
Abstract
Purpose of Review
Our systematic review aims to assess the overall evidence available in the literature regarding the role of physical activity (PA) in individuals with binge eating disorder (BED) and better understand the potential underlying mechanisms of action.
Recent Findings
Currently, the most effective and well-established psychological treatment for BED is cognitive behavioral therapy (CBT) with a remission rate around 80%. CBT is sometimes combined with pharmacotherapy targeting comorbidities associated with BED, such as obesity and depression. Another avenue of treatment that has been less studied is PA. It has been suggested that PA addresses the underlying mechanisms of BED and, thus, increases treatment efficiency.
Summary
This systematic review provides additional knowledge concerning the benefits of PA in the treatment of individuals with BED including reduction of binge eating (BE) episodes and improvement in other associated comorbidities. Potential mechanisms of action of PA include neurochemical alterations affecting the reward system, reduction of negative affect, and its anorexigenic effects.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Binge eating disorder (BED) is a severe eating disorder characterized by frequent (at least once a week) and persistent (at least 3 months) episodes of eating a large amount of food that are combined with feelings of loss of control over eating and high psychological distress [1]. It is the most common form of eating disorders, since its lifetime prevalence is higher than anorexia nervosa and bulimia nervosa combined, representing 3.5% among women and 2.0% among men [2]. In addition, there is a 5.7% lifetime prevalence of experiencing subclinical BED in both women and men [2], which means that these individuals do not meet all the BED diagnostic criteria but still experience binge eating (BE) episodes accompanied by emotional distress. Furthermore, BED is strongly associated with obesity [3], food cravings [4], and other medical and psychiatric comorbidities [5]. The lifetime prevalence of depression in individuals with BED is approximately 40% [6], compared to 5% [7] in the general population [8]. It has been shown that most BED patients have had at least one additional psychiatric disorder related to mood (49%), anxiety (41%), or substance abuse (22%) during their lifetime [9]. These additional disorders increase health care costs because of greater use of medications and result in a lower health-related quality of life [10]. Overall, BED represents a serious eating disorder associated with many comorbidities. The significant presence of comorbidities along with associated features in BED individuals requires an effective treatment that will target not only the BE problem, but also its wide range of comorbidities related to both physical and mental health [11].
It is well established that BED is caused by a combination of psychological and biological factors. The underlying mechanisms of BED are related to reward system dysfunction, cravings, emotional dysregulation, impulsivity, dietary restraint, and shape and body weight concerns [4]. First, individuals with BED have shown less activation in limbic regions implicated in the reward system when exposed to non-food rewarding stimuli and a hyper-reward response to food cues compared to those without BED [4]. In addition, Wang et al. [12] found that BE scores, but not body mass index (BMI), were associated with increased striatal dopamine release in response to food stimuli. However, because highly processed foods may also act on the dopamine system to decrease reward sensitivity, the role of reward hyposensitivity as a cause and/or effect of BED is unclear [13,14,15]. Second, the triggers of cravings, often observed in individuals with BED [16], may also produce an increased dopaminergic release by stimulating brain areas related to the reward system including the caudate nucleus and insula, amygdala, and hippocampus [17,18,19]. Third, the ineffective modulation of negative affect in BED individuals may induce cravings for highly processed foods and often occur before BE episodes [20, 21]. Indeed, since the 1990s, BE has been suggested as one of the coping mechanisms for emotional dysregulation [22]. Fourth, individuals with BED are known to have an increase in impulsivity, a decreased attention focus, and a higher proneness to make risky decisions associated with inability to guide future behavior using feedback [23,24,25]. An increase in impulsivity is believed to play a role in the initiation of cravings [26], in treatment success, and in remission rates [4]. Fifth, dietary restraint may be one contributing component to BED as a failed attempt to control or overcome the weight gain related to the addictive-like consumption of food [4]. Lastly, shape and body weight concerns can be perceived as a causal mechanism and/or as a consequence of bingeing. Although they appear to increase the risk of developing BED, shape and body weight concerns may also be due to negative outcomes such as weight gain associated with bingeing [4]. In light of these potential mechanisms associated with BED, treatment options which have the possibility to modulate those mechanisms are likely to be effective strategies.
Currently, the most effective and well-established psychological treatment for BED is cognitive behavioral therapy (CBT) [27, 28] with remission rates at approximately 60% [29]. Sometimes, CBT may be combined with pharmacotherapy, which generally includes antidepressants (including selective serotonin re-uptake inhibitors, serotonin-norepinephrine re-uptake inhibitors, tricyclics, and aminoketones), anti-epileptic, anti-obesity agents, anti-cravings or anti-addiction drugs, and/or drugs used for attention deficit hyperactivity disorder [30]. Some research have shown a modest effect of obesity and weight loss drugs (such as orlistat, topiramate, and zonisamide) on weight loss, although those conclusions are restricted to the short-term duration of the trials, high drop-out rates, and substantial placebo-response rates [28, 31]. Conversely, one study showed that the addition of fluoxetine, an antidepressant drug, did not affect the number of BE episodes [32], whereas another suggested that pharmacotherapy alone could also have a moderately positive effect on BE and depressive symptoms [28] in addition to a BE remission rate of 48.7% [31]. Furthermore, the addition of topiramate, an anti-epileptic agent, resulted in a significantly larger abstinence rate of BE compared to a placebo when added to CBT (84 versus 61% abstinence, respectively). However, due to the lack of studies with longitudinal designs, the long-term effectiveness of the addition of pharmacotherapy remains unclear [27].
Although these treatment options demonstrate good efficacy, there are a considerable number of patients who still do not achieve remission, experience side effects (with pharmacology), and, importantly, do not achieve a clinically significant improvement in other BED comorbidities such as obesity, depression, shape and body weight concerns, or anxiety [28]. Therefore, there is a need to investigate novel treatment approaches that target the underlying mechanisms and comorbidities, thus increasing their efficacy. Few experimental studies have used physical activity (PA) in addition to CBT treatment. According to Vancampfort et al. [33], this treatment combination seems to have a positive effect on BE episodes and comorbidities along with various symptoms of BED. Moreover, since individuals with BED also tend to have reduced PA levels or not participate in any exercise [34], PA could improve comorbidities related to BED physical and mental health. PA may also have the potential to influence the reward system [35••] resulting in important effect on BE episodes [36••]. Hence, there is a need to better understand how PA as a treatment approach affects BE as well as mental and physical health symptoms associated with BED and what level of PA may benefit this population. There is limited evidence on this treatment approach and methodologies are diverse. Therefore, this systematic review aims to assess the overall evidence available in the literature regarding the role of PA in individuals with BED and better understand the potential underlying mechanisms of action.
Methods
Search Strategy
This systematic review was conducted using the following online databases: PsychInfo, Medline, SPORTdiscus, and Cumulative Index to Nursing and Allied Health Literature (CINAHL). Our key words were determined by the components of the study question and the outcomes of interest using the “PICO” method—Population (individuals with BED), Intervention or Exposure (PA as a treatment option), Control or Comparator (no PA or other methods of treatment), and Outcomes of interest (BED symptoms, PA levels, and anthropometry measures). Key words for the study were as follows: “male” OR “female” OR “adult” OR “binge eating” OR “binge eating syndrome” OR “night eating” OR “night eating syndrome” AND “physical activity*” OR “exercise*” OR “lifestyle” AND “binge eating disorder symptoms” OR “disinhibition.” Only studies published in English or French until October 4, 2017, were considered for inclusion. The bibliographic database was created using EndNote X8 (Thomson Reuter, PA, USA).
Study Selection
The studies considered for inclusion involved (1) adult participants with BED, (2) PA as a treatment option, and (3) outcomes related to BED symptoms, PA levels, and anthropometry measures. Two independent reviewers (C.B., A.S.-L.) screened citation titles and abstracts for eligible studies, and a third reviewer (V.D.) was involved in resolving any disagreement between the two independent reviewers. Gray literature, books, clinical practice guidelines, commentaries, conference proceedings, editorials, letters, theses, narrative reviews, and systematic reviews were excluded from the study.
Data Extraction and Quality Assessment
Two reviewers (C.B., A.S.-L.) independently extracted data by using a form specifically designed for the review; any disagreements were resolved by a third reviewer (V.D.). The data extracted included details about the interventions, populations, study methods, and outcomes. In addition, for the quality assessment, the reviewers chose to use the risk of bias assessment following the Cochrane Handbook [37] for randomized controlled trials and using the characteristics recommended by Guyatt et al. [38] for observational studies. Further assessment of the quality of evidence following the GRADE method, which includes the risk of bias assessment, would have been inappropriate considering the limited number of included studies and the heterogeneity of the study designs and types of intervention. Two reviewers (C.B., A.S.-L.) independently assessed the risk of bias and any disagreements were resolved by a third reviewer (V.D.). The tool included six domains of risk of bias: selection, performance, detection, attrition, reporting, and any other sources of risk of bias. Seven items were assessed in RCTs (random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessments, incomplete outcome data, selective reporting, and other sources of bias), and six items were assessed in observational studies (participant selection, measurement of exposure, outcome assessment, incomplete outcome data, selective reporting, and other sources of bias). A critical assessment of the risk of bias level (high, low, unclear) was made for each item of the tool.
Results
Study Selection
The initial database search resulted in a total of 749 articles (Fig. 1). The screening phase resulted in the removal of the duplicates (n = 129) and ineligible records (n = 578), which left 43 full-text articles that were assessed for eligibility. Based on inclusion criteria, eight articles were selected for the study. Reasons for exclusion included studies not meeting the PICO criteria, not being an RCT or observational study, or not being published in a peer-reviewed journal (Fig. 1).

Flow diagram of the study selection
Study Characteristics
Study characteristics are shown in Table 1. Of the eight selected studies, five were intervention studies and three were observational studies. Five of the studies originated from the USA [40, 42, 44,45,46], two were from Australia [41, 43], and one was from Switzerland [39]. The duration of the RCTs’ intervention and follow-up periods varied from 12 weeks to 16 months. Most of the studies were conducted in women, i.e., a total of 705 women vs. 137 men were involved in the studies. The mean age of the participants ranged from 36 to 51 years and the average BMI was approximately 34 kg/m2. Also, the average weight of the participants in the four studies reporting this data was 93 kg [39, 43, 45, 46]. Furthermore, the studies assessing BE frequency [42, 43] and PA levels [40, 42] showed that the mean number of BE episodes was 5 days a week and that participants were mostly inactive. In most of the studies, BED was identified with self-reported questionnaires. All the study outcomes were measured using self-reported questionnaires and measures such as weight and height. As for the experimental studies, one had an intervention based on a 1-h length information session on goal setting and benefits of being physically active [40]. Three studies based their intervention on recommendations for light PA practice at home. First, Fossati et al. [39] recommended achieving 30 min of aerobic exercise three times a week. Second, Levine et al. [42] recommended three to five times per week of walking and a weekly caloric expenditure goal of 1000 cal. Lastly, Pendleton et al. [43] recommended performing aerobic exercises such as brisk walking at home three times a week and adding self-monitoring with the possibility of gym training. Furthermore, the study conducted by McIver et al. [41] had an intervention that included 1 h of yoga once a week and a recommendation to engage in a daily 30-min session of home-based practice.
Methodological Quality
The risk of bias assessment made on the five RCT studies (Fig. 2a) revealed that three studies had insufficient information to permit judgment of low or high risk for the random sequence generation and allocation concealment [39, 42, 43]. The other two studies were judged as high risk of bias for having explicitly unconcealed procedures for allocation [40, 41]. Only two studies were classified as a high risk of bias for having no reason for missing outcome data likely to be related to true outcomes, with an unbalance in numbers [41, 42] and one for selective reporting because of a lack of analysis in the control group compared to the intervention group [42]. All the RCTs were assessed as high risk of bias for other sources, such as non-optimal tools to identify BED [40,41,42,43], no comparison of baseline characteristics of participants or an unclear description of allocation group for BED [39], and no report of the number of BED participants in the intervention group [40].

Risk of bias assessment for a RCT intervention studies and b observational studies
For one [44] of the three observational studies (Fig. 2b), the only item judged as high risk of bias was the participant selection, which was made through a convenience sample for only one of the studies. For another observational study [46], all items were judged as high risk of bias except for the absence of missing outcome data. The reasons for the high-risk evaluation were related to the participant selection, lack of evidence of psychometric testing of subjective measures, inappropriate tools to measure outcome variables, and selective reporting. The third observational study was judged as low risk of bias for all items [45].
BED Outcomes
The outcomes of interest for BED-associated symptoms and comorbidities were divided into four categories: (1) BE episodes, (2) depression symptoms, (3) anxiety symptoms, and (4) body image (Table 1). Among intervention studies, results showed that the number of BE episodes was significantly reduced with PA when compared to other interventions [39,40,41, 43]. One study reported that abstinence from BE is related to the increase in PA, reduction of BMI, and improvement in depressive symptoms [43]. Also, the BED exercisers group from that study had twice the rate of abstinence post-intervention (59 vs. 30%) and had less BE episodes at follow-up (16 months) compared to the non-exercisers group [43]. In addition, Levine et al. [42] also reported that all women in the intervention group had a significant increase in PA and decrease in their BE (data not shown) while some women (28.6%) remained non-abstinent from BE post-intervention. Interestingly, they also found that abstinence over time significantly depended on exercise frequency. Similarly, the results from another study revealed a large and statistically significant decrease in the number of BE episodes for the intervention group [41]. Also, Mama et al. [40] showed an abstinence rate of 20% following the intervention compared to 13% in the dietary habits group. Furthermore, all intervention studies found a significant decrease of depressive symptoms with the addition of PA in the treatment of BED [39, 42, 43]. Fossati et al. [39] also found that PA had a significant decreasing effect on anxiety but did not have any effect on body dissatisfaction.
As for observational studies, not all results were similar to those of the intervention studies. With respect to depressive symptoms, Hrabosky et al. [44] found that the Beck Depression Inventory (BDI) score improvements were not related to PA. These authors also reported that higher PA levels in BED participants were associated with lower body shape concern for women. DeBoer et al. [45] found that the effect of anxiety sensitivity on BE episodes can be mediated by PA in different ways depending on the intensity. The association between anxiety sensitivity and BE was significant among individuals who reported engaging in low levels of moderate PA, but not among those who reported high levels of moderate PA. The contrary was observed for vigorous PA. Thus, although this study did not include individuals presenting BED, high levels of moderate PA or low levels of vigorous PA mediated the relationship between anxiety and BE [45].
PA Outcomes
Two experimental studies found that PA interventions involving yoga and aerobic exercises increased their PA levels by twofold their baseline value of PAs compared to the control group [41, 43]. In addition, Levine et al. [42] found that increased PA practice reduced the number of BE episodes and that individuals with BED in the intervention group increased their frequency and overall level of PA. One study observed an increase in moderate- and high-intensity activities post-intervention, but no change was observed in total daily energy expenditure (kcal/day) [39].
Furthermore, observational studies assessing PA practice found that individuals with BED reported PA levels similar to the obese population with or without BED, which is considerably lower than in a community sample [44], and more so during the young adult and adulthood [46].
Anthropometric Outcomes
At least two intervention studies found a significant positive effect of PA on body weight or BMI reduction when compared to control groups post-intervention [39, 41] or at follow-up (10 and 16 months) [43]. In fact, one of these studies showed a clinically significant reduction of four BMI points in the intervention group involving PA [43]. Other studies reported no effect on body weight loss [42], while other did not address weight loss outcomes [40, 41, 43]. In addition, results from the observational study addressing these outcomes suggest that structured PA compared to lifestyle PA (e.g., recreational sports vs. active transportation) weakly predicted body weight in women [44].
Discussion
This systematic review assessed the available data regarding the role of PA in the treatment of individuals with BED. Our results showed that PA has several benefits including the reduction of BE episodes and other aspects relative to BED comorbidities, such as depression and an improvement in physical health. Our review builds on previous work by Vancampfort et al. [47] which focused on RCTs studying the effect of PA in women with BED. There were a limited number of studies addressing this treatment approach in the scientific literature and there were still methodological limitations, mostly due to the reliance on self-reported questionnaires for the classification of individuals with BED. The present systematic review is the first to include not only RCTs but also observational studies in both women and men, which allows a wider perspective on the impact of PA in the treatment of individuals with BED.
Based on our findings, PA appears to be an effective treatment for the reduction of BE episodes as well as abstinence, although the efficacy in the long term remains unknown due to the limited amount of data available. Some promising results from Pendleton et al. [43] included the aspect of self-monitoring which may represent an interesting avenue of research. Similarly, results from the study by Colley et al. [48] showed that the use of heart rate monitors is adequately measuring PA levels and adherence to PA exercises when performed at home, but there was still a compliance problem related to the use of the monitor that needs to be addressed in future studies. In addition, PA appeared effective in decreasing depression and anxiety symptoms in individuals with BED, which was to be expected considering the established literature indicating beneficial effects of exercise on mental health [49].
Even though it was impossible to identify a specific type of exercise that was more effective in BED treatment in light of the present review, it appears that low PA level (e.g., yoga or walking between one to three times per week) is enough to exert a positive impact on BED, at least in the short term. One author hypothesized that moderate PA could exert a protective effect for individuals with elevated anxiety sensitivity through reduced psychological stress reactivity and decreased in negative affect. This would result in a reduction of eating as a coping mechanism and a decrease in the frequency of BE episodes [45]. These results highlight the need for further studies investigating different PA intensities, as well as the mode, frequency, duration, and timing to determine the most influential parameters for individuals with BED. Furthermore, Drenowatz et al. [35••] found that an increase in total exercise time was associated with an increased resistance towards food cravings and that resistance training reduced the probability to act upon those cravings, although those effects were more present in men than women and did not specifically address BED.
Also, according to the present findings, there was an increase in overall PA practice in the intervention groups, but the study designs excluded the possibility to assess the long-term retention of the practice. A previous study by Vancampfort et al. [33] showed that the principal determinants of functional exercise capacity in individuals with BED were the level of sports participation and perceived physical strength, in addition to the severity of depressive symptoms and BMI. Overall PA intervention helped to improve PA levels in individuals with BED, which is positive considering that some studies have found that they tend to have low physical activity level [44, 46].
The findings related to weight loss and BMI showed that aerobic and yoga training resulted in significant but modest reductions in BMI. One explanation for these results is the individual variability in weight changes in response to PA [50]. Accordingly, studies that involve PA intervention will include both responders and non-responders. The latter are likely to influence the magnitude of the outcome, since the results are often reported as mean values [51]. Otherwise, the effect of PA on body composition might also be influenced by the intensity level. For a given level of energy expenditure, high-intensity exercise favors negative energy, lipid balance, and metabolic adaptations in the muscle to a greater extent than lower-intensity exercise [52].
Mechanisms Involved in the Beneficial Effect of PA on BED Treatment
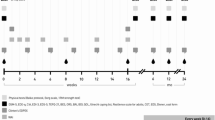
The beneficial effects of PA in the treatment of BED and its comorbidities demonstrated by this review are subject to many potential mechanisms of action (Fig. 3). One potential mechanism is related to the effect of exercise on the reward system. Food is considered as a natural reward that possesses hedonic components, comparable to a substance of abuse, that is a result of conditioning through similar brain pathways, which can be influenced by PA [36••]. Evidence also shows that PA can help decrease cravings [35••] and that food addiction, cravings, and BE share similar pathways, thus supporting this potential mechanism.

Potential acute and long-term effects of physical activity on binge eating
Second, another mechanism may be related to the impact of PA on negative affect. Some studies have shown that PA had a possible effect on neurotransmitters affecting mood, such as serotonin or endorphin secretion, and other neuroprotective functions [49, 53]. The benefits of PA on behavioral strategies allow the reduction of stress and improvement in mood through the hypothalamus-pituitary-adrenal axis [54,55,56,57] and thus address the underlying mechanism by increasing the tolerance to negative affect. Another study by Zschucke et al. [58] suggested that PA could reduce acute cravings based on the knowledge that stress and/or anxiety has been identified as a trigger of BE episodes. Therefore, PA could have an indirect effect on BE through its influence on mood, stress, and anxiety.
Lastly, another potential mechanism is related to improvement in appetite control. There are many exercise-induced physiological processes associated with appetite control, which includes the stimulation of gastric emptying, increase in appetite-related peptides such as peptide tyrosine tyrosine (PYY) and glucagon-like peptide-1 (GLP-1), and a positive balance in substrate oxidation [50]. In addition, the repeated practice of PA affects body composition in terms of lean and fat mass, which provokes changes in resting metabolic rate, and thus influences daily energy intake and thus daily energy needs [59••]. Combined with these processes, the timing of PA could also contribute to decreasing BE episodes. These hypotheses were addressed by studies which found that the anorexigenic effect of PA exists [60••, 61], at least in the short term [62]. The short-lasting action of exercise supports the vision that the optimal timing of PA bouts is before food intake [60••]. These results suggest that PA could have a positive effect if the exercise is performed before the BE episodes or during cravings, to reduce the caloric intake or replace BE episodes.
Limitations
The search strategy used in this study allowed a great reduction of the possible risk of not detecting major studies on the subject, although, as in all systematic reviews, the possibility remains. Also, the quality of evidence of the included studies was down rated because of the risk of bias assessment revealing several methodological flaws. First, there was a common problem related to the blinding of participants and personnel in interventions involving PA [63, 64]. Second, the assessment of the risk of bias revealed the use of inappropriate tools in the identification of BED in participants and evaluation of PA or to differentiate between BE with or without obesity. Indeed, the questionnaires used, although validated, present a risk of substantial error for estimating energy expenditure compared to using an accelerometer [65]. In addition, the use of self-reported measurement tools is subject to recall bias. Third, the diversity of interventions from the experimental studies (in terms of intensity, modality, frequency, and duration of PA) limits overall conclusions relative to the most appropriate intervention for BED individuals. Lastly, the studies that used a cross-sectional design such as observational studies did not allow the establishment of causality in the effect of PA on BED.
This systematic review of the literature highlights the need for future research to focus on high-quality RCTs involving a longer follow-up period to be able to draw firm conclusions concerning the positive effects of PA on BE over time. Future research should design studies which could permit the identification of the best PA characteristics, in terms of intensity, modality, frequency, duration, and timing [43]. Other studies also suggested that future research should assess motivational strategies to help participation and maintenance in PA interventions [47, 58, 66]. It would also be pertinent to address the profile of responders vs. non-responders to PA interventions. In addition, to providing strong results methodologically regarding PA levels, future studies should promote the use of objective electronic measurements, such as accelerometers, to measure physical fitness and allow a better understanding of the dose-response effect of PA in the treatment of BED [43, 45]. Special attention should also be placed on the diagnosis of BED in participants, preferably by a clinician specializing in the assessment of BED, to reduce shared method variance. Future studies should take into consideration the barriers relative to the practice of PA in BED patients. Those limits were related to the elevated costs of exercising (gym memberships) and appropriate sports clothing, the time-consuming and inconvenient schedule aspects of PA, and the negative influence of social environment [46].
Conclusion
This systematic review provided limited and a moderate quality of evidence concerning the positive effect of PA in treatment of individuals with BED on many aspects of its pathology and associated comorbidities. This could be explained by the neurochemical alterations causing changes in the reward system and the reduction of negative effect, as well as the anorexigenic effect of exercise and its timing prior to caloric intake. Future research relying on high-quality design and the use of appropriate tools to identify BED and measurement of PA levels are needed to draw stronger conclusions on the adequate PA interventions for individuals with BED to achieve the most benefits.
References
Papers of particular interest, published recently, have been highlighted as: •• Of major importance
American Psychiatric Association. Diagnostic and statistical manual of mental disorders: DSM-5. 5th ed. Arlington, Virginia. 2013. 947 p.
Hudson JI, Hiripi E, Pope HG, Kessler RC. The prevalence and correlates of eating disorders in the National Comorbidity Survey Replication. Biol Psychiatry. 2007;61(3):348–58. https://doi.org/10.1016/j.biopsych.2006.03.040.
Grucza RA, Przybeck TR, Cloninger CR. Prevalence and correlates of binge eating disorder in a community sample. Compr Psychiatry. 2007;48(2):124–31. https://doi.org/10.1016/j.comppsych.2006.08.002.
Schulte EM, Grilo CM, Gearhardt AN. Shared and unique mechanisms underlying binge eating disorder and addictive disorders. Clin Psychol Rev. 2016;44(Supplement C):125–39.
Treasure J, Claudino AM, Zucker N. Eating disorders. Lancet. 2010;375(9714):583–93. https://doi.org/10.1016/S0140-6736(09)61748-7.
Reichborn-Kjennerud T, Bulik CM, Sullivan PF, Tambs K, Harris JR. Psychiatric and medical symptoms in binge eating in the absence of compensatory behaviors. Obes Res. 2004;12(9):1445–54. https://doi.org/10.1038/oby.2004.181.
Pearson C, Janz T, Ali J. “Mental and substance use disorders in Canada” Health at a Glance. September. Statistics Canada Catalogue no. 82-624-X. 2013.
Kessler RC, McGonagle KA, Swartz M, Blazer DG, Nelson CB. Sex and depression in the National Comorbidity Survey I: lifetime prevalence, chronicity and recurrence. J Affect Disord. 1993;29(2):85–96. https://doi.org/10.1016/0165-0327(93)90026-G.
Grilo CM, White MA, Barnes RD, Masheb RM. Psychiatric disorder co-morbidity and correlates in an ethnically diverse sample of obese patients with binge eating disorder in primary care settings. Compr Psychiatry. 2013;54(3):209–16. https://doi.org/10.1016/j.comppsych.2012.07.012.
Grenon R, Tasca GA, Cwinn E, Coyle D, Sumner A, Gick M, et al. Depressive symptoms are associated with medication use and lower health-related quality of life in overweight women with binge eating disorder. Womens Health Issues. 2010;20(6):435–40. https://doi.org/10.1016/j.whi.2010.07.004.
Kolotkin RL, Westman EC, Østbye T, Crosby RD, Eisenson HJ, Binks M. Does binge eating disorder impact weight-related quality of life? Obes Res. 2004;12(6):999–1005. https://doi.org/10.1038/oby.2004.122.
Wang G-J, Geliebter A, Volkow ND, Telang FW, Logan J, Jayne MC, et al. Enhanced striatal dopamine release during food stimulation in binge eating disorder. Obesity (Silver Spring). 2011;19(8):1601–8. https://doi.org/10.1038/oby.2011.27.
Bello NT, Lucas LR, Hajnal A. Repeated sucrose access influences dopamine D2 receptor density in the striatum. Neuroreport. 2002;13(12):1575–8. https://doi.org/10.1097/00001756-200208270-00017.
Berridge KC. ‘Liking’ and ‘wanting’ food rewards: brain substrates and roles in eating disorders. Physiol Behav. 2009;97(5):537–50. https://doi.org/10.1016/j.physbeh.2009.02.044.
Johnson PM, Kenny PJ. Dopamine D2 receptors in addiction-like reward dysfunction and compulsive eating in obese rats. Nat Neurosci. 2010;13(5):635–41. https://doi.org/10.1038/nn.2519.
Ng L, Davis C. Cravings and food consumption in binge eating disorder. Eat Behav. 2013;14(4):472–5. https://doi.org/10.1016/j.eatbeh.2013.08.011.
Pelchat ML, Johnson A, Chan R, Valdez J, Ragland JD. Images of desire: food-craving activation during fMRI. NeuroImage. 2004;23(4):1486–93. https://doi.org/10.1016/j.neuroimage.2004.08.023.
Volkow ND, Wang G-J, Telang F, Fowler JS, Logan J, Childress A-R, et al. Cocaine cues and dopamine in dorsal striatum: mechanism of craving in cocaine addiction. J Neurosci. 2006;26(24):6583–8. https://doi.org/10.1523/JNEUROSCI.1544-06.2006.
Volkow ND, Wang G-J, Telang F, Fowler JS, Logan J, Childress A-R, et al. Dopamine increases in striatum do not elicit craving in cocaine abusers unless they are coupled with cocaine cues. NeuroImage. 2008;39(3):1266–73. https://doi.org/10.1016/j.neuroimage.2007.09.059.
Berg KC, Peterson CB, Crosby RD, Cao L, Crow SJ, Engel SG, et al. Relationship between daily affect and overeating-only, loss of control eating-only, and binge eating episodes in obese adults. Psychiatry Res. 2014;215(1):185–91. https://doi.org/10.1016/j.psychres.2013.08.023.
Goldschmidt AB, Crosby RD, Cao L, Engel SG, Durkin N, Beach HM, et al. Ecological momentary assessment of eating episodes in obese adults. Psychosom Med. 2014;76(9):747–52. https://doi.org/10.1097/PSY.0000000000000108.
McManus F, Waller G. A functional analysis of binge-eating. Clin Psychol Rev. 1995;15(8):845–63. https://doi.org/10.1016/0272-7358(95)00042-9.
Nasser JA, Gluck ME, Geliebter A. Impulsivity and test meal intake in obese binge eating women. Appetite. 2004;43(3):303–7. https://doi.org/10.1016/j.appet.2004.04.006.
Mobbs O, Iglesias K, Golay A, Van der Linden M. Cognitive deficits in obese persons with and without binge eating disorder. Investigation using a mental flexibility task. Appetite. 2011;57(1):263–71. https://doi.org/10.1016/j.appet.2011.04.023.
Svaldi J, Brand M, Tuschen-Caffier B. Decision-making impairments in women with binge eating disorder. Appetite. 2010;54(1):84–92. https://doi.org/10.1016/j.appet.2009.09.010.
Dawe S, Loxton NJ. The role of impulsivity in the development of substance use and eating disorders. Neurosci Biobehav Rev. 2004;28(3):343–51. https://doi.org/10.1016/j.neubiorev.2004.03.007.
Iacovino JM, Gredysa DM, Altman M, Wilfley DE. Psychological treatments for binge eating disorder. Curr Psychiatry Rep. 2012;14(4):432–46. https://doi.org/10.1007/s11920-012-0277-8.
Vocks S, Tuschen-Caffier B, Pietrowsky R, Rustenbach SJ, Kersting A, Herpertz S. Meta-analysis of the effectiveness of psychological and pharmacological treatments for binge eating disorder. Int J Eat Disord. 2010;43(3):205–17. https://doi.org/10.1002/eat.20696.
Dingemans AE, Spinhoven P, van Furth EF. Predictors and mediators of treatment outcome in patients with binge eating disorder. Behav Res Ther. 2007;45(11):2551–62. https://doi.org/10.1016/j.brat.2007.06.003.
Reas DL, Grilo CM. Current and emerging drug treatments for binge eating disorder. Expert Opin Emerg Drugs. 2014;19(1):99–142. https://doi.org/10.1517/14728214.2014.879291.
Reas DL, Grilo CM. Review and meta-analysis of pharmacotherapy for binge-eating disorder. Obesity. 2008;16(9):2024–38. https://doi.org/10.1038/oby.2008.333.
Grilo CM, Masheb RM. A randomized controlled comparison of guided self-help cognitive behavioral therapy and behavioral weight loss for binge eating disorder. Behav Res Ther. 2005;43(11):1509–25. https://doi.org/10.1016/j.brat.2004.11.010.
Vancampfort D, De Herdt A, Vanderlinden J, Lannoo M, Soundy A, Pieters G, et al. Health related quality of life, physical fitness and physical activity participation in treatment-seeking obese persons with and without binge eating disorder. Psychiatry Res. 2014;216(1):97–102. https://doi.org/10.1016/j.psychres.2014.01.015.
Vancampfort D, De Herdt A, Vanderlinden J, Lannoo M, Adriaens A, De Hert M, et al. The functional exercise capacity and its correlates in obese treatment-seeking people with binge eating disorder: an exploratory study. Disabil Rehabil. 2015;37(9):777–82. https://doi.org/10.3109/09638288.2014.942000.
•• Drenowatz C, Evensen LH, Ernstsen L, Blundell JE, Hand GA, Shook RP, et al. Cross-sectional and longitudinal associations between different exercise types and food cravings in free-living healthy young adults. Appetite. 2017;118(Supplement C):82–9. This review examines cross-sectional and longitudinal associations between different types of exercise and food cravings in adults. It highlights that aerobic exercise, resistance exercise, and total exercise are associated with a decrease in food craving and this is more specifically in men.
•• Hone-Blanchet A, Fecteau S. Overlap of food addiction and substance use disorders definitions: analysis of animal and human studies. Neuropharmacology. 2014;85(Supplement C):81–90. This review presents animal experimental studies and human models supporting the concept of food addiction including the neurobiological similarity between food addiction and substance use disorders. Although the current evidence advocating for human food addiction is inconsistent, this review highlights the share pathways between food addiction, cravings, and binge eating.
Higgins JPT, Altman DG. Assessing risk of bias in included studies. In: Cochrane Handbook for Systematic Reviews of Interventions. John Wiley & Sons, Ltd; 2008. p. 187–241. https://doi.org/10.1002/9780470712184.ch8.
Guyatt GH, Oxman AD, Vist G, Kunz R, Brozek J, Alonso-Coello P, et al. GRADE guidelines: 4. Rating the quality of evidence—study limitations (risk of bias). J Clin Epidemiol. 2011;64(4):407–15. https://doi.org/10.1016/j.jclinepi.2010.07.017.
Fossati M, Amati F, Painot D, Reiner M, Haenni C, Golay A. Cognitive-behavioral therapy with simultaneous nutritional and physical activity education in obese patients with binge eating disorder. Eat Weight Disord. 2004;9(2):134–8. https://doi.org/10.1007/BF03325057.
Mama SK, Schembre SM, O'Connor DP, Kaplan CD, Bode S, Lee RE. Effectiveness of lifestyle interventions to reduce binge eating symptoms in African American and Hispanic women. Appetite. 2015;95:269–74. https://doi.org/10.1016/j.appet.2015.07.015.
McIver S, O’Halloran P, McGartland M. Yoga as a treatment for binge eating disorder: a preliminary study. Complement Ther Med. 2009;17(4):196–202. https://doi.org/10.1016/j.ctim.2009.05.002.
Levine MD, Marcus MD, Moulton P. Exercise in the treatment of binge eating disorder. Int J Eat Disord. 1996;19(2):171–7. https://doi.org/10.1002/(SICI)1098-108X(199603)19:2<171::AID-EAT7>3.0.CO;2-K.
Pendleton VR, Goodrick GK, WSC P, Reeves RS, Foreyt JP. Exercise augments the effects of cognitive-behavioral therapy in the treatment of binge eating. Int J Eat Disord. 2002;31(2):172–84. https://doi.org/10.1002/eat.10010.
Hrabosky JI, White MA, Masheb RM, Grilo CM. Physical activity and its correlates in treatment-seeking obese patients with binge eating disorder. Int J Eat Disord. 2007;40(1):72–6. https://doi.org/10.1002/eat.20323.
Deboer LB, Tart CD, Presnell KE, Powers MB, Baldwin AS, Smits JAJ. Physical activity as a moderator of the association between anxiety sensitivity and binge eating. Eat Behav. 2012;13(3):194–201. https://doi.org/10.1016/j.eatbeh.2012.01.009.
Crandall KJ, Eisenman PA, Ransdell L, Reel J. Exploring binge eating and physical activity among community-dwelling women. Int J Psychol Behav Sci. 2011;1(1):1–8.
Vancampfort D, Vanderlinden J, De Hert M, Adámkova M, Skjaerven LH, Catalán-Matamoros D, et al. A systematic review on physical therapy interventions for patients with binge eating disorder. Disabil Rehabil. 2013;35(26):2191–6. https://doi.org/10.3109/09638288.2013.771707.
Colley RC, Hills AP, O'Moore-Sullivan TM, Hickman IJ, Prins JB, Byrne NM. Variability in adherence to an unsupervised exercise prescription in obese women. Int J Obes. 2008;32(5):837–44. https://doi.org/10.1038/sj.ijo.0803799.
Ströhle A. Physical activity, exercise, depression and anxiety disorders. J Neural Transm (Vienna). 2009;116(6):777–84.
King NA, Horner K, Hills AP, Byrne NM, Wood RE, Bryant E, et al. Exercise, appetite and weight management: understanding the compensatory responses in eating behaviour and how they contribute to variability in exercise-induced weight loss. Br J Sports Med. 2012;46(5):315–22. https://doi.org/10.1136/bjsm.2010.082495.
Boutcher SH, Dunn SL. Factors that may impede the weight loss response to exercise-based interventions. Obes Rev. 2009;10(6):671–80. https://doi.org/10.1111/j.1467-789X.2009.00621.x.
Tremblay A, Simoneau JA, Bouchard C. Impact of exercise intensity on body fatness and skeletal muscle metabolism. Metab Clin Exp. 1994;43(7):814–8. https://doi.org/10.1016/0026-0495(94)90259-3.
Helmich I, Latini A, Sigwalt A, Carta MG, Machado S, Velasques B, et al. Neurobiological alterations induced by exercise and their impact on depressive disorders. Clin Pract Epidemiol Ment Health : CP & EMH. 2010;6(1):115–25. https://doi.org/10.2174/1745017901006010115.
Childs E, de Wit H. Regular exercise is associated with emotional resilience to acute stress in healthy adults. Front Physiol. 2014;5:161.
Dinas PC, Koutedakis Y, Flouris AD. Effects of exercise and physical activity on depression. Ir J Med Sci. 2011;180(2):319–25. https://doi.org/10.1007/s11845-010-0633-9.
Goodwin RD. Association between physical activity and mental disorders among adults in the United States. Prev Med. 2003;36(6):698–703. https://doi.org/10.1016/S0091-7435(03)00042-2.
Stathopoulou G, Powers MB, Berry AC, Smits JAJ, Otto MW. Exercise interventions for mental health: a quantitative and qualitative review. Clin Psychol Sci Pract. 2006;13(2):179–93.
Zschucke E, Heinz A, Ströhle A. Exercise and physical activity in the therapy of substance use disorders. Sci World J. 2012;2012:19.
•• Blundell JE, Gibbons C, Caudwell P, Finlayson G, Hopkins M. Appetite control and energy balance: impact of exercise. Obes Rev. 2015;16:67–76. This study presents a summary of the impact of exercise on the appetite control. It highlights the effect of exercise on body composition, hormone sensitivity, and gastrointestinal peptides on satiety and thus compensatory response which largely depend on the biological responsiveness between individuals.
•• Albert M-H, Drapeau V, Mathieu M-E. Timing of moderate-to-vigorous exercise and its impact on subsequent energy intake in young males. Physiol Behav. 2015;151(Supplement C):557–62. This is the first study that specifically addresses the impact of “timing” of exercise on energy intake. Results revealed a reduced caloric and lipid intake in response to exercise prior lunch compared to delayed exercise and meal in young normal weight males, without any compensation later in the day.
Mathieu ME, Lebkowski A, Laplante E, Drapeau V, Thivel D. Optimal timing of exercise for influencing energy intake in children during school lunch. Appetite. 2018;120(Supplement C):416–22.
Imbeault P, Saint-Pierre S, Almeras N, Tremblay A. Acute effects of exercise on energy intake and feeding behaviour. Br J Nutr. 1997;77(4):511–21.
Mason S, Tovey P, Long AF. Evaluating complementary medicine: methodological challenges of randomised controlled trials. BMJ. 2002;325(7368):832–4.
Ritenbaugh C, Verhoef M, Fleishman S, Boon H, Leis A. Whole systems research: a discipline for studying complementary and alternative medicine. Altern Ther Health Med. 2003;9(4):32–6.
Jacobs DR Jr, Ainsworth BE, Hartman TJ, Leon AS. A simultaneous evaluation of 10 commonly used physical activity questionnaires. Med Sci Sports Exerc. 1993;25(1):81–91. https://doi.org/10.1249/00005768-199301000-00012.
Wolff E, Gaudlitz K, von Lindenberger B-L, Plag J, Heinz A, Ströhle A. Exercise and physical activity in mental disorders. Eur Arch Psychiatry Clin Neurosci. 2011;261(2):186–91. https://doi.org/10.1007/s00406-011-0254-y.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Claudine Blanchet, Marie-Ève Mathieu, Audrey St-Laurent, Shirley Fecteau, Nathalie St-Amour, and Vicky Drapeau declare they have no conflict of interest.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
This article is part of the Topical Collection on Psychological Issues
Rights and permissions
About this article

Cite this article
Blanchet, C., Mathieu, MÈ., St-Laurent, A. et al. A Systematic Review of Physical Activity Interventions in Individuals with Binge Eating Disorders. Curr Obes Rep 7, 76–88 (2018). https://doi.org/10.1007/s13679-018-0295-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13679-018-0295-x