Rose JB, Jakubowski W. The infectivity of Cryptosporidium parvum in healthy volunteers. N Engl J Med. 1995;332(13):855–9. doi:10.1056/NEJM199503303321304.
Schrappe M, Reiter A, Ludwig WD, Harbott J, Zimmermann M, Hiddemann W, et al. Improved outcome in childhood acute lymphoblastic leukemia despite reduced use of anthracyclines and cranial radiotherapy: results of trial ALL-BFM 90 German-Austrian-Swiss ALL-BFM Study Group. Blood. 2000;95(11):3310–22.
Chessbrought M. Medical laboratory manual for tropical countries, 2nd ed. Cambridge: ELBS. Tropical Health Technology and Butterworths; 1987.
Henriksen SA, Pohlenz JF. Staining of cryptosporidia by a modified Ziehl–Neelsen technique. Acta Vet Scand. 1981;22(3–4):594–6.
Ryan NJ, Sutherland G, Coughlan K, Globan M, Doultree J, Marshall J, et al. A new trichrome-blue stain for detection of microsporidial species in urine, stool, and nasopharyngeal specimens. J Clin Microbiol. 1993;31(12):3264–9.
Baron EJ. Rapid identification of bacteria and yeast: summary of a National Committee for Clinical Laboratory Standards proposed guideline. Clin Infect Dis. 2001;33(2):220–5. doi:10.1086/321816.
Osman GA, Makled KM, El-Shakankiry HM, Metwali DM, Abdel-Aziz SS, Saafan HH. Coccidian parasites as a cause of watery diarrhoea among protein energy malnourished and other immunocompromised Egyptian children. J Egypt Soc Parasitol. 1999;29(3):653–68.
Martin-Ampudia M, Mariscal A, Lopez-Gigosos RM, Mora L, Fernandez-Crehuet J. Under-notification of cryptosporidiosis by routine clinical and laboratory practices among non-hospitalised children with acute diarrhoea in Southern Spain. Infection. doi:10.1007/s15010-011-0188-3.
Hunter PR, Nichols G. Epidemiology and clinical features of Cryptosporidium infection in immunocompromised patients. Clin Microbiol Rev. 2002;15(1):145–54.
Hassan SI, Sabry H, Amer NM, Shalaby MA, Mohamed NA, Gaballah H. Incidence of cryptosporidiosis in immunodeficient cancer patients in Egypt. J Egypt Soc Parasitol. 2002;32(1):33–46.
Kaushik K, Khurana S, Wanchu A, Malla N. Evaluation of staining techniques, antigen detection and nested PCR for the diagnosis of cryptosporidiosis in HIV seropositive and seronegative patients. Acta Trop. 2008;107(1):1–7. doi:10.1016/j.actatropica.2008.02.007.
Gwavava NJ, Pinkerton CR, Glasgow JF, Sloan JM, Bridges JM. Small bowel enterocyte abnormalities caused by methotrexate treatment in acute lymphoblastic leukaemia of childhood. J Clin Pathol. 1981;34(7):790–5.
Relling MV, Fairclough D, Ayers D, Crom WR, Rodman JH, Pui CH, et al. Patient characteristics associated with high-risk methotrexate concentrations and toxicity. J Clin Oncol. 1994;12(8):1667–72.
Lennard L, Lewis IJ, Michelagnoli M, Lilleyman JS. Thiopurine methyltransferase deficiency in childhood lymphoblastic leukaemia: 6-mercaptopurine dosage strategies. Med Pediatr Oncol. 1997;29(4):252–5. doi:10.1002/(SICI)1096-911X(199710)29:4<252:AID-MPO3>3.0.CO;2-L.
Widemann BC, Balis FM, Murphy RF, Sorensen JM, Montello MJ, O’Brien M, et al. Carboxypeptidase-G2, thymidine, and leucovorin rescue in cancer patients with methotrexate-induced renal dysfunction. J Clin Oncol. 1997;15(5):2125–34.
Kaushik K, Khurana S, Wanchu A, Malla N. Serum immunoglobulin G, M and A response to Cryptosporidium parvum in Cryptosporidium-HIV co-infected patients. BMC Infect Dis. 2009;9:179. doi:10.1186/1471-2334-9-179.
Trad O, Jumaa P, Uduman S, Nawaz A. Eradication of Cryptosporidium in four children with acute lymphoblastic leukemia. J Trop Pediatr. 2003;49(2):128–30.
Acknowledgments
The authors thank all of the patients who participated in our study. We are grateful to Professor El-Rifai, Wael, Professor of Surgery and Cancer Biology, for his help in revising the manuscript.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Hassanein, S.M.A., Abd-El-Latif, M.M.S., Hassanin, O.M. et al. Cryptosporidium gastroenteritis in Egyptian children with acute lymphoblastic leukemia: magnitude of the problem. Infection 40, 279–284 (2012). https://doi.org/10.1007/s15010-011-0230-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s15010-011-0230-5