
Abstract
Purpose
The main objective of this paper is to determine the predicting factors that influence the intention to use Poison Information System (PIS) among healthcare professionals.
Methods
A quantitative approach was applied, using a five-point Likert scale questionnaire, adapted from previous studies. Data were collected from 167 healthcare professionals working for Malaysian Public Hospitals in Penang. Smart Partial Least Square (PLS) version 3.2.7 were used to analyse the proposed relationships.
Results
The results indicated that attitude and computer anxiety had a significant positive relation to the intention to use PIS among healthcare professionals wherein computer knowledge was found to have had a significant relationship with attitude and computer habit. Apart from that, technical support and training had a positive relationship with perceived ease of use. Surprisingly, computer habit, perceived usefulness, perceived ease of use, compatibility and facilitating condition did not significantly influence intention to use PIS.
Conclusion
The results of this study provided useful insights for healthcare agencies to understand the underlying elements that could improve the poison information management. The results proved that attitude and computer anxiety were critical factors among healthcare professionals managing poisoning cases in a highly stressful and unpredictable work environment. These factors must, therefore, be considered before implementing PIS in managing poisoning cases. The study also provided an understanding of how to improve system development by utilising the end user’s expectation on the implementation of the system.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Poisoning is a major public health problem worldwide. World Health Organization (WHO) estimated 193,460 people died from unintended poisoning worldwide in 2012 with 84% of these deaths occurring in low-and-middle-income countries. In the same year, unintended poisoning resulted in the loss of healthy life of over 10.7 million years [1]. Another research indicated that countries with low incomes and middle incomes (such as Malaysia) have higher poisoning death rates than high-income countries [2]. These poisoning cases, especially from accidental exposures, is sometimes unavoidable. Similarly, in order to detect dangerous trends in the community, a function known as toxicovigilance is carried out by the authorities concerned to regularly evaluate the reported incidences of poisoning at the national level [3]. Figure 1 displays the poisoning prevalence distribution and deaths according to the states in Malaysia. Most northern states in Malaysia, particularly Penang, reported a higher prevalence of poisoning admissions compared to other states, with approximately more than 100 admissions per 100,000 populations [3]. Figure 2 shows that between 2006 and 2015, there was a growing trend of poisoning exposure calls made to the National Poison Centre but noticed a sharp drop in 2012 and a steady rise in 2013 [2].

Prevalence of poisoning admission in Malaysia

Trends of the three most common poisoning exposure agents based on the calls received by the Malaysia National Poison Centre between 2006 and 2015
As reported by another study [4], British Columbia Drug and Poison Information Centre provided poison information using an electronic database system that records case information and data as a potential source of the population-based information on the use of health services and health status. Most poison information centre's performance discussed the centre's role, its existence, the quality of the centre and the recognition of the centre [5,6,7]. Therefore, most studies explained the technical part of poisoning cases which mentioned the number of cases reported, the process of handling the cases, the drug/poison effects, the admission of poisoning cases but very few on the information system they used [8, 9]. There is no study which has thoroughly studied the management of the systems which intend to use or adopt poison information systems among healthcare professionals.
The usage of computer device and internet among the healthcare professionals is high, so it is necessary to know the factors that would attract their intention to use Poison Information System (PIS). By realizing the necessities of healthcare professionals to use PIS, the findings of this study can provide awareness to the management by evolving effective strategies that will enable hospitals to generate new opportunities and values for their clients, increase healthcare staff's efficiency and effectiveness, and to remain competitive in the health industry.
Hence, the purpose of this research is to present a theoretical framework for evaluating the health professional intention to use PIS. Technology acceptance model (TAM) and the Theory of Planned Behaviour (TPB) were used as the theoretical basis for this study along with external variables such as PIS computer knowledge and technical support and training. This research also validated the factors determining the intention of healthcare professionals to use PIS and examined the relationships between these predictor variables.
The structure of this paper is as follows. Firstly, the study rationale and problem statement have been stated followed by the formulation of the research questions and research objectives. The next sections discuss the theoretical background and literature review leading to hypothesis development. The paper then describes research methodology followed by results and discussion. Lastly, the paper concludes by discussing the limitation of the study along with a conclusion and future work.
Problem statement and study rationale
Fourth Industrial Revolution era (IR 4.0) is expected to change how we live, work, communicate and provide information in real-time. Also, the things we value and how we value them in the future are likely to change. But when it comes to the health information system in Malaysia, it is still considered lagging in comparison to other industries. A local poison information system is still lacking in Malaysia. Health organisations still depend on external subscribed poison databases. There is no single organization dedicated to performing toxicovigilance in the country. As such, the country's poisoning surveillance information remains very scattered [3]. To align with IR 4.0, PIS is one of the systems that is expected to provide real-time poisoning information to healthcare professionals.
Research on the intention to use among healthcare professionals is still lacking. Most of the research is only based on clinical research. In addition to that, there are also limited studies on Malaysia’s toxicovigilance in general and specifically on the intention of health professionals to use PIS. Due to the PIS concept, which is still in the initial stage of development, factors affecting health professionals ' intention to use PIS in this area needs to be investigated [10]. While perceived usefulness and ease of use are the key factors most concerned to health professionals, there are other factors that influence the intention of health professionals to use PIS, such as computer knowledge, technical support and training.
Previous literature [3, 11] have shown that a variety of determinants such as self-efficacy, performance expectancy, social influence, perceived usefulness, attitude and so on affect the intention to use the healthcare information system, but this has not been consistently shown in previous research. Several studies in Malaysia have focused on the trend of poisoning cases [11], poisoning admission [3], paraquat poisoning calls to the Malaysia National Poisoning Centre [8], and evaluation of types of poisoning exposure calls. Another study [2] mentioned that future research should include the task of organizing the functions of PIS which remains hugely scattered. Thus, this paper targets this issue by considering the determinants which are common with other researchers in analysing the intention to use PIS among healthcare professionals by integrating two theories of TAM and TPB. In addition to that, this study also introduces two external factors which will influence some of the independent variables.
Theoretical background
In this study, the acceptance of PIS among healthcare professionals was analysed by the terms of intention to use. The research framework assessed the predictive value of both integrated TAM [12] and the TPB [13]. Both integrated theories are foremost theoretical models for such research and have gathered relatively strong empirical support from various end-users and business executives. The acceptance model of technology is a well-established model that has been widely used to predict and explain human behaviour [12]. The main constructs in TAM comprise of perceived ease of use, perceived usefulness, attitude toward using and intention to use. Among these, the most dominant determinants for system use are perceived usefulness and perceived ease of use, with perceived ease of use having a direct effect on perceived usefulness.
The TPB theory assists program implementers in designing interventions that address specific behaviour effectively. Three types of beliefs that tend to guide human behaviour are considered by implementers when using this theory: behavioural, normative and control. The usage of the theory of planned behaviour is to guess a person’s behaviour in a mandatory context, as compared to TAM. Noting this, TPB describes that attitude, subjective norms, and perceived behavioural control are influenced by individual behaviour. Firstly, attitude means the positive or negative feelings of an individual towards a specific behaviour. Then, subjective norms define the perception of an individual as to what other people think about a particular behaviour. Besides that, perceived behavioural control refers to the beliefs of an individual about the resources needed to facilitate behaviour. Research has shown that TPB explains substantial variations in the intention of healthcare professionals to use technology [14]. The previous study also revealed in their systematic review that TPB explained 59% of the variance in the intention of healthcare professionals to adopt different medical practices and systems to underline its suitability for this study [14].
Literature review and hypothesis development
Intention to use
The variable being tested or observed is a dependent variable where its value is determined or dependent on independent variables. The dependent variable of this study is the intention to use PIS among healthcare professionals. The term intention relates to something you want or plan to do, and adoption only relates to initial system or technology acceptance. Based on a previous study [15], the adoption of technology depends on the advantages or usefulness of such technology, its ease of use and, whenever a modernized method is cogitated to be more beneficial than an old-style system of carrying out the same undertakings, its adoption is high. Since PIS implementation is still underdeveloped for healthcare professionals, this research focuses on the intention to use, that will predict possible forcing factors influencing the use of PIS.
Computer knowledge
The level of expertise of an individual with basic computer hardware and software like internet browsers, emails, and Microsoft office tools determines computer knowledge [16]. There is evidence which states that the computer knowledge and skills of healthcare professionals boost positive attitudes towards the use of technology in work environments [17, 18]. Computer knowledge has a positive relationship on their attitude in using health information system [16]. This finding is consistent with several other studies mentioning that computer knowledge continues to be seen as a vital factor in enhancing the acceptance of healthcare technologies [19, 20]. With this, the following hypothesis was proposed:
H1
Healthcare professionals’ computer knowledge has a positive effect on attitude.
H2
Healthcare professionals’ computer knowledge has a positive effect on computer habit.
Technical support and training
The technical support and training mean that the individuals or a group of people provide optimum training of poison management. Technical support such as wireless network infrastructure, hardware facilities, software services and consultancy are very important to support practitioners efficiently and effectively [21]. Technical experts, appropriate training courses, and adequate resources are the types of support needed for health organisations [22, 23]. Thus, the higher chances for technology acceptance is dependent on a higher level of technical support [24]. Based on this argument, the hypotheses are as below:
H3
Technical support and training has a positive effect on perceived usefulness among healthcare professionals.
H4
Technical support and training has a positive effect on perceived ease of use among healthcare professionals.
Attitude
Attitude refers to the positive or negative feelings of an individual towards a particular behaviour [16]. The most direct predecessor of intent is attitude, which is well defined as the negative or positive feelings of an individual about the conduct of expected behaviour [12]. Regarding attitudes in technology content, a previous study [12] states that individuals are inspired to use a system that helps them fulfil their tasks. Previous findings showed that healthcare professionals’ positive attitudes towards the health information system had a tendency of willingness to use these systems at work without any hesitation [25, 26]. Earlier studies [12, 16] have mentioned that the higher usage of intention to use can be influenced by attitude. With this, the following hypothesis was proposed:
H5
Healthcare professionals’ attitude has a positive effect on the intention to use PIS.
Computer habit
Computer habit refers to goal-directed automaticity in the use of the computer [16]. Health information system and related technologies are more widely accepted in work settings by healthcare professionals with well-established computer habits [27]. Previous findings showed that computer habits are positively associated with the use of health information system use [16]. With this, the following hypothesis was proposed:
H6
Healthcare professionals’ computer habit has a positive effect on the intention to use PIS.
Perceived usefulness
Perceived usefulness is defined as the extent to which a healthcare professional believes that by using the health information system, it would enhance and improve their performance [21]. It has been shown that perceived usefulness forms an important effect on the intention of using a technology [27]. TAM theory suggests that perceived usefulness and perceived ease of use are related to the attitude towards accepting new technology, which affects acceptance intention. An earlier study shows that perceived usefulness is a valuable indicator of acceptance of technology [10, 15, 28, 29]. Perceived usefulness in some research has a direct impact on the intention to use and has increased its influence through attitude [27]. Thus, the perceived usefulness of PIS may be critical to the intention to use in addition to various application areas. The hypothesis is defined as follows:
H7
Perceived usefulness has a positive effect on the intention to use PIS among healthcare professionals.
Perceived ease of use
Perceived ease of use has been defined as the level to which a healthcare professional believes that they would be free from physical and mental effort to use health information systems [21]. It is the second key determinant of intention to be used in the original TAM after perceived usefulness [12]. Individuals favour reducing the effort required to do their job [30]. Various studies have validated the important relationship between perceived ease of use and intention to use [10, 15, 21, 31]. Previous studies in diverse organizational settings belief that the effect of perceived ease of use is more likely to have a positive relationship on the intention to use. Consequently, the set of hypotheses are proposed as follows:
H8
Perceived ease of use has a positive effect on perceived usefulness intention to use PIS among healthcare professionals.
H9
Perceived ease of use has a positive effect on the intention to use PIS among healthcare professionals.
Compatibility
Compatibility means the degree to which the prevailing values, past experiences and needs of the healthcare professionals in using health information system is considered consistent [21]. Compatibility is considered to be one of the five major constructs determining the acceptance of innovation [32]. According to another study, compatibility was the first facilitator to shape a positive attitude and use behaviour towards health information system [33]. With this, the hypothesis was proposed as below:
H10
Compatibility has a positive effect on the intention to use PIS among healthcare professionals.
Computer anxiety
Computer anxiety refers to the extent of tension increasing or a sense of nervousness for using health information systems [16]. Anxiety is defined as a personal characteristic and has a negative impact on technology acceptance [34]. Healthcare professionals with little or no fear at all of the computer technology have been shown to be more willing to accept the health information systems [35]. A study has also recognized that if users are anxious about health information systems, they have a tendency to think that their original values are inconsistent with the technological product [36]. With this, the following hypothesis was proposed:
H11
Healthcare professionals’ computer anxiety has a negative effect on the intention to use PIS.
Facilitating condition
Facilitating condition refers to the individuals’ belief of the resources needed to facilitate their behaviour into the intention to use the system [16]. Intention to use was found to positively influence facilitating condition [37]. Previous research has shown a positive effect of facilitating condition towards the intention of use [16, 38,39,40]. With this, the following hypothesis was proposed:
H12
Facilitating condition has a positive effect on the intention to use PIS among healthcare professionals.
Conceptual model
The proposed conceptual model describing the relationship between the predictor variables of intention to use PIS has been shown in Fig. 3. Variables of attitude, computer habit, computer anxiety and facilitating condition are an independent variable for intention to use. Two external variables of computer knowledge and technical support and training are proposed to have a direct effect on the independent variable towards intention to use PIS.

Conceptual model of intention to use PIS among healthcare professionals
Research methodology
Population and sampling
Healthcare professionals managing poisoning cases in Malaysian Public Hospitals are the population for this study. The healthcare professionals include physicians, pharmacists, medical assistants and nurses. Hence, their responses are very important in determining the factors that influence the intention to use PIS.
This study adopted a non-probability sampling technique to collect samples from the population. Since the actual sampling frame was unknown, the purposeful sampling method was applied to select the respondents. Power analysis was used to calculate and determine the sample size of this study. The G*Power was therefore used to calculate the minimum sample size required to perform the data analysis at a confidence level of 95%. To achieve 80% of power [41,42,43], the minimum sample size required for this study was 103 respondents.
Data collection procedure
Survey research is used in explaining the predictors of intention to use PIS and analysing the relationship between constructs. A survey form was created using a paper survey technique as well as free online survey tools such as Google Forms.
The questionnaires were sent through online Google Forms to the respective healthcare professionals who were managing poisoning cases in Malaysian Public Hospitals in Penang. The respondents, however, were very slow to respond even after several reminders were sent. To solve this lack of response, three weeks after the email, a paper survey technique was considered and implemented. A cover letter from Universiti Sains Malaysia, Penang was sent to the hospital managements of Malaysian Public Hospitals in Penang. Hospitals which agreed to pursue the survey were provided with a paper-based questionnaire. The response time given to all the hospitals to complete the questionnaire was 3 weeks. A representative was selected to help with the data collection throughout this research for each hospital. A representative from each hospital sent the questionnaires to their healthcare professionals respectively. Responding to the questionnaire took about 10 min for each respondent. Hence, the sampling of this study comprises of 167 respondents where 122 respondents were collected from a paper survey technique and the remaining 45 respondents were from an online survey.
Measurement of variables
Qualifying questions on the management of poisoning cases were added to the first part of the questionnaire to ensure only the specific healthcare professionals participated. Those who did not handle poisoning cases were excluded. There were 3 types of the scales used in the study such as nominal scale, ordinal scale and Likert scale for the answer options of the questionnaire [44, 45].
The questionnaire consisted of two sections: Section A and B. Section A contains 6 questions on the demographic profile by adopting nominal scale and ordinal scale to collect basic information such as gender, age, education level, etc.
Section B measures the constructs of the proposed conceptual model. The items were adapted from the previous study to confirm the content validity. 5-point Likert-scale was used to measure each item from “Strongly Disagree” to Strongly Agree”. The scales were ranked from 1 to 5 as (1) Strongly Disagree, (2) Disagree, (3) Neutral, (4) Agree, (5) Strongly Agree. The items assessing intention to use, perceived usefulness, perceived ease of use, compatibility and technical and support training were adapted from a previous study [21] whereas, the items for computer knowledge, attitude, computer habit, computer anxiety and facilitating organizational condition were adapted from another study [16].
Data analysis
Demographic data were analysed using IBM SPSS version 23 software. To assess the measurement model and structural model, this study used SmartPLS 3 version 3.2.
Results
Profile of the respondents
Out of 200 questionnaires distributed, a total of 167 were collected, which showed a response rate of 83.5%. Overall, 86 of them were male (51.5%) meanwhile 81 of them were female (48.5%). More than half of the respondents were at the age of 21–30 years (55.7%), 41.3% from 31 to 40 years and only 3% came from 41 to 50 years. There were no respondents above the age of 50 years. In addition to that, the majority of the respondents were medical doctors/officers (n = 64, 38.3%) medical specialist (n = 1, 0.6%), houseman doctors/officers (n = 50, 29.9%), medical assistants (n = 19, 11.4%), nurses (n = 13, 7.8%), pharmacists (n = 16, 7.8%) and others (n = 4, 2.4%). All of them were from the public hospital (100%). Since this study only focussed on those managing poisoning cases, 150 of them were from the emergency department (89.8%), 8 of them from pharmacy department (4.8%), 1 respondent from the medical department (0.6%) and 8 from other practice sites (4.8%). Of the total, 110 respondents had a working experience of fewer than 5 years (69.9%) meanwhile 57 of them had an experience equal to or more than 5 years (34.1%). The profile and demographic details are represented in Tables 1 and 2.
Measurement model
The evaluation for measurement model basically aimed at analysis on the composite reliability (CR), outer loadings, average variance extracted (AVE) and discriminant validity (Heterotrait-Monotrait ratio (HTMT)). According to the literature [46], the variables with a factor loading of 0.7 or above is highly acceptable while outer loading of 0.5 is adequate. Outer loading more than 0.4 is still acceptable for this study as stated by another study [47]. Each indicator between 0.4 and 0.7 should be considered for removal only to increase the composite reliability. Therefore, the values of composite reliability must be higher than 0.7 meanwhile the average variance extracted to be higher than 0.5. When the composite reliability value is less than 0.7, it shows that the theorized model concepts are not evaluated reliably by the item. Besides that, if the value of common variance extracted is below 0.5, the items show a bigger error than the variance illuminated via a hypothesized structure which is presented within the measure. The composite reliability value for each construct is within the range of 0.924 and 0.968 which exceeds the concept value of 0.7. Meanwhile, the common variance extracted value is also within the range of 0.756 and 0.909 which has also exceeded the suggested value of 0.5 [48]. The results of the measurement model are presented in Table 3.
Subsequently, discriminant validity of the model was assessed using Heterotrait-Monotrait ratio (HTMT) which is a more conservative approach [49]. It is also used to detect if the correlation among the measures is overlapping construct. As shown in Table 4 below which was generated in PLS output, all values on HTMT are below 0.85 and 0.900, so there is no discriminant validity issue.
Structural model
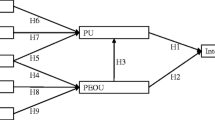
Ten direct hypotheses between the constructs were developed in this study, and two indirect hypotheses between external variables and independent variables were developed. In PLS, R2 measures the coefficient of the determination and the significant level of the path coefficient (beta value). One of the criteria to asses this model is by looking at R2, the endogenous latent values. This is a crucial evaluation to check on the goodness of the model [50]. This study finds, R2 for intention to use is 0.348, which is considered as being above substantial. The R2 value points out that the suggested model explained 34.8% of the variance in the dependent variable—intention to use PIS. The recommended value for R2 is from 0.02 to 0.12 (weak), 0.13 to 0.25 (moderate) and more than 0.26 (substantial) [51]. There were no multicollinearity issues as VIF is less than 3.9, which satisfied the rule of thumb, VIF should be less than 5 (Garson 2016). The structural model has been represented in Fig. 4.

The Structural Model after bootstrapping
In addition, in evaluating R2 value, one should examine the Q2 value as well. This measure indicated the model’s predictive tolerance. In the structural model, Q2 is more than zero, for a certain reflective variable. Q2 value was obtained by using the blindfolding procedure. It is only applicable to endogenous construct, which has a reflective model. To measure this predictive tolerance, the value of an exogenous construct which can be classified as 0.02, 0.15 and 0.35, where the predictive relevance is small, medium or large [48]. In this study, Q2 for endogenous intention to use (Q2 = 0.258) is above zero and has large predictive relevance.
The results shown in Table 5 states that the six hypotheses having a positive relationship and significance towards the intention to use PIS among healthcare professionals are computer knowledge with attitude and computer habit, technical support and training with perceived ease of use, perceived ease of use with perceived usefulness and attitude and computer anxiety with the intention to use. All of these with t-values greater than 1.645, is significant. The other variables are non-significant. Next, the effect size was assessed in the structural model for this study. The f2 value of 0.35 is considered a large effect size, 0.15 considered as medium effect size and 0.02 considered as small effect size [51].
Discussion
An integrated TAM and TPB was taken into account in this study by adding external factors like computer knowledge and technical support and training to investigate the determinants of the intention to use PIS. This study tested the model which incorporated factors and intention to use PIS among healthcare professionals in Malaysian Public Hospitals specifically in Penang area. Based on the analysis, out of 12 hypotheses which were designed, six of them were supported whereas another six were unsupported.
Healthcare professional’s computer knowledge was found to have a significant positive effect on attitude and computer habit toward PIS in the research location. This result is consistent with the viewpoint mentioning that computer knowledge continues to be viewed as an important factor that can enhance healthcare professionals’ intention to use healthcare technologies [16, 52]. Therefore, hypothesis 1 and 2 were accepted.
The technical support and training have a direct positive relationship and significant impact on perceived ease of use which was in contrast with another study [21]. The availability in the healthcare organization of technical support and training is of crucial importance to the success of PIS. Furthermore, appropriate and adequate technical support and training will enable individuals to resolve the uncertainties surrounding them to the intention to use or adoption of the new IT/IS and at the same time improve the self-efficacy of the use of PIS. They will feel physically and mentally effortless to have the intention to use PIS. But healthcare professionals showed the opposite result on perceived usefulness which was insignificant. Hence, a reasonable conclusion can be made that either the organizations may not provide technical support or training effectively and efficiently to healthcare professionals related to PIS, or there might be some problems occurring based on their past experiences which makes them feel lack of satisfaction on using the system. It may comprise of insufficient resources for utilizing the systems. Hence, hypothesis 3 is not supported whereas hypothesis 4 is supported.
Sampled healthcare professional’s’ attitudes toward PIS positively influenced their intention to use PIS at work. The results support the recent study that recommends the positive and significant relationship on attitude toward PIS intention to use [53,54,55,56]. They said that attitude is an important factor which needs additional investigation and possibly specification. Generally, the attitude of a person will be more favourable to a particular behaviour if he or she believes it will result in a positive outcome or prevent a negative outcome. So, healthcare professionals believe that their attitude would influence their intention to use PIS. Thus, hypothesis 5 is supported.
In addition, the results show that computer habit had insignificant influence on intention to use PIS. Computer habit indicates that continuously using the computer becomes the habit of users, as they will utilize PIS effectively. In the course of time, healthcare professionals whose computer behaviours have become spontaneous would not be more likely to use PIS at work. These results are similar to a preliminary study carried out in Spanish [57]. Thus, it showed that healthcare professionals do not trust that their computer usage frequently would not influence their intention to use PIS. This results in disparity [58] to the findings which showed a positive relationship [16]. Hence, hypothesis 6 is not accepted.
Perceived usefulness and perceived ease of use have no significant relation with the intention to use PIS among healthcare professionals in Penang. This can be credited to the complexity of socio-technical healthcare systems which means there is a difference between healthcare users and other industries’ users [59]. Whereas, there is a positive relationship between perceived ease of use towards perceived usefulness which is in contrast to another study [29]. The other study mentioned that the perceived ease of use factor in terms of using new technology is not the main factor to predict the intention to use the system. Another work [12, 30] states that all perceived ease of use and perceived usefulness predict the actual use indirectly through behavioural intent to use. Perceived ease of use is valid when users use this technology or have tried it once. Since there is no prototype for this research, however, users do not have experience on their own instead of imagining it. Therefore, user experience does not perceive this technology to be easy to use. It also has to do with time, the more it is used, the more used to one gets. Therefore, hypothesis 8 is supported whereas hypothesis 7 and 9 are not supported.
The results showed that compatibility is an insignificant factor in intention to use PIS. Thus, the finding is not consistent with previous studies which indicated that a higher level of acceptance can be achieved if a health information system is compatible with healthcare work practices [21, 58, 60, 61]. Obtaining greater success with the intention to use PIS will only happen when healthcare professionals have a higher perception of compatibility with their previous or existing practice processes. It might be insignificant when healthcare professionals find that the new technologies are not familiar or compatible with their experiences and style of living, so they can easily avoid using this technology. In addition to that, they may think that they have to struggle to learn how to use the technology and this process of learning is time-consuming and diminishes the perception of the usefulness of the technology. Consequently, hypothesis 10 is not accepted.
There was a significant negative relationship between healthcare professionals’ computer anxiety with the intention to use PIS. Hence, this result is reliable with studies by healthcare professionals, which includes nurses, which proved that computer anxiety had no effect on the intention to use a specific technology in the terms of like or dislike [16, 29, 36]. So, hypothesis 11 is supported.
Further, the study indicated that facilitating conditions in the organization including infrastructure support, technical and management support is critical to inspiring the intention of healthcare professionals to use PIS implemented in work environments. Although facilitating conditions have been proposed as a positive significant predictor of the intention to use them, the current results reveal that facilitating conditions have a negligible impact on the intention to use PIS. This factor was also found to be insignificant [58, 62,63,64]. This outcome is in contrast with other studies [65,66,67]. Their studies have proven that there is a positive relationship with the intention to use the system. In fact, facilitating conditions in certain cultures and environments cannot have a significant effect on the intention to use PIS because the existing infrastructure does not support such services [63]. Healthcare professionals do not depend on the facilities provided to influence them to use PIS. It can be related to non-availability or availability of a manual or helpdesk in a working environment. It is more related to feeling confident. This result indicated that Penang healthcare professionals who believed their organizations did not have high levels of facilitating conditions that corresponded to high intention and favourable outcomes of use. Consequently, hypothesis 12 is not supported.
Based on the profile of respondents, it is shown that 89.8% of the respondents are from the emergency department and the majority of them are physicians with 68.8% (specialist, medical doctor and houseman). It indicates that their nature of work in the emergency department is very busy and they really got no time to oversee the facilitating condition which the hospital management would provide for the PIS implementation. Besides that, due to their professions, they might have not believed that this PIS will increase their work performance. Even handling system is not a new thing to this profession, they might have a thought that it will be effortless to use. This reason could be why a few hypotheses are not supported such as perceived usefulness, perceived ease of use and facilitating condition. In addition to that, all the respondents 100% are from a public hospital which influenced the research results. As we know, to implement new technology in the government sector needs high financial contribution which is lacking in this era due to budgeting constraints.
Contribution and implications
Managerial implications
The managerial implications from this study are that healthcare organisations and the system developers of any related system should focus special attention to attitude, computer anxiety and computer knowledge as external factors. They should make sure that these predictors are fulfilled so that it can improve the intention to use PIS among healthcare professionals. This research is focused on PIS as in believing health professionals as a potential professional for giving information to the essential parties. Several researchers indicate that health information systems developers and users earn a lot of benefits by supplying this service in the recent market. Hence, this research investigated the factors influencing the intention to use PIS among health professionals in Penang. This research also emphasizes on PIS for health professionals only by which the research findings could be more useful, related and have extended information for health professionals, PIS organization, PIS development organization and other health-related industries.
Theoretical implications
This study extends the knowledge on the intention to use research by using integrated TAM and TPB models in the context of technology intention to use. Here we have introduced the new external factors that influenced some of the independent variables like attitude and computer habit. Based on the theoretical implications, this study is the first to develop and test an intention to use PIS to the best of our knowledge. First of all, findings show that the intention to use is openly influenced by attitude and computer anxiety. Furthermore, this input is a theoretical explanation and a research model developed empirically based on the theory of systems to explain the reason on IT-enabled resources to drive hospital performance in the context of healthcare.
Practical implications
From the healthcare professional’s point of view, this study shed some light on the intention to use and clarified the situation for the professionals when they want to use PIS technology for poisoning cases. Besides that, this research provides useful guidelines for hospital administration. This technology has relied on its attitude and computer anxiety. The technology provider could organize a training course to enhance other aspects including time. Furthermore, it is encouraged for technology developer to pay attention to these aspects to attract the user. Indeed, it is believed that people with higher information on PIS technology will have positive knowledge and skills on PIS technology, thus impacting intention to use PIS among healthcare professionals.
Limitations of the study
Even though this review found useful insights into the factors affecting the intention to use PIS, the interpretation of the results could be constrained due to some of the limitations. Firstly, the data gained from the respondents who are healthcare professionals for this study were only from public hospitals in Penang and not from the private sectors. In addition to that, the upcoming research should collect and compare data from different states in Malaysia so that the results will be more interesting. Second, the PIS exposure in Penang is still in its early stages, not yet implemented and the PIS applications types, standards and the management are still limited. In accordance to that, limited understanding and knowledge of PIS with insufficient applications will only result in a lower intention of the user to use it. Finally, this research only used the quantitative method which may influence the findings. So, the combination between quantitative analysis and qualitative analysis in this type of study might give a different and unique understanding and interpreting the intention to use PIS, since qualitative and quantitative aspects can complement each other in order to provide a better understanding.
Conclusion and future work
Governments around the world in today's digital world have turned their attention to incorporating information and communication technologies tools into their day-to-day activities. Combining TAM and TPB is the essential step to obtain a superior understanding of technology intention to use among healthcare professionals. In addition to that, the theoretical constructs combined into an integrated model can enable multiple variables to be considered as a useful approach to developing a PIS model theoretically. This research aimed to identify the relationship between factors influencing and the intention to use PIS among healthcare professional in Penang by considering computer knowledge and technical support and training as an external factor. Our findings suggest that computer knowledge relationships have a positive and significant effect on the healthcare professional’s attitude. Whereas technical support and training is significant towards perceived ease of use and lastly healthcare professional’s attitude, and their computer anxiety level is significant towards intention to use PIS. Since this research is at the early stage for this topic, future work should include discovering the role of alternative factors, such as external social pressures, perceived behavioural control or age-like moderator, in determining the intention of physicians and other relevant health actors to use health IT systems and eHealth services. Furthermore, providing real operation and experiments in future studies could be considered in order to notify interviewees more about poisoning services. PIS user acceptance factors for individuals with experience using PIS could also be extended to further discuss the intention of adoption. Finally, future study should include respondents from private hospitals or agencies to find out more on the factor that influences this intention to use PIS compared to this study which covers the respondents only from a public hospital.
References
WHO. Poisoning prevention and management. 2016. Retrieved from https://www.who.int/ipcs/poisons/en/. Accessed 23 July 2019.
Tangiisuran B, Jiva M, Ariff AM, Abdul Rani NA, Misnan A, Rashid SM, Dawson AH. Evaluation of types of poisoning exposure calls managed by the Malaysia National Poison Centre (2006–2015): a retrospective review. BMJ Open. 2018;8(12):1–7. https://doi.org/10.1136/bmjopen-2018-024162.
Rajasuriar R, Awang R, Hashim SBH, Rahmat HRBH. Profile of poisoning admissions in Malaysia. Hum Exp Toxicol. 2007;26(2):73–81. https://doi.org/10.1177/096032710707185.
McLean KE, Henderson SB, Kent D, Kosatsky T. Calls to the British Columbia drug and poison information centre: a summary of differences by health service areas. J Public Health Inf. 2014;6(2):e179.
Durigon M, Elliott C, Purssell R, Kosatsky T. Canadian poison control centres: preliminary assessment of their potential as a resource for public health surveillance. Clin Toxicol. 2013;51(9):886–91. https://doi.org/10.3109/15563650.2013.841182.
Karimzadeh I, Vazin A, Talebnia N, Hatami-mazinani N. Performance of drug and poison information center within a Referral University Hospital in Southwest of Iran Performance of Drug and Poison Information Center within a Referral University Hospital in Southwest of Iran. 2018.
Rhalem N, Aghandous R, Chaoui H, Eloufir R, Badrane N. Role of the Poison control centre of Morocco in the improvement of public health. Asia Pac J Med Toxicol. 2013;2(3):82–6.
Leong YH, Ariff AM, Khan HRM, Rani NAA, Majid MIA. Paraquat poisoning calls to the Malaysia National Poison Centre following its ban and subsequent restriction of the herbicide from 2004 to 2015. J Forensic Leg Med. 2018;56:16–20. https://doi.org/10.1016/j.jflm.2018.03.007.
Magalhães AFA, Caldas ED. Underreporting of fatal poisonings in Brazil—a descriptive study using data from four information systems. Forensic Sci Int. 2018;287:136–41.
Vitari C, Ologeanu-Taddei R. The intention to use an electronic health record and its antecedents among three different categories of clinical staff. BMC Health Serv Res. 2018;18(1):1–9. https://doi.org/10.1186/s12913-018-3022-0.
Awang R, Abd Rahman AF, Wan Abdullah WZA, Lajis R, Abdul Majid MI. Trends in inquiries on poisoning: a five-year report from the National Poison Centre, Malaysia. Med J Malay. 2003;58(3):375–9.
Davis F. Perceived usefulness, perceived ease of use, and user acceptance of information technology. MIS Q. 1989;13(3):319–40. https://doi.org/10.1016/S0305-0483(98)00028-0.
Ajzen I. Attitudes, traits and actions: disposition prediction of behavior in personality and social psychology. Adv Exp Soc Psychol. 1987;20:1–57.
Godin G, Bélanger-Gravel A, Eccles M, Grimshaw J. Healthcare professionals’ intentions and behaviours: a systematic review of studies based on social cognitive theories. Implement Sci. 2008;3(1):1–12. https://doi.org/10.1186/1748-5908-3-36.
Seth A, Coffie AJ, Richard A, Stephen SA. Hospital administration management technology adoption: a theoretical test of technology acceptance model and theory of planned behavior on HAMT adoption. Am J Public Health. 2019;7(1):21–6. https://doi.org/10.12691/ajphr-7-1-4.
Ifinedo P. Empirical study of Nova Scotia Nurses’ adoption of healthcare information systems: implications for management and policy-making. Kerman Univ Med Sci. 2018;7(74):317–27. https://doi.org/10.15171/ijhpm.2017.96.
Ifinedo P. The moderating effects of demographic and individual characteristicson nurses’ acceptance of information systems: a Canadian study. Int J Med Inform. 2016;87:27–35. https://doi.org/10.1016/j.ijmedinf.2015.12.012.
Poon EG, Jha AK, Christino M, Honour MM, Fernandopulle R, Middleton B, Kaushal R. Assessing the level of healthcare information technology adoption in the United States: a snapshot. BMC Med Inform Decis Mak. 2006;6:1–9. https://doi.org/10.1186/1472-6947-6-1.
Farokhzadian J, Khajouei R, Ahmadian L. Information seeking and retrieval skills of nurses: nurses readiness for evidence based practice in hospitals of a medical university in Iran. Int J Med Inform. 2015;84(8):570–7. https://doi.org/10.1016/j.ijmedinf.2015.03.008.
Kivuti Wanjuki L, Chepchirchir A. Computerization readiness. Online Journal of Nursing Informatics. 2011;15(1):9. Retrieved from https://phstwlp2.partners.org:2443/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=ccm&AN=2011164327&site=ehost-live&scope=site. Accessed 23 July 2019.
Wu JH, Wang SC, Lin LM. Mobile computing acceptance factors in the healthcare industry: a structural equation model. Int J Med Inform. 2007;76(1):66–77. https://doi.org/10.1016/j.ijmedinf.2006.06.006.
Igbaria M, Zinatelli N, Cragg P, Cavaye ALM. Personal computing acceptance factors in small firms: a structural equation model. MIS Q. 1997;21(3):279–305.
International Program on Chemical Safety & World Health Organization. Guidelines for poison control. World Health Organization. 1997.
Wendland J, Lunardi GL, Dolci DB. Adoption of health information technology in the mobile emergency care service. RAUSP Manage J, RAUSP-07-2018-0058. 2019. https://doi.org/10.1108/RAUSP-07-2018-0058
Huryk LA. Factors influencing nurses’ attitudes towards healthcare information technology. J Nurs Manage. 2010;18(5):606–12. https://doi.org/10.1111/j.1365-2834.2010.01084.x.
Leblanc G, Gagnon MP, Sanderson D. Determinants of primary care nurses’ intention to adopt an electronic health record in their clinical practice. Comput Inform Nurs. 2012;30(9):496–502. https://doi.org/10.1097/NXN.0b013e318257db17.
Shirley T, Todd Peter A. Understanding information technology usage: a test of competing models. information systems research. 1995. Retrieved from https://home.business.utah.edu/actme/7410/TaylorTodd.pdf. Accessed 23 July 2019.
Okcu S, Hancerliogullari Koksalmis G, Basak E, Calisir F (2019). Factors affecting intention to use big data tools: an extended technology acceptance model. Springer, Cham, pp. 401–416. https://doi.org/10.1007/978-3-030-03317-0_33.
Tsai JM, Cheng MJ, Tsai HH, Hung SW, Chen YL. Acceptance and resistance of telehealth: the perspective of dual-factor concepts in technology adoption. Int J Inf Manage. 2019;49:34–44. https://doi.org/10.1016/j.ijinfomgt.2019.03.003.
Venkatesh V. Determinants of perceived ease of use: integrating control, intrinsic motivation, acceptance model. Institute for operations research and the management sciences. 2000.
Gagnon MP, Ghandour EK, Talla PK, Simonyan D, Godin G, Labrecque M. Electronic health record acceptance by physicians: testing an integrated theoretical model. J Biomed Inform. 2014;48:17–27. https://doi.org/10.1016/j.jbi.2013.10.010.
Tornatzky LG, Klein KJ. Innovation charactersitic and innovation adoption-implementation: meta-analysis of the finding. IEEE Trans Eng Manage. 1982. https://doi.org/10.1109/TEM.1982.6447463.
Hung SY, Tsai JCA, Chuang CC. Investigating primary health care nurses’ intention to use information technology: an empirical study in Taiwan. Decis Support Syst. 2014;57(1):331–42. https://doi.org/10.1016/j.dss.2013.09.016.
van Raaij EM, Schepers JJL. The acceptance and use of a virtual learning environment in China. Comput Educ. 2008;50(3):838–52. https://doi.org/10.1016/j.compedu.2006.09.001.
Top M, Yılmaz A. Computer anxiety in nursing: an investigation from turkish nurses. J Med Syst. 2015. https://doi.org/10.1007/s10916-014-0163-5.
Xue L, Yen CC, Chang L, Chan HC, Tai BC, Tan SB, et al. An exploratory study of ageing women’s perception on access to health informatics via a mobile phone-based intervention. Int J Med Inform. 2012;81(9):637–48. https://doi.org/10.1016/j.ijmedinf.2012.04.008.
Venkatesh V, Thong JYL, Xu X. Consumer acceptance and use of information technology: extending the unified theory of acceptance and use of technology. MIS Q. 2012;36(1):157–78. https://doi.org/10.1111/j.1540-4560.1981.tb02627.x.
Bawack RE, Kala Kamdjoug JR. Adequacy of Utaut in clinician adoption of health information systems in developing countries: the case of Cameroon. Int J Med Inform. 2017;109:15–22. https://doi.org/10.1016/j.ijmedinf.2017.10.016.
Wharrad MAH, Windle R. British Computer Society Primary Health Care Specialist Group, Informatics in primary care. J Innov Health Inform. 2018;25(1):027–37. https://doi.org/10.14236/jhi.v25i1.965.
Seethamraju R, Diatha KS, Garg S. Intention to use a mobile-based information technology solution for tuberculosis treatment monitoring—applying a UTAUT model. Inf Syst Front. 2018;20(1):163–81. https://doi.org/10.1007/s10796-017-9801-z.
Abu-shanab E, Pearson M. Internet banking in Jordan: an Arabic instrument validation process. Int Arab J Inf Technol. 2009;6(3):235–44.
Karkonasasi K, Yu-n C, Mousavi SA. Intention to use SMS vaccination reminder and management system among health centers in Malaysia: the mediating effect of attitude. 2011.
Ooi KB, Lee VH, Tan GWH, Hew TS, Hew JJ. Cloud computing in manufacturing: the next industrial revolution in Malaysia? Expert Syst Appl. 2018;93:376–94. https://doi.org/10.1016/j.eswa.2017.10.009.
Dorsey ER, Topol EJ. State of telehealth. N Engl J Med. 2016;375(2):154–61. https://doi.org/10.1056/NEJMra1601705.
Article R. State of Telehealth; 2016. p. 154–161. https://doi.org/10.1056/NEJMra1601705
Henseler J, Ringle CM, Sinkovics RR. The use of partial least squares path modeling in international marketing. Adv Int Mark. 2009;20:277–319. https://doi.org/10.1108/S1474-7979(2009)0000020014.
Hulland J. %3c6. Hulland 1999.pdf%3e. 1999. 204:195–204. https://doi.org/10.1002/(SICI)1097-0266(199902)20:2%3c195::AID-SMJ13%3e3.3.CO;2-Z
Hair FJ Jr, Sarstedt M, Hopkins L, Kuppelwieser GV. Partial least squares structural equation modeling (PLS-SEM). Eur Bus Rev. 2014;26(2):106–21. https://doi.org/10.1108/EBR-10-2013-0128.
Hair J, Hollingsworth CL, Randolph AB, Chong AYL. An updated and expanded assessment of PLS-SEM in information systems research. Ind Manage Data Syst. 2017;117(3):442–58. https://doi.org/10.1108/IMDS-04-2016-0130.
Hair JF, Ringle CM, Sarstedt M. PLS-SEM: indeed a silver bullet. J Mark Theory Pract. 2011;19(2):139–52. https://doi.org/10.2753/MTP1069-6679190202.
Cohen J. Statistical power analysis for the behavioral sciences. New York: Academic Press; 1969.
Kijsanayotin B, Pannarunothai S, Speedie SM. Factors influencing health information technology adoption in Thailand’s community health centers: applying the UTAUT model. Int J Med Inform. 2009;78(6):404–16. https://doi.org/10.1016/j.ijmedinf.2008.12.005.
Dutta B, Peng MH, Sun SL. Modeling the adoption of personal health record (PHR) among individual: the effect of health-care technology self-efficacy and gender concern. Libyan J Med. 2018. https://doi.org/10.1080/19932820.2018.1500349.
Hu PJ, Chau PYK, Sheng ORL, Tam KY. Examining the technology acceptance model using physician acceptance of telem. J Manage. 1999;16(2):91–112.
Lee SY, Lee K. Factors that influence an individual’s intention to adopt a wearable healthcare device: the case of a wearable fitness tracker. Technol Forecast Soc Change. 2018;129:154–63. https://doi.org/10.1016/j.techfore.2018.01.002.
Zhao Y, Ni Q, Zhou R. What factors influence the mobile health service adoption? A meta-analysis and the moderating role of age. Int J Inf Manage. 2017. https://doi.org/10.1016/j.ijinfomgt.2017.08.006.
Asua J, Orruño E, Reviriego E, Gagnon MP. Healthcare professional acceptance of telemonitoring for chronic care patients in primary care. BMC Med Inform Decis Mak. 2012. https://doi.org/10.1186/1472-6947-12-139.
Talukder MS, Chiong R, Bao Y, Hayat Malik B. Acceptance and use predictors of fitness wearable technology and intention to recommend: an empirical study. Ind Manage Data Syst. 2019;119(1):170–88. https://doi.org/10.1108/IMDS-01-2018-0009.
Sherer SA, Meyerhoefer CD, Peng L. Applying institutional theory to the adoption of electronic health records in the US. Inf Manage. 2016;53(5):570–80. https://doi.org/10.1016/j.im.2016.01.002.
Li J, Ma Q, Chan AHS, Man SS. Health monitoring through wearable technologies for older adults: smart wearables acceptance model. Appl Ergon. 2019;75:162–9. https://doi.org/10.1016/j.apergo.2018.10.006.
Meri A, Hasan MK, Danaee M, Jaber M. Modelling the utilization of cloud health information systems in the Iraqi public healthcare sector Telematics and Informatics Modelling the utilization of cloud health information systems in the Iraqi public healthcare sector. Telemat Inform. 2019. https://doi.org/10.1016/j.tele.2018.12.001.
Donaldson LP. Advocacy by nonprofit human service agencies: organizational factors as correlates to advocacy behavior. J Community Pract. 2007;15(3):139–59. https://doi.org/10.1300/J125v15n03.
Farah MF. Mobile-banking adoption: empirical evidence from the banking sector in Pakistan. Int J Bank Mark. 2018. https://doi.org/10.1108/IJBM-10-2017-0215.
Rubin A, Ophoff J. Investigating adoption factors of wearable technology in health and fitness. Open Innov Conf (OI). 2018;2018:176–86.
Hossain A, Quaresma R, Rahman H. Investigating factors influencing the physicians’ adoption of electronic health record (EHR) in healthcare system of Bangladesh. 2019.
Dasgupta S, Gupta B. Espoused cultural values as antecedents of internet technology adoption in an emerging economy. Inf Manage. 2019. https://doi.org/10.1016/j.im.2019.01.004.
Vanneste D, Vermeulen B, Declercq A. Healthcare professionals’ acceptance of BelRAI, a web-based system enabling person-centred recording and data sharing across care settings with interRAI instruments: a UTAUT analysis. BMC Med Inform Decis Mak. 2013;13(1):1–14. https://doi.org/10.1186/1472-6947-13-129.
Acknowledgement
The authors would like to thank Universiti Sains Malaysia, Malaysia for funding this research under the Research University Grant Scheme (1001/PPAMC/8012234).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Iskandar, Y.H.P., Subramaniam, G., Majid, M.I.A. et al. Predicting healthcare professionals’ intention to use poison information system in a Malaysian public hospital. Health Inf Sci Syst 8, 6 (2020). https://doi.org/10.1007/s13755-019-0094-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s13755-019-0094-0