
Abstract
Background
The expression of Heat Shock Proteins (HSPs) is increased in various cancers and has been shown to correlate with biological tumor behaviour. This study aimed to investigate the impact of HSP70, HSP60 and HSP27 expression in colon cancer.
Material and methods
HSP expression was determined by immunohistochemistry on a tissue microarray with 355 primary resected colon carcinomas of all stages. Expression patterns were correlated with pathologic features (UICC pTNM category, tumor grading) and survival.
Results
Expression of HSP27, HSP60 and HSP70 ranged from negative to high. There was no correlation between HSP27, HSP60 and HSP70 expression among each other and with UICC pT category, presence of lymph node or distant metastases or tumor grading. High HSP70 expression was associated with worse overall survival (p < 0.001) and was an independent prognostic factor (p = 0.004) in multivariate analysis including the pathological parameters mentioned above. For patients without lymph node or distant metastases (UICC stages I/II) and with complete tumor excision, HSP70 expression was the only independent prognostic factor for survival (p = 0.001) and superior to UICC pT category. In left sided UICC stage I/II carcinomas, high HSP27 expression also had adverse prognostic impact and was an independent prognostic factor (p = 0.016) besides HSP70 (p = 0.002).
Conclusion
High HSP70 and HSP27 expression is associated with worse clinical outcome in colon cancer. Determination of tumoral HSP70 and HSP27 may be used as additional biomarker for risk stratification especially for UICC stage I/II patients.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
With over 1 million new cases diagnosed per year, colorectal cancer is one of the most common malignancies [1]. Although screening programs and improvement in therapy have resulted in decreasing death rates in most developed countries, in cancer death statistics colorectal cancer still shows in second place for women and third place for men [2]. The therapeutic concepts for colon and rectal cancer mainly are based upon the disease stage ranging from surgery alone for early stage carcinomas to multimodal treatment in advanced stages [3]. The UICC staging [4] represents the most widely used categorization system which bases on clinico-pathological properties, such as tumour size, lymphatic node and organ metastasis. However, there are considerable differences in patients’ outcome even within one single stage. For those cases conventional staging systems fail to predict the prognosis of the patients [5].
In the last years knowledge about the molecular genetics of colorectal cancer has increased significantly. Identification of molecules which may serve as prognostic and predictive biomarkers would greatly help to avoid toxic side effects and unnecessary costs caused by a better selection of patients for individualized therapeutic approaches in addition or instead of the currently used stage based stratification process [6]. Furthermore design of specific drugs against those molecules may help to develop targeted therapeutic approaches.
Heat Shock Proteins (HSPs) are highly conserved proteins, which occur in all types of cells, prokaryotic as well as eukaryotic. They belong to the group of molecular chaperones, whose function is to promote the correct folding of newly translated or denatured proteins. Heat Shock Proteins are sorted into groups according to their molecular weight in kDa. They are also often described as stress proteins, because they are induced by different kinds of pathophysiological stresses, as well as heat shock, and help the cell maintaining its integrity by refolding damaged proteins. In addition, they play an important role in the regulation of apoptosis [7]. It has been suggested, that the expression of Heat Shock Proteins is increased in various cancers. Given their function, it seems likely, that HSPs may influence tumour growth, differentiation and resistance to radio- and chemotherapy and thereby patientś survival [8–11]. The aim of this study was to evaluate the expression of HSP27, HSP60, HSP70 and phosphorylated HSP27 (pHSP27Ser15, pHSP27Ser78, pHSP27Ser82) in colon carcinomas and to analyse its influence on patients’ survival, as well as its association with a variety of pathological parameters including UICC pTNM classification and tumor grading.
2 Materials and methods
2.1 Patients and tissues
Formalin fixed, paraffin embedded archival cancer tissues from 355 patients with colon carcinoma who underwent surgery between 1993 and 2005 at the Klinikum Rechts der Isar of the Technische Universität München (Germany) were investigated. All patients had a primary resection without neoadjuvant radio- or chemotherapy. All patients gave informed consent for the use of additional molecular analysis at the time of operation. The use of archival tissue for molecular analysis was approved by the local ethical commission (No. 2136/08).
2.2 Immunohistochemistry
Immunohistochemistry was performed on formalin-fixed and paraffin-embedded (FFPE) tissue. For preparation of tissue microarrays (TMA) representative tumour sections were marked and a core needle biopsy specimen of 0.6 mm diameter was retrieved and placed in a recipient wax block by using a manual arrayer (Beecher Instruments; Sun Prairie, Wisconsin, USA).
The paraffin blocks were freshly cut (3 μm). After dewaxation and rehydration, heat-induced antigen retrieval using 10 mM citrate buffer, pH 6, was performed. Subsequent to H2O2 blocking using 3 % H2O2 in aqua dest., as well as avidin biotin blocking ( Avidin/Biotin blocking kit, Vector Laboratories, Inc., Burlingame, CA, USA), the sections were incubated with antibodies for HSP70 (mouse monoclonal; prediluted; dilution 1:1; Abcam, Cambridge, UK), HSP60 (rabbit polyclonal; dilution 1:2000; Abcam, Cambridge, UK), HSP27 (mouse monoclonal; dilution 1:250; Cell Signaling Technology, Inc., Boston, MA, USA), pHSP 27Ser78 (rabbit polyclonal; dilution 1:500; Cell Signaling, Inc., Boston, MA, USA), pHSP 27Ser82 (rabbit polyclonal; dilution 1:100; Cell Signaling, Inc., Boston, MA, USA) or pHSP 27S15 (rabbit polyclonal; dilution 1:500; Abcam Cambridge, UK), followed by secondary biotinylated antibody. Immunodetection was performed with the Dako REAL™ Detection system Peroxidase/ DAB+kit (DAKO, Glostrup, DK). Appropriate positive and negative controls were included in each reaction.
Expression of HSPs (Fig. 1) was almost entirely cytoplasmic, so that only cytoplasmic staining was evaluated to determine HSP expression. This was assessed based on the intensity of immunostaining and the percentage of stained tumor cells. The intensity was scored as 0 (no immunostaining), 1 (weak immunostaining), 2 (moderate immunostaining) or 3 (strong immunostaining). The percentage of nuclear positive tumour cells was scored as 0 (none), 1 (<10 %), 2 (10–50 %), 3 (51–80 %) or 4 (>80 %). Multiplication of the scores for intensity and percentage resulted in a staining index (immunoreactivity score; IRS) ranging from 0 to 12. The distributions of the IRS for all HSPs are given as electronic supplemental material (supplement 1). In a second step we searched for optimal thresholds for a classification of HSP expression. This was done by analysing the median, the terciles and the quartiles as cut off in order to achieve groups of equal size. Next, all these divisions were correlated with survival. The distribution into terciles (i.e. three groups of comparable sizes) was shown to reveal the most significant prognostic information with respect to overall survival (data not shown). Accordant to this, the expression of HSPs was then divided into low—moderate—high: For HSP 27 staining index of 0 was defined as low, of 1–2 as moderate and 3–12 as high (Fig. 1A-C). Concerning phosphorylated HSP for pHSP27S15 staining index of 0 was defined as low, 1–2 as moderate and 3–12 as high. For pHSP27Ser78 and pHSP27Ser82 only two groups were built: 0 as staining negative and 1 as staining positive. For HSP70, a staining index of 0–1 was defined as low, a staining index of 2–3 as moderate, of 4–12 as high (Fig. 1D-F). For HSP 60 expression staining index of 0–4 was defined as low, of 6 as moderate and of 8–12 as high.

Examples of immunohistochemical stainings for HSP27 and HSP70 in colon carcinomas (magnification x200). a low HSP27 expression (immunoreactivity score IRS = 0), b moderate HSP27 expression (IRS = 2), c high HSP27 expression (IRS = 9); d low HSP70 expression (IRS = 0), b moderate HSP70 expression (IRS = 3), c high HSP70 expression (IRS = 8)
To ensure the reliability of the staining results obtained from TMAs we compared HSP70, HSP60 and HSP27 immunohistochemical stainings of whole tumor sections with corresponding TMA cores. For that purpose, a test-TMA was constructed from 28 gastrointestinal tumors (4 esophageal squamous cell carcinomas, 4 esophageal adenocarcinomas, 10 gastric carcinomas and 10 colon carcinomas) which contained 3 cores of each tumor for comparison of the staining results of the three TMA cores with each other. Moreover, evaluation of HSP expression was performed by at least two independent observers (KB, JSH, ED, RL) and discrepancies were discussed on a multihead microscope to gain a final consent.
2.3 Statistical analysis
IBM SPSS 19.0 Statistics statistical software (SPSS Inc., Chicago, IL, USA) was used for statistical analysis. Associations between immunohistochemical expression patterns and pathological features were given in crosstabs and were evaluated with X² test. Correlations between staining results were determined by Spearman’s correlation analysis. Differences between the test-tissue microarrays were analyzed using the Friedman test. Survival analysis was performed using Kaplan-Meier estimates, log rank tests and Cox’s proportional hazards regression analysis. All tests were 2-sided, and the significance level was set at 5 %.
3 Results
3.1 Patients and pathologic findings
Two hundred of the patients were male (56 %), 155 female (44 %). The mean age was 65 ± 12 years (median: 66, range: 25 to 91). For the purpose of this study, all tumors were reclassified according to the current UICC TNM-classification [4]. Twenty one tumors were adjudged as pT1 (5.9 %), 62 as pT2 (17.5 %), 193 as pT3 (54.4 %) and 79 as pT4 (22.3 %). Lymph node metastases (pN1abc-pN2ab) were present in 140 (39.4 %) and organ metastases in 56 patients (15.8 %). 292 patients (82.3 %) had left sided carcinomas, 63 patients (17.7 %) had right sided carcinomas. Tumor grading was G1 (well differentiated) in 3 cases (0.8 %), G2 (moderately differentiated) in 230 cases (64.8 %) and G3-G4 (poorly differentiated) in 122 cases (34.3 %) (Table 1). Mean overall survival of all patients was 65 ± 37.7 months. Mean follow up time for surviving patients was 87 ± 27.6 months.
3.2 HSP expression in colon carcinomas
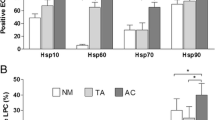
There was no significant difference in the staining results between the three TMA cores of the test-TMA for all HSPs investigated. Demonstrating homogenous staining patterns, the large TMA of colon carcinoma samples could be analysed for HSP27 and pHSP27 (pHSP27Ser15, pHSP27Ser78, pHSP27Ser82), HSP60 and HSP70. For HSP70 353 cases were evaluable: 96 (27.2 %) showed low, 116 (32.9 %) moderate and 141 (39.9 %) high staining intensity (Table 2) 351 cases were evaluable for HSP60: 108 (30.8 %) with low, 24 (6.8 %) with moderate and 219 (62.4 %) with high staining intensity (Table 3). 350 cases were analysed for HSP27 expression: 169 (48.3 %) showed low, 103 (29.4 %) moderate and 78 (22.3 %) high staining intensity (Table 4). For pHSP27Ser15 351 cases were evaluable, 135 (38.5 %) showed low, 111 (31.6 %) moderate and 105 (29.9 %) high staining intensity. For pHSP27Ser78 and pHSP27Ser82 350 cases and 342 cases, respectively could be analysed. Only 4 (1.1 %) were staining positive for pHSP27Ser78 and 32 (9.4 %) for pHSP27Ser82. There was no significant correlation between HSP70, HSP60 and HSP27 expression. In contrast, significant correlations could be observed between HSP27 and pHSP27s (p < 0.001 each).
3.3 Association between clinicopathological parameters and HSP expression
HSP27, HSP60 and HSP 70 expression was neither associated with tumor category (UICC pT category), nor presence of lymph node metastases or distant metastases (Tables 2, 3 and 4). In contrast, low HSP27Ser15 expression was associated with absence of lymph node metastases (p = 0.048) and low HSP 27Ser82 expression was associated with the absence of distant metastases (p = 0.005). Moreover, low HSP 27Ser82 expression was associated with better tumor differentiation grade (p = 0.039) (data not shown).
3.4 Association between patient survival and HSP expression
In univariate analysis, the factors UICC pT category, presence of lymph node or distant metastases at the time of surgery, resection status, tumor differentiation (grading) and HSP70 expression were associated with patients’ overall survival (p < 0.001 each, Fig. 2A). High HSP27 expression was also associated with poor prognosis. This did not reach statistical significance (p = 0.185, Fig. 2B) for the whole cohort, but in the group of patients with left sided carcinomas (p = 0.023). In multivariate analysis, the factors higher pT category (p = 0.019), presence of lymph node metastases (p < 0.001) or distant metastases (p = 0.008), incomplete tumor resection (p = 0.019) and high HSP70 expression (p = 0.007) were independent adverse prognostic factors for overall survival (Table 5A). Tumor localisation per se had no impact on patients’ prognosis (p = 0.314). In left sided carcinomas (n = 282), high HSP27 expression also was an adverse independent prognostic factor, in addition to high HSP70 expression (p = 0.008), pT category (p = 0.019), lymph node metastases (p < 0.001) and distant metastases (p = 0.019) (Table 5B). Subgroup analysis of UICC stage I/II patients (n = 210) revealed HSP70 expression as the only independent prognostic factor besides resection status (p < 0.001 and p < 0.007, respectively; Fig. 2C, Table 5C), which was superior to the depth of tumor invasion (UICC pT category; p = 0.632). This was also the case when regarding left sided UICC stage I/II carcinomas only. In this particular group of patients (n = 175), high HSP27 expression also had adverse prognostic impact (Fig. 2D) and was independent prognostic factor (p = 0.013) besides HSP70 (p = 0.002; Table 5D).

HSP70 and HSP27 expression in colon carcinomas and overall survival. a HSP70 expression in all patients, b HSP27 expression in all patients, c HSP70 expression in UICC stage I/II carcinoma patients, d HSP27 expression in left sided UICC stage I/II carcinoma patients
We furthermore investigated whether the fact that the patients of our collection have been operated and treated during a long time period between 1993 and 2005 might introduce a certain bias for survival analysis. We additionally performed separate survival analysis for the cases from 2001 to 2005 (i.e. older than 5 years, n = 217) and 1993–2000 (i.e. older than 10 years; n = 138). In the first group, HSP70 maintained its prognostic significance (p = 0.001), in the latter, however, the survival curves came closer when regarding the long term survival. For this specific subgroup, this had a negative impact on total significance (p = 0.25). However, when analyzing UICC stage I/II tumors only, in both groups there was a significant correlation between HSP70 expression and survival (p = 0.003 and p = 0.049, respectively). For HSP27, where the most important findings were obtained in the group of left sided, non-metastasized tumors, there were similar findings. However, the difference in the 1993–2000 group was nearly significant (p = 0.082), and in the 2001–2005 group it was clearly significant. (p = 0.016). The survival curves of this analysis are given as supplemental material (supplement 2).
4 Discussion
We present a study about the expression of the heat shock proteins HSP27, HSP60 and HSP70 in a large collection of patients with primary resected colon carcinomas and the correlation of the expression patterns with pathologic features and patient survival. Increased expression of heat shock proteins has been reported to occur in many human malignancies and to show association with biological tumor behavior [8–10]. For colon and colorectal carcinomas there are scare data about the association between HSP60 expression and the presence of lymph node metastases in a small study [12]. Data about HSP70 expression in human cancer tissue exist in a slightly more extent: HSP70 expression has been reported to be elevated in colon cancer in several, albeit small studies, indicating an association of high HSP70 expression with aggressive tumor behavior [13–15]. Interestingly, externalization of HSP70 onto the cell membrane has been proven to be tumor specific in colon cancer cells and appears to correlate with patient prognosis [16]. In another study, high serum HSP70 levels were associated with poor clinical outcome of colon cancer patients [17]. However, the neoplastic origin of soluble HSP70 has not been proven yet and systemic mechanisms like the immunoresponse of the host towards cancer cells may cause increased HSP70 levels in non-neoplastic cells as well.
In our study, high expression of HSP27 was observed in 22 % of the cases, high HSP60 expression of HSP60 was observed in 62 % of the cases and high tumoral HSP70 could be detected in 40 %. We also investigated phosphorylation of HSP27 which could be observed for pHSP27Ser15 in over 60 % of the cases with 30 % showing high staining intensity. For pHSP27Ser78 and pHSP27Ser82 only small subsets of cases showed immunoreactivity. We could not demonstrate significant associations between clinicopathologic features like UICC pT or pN category and HSP27, HSP 60 or HSP70 expression, only an association between the presence of lymph node and distant metastases and the phosphorylation of HSP27, indicating an influence of aggressive tumor behaviour on phosphorylation of stress proteins. Therefore we were not able to reproduce some findings of others in our large cohort of colon cancer patients. However, and most importantly, we were able to demonstrate the prognostic value of high HSP70 expression, which was associated with worse clinical outcome of the patients. HSP70 expression was shown to be an independent prognostic factor in the whole patient cohort and even more in the group of UICC stage I/II patients. According to current therapeutic concepts this group of patients usually is treated by surgery alone, while in stage III tumors surgical resection followed by adjuvant chemotherapy is the currently recommended treatment. In stage II disease, however, the role of adjuvant CTX remains controversial due to its limited efficacy but potentially adverse effects on the other hand. However, it is recognized that up to 30 % of stage II patients will experience recurrence after resection. Clinical staging alone seems to have limitations as the only determinant of treatment strategies [18–20]. Many morphologic or molecular biomarkers have been investigated, but unfortunately, at present none of them have been proven to provide sufficient prognostic information which would allow to serve for risk stratification in these patients [5, 6]. In this context we consider the association of high tumoral HSP70 expression with bad clinical outcome as a promising observation that allows to identify prognostic biomarkers for colon cancer; in particular, as this findings were apparent especially in the subgroup analysis of patients without lymph node or distant metastases (i.e. UICC stages I/II), where HSP70 expression was independent prognostic factor for survival and superior to UICC pT category. Patients of this subgroup with high tumoral HSP70 levels may be candidates for adjuvant treatment (e.g. chemotherapy, or targeted therapies, see below) because of their increased risk for disease related death.
Interestingly, we also could demonstrate a significant association between high HSP27 expression and poor prognosis. However, this phenomenon could only be found in the cohort of patients with left sided carcinomas. Tweedle at al. report that overexpression of HSP27 was associated with poor survival in rectal cancer [21], which is in line with our findings. This interesting finding may be explained by the different genetic molecular background of right sided vs. left sided colon cancer with microsatellite instability and CpG island methylator phenotypes on the one hand and chromosomal instability on the other hand [22, 23], and the closer genetic similarity of left sided colon cancer to rectal cancer. In contrast to HSP70, the biological effects of HSP27 may therefore differ depending from the interaction with the genes involved in carcinogenesis. Nevertheless, our findings could also confirm the impact of HSP27 on tumor behavior in colon and rectal cancer.
We determined the expression of HSPs by immunohistochemistry, which showed a cytoplasmic staining for all HSPs and which could be characterized by using a semi-quantitative immunoreactivity score. We did not observe a specific membranous staining which could be indicative for a externalisation of HSP70 as it has been described by Pfister et al. [16]. However, our findings support the observation that cytoplasmic HSP levels have impact on patients prognosis, and tumor cell specific HSP expression can visualised by immunostaining.
If applied carefully, immunohistochemistry is a very simple and useful tool which provides valuable information about protein expression. On the other hand, however, one has to consider, that estimation of the intensity of immunoreactivity is error-prone with respect to reproducibility and representativeness—especially when applied on a tissue microarray (TMA). We tried to face these problems by a) using a semiquantitative scoring, which provides more detailed information as compared to simple estimation of staining intensity, b) by evaluation of at least two independent observers and gaining final diagnosis on a multihead microscope in case of divergency, c) assessment of the representativeness of TMA cores by comparison with whole slides in a test array. The latter also was done in order to investigate intratumoral heterogeneity of HSP expression, which may be the source of a technical bias. We did not observe significant intratumoral heterogeneity in the test-array, so that we consider our TMA approach as appropriate. Finally, we chose the thresholds for the determination of the expression levels after careful analysis of raw data (i.e. immunoreactive scores) with respect to a plausible distribution and their prognostic relevance.
A second potential limitation of our study is the fact that our collection generated from cases which have been operated and treated between 1993 and 2005. This might introduce a certain bias for survival analysis. In order to investigate this influence we additionally performed separate survival analysis for early and late cases. There were only some discrepancies for HSP70 when comparing early cases with late cases, i.e. closeness of the survival curves in the long time follow up, but the main results of the study with regard to the clinical relevance of HSP70 and HSP27 as a prognostic biomarker retained their significance. Furthermore, these results also suggest that the main prognostic impact of HSP70 or HSP27 expression may be within the first 5 years after surgery. However, this is the period when early relapse of disease occurs and may be eventually fatal—in contrast to longer follow up times when also comorbidities may influence survival.
High expression of HSPs in tumors also may influence their responsiveness towards targeted anti-HSP therapies or conventional antitumoral therapies like chemotherapy and radiation [10]. We have demonstrated that high HSP27 expression was associated with better tumor response to neoadjuvant chemotherapy in esophageal adenocarcinomas [24]. In cell line experiments, upregulation of HSP27 and downregulation of HSP60 and 70 was observed in colon cancer cell lines after 5FU treatment [25], and high pretreatment HSP27 expression was associated with 5FU resistance [26]. Choi et al. report a correlation of high HSP27 expression and decreased sensitivity to irinotecan of colon cancer cells, which was also confirmed by tissue based analysis of cancer specimens of a small patient cohort [27]. Notwithstanding, there is still a lack of a comprehensive investigation about the role of HSPs concerning response to conventional adjuvant or neoadjuvant treatment in colon and rectal cancer, respectively.
In the last years, novel therapeutic agents which direct to the inhibition of heat shock proteins have been developed and have already been emerged as powerful anti-tumoral agents in preclinical settings [28, 29]. The most investigated drugs are Geldamycin (17-AAG) and radiciol which act as an inhibitor of HSP90. These substances have been demonstrated to have antitumoral effects alone, and dependent from or interacting with other molecules like HER2 and EGFR [29–31]. Clinical studies of HSP90 inhibitors alone and in combination with other chemotherapeutic drugs are underway. For HSP70 it would be desirable to overcome the bad prognostic impact of elevated HSP tumoral levels which are associated with an anti-apoptotic effect by inhibition of the molecule. Anti-HSP70 like substances like quercetin and triplotide have been developed and caused inhibition of tumor growth in pancreatic and colon cancer cells in vitro [32–34]. Similar experiments have been conducted concerning HSP27 inhibition [28]. However, this approach has emerged to be challenging due to the structural complexity of this molecule [29] including the frequently observed phosphorylation state which also could be observed in our study. Therefore, although representing a promising approach, the application of HSP27 inhibitors, as well as of HSP70 inhibitors—alone or as combination with other anticancer drugs—has not reached preclinical levels yet.
In summary, we detected the expression of HSP27, HSP60 and HSP70 in a significant subset of colon carcinomas. High HSP27 and HSP70 expression could be demonstrated to be associated with worse clinical outcome, which was particularly the case when regarding left sided, non-metastasized carcinomas only. Therefore, determination of tumoral HSP27 and HSP70 may be used as additional biomarker for risk stratification or therapeutic decisions (e.g. adjuvant chemotherapy) in colon cancer patients especially in UICC stage I/II patients. Our findings warrant validation of the impact of HSP 27 and HSP70 expression in an independent collective of colon carcinomas. Moreover, a potential role of HSP27 or HSP70 expression concerning response to conventional chemotherapy and/or HSP targeted therapies may also be the target of future investigations.
References
J. Ferlay, H.-R. Shin, F. Bray et al., Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int. J. Cancer 127, 2893–2917 (2010)
A. Jemal, R. Siegel, E. Ward et al., Cancer statistics, 2009. CA Cancer J. Clin. 59, 225–249 (2009)
D.V.T. Catenacci, M. Kozloff, H.L. Kindler, B. Polite, Personalized Colon Cancer Care in 2010. Semin. Oncol. 38, 284–308 (2011)
L. Sobin, M.L. Gospodarowicz, Ch Wittekind, TNM classification of malignant tumors (John Wiley & Sons, New York, 2010)
M.G. Mutch, Molecular profiling and risk stratification of adenocarcinoma of the colon. J. Surg. Oncol. 96, 693–703 (2007)
S. Tejpar, M. Bertagnolli, F. Bosman et al., Prognostic and predictive biomarkers in resected colon cancer: current status and future perspectives for integrating genomics into biomarker discovery. Oncologist 15, 390–404 (2010)
S. Lindquist, E.A. Craig, The heat-shock proteins. Annu. Rev. Genet. 22, 631–677 (1988)
S.K. Calderwood, M.A. Khaleque, D.B. Sawyer, D.R. Ciocca, Heat shock proteins in cancer: chaperones of tumorigenesis. Trends Biochem Sci 31, 164–172 (2006)
D.R. Ciocca, S.K. Calderwood, Heat shock proteins in cancer: diagnostic, prognostic, predictive, and treatment implications. Cell Stress Chaperones 10, 86–103 (2005)
A.A. Khalil, N.F. Kabapy, S.F. Deraz, C. Smith, Heat shock proteins in oncology: Diagnostic biomarkers or therapeutic targets? Biochim. Biophys. Acta 1816, 89–104 (2011)
M. Sherman, G. Multhoff, Heat shock proteins in cancer. Ann. N. Y. Acad. Sci. 1113, 192–201 (2007)
F. Cappello, S. David, F. Rappa et al., The expression of HSP60 and HSP10 in large bowel carcinomas with lymph node metastase. BMC Cancer 5, 139 (2005)
T.S. Hwang, H.S. Han, H.K. Choi et al., Differential, stage-dependent expression of Hsp70, Hsp110 and Bcl-2 in colorectal cancer. J. Gastroenterol. Hepatol. 18, 690–700 (2003)
Y. Kanazawa, H. Isomoto, M. Oka et al., Expression of heat shock protein (Hsp) 70 and Hsp 40 in colorectal cancer. Med Oncol 20, 157–164 (2003)
X.P. Wang, G.Z. Liu, A.L. Song et al., Expression and significance of heat shock protein 70 and glucose-regulated protein 94 in human esophageal carcinoma. World J. Gastroenterol. 11, 429–432 (2005)
K. Pfister, J. Radons, R. Busch et al., Patient survival by Hsp70 membrane phenotype: association with different routes of metastasis. Cancer 110, 926–935 (2007)
J. Kocsis, T. Meszaros, B. Madaras et al., High levels of acute phase proteins and soluble 70 kDa heat shock proteins are independent and additive risk factors for mortality in colorectal cancer. Cell Stress Chaperones 16, 49–55 (2011)
A.B. Benson, D. Schrag, M.R. Somerfield et al., American Society of Clinical Oncology Recommendations on Adjuvant Chemotherapy for Stage II Colon Cancer. J. Clin. Oncol. 22, 3408–3419 (2004)
J.L. Marshall, D.G. Haller, A. de Gramont et al., Adjuvant Therapy for Stage II and III Colon Cancer: Consensus Report of the International Society of Gastrointestinal Oncology. Gastrointest Cancer Res 1, 146–154 (2007)
T. Andre, A. de Gramont, An overview of adjuvant systemic chemotherapy for colon cancer. Clin. Colorectal Cancer 4(Suppl 1), S22–S28 (2004)
E.M. Tweedle, I. Khattak, C.W. Ang et al., Low molecular weight heat shock protein HSP27 is a prognostic indicator in rectal cancer but not colon cancer. Gut 59, 1501–1510 (2010)
A. Marx, P. Simon, R. Simon et al., AMACR expression in colorectal cancer is associated with left-sided tumor localization. Virchows Archiv 453, 243–248 (2008)
B. Iacopetta, Are there two sides to colorectal cancer? Int. J. Cancer 101, 403–408 (2002)
R. Langer, K. Ott, K. Specht et al., Protein expression profiling in esophageal adenocarcinoma patients indicates association of heat-shock protein 27 expression and chemotherapy response. Clin. Cancer Res. 14, 8279–8287 (2008)
C.S. Wong, V.W. Wong, C.M. Chan et al., Identification of 5-fluorouracil response proteins in colorectal carcinoma cell line SW480 by two-dimensional electrophoresis and MALDI-TOF mass spectrometry. Oncol Rep 20, 89–98 (2008)
M. Tsuruta, H. Nishibori, H. Hasegawa et al., Heat shock protein 27, a novel regulator of 5-fluorouracil resistance in colon cancer. Oncol Rep 20, 1165–1172 (2008)
D.H. Choi, J.S. Ha, W.H. Lee et al., Heat shock protein 27 is associated with irinotecan resistance in human colorectal cancer cells. FEBS Lett. 581, 1649–1656 (2007)
V. Dudeja, S.M. Vickers, A.K. Saluja, The role of heat shock proteins in gastrointestinal diseases. Gut 58, 1000–1009 (2009)
G. Jego, A. Hazoume, R. Seigneuric, C. Garrido, Targeting heat shock proteins in cancer. Cancer Lett (2010)
Y. Fukuyo, C.R. Hunt, N. Horikoshi, Geldanamycin and its anti-cancer activities. Cancer Lett. 290, 24–35 (2010)
U. Banerji, Heat Shock Protein 90 as a Drug Target: Some Like It Hot. Clin. Cancer Res. 15, 9–14 (2009)
A. Aghdassi, P. Phillips, V. Dudeja et al., Heat shock protein 70 increases tumorigenicity and inhibits apoptosis in pancreatic adenocarcinoma. Cancer Res. 67, 616–625 (2007)
P.A. Phillips, V. Dudeja, J.A. McCarroll et al., Triptolide induces pancreatic cancer cell death via inhibition of heat shock protein 70. Cancer Res. 67, 9407–9416 (2007)
Z.P. Yuan, L.J. Chen, L.Y. Fan et al., Liposomal quercetin efficiently suppresses growth of solid tumors in murine models. Clin. Cancer Res. 12, 3193–3199 (2006)
Acknowledgements
The authors thank Mrs Melitta Winkler for expert technical assistance. This study was supported by the Deutsche Forschungsgemeinschaft (DFG), grant number LA2706/1-1.
Conflict of Interest
The authors declare no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bauer, K., Nitsche, U., Slotta-Huspenina, J. et al. High HSP27 and HSP70 expression levels are independent adverse prognostic factors in primary resected colon cancer. Cell Oncol. 35, 197–205 (2012). https://doi.org/10.1007/s13402-012-0079-3
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13402-012-0079-3